Supramalleolar Opening-Wedge Osteotomy for Varus Ankle Osteoarthritis: A Masterclass

Key Takeaway
This masterclass details supramalleolar opening-wedge osteotomy for varus ankle osteoarthritis. We cover patient selection, preoperative planning, meticulous surgical technique, and postoperative care. Fellows will gain a comprehensive understanding of correcting varus and anterior opening deformities, emphasizing anatomical precision, hardware application, and complication avoidance for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The paradigm of managing ankle osteoarthritis has shifted dramatically over the past two decades. Historically, ankle arthrodesis was considered the gold standard for end-stage disease, while total ankle arthroplasty (TAA) emerged as an alternative for older, lower-demand patients. However, for the younger, active patient presenting with asymmetric, malalignment-driven osteoarthritis, joint-sacrificing procedures are suboptimal. Enter the supramalleolar osteotomy (SMOT), frequently referred to in the literature as the low tibial osteotomy (LTO). This joint-preserving procedure is a masterclass in applied biomechanics, designed to realign the mechanical axis of the lower extremity, redistribute articular contact stresses, and facilitate the biological regeneration of the intra-articular environment.
Varus-type osteoarthritis of the ankle is a progressive, debilitating condition characterized by a varus deformity of the distal tibia combined with an anterior opening of the articular surface. Epidemiologically, this pathology presents with a distinct demographic predilection, manifesting predominantly in middle-aged and elderly women, and frequently occurs bilaterally. The etiology is often insidious, linked to subtle constitutional varus alignment of the lower extremity, chronic lateral ligamentous instability, or a combination thereof, which gradually overloads the medial compartment of the tibiotalar joint.
To standardize diagnosis and guide surgical decision-making, we rely on the Takakura classification, later modified by Tanaka, which delineates the progressive stages of varus ankle osteoarthritis based on weight-bearing radiographic findings:
* Stage 1: The joint space remains preserved with no measurable narrowing. However, early subchondral sclerosis and nascent osteophyte formation are evident, typically localized to the medial gutter and the anteromedial corner of the tibial plafond.
* Stage 2: This stage is characterized by definitive, measurable narrowing of the medial joint space. The lateral joint space remains preserved, indicating an asymmetric loading pattern.
* Stage 3: Progressive medial joint space collapse leads to complete obliteration, resulting in subchondral bone-on-bone contact medially.
* Stage 3a: The obliteration and subchondral contact are anatomically restricted to the facet of the medial malleolus and the medial border of the talar dome.
* Stage 3b: The obliteration has advanced centrally, extending to the roof (superior articular surface) of the talar dome.
* Stage 4: The terminal stage of the disease, representing complete, global obliteration of the entire tibiotalar joint space with extensive subchondral cyst formation, severe sclerosis, and rigid deformity.

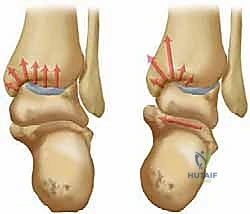
Stages of varus-type osteoarthritis of the ankle, demonstrating the progressive medial joint space collapse characteristic of the Takakura-Tanaka classification.
The fundamental biomechanical catastrophe in varus-type osteoarthritis is the exponential concentration of stress on the medial side of the ankle. This is directly driven by a varus tilt of the distal joint surface of the tibia relative to the mechanical axis of the tibia. This imbalance initiates a vicious cycle: eccentric loading causes focal cartilage degradation in the anteromedial corner, which further increases the varus deformity, subsequently driving the degenerative cascade laterally across the talar dome. The primary objective of the supramalleolar opening-wedge osteotomy is to surgically interrupt this cycle. By correcting the extra-articular deformity, we shift the mechanical axis laterally, unloading the compromised medial compartment and creating a mechanical environment conducive to the repair of chondral defects via fibrocartilaginous metaplasia.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the ankle joint is non-negotiable for the orthopedic surgeon attempting a supramalleolar osteotomy. The tibiotalar joint is a highly congruent, inherently stable hinge joint. Unlike the knee, which relies heavily on menisci and robust ligamentous complexes for stability, the ankle derives its stability from the osseous architecture of the mortise and the intricate balance of the syndesmotic and collateral ligaments. The articular cartilage of the ankle is uniquely thin—averaging only 1.0 to 1.7 mm—yet it possesses a higher proteoglycan content and greater compressive stiffness than knee cartilage. This makes the ankle highly resistant to physiological axial loads but exquisitely vulnerable to shear forces generated by angular malalignment.
In the setting of a varus distal tibia, the center of rotation of angulation (CORA) is typically located at or just proximal to the tibiotalar joint line. This malalignment shifts the ground reaction force vector medially during the stance phase of gait, creating a "varus thrust." The deltoid ligament complex, particularly the deep components, becomes chronically contracted, while the lateral collateral ligaments (anterior talofibular, calcaneofibular) are subjected to chronic attenuation.

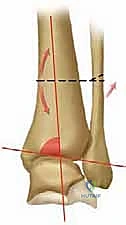
Varus-type osteoarthritis is characterized by varus tilt of the distal joint surface, shifting the mechanical axis and concentrating stress on the medial articular facet.
When performing the supramalleolar opening-wedge osteotomy, the surgeon must manipulate the distal tibial anatomy with extreme precision. The osteotomy is typically planned 2 to 3 centimeters proximal to the articular surface to ensure adequate cancellous bone for rapid healing while leaving a sufficient distal segment for robust hardware fixation. The anteromedial approach exploits the internervous and intervascular planes, but vigilance is required to protect the great saphenous vein and the saphenous nerve, which course directly over the medial malleolus. Furthermore, the integrity of the lateral tibial cortex is paramount; it must be preserved as a living plastic hinge. If this hinge is violated, the inherent stability of the osteotomy is lost, significantly increasing the risk of delayed union, nonunion, or catastrophic intra-articular extension of the fracture line.
Biomechanically, the osteotomy is not merely a coronal plane correction. Varus osteoarthritis frequently presents with an associated recurvatum deformity or an anterior opening of the distal tibial articular surface. Therefore, the supramalleolar osteotomy must often be biplanar. By creating an anteromedial opening wedge—where the wedge is slightly wider anteriorly than medially—the surgeon simultaneously corrects the varus tilt and the anterior opening, restoring the native sagittal tilt of the tibial plafond and optimizing the contact area of the talus within the mortise.
Exhaustive Indications and Contraindications
Patient selection is the most critical determinant of success in supramalleolar osteotomy. The procedure is technically demanding, and applying it to the wrong patient profile will inevitably lead to early failure and the need for salvage arthrodesis or arthroplasty. The ideal candidate is a physiologically young, active patient presenting with Takakura Stage 2 or Stage 3a varus ankle osteoarthritis. In these stages, the lateral compartment cartilage is preserved, and the medial joint space collapse is reversible once the mechanical axis is realigned.
Patients typically present with deep, aching ankle pain that is exacerbated by the initiation of gait and prolonged ambulation. As the disease advances, swelling and mechanical catching may occur. On physical examination, point tenderness is reliably elicited along the medial joint line and the medial gutter. Crucially, preoperative ankle range of motion must be functional. A stiff ankle with less than 10 degrees of dorsiflexion and 25 degrees of plantarflexion is a poor candidate for joint preservation, as the osteotomy relies on dynamic joint excursion to stimulate fibrocartilage regeneration.
Before committing to surgical intervention, a rigorous differential diagnosis must be entertained to rule out systemic or non-mechanical causes of ankle pain and varus deformity. Posttraumatic osteoarthritis (e.g., malunited pilon or ankle fractures) may require more complex intra-articular osteotomies. Rheumatoid arthritis, infectious arthritis, Charcot neuroarthropathy, and crystal-induced arthropathies (gout, pseudogout) represent distinct pathophysiological entities where a simple realignment osteotomy is either contraindicated or highly likely to fail.
Indication and Contraindication Matrix
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Ideal Indications | Takakura Stage 2 or 3a Varus OA | Lateral cartilage is preserved; medial collapse is reversible via realignment. |
| Ideal Indications | Age < 65 years (Physiological) | Higher biological potential for fibrocartilage regeneration and bone healing. |
| Ideal Indications | Functional Range of Motion | Preserved ROM is necessary for postoperative joint mechanics and cartilage nutrition. |
| Relative Contraindications | Takakura Stage 3b | Central talar dome cartilage is compromised; outcomes are significantly less predictable. |
| Relative Contraindications | Talar Tilt Angle > 10 degrees | Severe ligamentous incompetence or talar deformity makes achieving a congruent mortise difficult. |
| Absolute Contraindications | Takakura Stage 4 (Global OA) | Complete loss of articular cartilage; requires arthrodesis or total ankle arthroplasty. |
| Absolute Contraindications | Active Infection or Charcot Joint | High risk of catastrophic failure, nonunion, and hardware infection. |
| Absolute Contraindications | Severe Osteoporosis | Inability of the bone to support structural graft and rigid plate fixation. |
Pre-Operative Planning, Templating, and Patient Positioning
The foundation of a successful supramalleolar osteotomy is laid long before the first incision, beginning with a comprehensive trial of nonoperative management and culminating in meticulous radiographic templating. Nonoperative strategies are particularly effective for Stage 1 and early Stage 2 disease. Activity modification, targeted physical therapy emphasizing peroneal strengthening, and pharmacologic interventions (NSAIDs, intra-articular hyaluronic acid) form the first line of defense.
Orthotic management is a cornerstone of conservative care. A custom-molded rigid ankle-foot orthosis or a well-designed shoe insert featuring a lateral (outer) wedge and a medial flare can significantly alter the ground reaction force vector. By shifting the center of pressure laterally, these orthotics offload the medial compartment, providing substantial symptomatic relief and potentially slowing disease progression.



Examples of conservative management: A shoe insert with an outer wedge designed to offload the medial compartment. A. Lateral view. B. Posterior view.
When conservative measures are exhausted, surgical planning begins with high-quality, weight-bearing radiographs. A standard ankle series is insufficient; full-length weight-bearing tibial and hindfoot alignment views are mandatory to assess the entire mechanical axis. The surgeon must meticulously measure two critical angles to dictate the geometry of the osteotomy:
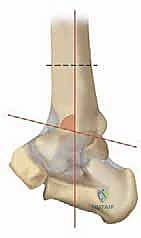
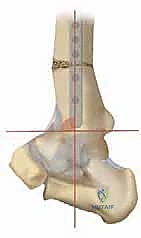
- TAS angle (Tibial Ankle Surface angle): Measured on the weight-bearing AP radiograph, this is the angle between the longitudinal anatomical axis of the tibial shaft and the distal articular surface of the tibia. Normal values range from 88 to 90 degrees. In varus osteoarthritis, this angle is significantly decreased.
- TLS angle (Tibial Lateral Surface angle): Measured on the weight-bearing lateral radiograph, this is the angle between the longitudinal axis of the tibia and the distal articular surface. Normal values are typically 80 to 81 degrees. An altered TLS angle indicates a sagittal plane deformity (anterior or posterior opening) that must be addressed simultaneously.




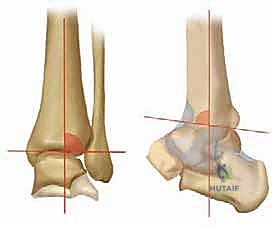
Comprehensive radiographic evaluation: The angle between the tibial shaft and the distal joint surface of the tibia on the AP view (TAS angle) and on the lateral view (TLS angle) must be precisely calculated.
Digital Templating and Wedge Calculation
Modern preoperative planning relies on digital templating software. The goal is to design an anteromedial opening-wedge osteotomy. The open-wedge technique is overwhelmingly preferred over a lateral closing-wedge osteotomy. A closing-wedge technique requires a concomitant fibular osteotomy, shortens the limb, and can slacken the lateral ligamentous complex and peroneal tendons, exacerbating lateral instability.
Using the preoperative TAS angle, the surgeon calculates the required degree of coronal correction to achieve a postoperative TAS of 90 to 92 degrees (slight overcorrection is often targeted to ensure medial unloading). The width of the wedge base is calculated geometrically based on the width of the distal tibia at the planned osteotomy site. If a sagittal plane correction is required (to correct an anterior opening), the anterior cortex must be opened wider than the medial cortex, creating a trapezoidal wedge.
Preoperative digital templating is utilized to calculate the exact dimensions of the anteromedial opening wedge required to restore the TAS and TLS angles.
Patient positioning is critical for intraoperative success. The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg until the patella points directly toward the ceiling, neutralizing the natural external tibial torsion and allowing for true AP and lateral fluoroscopic views. A sterile tourniquet is applied to the proximal thigh, and the iliac crest is prepped and draped if autologous structural bone grafting is planned.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the supramalleolar opening-wedge osteotomy demands meticulous soft tissue handling and precise osseous manipulation. The procedure begins with a 6 to 8-centimeter longitudinal incision centered over the anteromedial aspect of the distal tibia, starting just proximal to the tip of the medial malleolus and extending proximally. Dissection is carried sharply through the subcutaneous tissue. The great saphenous vein and the saphenous nerve are carefully identified, mobilized, and protected with a vessel loop, typically retracted anteriorly.
The periosteum is incised longitudinally and elevated meticulously to expose the anteromedial, medial, and anterior surfaces of the distal tibia. Extensive periosteal stripping should be avoided to preserve the osteogenic potential of the bone. Under direct fluoroscopic guidance, a smooth Kirschner wire (K-wire) or a specialized guide pin is advanced from medial to lateral. The starting point is typically 2.5 to 3.0 centimeters proximal to the medial tibiotalar joint line. The trajectory of the pin must be perfectly parallel to the distal tibial articular surface in the coronal plane. Crucially, the pin must stop 5 to 8 millimeters short of the lateral tibial cortex to mark the boundary of the lateral hinge.

Intraoperative fluoroscopy confirming the correct trajectory of the guide pin, parallel to the joint line and preserving the lateral cortical hinge.
Osteotomy Execution and Wedge Opening
Once the guide pin is verified in both AP and lateral planes, the osteotomy is initiated using an oscillating saw. The saw blade is placed immediately proximal to the guide pin. Copious cold saline irrigation is mandatory during sawing to prevent thermal necrosis of the bone, which can catastrophicly delay healing. The surgeon must maintain a steady hand, ensuring the cut remains strictly parallel to the pin. The anterior and medial cortices are completely transected. The posterior cortex is often the most challenging; it must be cut carefully to avoid plunging into the posterior neurovascular bundle. The saw is stopped precisely at the depth of the guide pin, preserving the lateral 5 to 8 millimeters of the intact lateral cortex.
The opening of the wedge is the most delicate phase of the operation. Broad, flat osteotomes are sequentially inserted into the osteotomy site. The surgeon must open the wedge gradually, allowing the viscoelastic properties of the lateral cortical hinge to accommodate the deformation without fracturing. Laminar spreaders can be utilized to maintain the opening. The gap is opened until the pre-calculated wedge width is achieved. Intraoperative fluoroscopy is then used to verify the correction of the TAS and TLS angles and to ensure the mechanical axis has shifted laterally.


Gradual opening of the osteotomy site using laminar spreaders and osteotomes, ensuring the lateral hinge remains intact.
Grafting and Rigid Internal Fixation
With the desired correction achieved, the resulting void must be filled with a structural bone graft. Autologous tricortical iliac crest bone graft remains the gold standard due to its unmatched osteoconductive, osteoinductive, and osteogenic properties. However, structural allografts (e.g., femoral head or fibular wedges) or advanced synthetic porous titanium or tricalcium phosphate wedges are increasingly utilized to avoid donor site morbidity. The graft is meticulously fashioned to match the dimensions of the defect and gently impacted into place.
Rigid internal fixation is paramount to maintain the correction and facilitate early rehabilitation. An anatomically contoured, low-profile anteromedial locking plate is the implant of choice. The plate is positioned to bridge the osteotomy, and locking screws are placed distally into the epiphyseal/metaphyseal bone and proximally into the tibial diaphysis. The locking mechanism provides fixed-angle stability, which is essential in the metaphyseal bone of the distal tibia, particularly in older patients with compromised bone density.


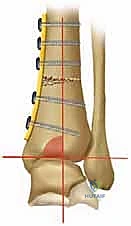
Application of an anatomically contoured anteromedial locking plate. The structural graft is visible within the osteotomy void, providing mechanical support and a biological scaffold.
Following fixation, final fluoroscopic images are obtained to confirm hardware placement, graft position, and overall alignment. The wound is irrigated, and the periosteum and subcutaneous tissues are closed in layers. A meticulous skin closure is critical, as the anteromedial soft tissue envelope is notoriously thin and prone to breakdown.
Clinical & Radiographic Imaging Archive