Supracondylar Humeral Osteotomy: A Masterclass in Cubitus Varus Correction
Key Takeaway
This masterclass details supracondylar humeral osteotomy for cubitus varus. We cover comprehensive anatomy, meticulous preoperative templating, and step-by-step intraoperative execution. Learn precise K-wire fixation, managing lateral condylar prominence, and critical neurovascular protection. Postoperative care and complication strategies are also thoroughly discussed, ensuring fellows gain a complete understanding of this challenging pediatric elbow deformity correction.
Fellows, welcome to the operating theater. Today, we are tackling a fascinating and often cosmetically challenging pediatric deformity: cubitus varus. Specifically, we will be addressing it with a supracondylar humeral osteotomy. This procedure is not merely about straightening an arm; it is about restoring a child's confidence, normalizing upper extremity biomechanics, and preventing potential long-term neurologic and structural complications. Let us scrub in and walk through this procedure with the precision, respect, and purpose that pediatric bone demands.
Comprehensive Introduction and Patho-Epidemiology
Before we make any incisions, it is absolutely crucial to understand the pathology we are addressing. Cubitus varus, colloquially known as the "gunstock deformity," is a structural malalignment of the distal humerus characterized by a complete loss or reversal of the physiological valgus "carrying angle" between the upper arm and the forearm. Historically, this deformity represented one of the most frequent and notorious complications following a pediatric supracondylar humerus fracture, with historical literature citing frequencies as staggeringly high as 30%. It stands as a testament to modern advancements in closed reduction and percutaneous pinning techniques that we see this less frequently as a new complication today. However, we still frequently manage the sequelae of older, malunited fractures, neglected injuries, or cases from resource-limited settings.
The pathogenesis of post-traumatic cubitus varus is rooted almost exclusively in the malunion of a supracondylar humerus fracture, rather than an injury to the physis itself. The deformity is primarily a metaphyseal coronal plane malalignment. This varus angulation typically results from medial column comminution at the time of the initial injury, causing the fracture fragment to collapse into varus during the healing phase. Less commonly, it can be driven by a failure to adequately reduce internal rotation of the distal fragment, which biomechanically translates into coronal varus when the arm is extended, or by lateral gaping at the fracture site due to inadequate fixation. Crucially, fellows must recognize that this is not due to a growth disturbance of the distal humerus epiphysis; the physis remains open and functional, but it is growing from a malaligned metaphyseal base.
When we evaluate these young patients in the clinic, a detailed and empathetic history is paramount. We must understand both parental and patient expectations. While there is often little functional deficit in activities of daily living, the cosmetic appearance is usually the primary driving force for consultation. Visual inspection will immediately reveal a varus deviation of the mechanical axis compared to the unaffected, contralateral side. Range of motion must be documented meticulously. While cubitus varus itself often does not limit flexion or extension significantly, coexisting sagittal plane deformities (typically extension malunions at the fracture site) can lead to clinically significant hyperextension of the elbow and a corresponding loss of terminal flexion.
Furthermore, a thorough examination of the neurovascular status is absolutely essential. We are particularly concerned about the median, ulnar, and radial nerves. Tardy ulnar nerve palsy is a known long-term complication of untreated cubitus varus. This occurs due to the chronic malpositioning of the medial head of the triceps muscle, which shifts the olecranon medially within the olecranon fossa, subsequently stretching the ulnar nerve over the medial epicondyle or causing it to subluxate. Additionally, it is vital to distinguish true post-traumatic cubitus varus from other conditions in our differential diagnosis, such as medial humeral condylar growth arrest, malunited lateral humeral condyle fractures, or congenital dislocations of the radial head.
Detailed Surgical Anatomy and Biomechanics
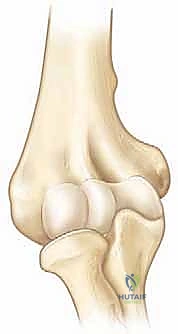
A profound, three-dimensional understanding of the distal humeral anatomy is our primary compass in this procedure. The distal humerus, particularly in a skeletally immature patient, is a delicate and highly complex structural unit. The osteology consists of two diverging structural columns: a medial column ending in the medial epicondyle, and a lateral column ending in the lateral epicondyle and capitellum. These columns are separated by the wafer-thin bone of the olecranon fossa posteriorly and the coronoid fossa anteriorly. In children, the cortices of the distal humerus are thinner, and the anteroposterior (AP) diameter is significantly decreased compared to adults. This anatomical reality directly dictates our osteotomy technique, necessitating precise saw cuts to avoid catastrophic fracturing of the columns and influencing our choice of fixation implants.
The neurovascular topography surrounding the distal humerus is unforgiving, and this is where the surgeon must be most vigilant. The median nerve and brachial artery run along the medial border of the biceps brachii muscle in the upper arm, eventually lying anterior and slightly medial in the cubital fossa. While our preferred approach for the osteotomy is lateral, we must be acutely aware of these anterior structures, especially if an anterior retractor is placed too vigorously or if the saw blade breaches the anterior cortex uncontrollably.
The radial nerve is of paramount relevance to our lateral approach. It enters the anterior compartment of the arm in the distal third, piercing the lateral intermuscular septum and traveling between the brachialis and brachioradialis muscles. Crucially, it passes directly over the anterolateral aspect of the distal humerus before entering the supinator muscle in the proximal forearm. Its immediate proximity to our lateral incision and the planned osteotomy site demands meticulous, layer-by-layer dissection and absolute protection with blunt retractors. Conversely, the ulnar nerve runs posterior to the medial epicondyle within the cubital tunnel. Although our primary surgical dissection is lateral, when we apply a valgus force to close the lateral wedge osteotomy, the medial structures undergo tension. The ulnar nerve must be actively protected, as it is easily stretched during this maneuver, potentially leading to devastating iatrogenic neurapraxia.
From a biomechanical perspective, the cubitus varus deformity alters the normal force vectors across the elbow joint. The mechanical axis of the upper extremity is shifted medially. This medial shift alters the line of pull of the triceps and biceps, decreasing their mechanical advantage. Furthermore, this abnormal alignment places increased tensile stress on the lateral collateral ligamentous complex and increased compressive forces on the medial radiocapitellar joint. Over time, this altered biomechanical environment is hypothesized to contribute to an increased risk of subsequent lateral condyle fractures, as the lateral column is subjected to abnormal stress shielding and altered force transmission during falls. Correcting the alignment restores the physiological distribution of forces across the pediatric elbow.
Exhaustive Indications and Contraindications
The decision to proceed with a supracondylar humeral osteotomy is not one to be taken lightly. The primary indication is a skeletally immature child presenting with a static, well-defined post-traumatic cubitus varus deformity that is cosmetically unacceptable to the patient and their family. However, the indications extend beyond mere cosmesis. We intervene to prevent the well-documented long-term sequelae of the deformity. Chief among these is tardy ulnar nerve palsy, which can present years or even decades after the initial injury due to chronic traction and friction within the altered cubital tunnel. Additionally, correcting the mechanical axis mitigates the increased risk of secondary fractures, particularly lateral condyle fractures, and restores normal joint kinematics.
Timing is a critical component of our surgical indications. We mandate waiting at least one full year following the initial supracondylar fracture before considering corrective osteotomy. This waiting period serves two vital purposes: first, it ensures that the fracture has fully healed and the bone has undergone maximal spontaneous remodeling (though coronal plane deformities do not remodel significantly); second, and more importantly, it allows us to definitively rule out avascular necrosis (AVN) of the distal humeral epiphysis, particularly the trochlea. Performing an osteotomy in the presence of evolving AVN can lead to catastrophic joint destruction.
Contraindications must be rigorously respected to avoid disastrous outcomes. Absolute contraindications include active local or systemic infection, severe soft tissue compromise around the elbow that would preclude safe incision and healing, and a functionally painless elbow in a patient (or family) with unrealistic cosmetic expectations. Relative contraindications encompass profound preoperative stiffness or intra-articular incongruity, as an extra-articular metaphyseal osteotomy will not correct intra-articular pathology and may, in fact, exacerbate stiffness.
| Category | Specific Factors | Clinical Rationale |
|---|---|---|
| Absolute Indications | Cosmetically unacceptable deformity | Psychosocial impact on the developing child. |
| Symptomatic tardy ulnar nerve palsy | Prevent irreversible axonal damage and intrinsic muscle wasting. | |
| Posterolateral rotatory instability | Restoring the mechanical axis normalizes ligamentous tension. | |
| Relative Indications | Prevention of secondary fractures | Altered biomechanics increase risk of lateral condyle fractures. |
| Hyperextension deformity > 15 degrees | Can be corrected simultaneously with a multiplanar osteotomy. | |
| Absolute Contraindications | Active joint or soft tissue infection | High risk of osteomyelitis and hardware failure. |
| Evolving avascular necrosis | Osteotomy will not salvage the joint and may accelerate collapse. | |
| Less than 1 year post-injury | Must allow for complete healing and stabilization of the deformity. | |
| Relative Contraindications | Severe intra-articular incongruity | Extra-articular osteotomy will not address the primary mechanical block. |
Pre-Operative Planning, Templating, and Patient Positioning
Precision in the operating room is born from exhaustive preoperative planning. We do not simply "wing it" when correcting pediatric deformities; every cut, every angle, and every millimeter of translation is meticulously calculated beforehand. The foundation of this planning relies on high-quality, standardized imaging.
Imaging and Diagnostic Studies
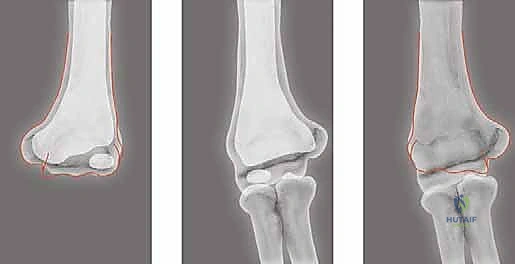
We always commence with standard anteroposterior (AP) and lateral radiographs of the affected elbow.

However, standard views are insufficient for precise templating. We mandate an AP radiograph of both the affected and the unaffected elbows, taken with the arms in full extension and maximal supination. It is imperative that these images include the distal humerus, the entire forearm, and the wrist to allow for accurate calculation of the mechanical axis. This bilateral comparison is the absolute cornerstone of our templating process. In very young children, or in cases where a subtle distal humeral growth disturbance (such as a partial physeal arrest) is suspected alongside the malunion, an MRI of the elbow can be an invaluable adjunct to evaluate the unossified cartilaginous anlage.
Templating the Correction
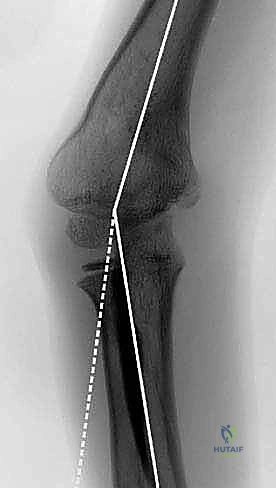
Templating is where the surgery is truly won or lost. Using the bilateral AP radiographs, we first determine the Angle of Baumann and the Humeral-Elbow-Wrist (HEW) angle for both the affected and unaffected sides. The difference in the carrying angle (or HEW angle) between the two sides quantifies the exact magnitude of the cubitus varus deformity.
We utilize a tracing superimposition technique. A tracing of the normal, unaffected arm is made on translucent tracing paper. This tracing is then flipped (reversed) and carefully superimposed over the radiograph of the operative arm. By aligning the diaphyses, the required angle of correction becomes visually and mathematically apparent. The angle of the laterally based bone wedge to be removed will precisely equal the angle of desired correction.
The design of the osteotomy itself requires nuanced understanding. The distal osteotomy cut is planned just proximal to the olecranon fossa to ensure we are in metaphyseal bone, which heals rapidly, while avoiding intra-articular penetration. Crucially, we plan the osteotomy with equal lengths of the proximal and distal limbs along the lateral cortex. This specific geometry diminishes the tendency for a lateral condylar prominence (the dreaded "lazy-S" deformity) post-correction. While a medial hinge provides excellent intrinsic stability, simply closing a lateral wedge on a medial hinge invariably shifts the mechanical axis of the forearm laterally. In patients where this shift would create an unacceptable cosmetic bump, we must anticipate performing a complete osteotomy, allowing for controlled medial translation of the distal fragment to centralize the mechanical axis.
Patient Positioning
Once the plan is finalized, patient positioning must facilitate flawless execution. The patient is placed supine on the operating table, with the patient's head shifted slightly away from the operative side. The affected arm is positioned on a radiolucent extremity hand table. This setup allows for completely unrestricted intraoperative fluoroscopy in multiple planes.
A sterile upper arm tourniquet is applied as proximal as possible. This is indispensable for achieving a bloodless field, which is a prerequisite for the safe identification and protection of the delicate neurovascular structures, particularly the radial nerve. The C-arm fluoroscopy unit is draped and brought in from either the head or the foot of the table, positioned to allow for immediate, effortless AP and lateral views of the elbow without needing to awkwardly reposition the patient's arm. This real-time radiographic feedback is critical during the osteotomy and subsequent hardware fixation.
Step-by-Step Surgical Approach and Fixation Technique
With the plan templated and the patient optimally positioned, we proceed with the surgical execution. The preferred approach for a lateral closing wedge osteotomy is, naturally, a lateral approach.
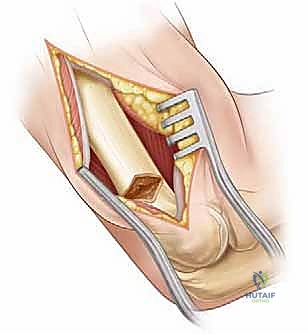
Incision and Exposure
We begin with a straight longitudinal incision, approximately 6 to 8 centimeters in length, centered precisely over the lateral epicondylar ridge of the distal humerus.
This incision is deliberately placed slightly posterior to the epicondylar ridge itself. We carry the dissection sharply down through the dermis and subcutaneous tissues, achieving meticulous hemostasis with bipolar electrocautery. The deep dissection aims to exploit the internervous plane between the lateral head of the triceps muscle (innervated by the radial nerve) posteriorly and the extensor carpi radialis longus (ECRL) and brachioradialis (also innervated by the radial nerve, but distinct muscle bellies) anteriorly.
Using blunt dissection, we carefully separate these muscle groups. The triceps is elevated and retracted posteriorly, while the anterior compartment musculature is mobilized anteriorly. As we deepen our dissection to the bone, we incise the periosteum longitudinally along the lateral supracondylar ridge. Subperiosteal elevation is performed anteriorly and posteriorly just enough to expose the planned osteotomy site. We must be exceptionally careful anteriorly to avoid breaching the periosteal sleeve and endangering the radial nerve, which lies in close proximity to the brachialis muscle.
Osteotomy Execution
Under direct fluoroscopic guidance, we translate our preoperative template to the bone. We frequently utilize smooth Kirschner wires (K-wires) as physical guide pins for our saw cuts.
The distal pin is placed parallel to the joint line (referencing the capitellum and trochlea), and the proximal pin is placed at the predetermined angle of correction relative to the distal pin. The intersection of these pins dictates the apex of our wedge, which should ideally sit at the medial cortex.
Using a fine-toothed oscillating saw with continuous cool saline irrigation to prevent thermal necrosis of the pediatric bone, we perform the osteotomy.
The cuts are made immediately adjacent to our guide pins. We cut through the lateral, anterior, and posterior cortices, taking great care as we approach the medial cortex. Depending on our preoperative plan regarding medial translation, we either leave a 1-2 millimeter medial cortical hinge intact to act as a stabilizing fulcrum, or we complete the cut entirely. If the wedge is removed and the osteotomy is closed, we assess the alignment clinically and fluoroscopically. If a lateral prominence is noted, the medial hinge is deliberately fractured, and the distal fragment is translated medially by 5 to 10 millimeters until the lateral cortices are flush.
Fixation Construct
Once the wedge is closed and the desired valgus alignment and translation are achieved, rigid fixation is required. The choice of fixation depends on the surgeon's preference, the child's age, and the intrinsic stability of the osteotomy.
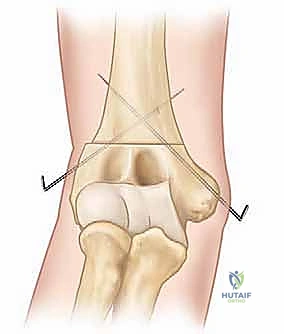
For younger children with a stable medial hinge, crossed divergent K-wires (typically 1.6mm or 2.0mm) driven from the lateral condyle into the medial diaphysis, and from the medial epicondyle into the lateral diaphysis, provide excellent stability. However, placing the medial pin carries a risk to the ulnar nerve, often necessitating a small medial incision to protect it.
Alternatively, and increasingly favored in older children or when medial translation has been performed, lateral plate fixation is utilized. A pre-contoured pediatric distal humerus locking plate or a reconstructed pelvic reconstruction plate is applied to the lateral column. This provides robust, rigid fixation, eliminates the need for medial pin placement, and allows for earlier postoperative mobilization. Regardless of the method, final AP and lateral fluoroscopic images are obtained to confirm perfect restoration of Baumann's angle, anatomical alignment, and secure hardware placement.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and execution, supracondylar osteotomies carry a distinct profile of potential complications. The astute surgeon must be prepared to identify and manage these effectively.
Neurologic injury is the most feared immediate complication. The radial nerve is at risk during the lateral exposure and anterior retractor placement. Radial nerve neurapraxia occurs in approximately 2-5% of cases and typically resolves spontaneously with observation. Ulnar nerve injury is less common but can occur either from direct trauma during medial K-wire placement or from excessive traction when closing a large lateral wedge. If a medial pin is used, a mini-open technique to visualize and protect the ulnar nerve is mandatory.
The most common cosmetic complication is the development of a lateral condylar prominence, often referred to as the "lazy-S" deformity. This occurs when a simple lateral closing wedge osteotomy is performed without medial translation of the distal fragment, effectively shifting the mechanical axis of the forearm laterally relative to the humeral shaft. While functionally benign, it can be highly distressing to the patient. Prevention, through meticulous templating and intraoperative medial translation, is the best management.
Loss of fixation, nonunion, or malunion are rare but significant complications, particularly if fixation was tenuous or if the patient is non-compliant with postoperative immobilization.


Deep infection is exceptionally rare (<1%) but requires immediate surgical debridement and appropriate intravenous antibiotic therapy. If fixation is lost early, revision surgery with more robust hardware (e.g., switching from pins to a locking plate) is indicated.
| Complication | Estimated Incidence | Prevention / Salvage Strategy |
|---|---|---|
| Lateral Condylar Prominence | 15 - 30% (if not translated) | Prevention: Preoperative templating; intraoperative medial translation of the distal fragment. Salvage: Revisional osteotomy or lateral condylectomy (rarely indicated). |
| Radial Nerve Neurapraxia | 2 - 5% | Prevention: Meticulous blunt dissection; avoid aggressive anterior retraction. Salvage: Observation; EMG at 6 weeks if no recovery; nerve exploration if completely transected (rare). |
| Ulnar Nerve Injury | 1 - 3% | Prevention: Mini-open medial approach for pin placement; avoid over-correction into extreme valgus. Salvage: Pin removal if impinging; ulnar nerve transposition if traction neuropathy persists. |
| Loss of Fixation / Malunion | 2 - 4% | Prevention: Rigid fixation (plates > pins for unstable cuts); strict post-op immobilization. Salvage: Revision open reduction and rigid internal fixation with bone grafting if nonunion occurs. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation phase is as critical as the surgical execution itself. The protocol is phased to balance the need for bone healing with the goal of restoring full range of motion.
In the immediate postoperative phase (Weeks 0-3), the primary goal is protecting the osteotomy and managing edema. The patient is placed in a well-padded long arm cast or a rigid posterior splint with the elbow flexed to approximately 60-90 degrees and the forearm in neutral rotation. The arm must be kept strictly elevated to minimize swelling. Pain management is optimized, and the patient is discharged home once comfortable. During this period, absolute immobilization of the elbow is required, though active range of motion of the fingers and shoulder is strongly encouraged to prevent secondary stiffness.
The intermediate phase (Weeks 3-6) begins with the first postoperative clinic visit. Radiographs are obtained to assess early callus formation and hardware position. If K-wires were utilized and left protruding through the skin, they are typically removed in the clinic at the 3 to 4-week mark, provided radiographic healing is progressing. The cast is discontinued, and the patient is transitioned to a removable hinged elbow brace. Active and active-assisted range of motion exercises for elbow flexion, extension, pronation, and supination are initiated. Passive, forceful stretching is strictly prohibited, as it can induce heterotopic ossification or compromise the healing osteotomy.
The advanced rehabilitation phase (Weeks 6-12 and beyond) focuses on restoring full strength and terminal range of motion. Once radiographic union is definitively confirmed (typically around 6-8 weeks), the brace is discontinued entirely. Progressive resistance exercises are introduced to strengthen the biceps, triceps, and forearm musculature. Patients are gradually allowed to return to full, unrestricted activities, including contact sports, usually by the 3 to 4-month mark, contingent upon full radiographic consolidation and symmetrical strength recovery. Long-term follow-up is maintained for at least 1-2 years to monitor for any late growth disturbances, though this is exceedingly rare following a purely metaphyseal osteotomy.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of cubitus varus has evolved significantly over the past several decades, guided by robust clinical literature. Historically, the French osteotomy (a lateral closing wedge combined with derotation) and the dome osteotomy were heavily debated. The dome osteotomy, while theoretically avoiding the lateral prominence by rotating the distal fragment along a semicircular cut, is technically demanding and carries a higher risk of instability and neurovascular injury.
Modern consensus, heavily influenced by the work of authors like Bellemore and Wilkins, strongly favors the modified lateral closing wedge osteotomy with medial translation. Landmark comparative studies have demonstrated that when accompanied by appropriate medial translation, the lateral closing wedge provides the most reliable correction of the mechanical axis with the lowest complication profile.
Furthermore, recent literature has focused heavily on fixation constructs. While crossed K-wires remain a staple in younger children due to their low cost and ease of removal, biomechanical studies and retrospective clinical reviews increasingly advocate for lateral plate fixation in older children and adolescents. Plating provides superior torsional and bending stiffness, allowing for earlier mobilization and theoretically reducing the risk of loss of fixation. Ultimately, the definitive textbook approach requires the surgeon to be facile with templating, precise with their osteotomy execution, and adaptable in their choice of fixation to meet the specific anatomical demands of each pediatric patient.
