Superior Peroneal Retinaculoplasty with Periosteal Flap Augmentation for Dislocating Peroneal Tendons: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on superior peroneal retinaculoplasty with periosteal flap augmentation. We'll meticulously cover comprehensive anatomy, preoperative planning, and step-by-step intraoperative execution. Learn critical pearls, pitfalls, and post-operative management for dislocating peroneal tendons, ensuring optimal outcomes for your patients.
Comprehensive Introduction and Patho-Epidemiology
The Biomechanical Imperative of the Peroneal Tendons
Welcome, colleagues, to the operating theater. Today, we are tackling a fascinating, biomechanically complex, and often misdiagnosed condition: recurrent subluxation or dislocation of the peroneal tendons. While statistically less common than the ubiquitous lateral ankle sprain, the impact of peroneal instability on a patient's quality of life is profound, frequently leading to chronic debilitating pain, objective weakness, and functional instability. Our primary objective in this masterclass is to deconstruct and execute a Superior Peroneal Retinaculoplasty with Periosteal Flap Augmentation. This is a robust, highly reliable soft tissue procedure meticulously designed to recreate a stable fibular sulcus, augment the primary restraints, and secure the peroneal tendons against the sheer forces of dynamic ankle motion.
Before we consider making an incision, we must establish a crystal-clear understanding of the underlying pathomechanics. Peroneal tendon subluxation is fundamentally a mechanical failure of a dynamic pulley system. This failure is often initiated by an acute traumatic event but is frequently compounded by inherent anatomical predispositions. To conceptualize this, imagine the peroneal tendons as a high-tension cable, the retromalleolar fibular sulcus as its guiding pulley, and the Superior Peroneal Retinaculum (SPR) as the unyielding retaining strap. When any single component of this triad fails—be it through acute avulsion, chronic attenuation, or congenital dysplasia—the cable inevitably escapes the pulley.

The prototypical acute mechanism of injury is frequently observed in alpine skiers, gymnasts, and field athletes. It involves a sudden, forceful ankle dorsiflexion combined with a powerful, explosive eccentric contraction of the peroneal musculature, often while the foot is planted in eversion. This specific vector of forces sharply tightens the SPR, drastically decreasing its functional diameter and exponentially increasing the compartmental pressure against the posterior fibula. Unable to withstand this sudden spike in tension, the retinaculum typically fails at its weakest point: the periosteal attachment along the lateral ridge of the distal fibula. Recurrent episodes following this initial insult lead to chronic instability, progressive attenuation of the remaining retinacular tissue, and ultimately, direct attritional injury to the tendons themselves.
Pathophysiology of Retinacular Failure
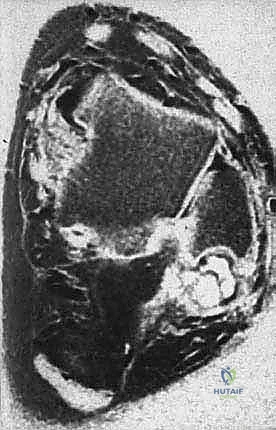
The pathophysiology of peroneal tendon dislocation cannot be fully appreciated without examining the anatomical predispositions that set the stage for failure. The morphology of the fibular groove is highly variable among the general population. Cadaveric and advanced imaging studies demonstrate that approximately 11% of individuals lack a distinct, concave fibular groove altogether, while up to 7% exhibit a convex posterior fibular morphology. A normal, competent sulcus averages 3 mm in depth and 6 mm in width, augmented by a fibrocartilaginous ridge that deepens the concavity. When this bony and cartilaginous contour is inherently shallow or convex, the tendons lack the necessary osseous containment, placing an insurmountable burden entirely on the SPR.


Furthermore, the integrity of the SPR itself is often compromised in chronic cases. We frequently encounter an SPR that is not only avulsed but severely attenuated, thinned out, or replaced by disorganized scar tissue. The native insertion of the SPR into the periosteum of the fibula is structurally weaker than a true ligament-to-bone insertion, making it highly susceptible to stripping. When the SPR is stripped away, it often takes a sleeve of periosteum with it, creating a false pouch lateral to the fibula where the tendons can chronically subluxate. This "pouch" formation is a hallmark of chronic instability and must be meticulously obliterated during surgical reconstruction.
Another critical pathophysiological factor is the presence of space-occupying lesions within the retromalleolar space, most notably a low-lying peroneus brevis (PB) muscle belly or an anomalous peroneus quartus muscle. A distal extension of the PB muscle belly—where the musculotendinous junction extends distal to the tip of the fibula—drastically increases the cross-sectional volume within the confined fibular sulcus. This creates a functional "mass effect" during muscle contraction, forcing the tendons anteriorly and laterally against the SPR, thereby increasing the sheer stress on the retinaculum and predisposing the patient to both subluxation and longitudinal split tears of the peroneus brevis.
Eckert and Davis Classification and Morphological Variants
To standardize our communication and surgical planning, we rely heavily on the Eckert and Davis classification system for acute SPR injuries, later modified by Oden. This classification describes the specific morphological pattern of retinacular failure. Grade I injuries represent a separation of the retinaculum from the fibrocartilaginous lip and the lateral malleolus. The SPR is elevated, creating a pouch, but the tendons are generally reducible. Grade II injuries involve the elevation of the distal 1 to 2 cm of the dense fibrous lip along with the SPR. The structural integrity of the labrum is compromised, and the tendons frequently fail to remain reduced even in the absence of applied tension.


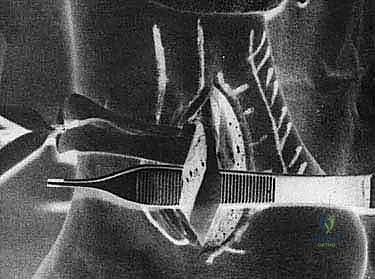
Grade III injuries are characterized by an avulsion of a thin cortical fragment of bone from the posterior aspect of the lateral malleolus, along with the attached collagenous lip and deep fascia. This is the classic "fleck sign" visible on mortise radiographs. The bony avulsion indicates a high-energy failure of the periosteal hinge. Finally, Oden's addition of Grade IV describes a tear through the mid-substance of the SPR itself, or an avulsion from its posterior attachment on the calcaneus or deep fascia, though this is exceedingly rare compared to the classic fibular stripping seen in Grades I-III.
Understanding these grades is not merely an academic exercise; it directly dictates our surgical approach. A Grade III injury with a large bony fragment might be amenable to direct osteosynthesis with small fragment screws or anchors, whereas a chronic Grade I or II injury with severe periosteal stripping and pouch formation necessitates the comprehensive retinaculoplasty and periosteal flap augmentation we are discussing today. The presence of a false pouch must be identified and eliminated to restore the physiological tension of the lateral compartment.
Detailed Surgical Anatomy and Biomechanics
Osteology of the Distal Fibula and Retromalleolar Sulcus
A profound mastery of the regional osteology is the bedrock of successful peroneal tendon surgery. The distal fibula serves not only as the lateral strut of the ankle mortise but also as the primary osseous restraint for the peroneal tendons. The retromalleolar sulcus, located on the posterior aspect of the lateral malleolus, is the anatomical cradle for these tendons. Its lateral border is formed by the lateral ridge of the fibula, which serves as the attachment site for the SPR. The medial border blends into the posterior tibiofibular ligament and the posterior aspect of the ankle joint capsule.


The morphology of this sulcus is critical. As previously noted, its depth is highly variable. The concavity is dynamically enhanced in vivo by a dense, fibrocartilaginous ridge (often referred to as the peroneal labrum) that lines the medial and lateral margins of the groove. This labrum effectively deepens the sulcus by an additional 1 to 2 millimeters, providing a smooth, frictionless surface for tendon excursion. During groove-deepening procedures, extreme care must be taken to preserve this fibrocartilaginous rim if possible, or to reconstruct a functional equivalent, to prevent postoperative tendon fraying against raw cancellous bone.
Biomechanically, the fibular sulcus acts as a fulcrum. As the peroneal muscles contract to evert and plantarflex the foot, the tendons are pulled tightly against this bony fulcrum. The reactive force generated by this vector is directed posterolaterally, directly challenging the integrity of the SPR. If the bony fulcrum is flat or convex, the vector force is shifted entirely onto the soft tissue restraints, significantly lowering the threshold for mechanical failure during athletic activities.
The Superior Peroneal Retinaculum and Ligamentous Restraints
The Superior Peroneal Retinaculum (SPR) is the undisputed primary restraint against peroneal tendon subluxation. It is a distinct, thickened band of the deep crural fascia. Anatomically, it originates from the periosteum of the posterolateral ridge of the distal fibula. From this origin, it courses posteromedially to insert onto the lateral wall of the calcaneus, blending with the Achilles tendon sheath and the superficial fascia of the leg. The SPR forms the posterolateral roof of the retromalleolar fibro-osseous tunnel.

The architecture of the SPR is not uniform; it exhibits significant inter-individual variability in thickness, width, and distinctness from the surrounding fascia. In some patients, it is a robust, distinct ligamentous band, while in others, it is a thin, diaphanous continuation of the crural fascia. This inherent variability explains why some individuals are more prone to injury under similar biomechanical loads. Furthermore, the SPR does not act in isolation. It works synergistically with the calcaneofibular ligament (CFL), which lies deep to the peroneal tendons and forms the floor of the tendon sheath distal to the fibula.
During surgical reconstruction, recreating the precise tension of the SPR is an intraoperative balancing act. If the retinaculoplasty is left too lax, the patient will experience recurrent subluxation. Conversely, if the repair is excessively tight, it can result in stenosing tenosynovitis, profound restriction of tendon excursion, and iatrogenic pain. The periosteal flap augmentation technique provides a dual advantage: it reinforces the attenuated SPR with robust, vascularized periosteal tissue, and allows for precise, titratable tensioning of the repair over the repositioned tendons.
Musculotendinous Architecture and Anomalous Variants
The lateral compartment of the leg houses the peroneus longus (PL) and peroneus brevis (PB) muscles, both innervated by the superficial peroneal nerve. The PB muscle originates from the distal two-thirds of the lateral fibular shaft, while the PL originates more proximally from the head and proximal two-thirds of the fibula. As they descend toward the retromalleolar sulcus, their spatial relationship is highly specific and clinically relevant: the PB tendon lies anterior and medial (deep) to the PL tendon. The PB is directly apposed to the fibular sulcus, making it highly susceptible to mechanical attrition, longitudinal split tears, and tenosynovitis when the sulcus is shallow or the retinaculum is incompetent.


Anomalous muscle variants are frequently encountered during peroneal exploration and must be systematically addressed. The most common variant is the peroneus quartus muscle, present in approximately 10% to 20% of the population. It typically originates from the distal PB muscle belly or the fibula and inserts onto the retrotrochlear eminence of the calcaneus. When present, its muscle belly or tendon occupies valuable real estate within the already constrained retromalleolar tunnel. This overcrowding exacerbates the "mass effect," pushing the primary tendons laterally and increasing tension on the SPR.
Similarly, a low-lying PB muscle belly—where muscular tissue extends into the fibular groove rather than transitioning to tendon proximally—creates a similar pathological crowding. During surgery, it is imperative to identify these space-occupying structures. If a peroneus quartus is present and contributing to overcrowding, it should be routinely excised. If a low-lying PB muscle belly is identified, a debulking tenosynovectomy or meticulous muscle belly resection (preserving the tendon proper) may be necessary to decompress the tunnel and allow for a tension-free retinacular repair.
Critical Neurovascular Topography
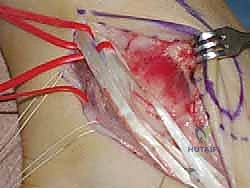
The surgical approach to the lateral ankle is fraught with potential neurovascular pitfalls, the most significant of which is the sural nerve. The sural nerve provides sensory innervation to the posterolateral aspect of the distal third of the leg and the lateral border of the foot. It typically courses distally in the subcutaneous fat, running in close proximity to the small saphenous vein. As it approaches the ankle, it curves posterior and inferior to the lateral malleolus, crossing directly over the superficial aspect of the peroneal tendon sheath.


The arborization pattern of the sural nerve is notoriously variable. It frequently branches into lateral calcaneal and lateral dorsal cutaneous branches proximal to or directly over the operative field. Iatrogenic injury to the sural nerve—whether through direct transection, aggressive traction neuropraxia, or entrapment in the retinacular repair—is a devastating complication. It can result in intractable neuropathic pain, painful neuromas, and complex regional pain syndrome (CRPS), which can completely overshadow a biomechanically successful tendon repair.
Therefore, meticulous, blunt subcutaneous dissection is mandatory. The nerve must be definitively identified, gently mobilized, and protected with a vessel loop or delicate retraction throughout the entirety of the procedure. Deep to the fascial layer, the peroneal artery gives off calcaneal branches that supply the lateral hindfoot, but these are generally protected if the dissection remains strictly within the sub-periosteal or intra-sheath planes. Hemostasis must be meticulous to prevent postoperative hematoma, which can increase pressure on the skin flaps and compromise wound healing in this notoriously fragile soft-tissue envelope.
Exhaustive Indications and Contraindications
Defining the Operative Candidate
The decision to proceed with a Superior Peroneal Retinaculoplasty and Periosteal Flap Augmentation is predicated on a careful synthesis of the patient's clinical history, physical examination, and advanced imaging. The classic indication is a patient presenting with chronic, symptomatic recurrent subluxation or dislocation of the peroneal tendons that has proven refractory to a dedicated trial of conservative management. Conservative measures typically include a period of immobilization, non-steroidal anti-inflammatory drugs (NSAIDs), lateral heel wedges, and rigorous physical therapy focusing on peroneal strengthening and proprioceptive retraining.


Acute, first-time dislocations present a more nuanced decision-making paradigm. While some literature supports a trial of non-operative management (e.g., short-leg cast in slight plantarflexion and inversion for 4-6 weeks), the failure rate and subsequent risk of recurrent instability are unacceptably high, particularly in young, high-demand athletes. Therefore, acute surgical repair is increasingly favored for competitive athletes or individuals with high occupational demands to ensure a rapid and reliable return to function. Furthermore, the presence of a Grade III injury (bony avulsion) or concomitant structural pathology, such as a high-grade longitudinal split tear of the peroneus brevis, serves as an absolute indication for early surgical intervention.
Patients who report a painful "snapping" sensation lateral to the fibula, accompanied by objective weakness in eversion and a positive apprehension test, are prime candidates. The goal is not merely to restore anatomy, but to halt the progression of attritional tendon damage. Every episode of subluxation acts like a saw blade against the fibular ridge, progressively fraying the PB tendon. Intervening before a simple subluxation evolves into a complex, irreparable tendon tear is the hallmark of astute orthopedic management.
Absolute and Relative Contraindications
While this procedure is highly efficacious, it is not universally applicable. Absolute contraindications are primarily related to the viability of the host environment. Active local or systemic infection precludes any elective soft tissue reconstruction. Severe peripheral vascular disease (PVD) or profound microvascular compromise (as seen in poorly controlled, long-standing diabetes mellitus) constitutes a near-absolute contraindication due to the high risk of catastrophic wound dehiscence and flap necrosis over the lateral malleolus.

Relative contraindications require careful preoperative optimization and patient counseling. Chronic heavy tobacco use significantly impairs microcirculation and exponentially increases the risk of delayed wound healing and infection. We strongly advocate for strict smoking cessation for a minimum of 4-6 weeks prior to surgery. Additionally, severe, uncorrected hindfoot varus malalignment is a critical relative contraindication. A varus hindfoot places continuous, excessive eccentric load on the peroneal tendons and the lateral soft tissue restraints. Performing a retinaculoplasty in the setting of an uncorrected cavovarus foot is a recipe for early mechanical failure and recurrent dislocation. In such cases, a concomitant lateralizing calcaneal osteotomy or first metatarsal dorsiflexion osteotomy must be strongly considered to correct the underlying biomechanical driver.
Patient compliance is another vital consideration. The postoperative rehabilitation protocol requires strict adherence to weight-bearing restrictions and phased mobilization. Patients with severe psychiatric comorbidities, substance abuse issues, or those who are otherwise unable to comprehend or adhere to the rigorous postoperative regimen are poor candidates for this complex reconstruction.
Decision-Making Matrix for Retinaculoplasty
| Clinical Scenario | Primary Pathology | Recommended Surgical Intervention | Rationale |
|---|---|---|---|
| Acute, First-Time Dislocation (Athlete) | Grade I/II SPR avulsion, no tendon tear | Direct SPR repair to fibula +/- groove deepening | High risk of recurrence with conservative care; early return to sport. |
| Acute Dislocation with "Fleck Sign" | Grade III SPR bony avulsion | Open Reduction Internal Fixation (ORIF) of fragment or anchor repair | Restores native bone-to-bone healing of the periosteal hinge. |
| Chronic Recurrent Subluxation | Attenuated SPR, shallow groove, false pouch | Retinaculoplasty + Periosteal Flap + Groove Deepening | Native SPR is insufficient; requires robust augmentation and osseous containment. |
| Chronic Subluxation + PB Split Tear | Attenuated SPR, attritional tendon injury | Retinaculoplasty + Groove Deepening + PB Tubularization/Repair | Must address both the instability and the structural tendon damage to relieve pain. |
| Subluxation + Severe Hindfoot Varus | Biomechanical overload of lateral structures | Retinaculoplasty + Lateralizing Calcaneal Osteotomy | Soft tissue repair will fail if the underlying bony varus malalignment is not corrected. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Provocative Testing
The clinical evaluation begins with a meticulous history, focusing on the mechanism of injury, the chronicity of symptoms, and the specific nature of the pain. Patients frequently report a persistent, deep aching pain localized to the posterolateral ankle, exacerbated by uneven terrain or pivoting maneuvers. A sensation of snapping, popping, or the tendon "giving way" is classic. Distinguishing this from a standard lateral ankle sprain is paramount. While an anterior talofibular ligament (ATFL) injury presents with tenderness anterodistal to the lateral malleolus, peroneal pathology presents with exquisite tenderness directly posterior to the fibula, along the course of the tendon sheath.


Physical examination must be systematic. Inspection may reveal mild retromalleolar swelling or fullness, representing tenosynovitis or the presence of a false pouch. The cornerstone of the physical exam is provocative testing. The Peroneal Tendon Subluxation Test is performed with the patient seated or prone. The examiner places the ankle in slight plantarflexion and inversion, then resists the patient's active, forceful dorsiflexion and eversion. The examiner's fingers are placed lightly over the retromalleolar groove. A positive test is indicated by palpable or visible anterior translation (subluxation) of the tendons over the fibular ridge, often accompanied by a reproducible "snap" and patient apprehension.
Additionally, the examiner must assess hindfoot alignment. The patient should be observed standing from behind to evaluate for a varus heel (peek-a-boo heel sign), which would suggest a cavovarus foot structure. The Coleman block test can be utilized to determine if the hindfoot varus is flexible and driven by a plantarflexed first ray. Finally, a thorough neurological examination, specifically mapping the sensory distribution of the sural and superficial peroneal nerves, must be documented preoperatively to establish a baseline and rule out pre-existing neuropathy.
Advanced Imaging and Radiographic Assessment
While the diagnosis of peroneal subluxation is primarily clinical, advanced imaging is indispensable for preoperative surgical mapping. Standard weight-bearing radiographs (AP, lateral, and mortise views of the ankle) are the initial step. They are crucial for ruling out occult fractures, evaluating joint space narrowing, and assessing overall osseous alignment. As previously discussed, the mortise view must be scrutinized for the "fleck sign"—a small cortical avulsion fragment adjacent to the lateral border of the distal fibula, which is pathognomonic for a Grade III SPR avulsion.


Magnetic Resonance Imaging (MRI) without contrast is the gold standard for soft tissue evaluation. High-resolution axial cuts are particularly critical. MRI allows the surgeon to assess the precise morphology of the fibular sulcus (flat, shallow, or convex) and the integrity of the SPR. It is highly sensitive for detecting concomitant tendon pathology, such as tenosynovitis, tendinosis, or longitudinal split tears of the peroneus brevis, which appear as a "C-shaped" or "boomerang" tendon wrapping around the peroneus longus. Furthermore, MRI is excellent for identifying anomalous structures like a peroneus quartus muscle or a low-lying PB muscle belly that may necessitate intraoperative debridement.
Dynamic ultrasound is an increasingly valuable, cost-effective adjunct in our diagnostic armamentarium. Unlike static MRI, ultrasound allows for real-time visualization of the tendons during provocative maneuvers. The transducer is placed transversely over the retromalleolar groove while the patient actively dorsiflexes and everts the ankle. The examiner can dynamically visualize the tendons snapping anteriorly over the fibular ridge, confirming the diagnosis with 100% specificity. It also allows for dynamic assessment of tendon tears and the presence of fluid within the sheath.
Anesthesia, Patient Positioning, and Operative Setup
The procedure is typically performed under general anesthesia or a robust regional block (spinal or popliteal sciatic nerve block combined with a saphenous nerve block), depending on patient comorbidities and anesthesiologist preference. A regional block provides excellent intraoperative muscle relaxation and profound postoperative analgesia, significantly reducing the requirement for systemic narcotics in the immediate recovery phase.


Patient positioning is critical for optimal exposure. The patient is typically placed in the lateral decubitus position, with the operative leg facing upward
Clinical & Radiographic Imaging Archive