Arthroscopic Subscapularis Repair: An Intraoperative Masterclass for Fellows
Key Takeaway
This masterclass provides an exhaustive guide to arthroscopic subscapularis repair. Fellows will learn intricate surgical anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative technique. We cover portal placement, visualization pearls, tendon mobilization, and precise hardware application, emphasizing neurovascular safety and avoiding common pitfalls. Postoperative rehabilitation and complication management are also thoroughly discussed for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we delve into the intricate world of arthroscopic subscapularis repair, a procedure that, while historically underappreciated, is critical for restoring shoulder function and stability. For decades, the subscapularis was deemed the "forgotten tendon" or the "hidden lesion" of the rotator cuff. Open approaches were morbid, and early arthroscopic techniques lacked the sophisticated visualization and instrumentation required to adequately address this anterior structure. However, with the advent of 30-degree and 70-degree arthroscopes, alongside advanced portal placement strategies, our ability to identify and anatomically restore the subscapularis has revolutionized shoulder surgery. This isn't just about fixing a tear; it's about understanding the biomechanics, the anatomy, and the nuances that differentiate a good outcome from an excellent one. Scrub in, let's begin.
The epidemiology of subscapularis tears presents a bimodal distribution that dictates our clinical suspicion and surgical approach. In the younger, active demographic, tears are typically traumatic, resulting from a forceful hyperextension or external rotation injury with the arm in adduction. These acute events often lead to avulsion-type injuries, sometimes taking a piece of the lesser tuberosity with them. Conversely, in the older population, tears are predominantly degenerative, insidious in onset, and frequently associated with anterosuperior impingement and concomitant supraspinatus pathology. Recognizing this bimodal nature is essential, as the tissue quality, retraction patterns, and associated labral or biceps pathologies vary significantly between these two cohorts.
A critical element of the pathogenesis, particularly in degenerative tears, is the concept of subcoracoid impingement. The normal subcoracoid space—the coracohumeral interval—typically ranges from 8.4 mm to 11 mm. When this space is stenotic (less than 6 mm), the prominent coracoid tip mechanically abuts the superficial surface of the subscapularis tendon during internal rotation and forward elevation.
This mechanical abutment creates a destructive "roller-wringer effect." As the tendon glides beneath the coracoid, the indentation generates immense tensile forces on the convex, articular (under) surface of the tendon. Over time, this repetitive microtrauma leads to fiber failure, typically initiating as an articular-sided, partial-thickness tear at the superior aspect of the insertion. If left untreated, this progressive failure propagates inferiorly and medially, ultimately culminating in a massive, retracted full-thickness tear that severely compromises glenohumeral kinematics.
Detailed Surgical Anatomy and Biomechanics
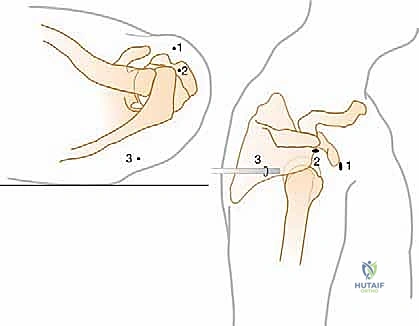
Before we make a single incision or establish a portal, a profound, three-dimensional understanding of the subscapularis muscle and tendon complex is paramount. The subscapularis is the largest, strongest, and most powerful of the rotator cuff muscles, generating roughly 50% of the total cuff force. It originates from the medial two-thirds of the anterior scapular fossa, a broad, multipennate origin that allows for its massive force generation. From this origin, the muscle belly courses laterally, passing deep to the coracoid process, before transitioning into a robust tendon that inserts onto the lesser tuberosity of the proximal humerus.
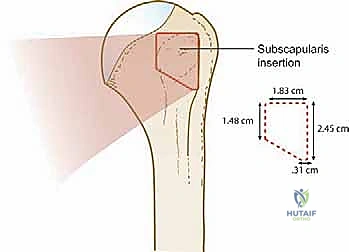
The footprint of the subscapularis on the lesser tuberosity is highly specific and clinically relevant. It forms a trapezoidal shape, approximately 2.5 to 3.0 cm in superior-to-inferior length, with its widest and thickest portion located cephalad. This insertion footprint has been famously described as resembling the shape of the state of Nevada. The superior 60% of the tendon is tendinous and robust, representing the primary site of pathology and the most critical area for surgical restoration. The inferior 40% is more muscular, inserting directly onto the humeral shaft, and is rarely involved in isolated degenerative tears.
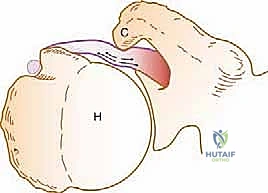
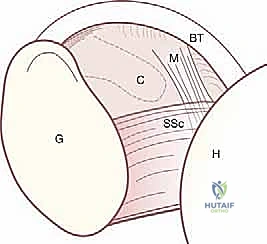
Crucially, the superior aspect of the subscapularis tendon is not an isolated structure; it is intimately confluent with the deep glenohumeral joint capsule and the medial sling of the long head of the biceps tendon. This medial sling, comprised of fibers from the superior glenohumeral ligament (SGHL) and the coracohumeral ligament (CHL), forms a dynamic pulley that stabilizes the biceps within the bicipital groove. When the superior subscapularis tears and retracts medially, it invariably pulls this sling complex with it. This anatomic linkage creates the pathognomonic arthroscopic "comma sign"—a comma-shaped arc of tissue that serves as an infallible roadmap to the retracted superolateral edge of the subscapularis tendon.


From a biomechanical standpoint, the subscapularis is the primary internal rotator and adductor of the humerus. However, its most vital role is dynamic glenohumeral stabilization. It acts as a crucial anterior restraint to humeral head translation. In concert with the posterior cuff (infraspinatus and teres minor), it establishes the transverse-plane force couple. This force couple dynamically compresses the humeral head into the glenoid concavity during motion—effectively maintaining the "golf ball on the golf tee." A torn subscapularis disrupts this delicate balance, leading to superior and anterior humeral head migration, altered arthrokinematics, and accelerated glenohumeral arthropathy.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic subscapularis repair requires a meticulous synthesis of the patient's history, specific physical examination findings, and advanced imaging. Patients typically present with anterior shoulder pain, weakness in internal rotation, and significant difficulty with activities performed in front of the body, such as lifting objects or tucking in a shirt. Unlike posterosuperior cuff tears, which primarily limit overhead function, subscapularis deficiency manifests as debilitating weakness below the shoulder level.
Physical examination is the cornerstone of diagnosis, utilizing specific provocative maneuvers to isolate the upper and lower fibers of the tendon. The Bear Hug test is the most sensitive maneuver for identifying upper-third articular-sided partial tears; it is positive if the patient cannot resist the examiner pulling their hand off the contralateral shoulder. The Napoleon test (Belly Press) evaluates the mid-to-lower fibers; an inability to maintain the wrist in a neutral or extended position while pressing the belly indicates a significant tear. Finally, the Lift-off test evaluates the entire tendon but requires the patient to achieve sufficient internal rotation to place the hand behind the back; a positive result (inability to lift the hand away from the lumbar spine) strongly correlates with a massive, complete tear.
Imaging confirms the clinical suspicion and guides preoperative templating. Standard radiographs (AP, true AP/Grashey, axillary, and outlet views) are essential to rule out fractures, assess the acromial morphology, and evaluate for anterior or superior humeral head migration. However, non-contrast Magnetic Resonance Imaging (MRI) is the gold standard. Axial T2-weighted sequences are paramount for visualizing the subscapularis tendon, assessing the degree of medial retraction, evaluating the integrity of the biceps sling, and measuring the coracohumeral interval. Furthermore, sagittal T1 sequences must be scrutinized to evaluate the Goutallier stage of fatty infiltration within the subscapularis muscle belly, as advanced atrophy significantly impacts reparability and prognosis.
| Parameter | Indications for Arthroscopic Repair | Contraindications for Arthroscopic Repair |
|---|---|---|
| Tear Characteristics | Acute traumatic tears in active patients; Symptomatic partial or full-thickness tears failing conservative management. | Massive, immobile, chronically retracted tears that cannot be mobilized to the footprint. |
| Muscle Quality | Goutallier Stage 0, 1, or 2 (Minimal to moderate fatty infiltration). | Goutallier Stage 3 or 4 (Severe fatty infiltration and irreversible muscle atrophy). |
| Patient Factors | High functional demands; compliance with strict postoperative rehabilitation protocols. | Medically unstable patients; inability to comply with postoperative restrictions; active joint infection. |
| Associated Pathology | Concomitant reparable supraspinatus/infraspinatus tears; biceps pathology requiring tenodesis. | Severe glenohumeral osteoarthritis (Hamada Grade 4/5); fixed anterior shoulder escape (pseudoparalysis). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a fluid and successful arthroscopic subscapularis repair. Prior to entering the operating room, the surgical team must review the MRI to anticipate the tear pattern (Lafosse classification), the required number of anchors, the need for a concomitant biceps tenodesis, and whether a coracoplasty will be necessary. The anesthesiologist typically administers a regional interscalene nerve block for postoperative analgesia, followed by the induction of general anesthesia with endotracheal intubation to ensure airway security during lateral positioning.
While some surgeons prefer the beach chair position, the lateral decubitus position is highly advantageous for subscapularis repair and is our preferred method. It provides superior visualization of the anterior compartment, naturally distracts the glenohumeral joint, and allows for excellent access to the inferior and medial aspects of the subscapularis. The patient is placed in the lateral position, supported by a vacuum beanbag. An axillary roll is meticulously placed in the contralateral axilla to protect the dependent brachial plexus, and all bony prominences are heavily padded.

The operative arm is placed in a sterile traction sleeve and suspended using a balanced suspension system. We typically apply 10 to 15 pounds of traction, positioning the arm in roughly 45 degrees of abduction and 20 degrees of forward flexion. Crucially, the operating table is tilted backward approximately 10 to 15 degrees. This slight reverse Trendelenburg orientation brings the glenoid face parallel to the floor, optimizing the trajectory for anterior anchor placement and improving fluid dynamics within the joint.
Portal placement must be precise to establish optimal viewing and working angles.
1. Standard Posterior Portal: Established first for initial intra-articular diagnostic viewing.
2. Anterior Mid-Glenoid Portal: Placed just superior to the upper border of the subscapularis tendon, using an outside-in spinal needle technique to ensure a perfect angle for anchor insertion into the lesser tuberosity.
3. Anterolateral Portal: Located at the anterior corner of the acromion, used for viewing the anterior compartment and managing the subdeltoid space.
4. Accessory Superolateral Portal: Often required for suture management and passing instruments.
The judicious use of a 70-degree arthroscope through the posterior portal is an absolute game-changer, allowing the surgeon to look "around the corner" of the humeral head to visualize the entire subscapularis footprint and the coracohumeral interval.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Biceps Management
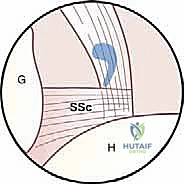
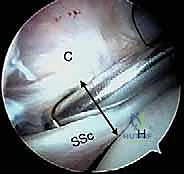
The procedure commences with a comprehensive diagnostic arthroscopy from the posterior portal. We systematically evaluate the labrum, the articular cartilage, and the entire rotator cuff. The subscapularis is inspected utilizing a 30-degree, and subsequently a 70-degree, arthroscope. We look for the "comma sign," which immediately betrays a retracted superior subscapularis tear. The long head of the biceps tendon is probed; in the setting of a subscapularis tear, the medial sling is invariably compromised, leading to biceps subluxation, instability, or intrinsic tearing.
Because the biceps tendon frequently acts as a mechanical block to subscapularis mobilization, and because an unstable biceps is a known pain generator, we almost universally perform a biceps tenotomy or tenodesis prior to addressing the subscapularis. Releasing the biceps dramatically opens the anterior interval, providing a clear, unobstructed view of the subscapularis tendon edge and the lesser tuberosity.

Coracoplasty and Subcoracoid Decompression
Once the biceps is managed, attention turns to the subcoracoid space. If preoperative imaging or intraoperative dynamic assessment (internal rotation of the arm) demonstrates a stenotic coracohumeral interval (less than 6 mm) with impingement on the subscapularis, a coracoplasty is mandatory. Failure to decompress this space will subject the new repair to the same "roller-wringer" forces that caused the initial tear, virtually guaranteeing a retear.



Viewing from the posterior or anterolateral portal, an electrocautery device is introduced through the anterior working portal to clear the soft tissue off the posterolateral aspect of the coracoid process. We then use a motorized burr to resect the prominent posterolateral tip of the coracoid, typically removing 5 to 8 mm of bone. The goal is to achieve a minimum of 7 to 8 mm of clearance between the coracoid and the subscapularis tendon during dynamic internal rotation. Strict adherence to staying lateral to the conjoint tendon is critical to avoid catastrophic injury to the musculocutaneous nerve.
Tendon Mobilization and the Three-Sided Release
Chronic, retracted subscapularis tears require extensive mobilization to achieve a tension-free repair at the anatomic footprint. This is achieved through a systematic "three-sided release."
First, the anterior release involves clearing the adhesions between the anterior surface of the subscapularis and the conjoint tendon/coracoid process.
Second, the superior release requires dividing the scarred coracohumeral ligament and the rotator interval tissue, separating the subscapularis from the supraspinatus.
Third, the posterior (intra-articular) release involves elevating the tendon off the anterior glenoid neck and releasing the middle glenohumeral ligament.





During these releases, the surgeon must be acutely aware of the neurovascular anatomy. The axillary nerve courses inferiorly, resting precariously close to the inferior border of the subscapularis. Dissection must remain superior to the inferior muscular border. Traction sutures can be placed in the comma tissue to pull the tendon laterally, assessing excursion. A properly mobilized tendon should easily reach the lesser tuberosity without undue tension when the arm is in neutral rotation.
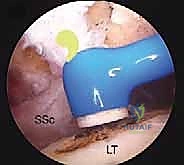
Footprint Preparation and Anchor Fixation
With the tendon mobilized, the lesser tuberosity footprint is prepared. Using a motorized shaver and a light burr, the soft tissue remnants are cleared, and the cortical bone is gently decorticated to expose a bleeding cancellous bed, optimizing the biologic environment for tendon healing. Care is taken not to over-resect the bone, which could compromise anchor purchase.



Anchor placement is executed through the anterior mid-glenoid portal. For a standard upper-third tear, a single double-loaded anchor placed at the superior aspect of the lesser tuberosity is often sufficient. For larger tears, two or three anchors may be required, placed in a superior-to-inferior cascade. The anchors must be inserted orthogonally to the bone surface to maximize pullout strength.





Suture passing is technically demanding due to the anterior and medial position of the tendon. We utilize penetrating suture passers (e.g., a tissue penetrator with a nitinol loop) to pass the sutures through the tendon in a mattress or modified Mason-Allen configuration. Grasping the "comma sign" tissue is an excellent strategy to ensure the superior, most robust portion of the tendon is captured. Once all sutures are passed, knots are tied sequentially, or knotless anchors are utilized to compress the tendon securely against the decorticated footprint.






