Surgical Dislocation of the Hip for Femoroacetabular Impingement: A Masterclass

Key Takeaway
Welcome, fellows, to an immersive masterclass on surgical hip dislocation for femoroacetabular impingement (FAI). We'll meticulously cover preoperative planning, patient positioning, and the intricate intraoperative steps, emphasizing crucial anatomy, precise instrument handling, and potential pitfalls. This comprehensive guide ensures you gain a granular understanding of the procedure from incision to closure, preparing you for successful FAI correction and superior patient care.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a masterclass on a procedure that revolutionized joint preservation: the surgical dislocation of the hip. We are addressing a common yet often debilitating condition in active young adults: Femoroacetabular Impingement (FAI). This is not merely a clinical syndrome of vague hip pain; it is a discrete, mechanically driven pathologic condition characterized by structural abnormalities of either the femoral head–neck junction, the acetabulum, or both. These morphological deviations lead to abnormal contact forces during terminal arcs of motion, precipitating premature labral tearing and chondral degenerative changes within an otherwise nondysplastic hip.
Think of FAI as a profound mechanical mismatch. The evidence in contemporary orthopedic literature is unequivocally clear: FAI is a primary etiologic driver of early-onset osteoarthrosis, particularly in our younger, highly active patient demographic. While isolated cam or pincer FAI can occur in isolation, the vast majority of cases we encounter in clinical practice (approximately 70-80%) represent a mixed morphology, where a combination of both types drives the intra-articular pathology. The impingement itself takes place during specific extreme physiologic hip motions—primarily flexion, adduction, and internal rotation—where the abnormal bony morphology causes the femoral head–neck junction to abut the acetabular rim, acting as a fulcrum that leverages the joint apart.
Pathogenesis of Cam Impingement
Let us rigorously review the primary mechanisms of impingement, as a profound understanding of these distinct pathomechanical entities dictates our surgical strategy. Cam FAI is fundamentally a femoral-sided pathology caused by deformities of the femoral head–neck junction. Imagine the classic "pistol grip deformity" or an aspheric femoral head, where the normally smooth, concave transition from the articular surface of the head to the femoral neck is disrupted by an extra bony prominence or insufficient offset.
During hip flexion and internal rotation, this aspherical, non-concentric head–neck junction is forcefully jammed into the acetabulum. Because the acetabulum is a fixed hemisphere, the cam lesion creates a massive shearing force against the articular cartilage. This repetitive microtrauma leads to a characteristic "outside-in" delamination pattern, resulting in labrocartilaginous separation and the shearing of the acetabular cartilage away from the subchondral bone. The cartilage damage here can be devastatingly extensive, often involving full-thickness flaps or delamination defects extending up to 15 to 20 mm toward the cotyloid fossa, while the labrum itself may initially remain remarkably intact but detached from the articular margin.
Pathogenesis of Pincer Impingement
Conversely, Pincer FAI is an acetabular-sided pathology. Here, the femoral head–neck junction is typically normal and concentric, but the acetabulum itself exhibits pathologic overcoverage. This overcoverage can be focal, such as in cranial acetabular retroversion, or more global, as seen in coxa profunda or protrusio acetabuli. This excessive bony coverage leads to a premature linear contact between the acetabular rim and the normal femoral neck during physiologic range of motion.

The labrum, caught in this relentless mechanical squeeze between the femoral neck and the prominent acetabular rim, eventually undergoes intrasubstance degeneration, hypertrophies, tears, and can frequently ossify, further deepening the acetabulum. Crucially, as the anterior neck abuts the anterior rim, the femoral head is levered out posteroinferiorly in a fulcrum effect. This subtle subluxation leads to a characteristic "contrecoup" chondral lesion on the posteroinferior femoral head and corresponding posterior acetabular cartilage. Unlike cam impingement, the anterior cartilage damage in pure pincer impingement is typically restricted to a narrow circumferential strip immediately adjacent to the labrum.
Patient Presentation and Clinical Evaluation
Patients presenting with symptomatic FAI are typically active young adults, often involved in sports requiring high degrees of hip flexion and rotation (e.g., hockey, soccer, martial arts). They frequently present with an insidious onset of deep, aching groin pain, which might initially be attributed to a minor athletic strain. The pain is usually intermittent, exacerbated by athletic activities, extensive walking, pivoting, or even prolonged sitting in low chairs. It is paramount for the orthopedic surgeon to meticulously differentiate this from other potential causes of groin pain, including adductor tendinopathy, iliopsoas bursitis, osteitis pubis, or athletic pubalgia (sports hernias). Furthermore, we must rule out referred lumbosacral radiculopathy, nerve compression syndromes, and intra-abdominal pathologies.
On rigorous clinical examination, the hallmark symptoms are groin pain provoked by motion and a significantly limited internal rotation of the hip when flexed to 90 degrees. The classic anterior impingement test (FADIR: Flexion to 90 degrees, Adduction, and Internal Rotation) will typically be strongly positive, sharply reproducing the patient's chief complaint. Despite these specific mechanical limitations, overall gross hip function and gait might appear deceptively unaffected, which can obscure the severity of the underlying intra-articular derangement if a high index of suspicion is not maintained.
Detailed Surgical Anatomy and Biomechanics
The profound success and safety of surgical hip dislocation rely entirely on an absolute, uncompromising mastery of the extra-articular and intra-articular vascular anatomy. The procedure, pioneered by Professor Reinhold Ganz, is predicated on the ability to dislocate the femoral head anteriorly while entirely preserving its blood supply.
The Deep Branch of the Medial Femoral Circumflex Artery
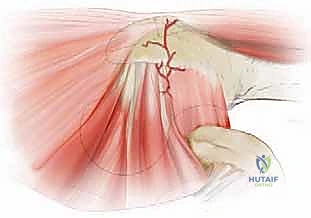
Fellows, before a scalpel ever touches the skin, you must visualize the critical vascular lifeline: the deep branch of the medial femoral circumflex artery (MFCA). This single vessel is the primary, indispensable blood supply to the mature femoral head. Failure to respect its anatomical course will inevitably result in the catastrophic, limb-altering complication of avascular necrosis (AVN) of the femoral head.

The MFCA typically branches off the deep femoral artery (profunda femoris), though variations exist. It courses posteriorly between the pectineus and psoas muscles. The critical surgical anatomy begins as it follows the inferior border of the obturator externus muscle. It reaches the intertrochanteric crest just proximal to the upper border of the quadratus femoris muscle. At this precise junction, it gives off a crucial trochanteric branch, which anastomoses with the descending branch of the superior gluteal artery.
Terminal Course and Retinacular Vessels
After giving off the trochanteric branch, the deep branch of the MFCA crosses the tendon of the obturator externus muscle posteriorly. This is a vital landmark: the obturator externus tendon protects the artery from inferior retractors during the approach. The artery then continues its course superiorly and anteriorly, lying superficial to the superior and inferior gemellus muscles and the obturator internus tendon.
Finally, the MFCA perforates the joint capsule at the level of the superior border of the piriformis tendon. Once intracapsular, it travels along the posterosuperior femoral neck within the synovial fold (the retinaculum of Weitbrecht) as the lateral epiphyseal arteries. These terminal retinacular vessels enter the epiphysis just proximal to the physeal scar. Our entire surgical approach—specifically the trochanteric flip osteotomy and the precise Z-shaped capsulotomy—is meticulously designed to leave this posterosuperior retinacular complex completely undisturbed.
Biomechanics of the Impingement-Free Arc
The ultimate biomechanical goal of surgical dislocation is to restore an impingement-free arc of motion while maintaining the structural integrity and stability of the hip joint. Normal hip flexion should reach at least 110 to 120 degrees, and internal rotation in 90 degrees of flexion should reach 20 to 30 degrees without osseous abutment.
In cam impingement, restoring this arc requires a precise femoral osteochondroplasty. We must resect the aspherical portion of the head-neck junction to recreate a normal, concave femoral neck offset. However, we must be exquisitely careful not to resect more than 30% of the cross-sectional diameter of the femoral neck, as exceeding this threshold exponentially increases the risk of iatrogenic femoral neck fracture. In pincer impingement, restoring the arc requires trimming the prominent acetabular rim. This must be balanced against the risk of creating iatrogenic dysplasia; thus, the lateral center edge angle must never be reduced to less than 25 degrees.
Exhaustive Indications and Contraindications
Patient selection is the absolute bedrock of successful joint preservation surgery. Surgical dislocation is a major, invasive procedure, and its application must be strictly governed by rigorous clinical and radiographic criteria.
Defining the Ideal Surgical Candidate
The ideal candidate for surgical dislocation of the hip is a young (typically 15 to 40 years old), highly active patient with symptomatic, clinically confirmed FAI that has proven refractory to a minimum of 3 to 6 months of comprehensive conservative management (activity modification, NSAIDs, and core/pelvic stabilization physiotherapy).
Crucially, the patient must have preserved articular cartilage. Radiographically, this translates to a preserved joint space of at least 2 mm on a standardized weight-bearing AP pelvis radiograph, with no evidence of subchondral cysts or significant osteophyte formation. The patient must also have a deformity that is too complex, too posterior, or too extensive to be safely and adequately addressed via hip arthroscopy. Examples include massive global cam lesions, severe coxa profunda requiring extensive rim trimming and labral advancement, or cases associated with prior pediatric hip diseases like Slipped Capital Femoral Epiphysis (SCFE) or Legg-Calvé-Perthes disease.
Contraindications to Joint Preservation
We must be equally rigorous in identifying patients for whom this procedure is contraindicated. The most absolute contraindication is established, advanced osteoarthritis. Patients with Tönnis grade 2 or 3 changes, or those with less than 2 mm of joint space on any radiographic view, will predictably fail joint preservation and should be directed toward total hip arthroplasty.
Age is a relative contraindication; outcomes in patients over the age of 50 are significantly inferior, largely due to the presence of irreversible, albeit sometimes radiographically subtle, chondral wear. Furthermore, severe acetabular dysplasia (Lateral Center Edge Angle < 20 degrees) is an absolute contraindication for isolated osteochondroplasty or rim trimming. These patients suffer from static instability, not impingement; removing bone from a dysplastic hip will rapidly accelerate catastrophic subluxation and failure. Such patients require a periacetabular osteotomy (PAO).
Table of Indications and Contraindications
| Category | Indications for Surgical Dislocation | Contraindications for Surgical Dislocation |
|---|---|---|
| Clinical | Symptomatic FAI failed non-op management | Asymptomatic radiographic FAI |
| Age | Typically 15 - 40 years old | > 50 years old (relative, high risk of early OA) |
| Radiographic | Joint space > 2mm, Tönnis Grade 0 or 1 | Joint space < 2mm, Tönnis Grade 2 or 3 |
| Morphology | Complex/posterior Cam, severe SCFE/Perthes | Severe dysplasia (LCEA < 20°), requiring PAO |
| Systemic | Medically fit for major open surgery | Active joint infection, severe osteopenia |
Pre-Operative Planning, Templating, and Patient Positioning
Our success in surgical hip dislocation for FAI hinges entirely on meticulous, obsessive preoperative planning. This is the phase where we construct a three-dimensional mental model of the patient's unique pathoanatomy and map out our exact bony resections.
Standardized Radiographic Protocol
We begin by reviewing a strict, standardized radiographic protocol. The Anteroposterior (AP) Pelvic View is foundational. We scrutinize the acetabulum for global overcoverage (coxa profunda, where the fossa touches the ilioischial line; or protrusio, where the femoral head crosses the ilioischial line).

For proper assessment, the central x-ray beam must be centered exactly 2 cm above the symphysis pubis, with the coccyx pointing directly toward the symphysis, separated by 1 to 2 cm. Any rotation or tilt of the pelvis will falsely project acetabular retroversion or anteversion. We specifically look for the "figure-8 sign" (crossover sign), indicating cranial acetabular retroversion where the anterior rim projects lateral to the posterior rim. We also measure the lateral center edge angle (LCEA) of Wiberg. This angle dictates exactly how many millimeters of acetabular rim can be safely resected without inducing iatrogenic instability.
Lateral Imaging and Advanced Modalities
The Lateral Cross-Table View (or Lauenstein/Dunn View) is essential for assessing the anterior and anterolateral contour of the femoral head–neck junction.

Here, we are looking for the loss of concavity or the presence of discrete anterior bumps characteristic of cam lesions. We quantify this using the alpha-angle of Nötzli. An alpha angle greater than 50 to 55 degrees is generally considered pathologic. Beyond plain films, MR Arthrography is our gold standard for evaluating the soft tissues. It is highly sensitive for detecting labral tears, paralabral cysts, and chondral delamination. Furthermore, radial CT or MRI reconstructions, reformatted exactly along the central axis of the femoral neck, are invaluable for mapping the precise clock-face location and depth of the cam lesion.
Patient Positioning and Preparation
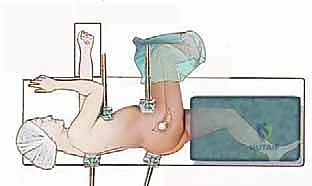
Proper patient positioning is paramount for safe surgical execution and dynamic intraoperative assessment. The patient is placed in a strict, true lateral decubitus position on a rigid radiolucent table.

This true lateral orientation is critical; if the pelvis rolls anteriorly or posteriorly, our intraoperative perception of acetabular version will be dangerously skewed. The patient is stabilized with rigid pelvic supports—one firmly against the sacrum and one slightly cephalad to the pubic symphysis. The lower, dependent leg is heavily padded and placed in a tunnel bolster to prevent peroneal nerve palsy and provide a flat bearing surface for the operative leg. The entire operative leg, from the toes to the costal margin, is meticulously prepped and draped free. A sterile bag or pocket is created anteriorly at the edge of the table; this will safely receive the distal leg when the hip is dislocated and the leg is placed in extreme external rotation and flexion.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach is a masterclass in respecting fascial planes and vascular territories. We utilize a Gibson approach combined with a digastric trochanteric flip osteotomy.
Superficial Dissection and the Gibson Interval
We make a longitudinal incision centered over the greater trochanter, extending proximally toward the posterior superior iliac spine and distally along the femoral shaft. The fascia lata is incised in line with the skin incision.
We then identify the interval between the gluteus maximus (which is retracted posteriorly) and the gluteus medius (retracted anteriorly). This is the Gibson interval. Unlike the Kocher-Langenbeck approach, we do not split the gluteus maximus, which reduces bleeding and preserves superior soft tissue integrity.

Once the interval is developed, we expose the posterior border of the gluteus medius down to its insertion on the greater trochanter. We identify the piriformis tendon and the short external rotators.
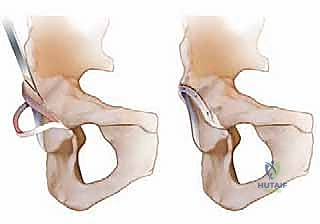
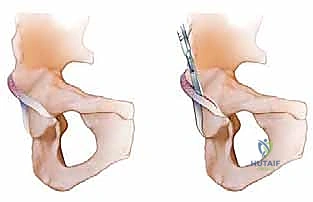
The Trochanteric Flip Osteotomy
This is the most critical step of the approach. We perform a flat, digastric osteotomy of the greater trochanter. The osteotomy must be roughly 1.5 cm thick.

Crucially, the osteotomy starts at the posterior border of the greater trochanter, anterior to the insertion of the piriformis tendon. The piriformis fossa must remain intact on the stable femoral bed, as the terminal branches of the MFCA run immediately adjacent to it.

The osteotomy exits distally just below the vastus lateralis ridge. The gluteus medius and minimus remain attached proximally, and the vastus lateralis remains attached distally, creating a mobile, digastric bony flap. This flap is retracted anteriorly, completely exposing the superior and anterior hip capsule while protecting the superior gluteal neurovascular bundle.
Capsulotomy and Safe Dislocation
With the capsule exposed, we perform a precise Z-shaped capsulotomy (for the right hip) or an inverse Z-shaped capsulotomy (for the left hip).

The longitudinal limb runs along the anterosuperior axis of the femoral neck. The proximal transverse limb runs parallel to the acetabular rim. The distal transverse limb runs parallel to the intertrochanteric line.

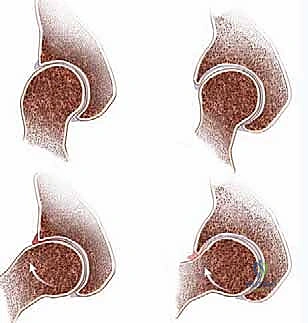
Surgical Warning: The capsulotomy must never extend posterosuperiorly beyond the equator of the femoral head, as this will sever the retinacular vessels and cause AVN. Once the capsule is opened and tagged, the hip is externally rotated, and the ligamentum teres is sharply sectioned with curved scissors or a specialized knife.
The leg is then placed into the sterile anterior bag in a position of flexion, adduction, and extreme external rotation. The femoral head gently dislocates anteriorly, providing a 360-degree view of the femoral head and complete access to the acetabulum.

Intra-Articular Resection and Repair
We now address the pathology. For the cam lesion, we perform a femoral osteochondroplasty using high-speed burrs and curved osteotomes.
We meticulously recreate the concave femoral head-neck offset, constantly checking our depth with spherical templates to avoid resecting more than 30% of the neck diameter
Clinical & Radiographic Imaging Archive