Mastering Open Rotator Cuff Repair: Acromioplasty, Distal Clavicle Excision, and Posterosuperior Tendon Reconstruction

Key Takeaway
This masterclass guides fellows through open rotator cuff repair, acromioplasty, and distal clavicle excision. We cover critical surgical anatomy, meticulous patient positioning, and a step-by-step intraoperative execution for massive posterosuperior tears. Learn pearls, pitfalls, and comprehensive postoperative management to optimize patient outcomes in challenging cases.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater. Today, we are undertaking a highly complex and demanding case: the reconstruction of a massive, retracted posterosuperior rotator cuff tear requiring an open surgical approach, combined with a symptomatic acromial spur and acromioclavicular (AC) joint arthropathy. Over the past two decades, arthroscopic techniques have undoubtedly become the mainstay for the vast majority of rotator cuff repairs, offering minimized soft tissue morbidity and accelerated early rehabilitation. However, understanding and mastering the open approach remains an absolute, non-negotiable requirement for the comprehensive orthopedic shoulder surgeon. For those complex, chronic tears that demand maximal visualization, robust tendinous mobilization, extensive capsular releases, and direct, tactile tissue handling, the open approach is unparalleled. This is the arena where foundational surgical principles, anatomical mastery, and meticulous technique truly shine.
The epidemiology of rotator cuff disease represents a continuum from age-related microstructural degeneration to acute, catastrophic traumatic avulsions. Rotator cuff tears are highly prevalent, with incidence increasing linearly with patient age; asymptomatic full-thickness tears are present in over 30% of patients older than 60 years. The progression from a partial-thickness articular or bursal-sided tear to a full-thickness defect, and ultimately to a massive, retracted tear, is driven by a combination of intrinsic tendon degeneration and extrinsic mechanical impingement. A "massive" tear is classically defined in the orthopedic literature as a defect measuring greater than 5 centimeters in maximum diameter or involving the complete avulsion of two or more distinct rotator cuff tendons. These massive defects present a unique biomechanical and biological challenge, as the chronic absence of tension leads to progressive muscle atrophy and irreversible fatty infiltration.
Pathophysiologically, the failure of the rotator cuff is multifactorial. Intrinsic theories point to age-related microvascular hypoperfusion, particularly within the "critical zone" of the supraspinatus tendon—an area located approximately 1 centimeter proximal to its insertion on the greater tuberosity. Extrinsic theories, popularized by Charles Neer, emphasize repetitive mechanical compression of the cuff tendons between the humeral head and the rigid coracoacromial arch during forward elevation and internal rotation. As a tear enlarges, particularly involving the supraspinatus and infraspinatus, the crucial transverse force couple is disrupted. This disruption leads to the uninhibited superior pull of the deltoid muscle, resulting in proximal migration of the humeral head, which further exacerbates subacromial impingement and accelerates the degenerative cascade, creating a vicious, self-perpetuating cycle of joint destruction.
The rationale for concomitant procedures—specifically acromioplasty and distal clavicle excision—is rooted in optimizing the mechanical environment to protect our biological repair. An anterior acromioplasty, which involves resecting the anteroinferior prominence of the acromion and releasing the coracoacromial ligament, decompresses the subacromial space. This is critical in patients with a Type III (hooked) acromion, which mechanically abrades the superior surface of the cuff. Similarly, a distal clavicle excision (the open Mumford procedure) is indicated when concurrent AC joint arthropathy presents with inferior osteophytes that directly impinge upon the underlying supraspinatus musculotendinous junction. By meticulously addressing these bony impingement lesions, we drastically reduce the mechanical sheer stresses on our newly repaired tendon constructs, thereby optimizing the biological milieu for primary healing.

Detailed Surgical Anatomy and Biomechanics
Let us begin with an exhaustive review of the surgical anatomy that underpins our understanding of this complex pathology. The rotator cuff is not merely a static group of muscles; it is a highly dynamic, intricately coordinated stabilizer and mover of the glenohumeral joint. It comprises four distinct musculotendinous units. The supraspinatus originates from the supraspinous fossa of the scapula and inserts on the superior facet of the greater tuberosity; it is primarily responsible for the initiation of abduction and superior stability. The infraspinatus originates from the infraspinous fossa and inserts on the middle facet of the greater tuberosity, acting as the primary external rotator. The teres minor originates from the lateral border of the scapula and inserts on the inferior facet, also contributing to external rotation and providing crucial restraint against superior humeral migration. Finally, the subscapularis originates from the anterior subscapular fossa and inserts on the lesser tuberosity, serving as the primary internal rotator and anterior stabilizer.
The supraspinatus, infraspinatus, and teres minor collectively form the posterosuperior cuff. Their coordinated action is fundamentally biomechanical: they do not merely rotate the humerus, but critically, they compress the humeral head into the shallow glenoid fossa. This mechanism, known as "concavity compression," creates a stable, centralized fulcrum that allows the massive, overlying deltoid muscle to efficiently elevate the arm. When a massive posterosuperior defect occurs, this suspension bridge-like cable system (as described by Burkhart) fails. The loss of concavity compression allows the deltoid's superiorly directed force vector to dominate, leading to superior humeral head migration, altered glenohumeral kinematics, and eventual cuff tear arthropathy. Overlying these tendons is the subacromial bursa, a highly innervated, fluid-filled sac that reduces friction but becomes a primary source of nociception when inflamed.
Above this entire musculotendinous complex lies the coracoacromial arch, a rigid osseoligamentous structure formed by the undersurface of the acromion, the coracoacromial (CA) ligament, the coracoid process, and the distal clavicle at the AC joint. While this arch provides necessary superior restraint against catastrophic humeral head escape, it paradoxically becomes a source of extrinsic impingement. Acromial morphology, famously classified by Bigliani, dictates impingement risk: Type I is flat, Type II is curved, and Type III is hooked. The Type III acromion, along with inferiorly projecting osteophytes from a degenerated AC joint, drastically reduces the subacromial space, directly abrading the critical zone of the supraspinatus during arm elevation.
As we dissect through the layers, we must maintain absolute vigilance regarding our critical neurovascular neighbors. The axillary nerve, a branch of the posterior cord of the brachial plexus, exits the quadrangular space and wraps around the surgical neck of the humerus. It lies approximately 5 to 7 centimeters distal to the lateral edge of the acromion, innervating the deltoid and teres minor. Excessive distal splitting of the deltoid during our approach can catastrophically jeopardize this nerve. The suprascapular nerve runs through the suprascapular notch (innervating the supraspinatus) and courses around the spinoglenoid notch (innervating the infraspinatus). While less at risk during the initial superior approach, aggressive posterior dissection or excessive lateral traction on a severely retracted, scarred tendon can place traction on this nerve, leading to iatrogenic neuropathy. The cephalic vein lies in the deltopectoral groove, and while not directly in our anterolateral field today, careful subcutaneous dissection and hemostasis are always warranted.

Exhaustive Indications and Contraindications
Defining the ideal candidate for an open rotator cuff repair versus an all-arthroscopic approach requires nuanced clinical judgment. The primary indication for an open approach is a massive, chronic, and severely retracted tear (Patte Stage 3) where the tendon edges have scarred down to the glenoid neck. In these scenarios, the surgeon must perform extensive, multidirectional soft tissue releases—including coracohumeral ligament transection, anterior interval slides, and posterior interval slides—to mobilize the tendon laterally to the anatomic footprint. The open approach provides the necessary tactile feedback and three-dimensional visualization to safely elevate the cuff off the underlying capsule and neurovascular structures. Furthermore, open repair is strongly indicated when massive tendinous defects are coupled with severe, mechanically significant bony pathology that is difficult to adequately address arthroscopically in a timely manner.
Indications for concurrent procedures must be strictly evidence-based. Symptomatic AC joint arthropathy—characterized by localized superior shoulder pain, exquisite tenderness over the AC articulation, a positive cross-body adduction test, and radiographic evidence of joint space narrowing with inferior osteophytosis—is a definitive indication for a distal clavicle excision (Mumford procedure). An anterior acromioplasty is indicated in the presence of a structurally significant Type III hooked acromion or a massive subacromial spur that is clearly abutting the superior aspect of the rotator cuff, particularly when the coracoacromial ligament is heavily thickened and contracted, contributing to anterior-superior impingement.
Conversely, we must rigorously respect the absolute and relative contraindications to open rotator cuff repair to avoid catastrophic surgical failures. Advanced physiological age coupled with low functional demands and minimal pain often warrants conservative management rather than massive open reconstruction. A critical contraindication is the presence of severe glenohumeral osteoarthritis with superior humeral head migration (cuff tear arthropathy, Hamada Grade 3 or higher). In such cases, attempting a primary tissue repair is biologically futile and biomechanically unsound; these patients are definitively better served by a Reverse Total Shoulder Arthroplasty (RTSA). Furthermore, high-grade fatty infiltration of the rotator cuff musculature (Goutallier Grade 3 or 4), as seen on preoperative MRI, indicates irreversible muscle degeneration. Even if a structural repair is achieved, the muscle lacks the contractile capacity to function, leading to inevitable re-tear and poor clinical outcomes.
Neurological and systemic contraindications must also be meticulously evaluated. Concomitant, unaddressed cervical radiculopathy (e.g., C5-C6 root compression) mimicking shoulder pain is a frequent pitfall; operating on the shoulder will not relieve neurogenic pain originating from the spine. An axillary nerve palsy resulting in profound deltoid dysfunction is an absolute contraindication for cuff repair, as the deltoid is the primary motor unit required for elevation once the cuff is stabilized. Finally, active localized or systemic infection, severe medical comorbidities precluding safe anesthesia, and documented patient non-compliance with complex postoperative rehabilitation protocols are strict contraindications to this elective, demanding procedure.
| Category | Indications for Open Repair & Adjuncts | Absolute & Relative Contraindications |
|---|---|---|
| Tear Characteristics | Massive, retracted tears (Patte Stage 3) requiring extensive mobilization; Revision repairs with poor tissue quality. | High-grade fatty infiltration (Goutallier 3/4); Irreparable tears with fixed superior humeral escape. |
| Bony Pathology | Symptomatic AC arthropathy with inferior osteophytes (requires Mumford); Type III hooked acromion with impingement (requires Acromioplasty). | Severe glenohumeral osteoarthritis / Cuff Tear Arthropathy (Hamada Grade $/ge$ 3) - indicates RTSA. |
| Neurologic Status | Intact axillary and suprascapular nerve function; Normal cervical spine exam. | Axillary nerve palsy (deltoid dysfunction); Active cervical radiculopathy mimicking shoulder pain. |
| Patient Factors | High functional demand; Compliant with prolonged rehabilitation; Medically optimized. | Advanced physiological age with low demand; Active infection; Inability to comply with complex rehab. |


Pre-Operative Planning, Templating, and Patient Positioning
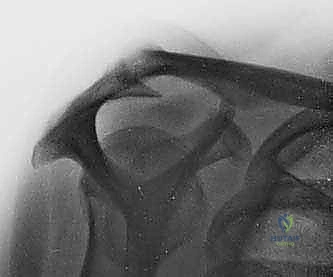
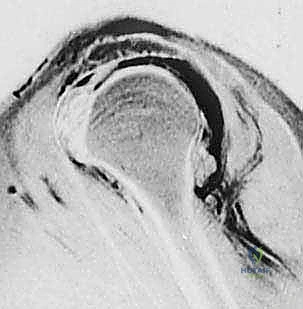
Before a single incision is made, meticulous, exhaustive preoperative planning is the cornerstone of a successful surgical outcome. Our diagnostic journey relies heavily on advanced imaging modalities. Standard radiographs are absolutely crucial and must never be bypassed. Anteroposterior (AP) views in internal and external rotation allow us to assess the glenohumeral joint space, identify cystic changes in the greater tuberosity, and evaluate inferior humeral osteophytes. The axillary view is mandatory to evaluate glenoid morphology, rule out posterior humeral head subluxation, and assess AC joint alignment. The outlet view (Scapular Y-view) is critical for assessing acromial morphology, identifying the "hooked" Type III acromion associated with impingement. We must also carefully measure the acromiohumeral interval (AHI) on a true AP (Grashey) view; an AHI of less than 7 millimeters is highly indicative of a massive rotator cuff tear with superior migration, while an AHI of less than 5 millimeters suggests advanced, potentially irreparable disease.
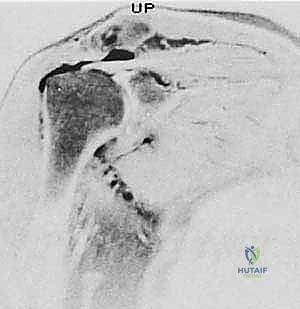
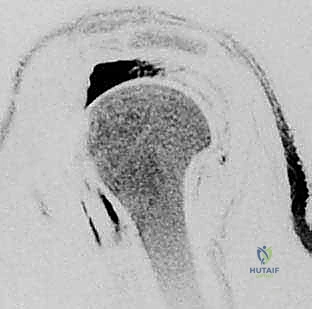
Magnetic Resonance Imaging (MRI) serves as our gold standard for soft tissue evaluation and surgical templating. It provides a comprehensive three-dimensional view of the cuff architecture. T2-weighted coronal oblique images clearly delineate the tear's medial-to-lateral extent and the degree of tendon retraction. T2-weighted sagittal oblique images are vital for understanding the anterior-to-posterior extent of the defect, specifically evaluating the involvement of the teres minor and the subscapularis. Most importantly, T1-weighted sagittal oblique images must be scrutinized to assess the degree of fatty infiltration within the muscle bellies using the Goutallier classification system. Identifying Grade 3 (equal fat and muscle) or Grade 4 (more fat than muscle) infiltration drastically alters our surgical decision-making, shifting the paradigm from primary repair toward salvage procedures or arthroplasty.
Surgical templating involves anticipating the required releases and fixation strategy based on the MRI findings. If severe retraction is noted, we must plan for a robust anterolateral approach, anticipating the need to perform an anterior interval slide (releasing the coracohumeral ligament and the interval between the supraspinatus and subscapularis) and a posterior interval slide (separating the supraspinatus from the infraspinatus). We must also evaluate the bone stock of the greater tuberosity; if significant cystic degeneration is present, we must plan for specialized fixation techniques, such as utilizing larger diameter anchors, cortical fixation devices, or a transosseous-equivalent double-row construct to maximize footprint compression and prevent anchor pull-out in osteoporotic bone.
Patient positioning is a critical, often underappreciated step that dictates the flow of the entire operation. For an open rotator cuff repair, we strongly favor the modified beach chair (or sitting) position. The patient is placed on a specialized shoulder chair with the backrest elevated to approximately 70 to 80 degrees. This upright orientation utilizes gravity to pull the arm inferiorly, naturally opening the subacromial space. Ensure meticulous padding at all pressure points—specifically the sacrum, heels, and the posterior aspect of the head. The head must be secured in a well-padded, specialized headrest, slightly flexed and rotated away from the operative shoulder to maximize access to the superior aspect of the joint. The operative arm must be draped entirely free. This is paramount, fellows; it allows the surgeon uninhibited mobility of the extremity throughout the case to dynamically assess tendon tension, facilitate mobilization, and test the integrity of the final repair construct.



Step-by-Step Surgical Approach and Fixation Technique
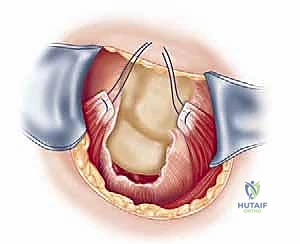
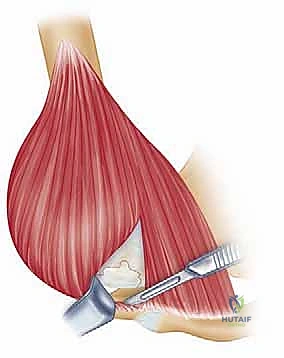
The surgical approach begins with a meticulously planned anterolateral incision, typically utilizing Langer's lines for optimal cosmesis. The incision extends approximately 4 to 5 centimeters distally from the anterolateral tip of the acromion. Following sharp dissection through the skin and subcutaneous tissues, we identify the raphe separating the anterior and middle thirds of the deltoid muscle. We perform a longitudinal split of the deltoid precisely along this avascular raphe. It is a strict, inviolable rule that this split must not extend further than 5 centimeters distal to the lateral edge of the acromion to absolutely protect the axillary nerve, which traverses transversely on the undersurface of the muscle. A heavy stay suture (e.g., #1 Vicryl) is placed at the distal apex of the split to prevent inadvertent propagation of the dissection during forceful retraction.
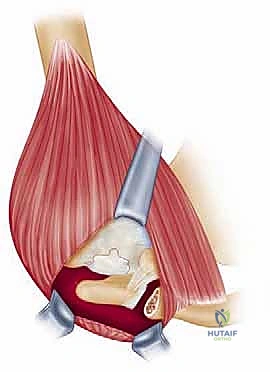
Once the subacromial space is entered, a thorough subacromial bursectomy is mandatory. The hypertrophied, inflamed bursa is excised using electrocautery and rongeurs to expose the underlying rotator cuff and the coracoacromial arch. We then direct our attention to the acromioplasty. The coracoacromial ligament is identified and released from its attachment on the anteroinferior aspect of the acromion. Using an oscillating saw or a motorized cutting burr, an anterior acromioplasty is performed. The goal is to resect the anterior prominence and the inferior surface of the anterior third of the acromion, effectively converting a curved or hooked acromion into a flat, Type I morphology. If a distal clavicle excision is indicated, the dissection is carried medially over the AC joint. The capsule is incised longitudinally, and approximately 8 to 10 millimeters of the distal clavicle is resected using an oscillating saw, taking supreme care to preserve the superior and posterior AC capsular ligaments to prevent iatrogenic horizontal instability of the clavicle.
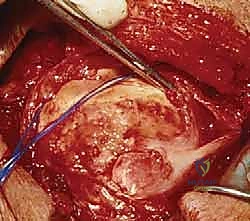
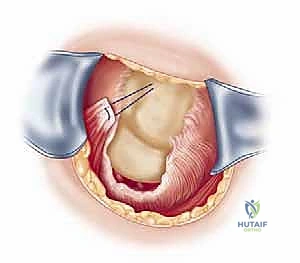
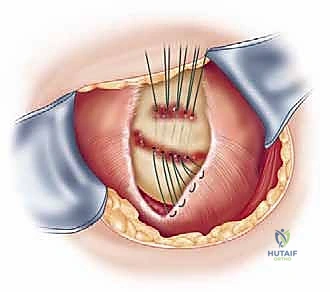
Attention is then turned to the rotator cuff defect. The retracted edges of the supraspinatus and infraspinatus are identified, grasped with Allis clamps, and tagged with heavy traction sutures (e.g., #2 FiberWire). Extensive mobilization is almost always required for massive tears. We perform a systematic release: first, an intra-articular release of the capsule from the undersurface of the tendons; second, an extra-articular release of the coracohumeral ligament; and third, if tension remains high, anterior and posterior interval slides. The goal is to achieve a tension-free excursion of the tendon edge to the lateral aspect of the greater tuberosity footprint with the arm in neutral rotation and 20 degrees of abduction.
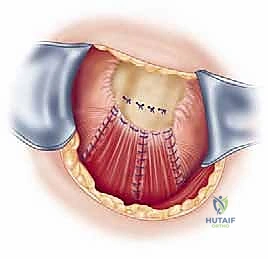
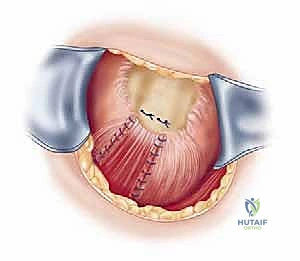
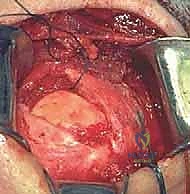
Footprint preparation and fixation are the final, critical steps. The greater tuberosity footprint is meticulously decorticated using a high-speed burr or curette to expose a bleeding, cancellous bone bed, optimizing the biological environment for tendon-to-bone healing. For a massive tear, we typically utilize a transosseous-equivalent double-row construct. Medial row anchors (typically 4.5mm or 5.5mm fully threaded titanium or PEEK anchors) are placed precisely at the articular margin. The sutures are passed through the tendon using a specialized suture-passing instrument, utilizing horizontal mattress or modified Mason-Allen configurations to maximize tissue grip. The medial row is tied, securing the tendon to the medial footprint. The suture tails are then brought laterally, crisscrossed over the tendon surface to create a pressurized footprint, and secured with lateral row knotless anchors placed 1 to 2 centimeters lateral to the medial row. The repair is dynamically tested under direct visualization by taking the arm through a full range of motion. Meticulous closure is paramount, particularly the robust, watertight repair of the deltoid fascia using non-absorbable sutures to prevent catastrophic postoperative dehiscence.



Complications, Incidence Rates, and Salvage Management
The open approach to massive rotator cuff tears, while powerful, carries a distinct and serious complication profile that the orthopedic surgeon must be prepared to manage. The most devastating, approach-specific complication is postoperative
Clinical & Radiographic Imaging Archive