
Welcome to the operating theater and to this definitive masterclass on anterior shoulder reconstruction. Today, we are tackling a complex, multifaceted, and historically overlooked pathology: the subscapularis tear, frequently accompanied by long head of the biceps (LHB) pathology and subcoracoid impingement. This procedure—combining subscapularis repair, coracoid recession (coracoplasty), and biceps tenodesis—demands meticulous attention to detail, a profound understanding of shoulder biomechanics, and precise spatial awareness of anterior shoulder anatomy. What follows is a comprehensive, textbook-level exploration of the patho-epidemiology, surgical anatomy, operative execution, and postoperative management required to master this challenging clinical scenario.
Comprehensive Introduction and Patho-Epidemiology
Historically referred to as the "forgotten tendon" of the rotator cuff, the subscapularis is now recognized as the critical anterior force couple of the glenohumeral joint. A thorough understanding of the underlying pathology is paramount before any surgical intervention is considered. Subscapularis tears, while historically reported as less common than supraspinatus or infraspinatus tears, are increasingly recognized due to advanced imaging and improved arthroscopic diagnostic techniques. They occur in approximately 2% to 8% of all rotator cuff tears, though autopsy and advanced MRI studies suggest the true prevalence of partial-thickness tears may be significantly higher.
The impact of a subscapularis deficiency on shoulder stability and kinematics is profound. As the largest and strongest of the rotator cuff muscles, it provides over 50% of the cuff's total cross-sectional area and is primarily responsible for internal rotation. More importantly, it acts as a dynamic anterior stabilizer, resisting anterior and inferior translation of the humeral head. When the subscapularis fails, the glenohumeral joint loses its anterior restraint, leading to altered kinematics, accelerated wear of the long head of the biceps, and secondary impingement syndromes.

Subcoracoid impingement is frequently implicated in the pathogenesis of subscapularis tears. This condition occurs when the coracohumeral distance is pathologically narrowed (typically less than 6 mm), causing the lesser tuberosity and the subscapularis tendon to abut against the posterolateral aspect of the coracoid process during forward elevation and internal rotation. This repetitive mechanical abrasion leads to a predictable cascade: bursal-sided fraying of the subscapularis, progressive tendinopathy, and eventual structural failure. This impingement can be idiopathic, post-traumatic, or iatrogenic following previous anterior shoulder surgery.

The Long Head of the Biceps (LHB) tendon is a highly frequent companion to subscapularis pathology. Because the superior fibers of the subscapularis form the medial wall of the bicipital groove and contribute to the biceps reflection pulley, a tear in this region inevitably destabilizes the LHB. Pathologies include severe tenosynovitis, subluxation, and frank dislocation. Medial subluxation of the LHB over the lesser tuberosity is considered pathognomonic for a superior subscapularis tear. Degenerative tears are common in older patients, while acute traumatic tears—often resulting from forced external rotation of an adducted arm or hyperextension—are typical in younger, athletic populations.
Detailed Surgical Anatomy and Biomechanics
A precise anatomical roadmap is the orthopedic surgeon's most critical tool in the operating room. Mastery of the anterior shoulder anatomy is non-negotiable when navigating the deltopectoral interval and performing extensive capsular releases.
Neurovascular Structures
The neurovascular anatomy of the anterior shoulder dictates our safe zones for dissection and retraction. The subscapularis muscle is innervated by the upper and lower subscapular nerves (C5–C8), branching from the posterior cord of the brachial plexus. These nerves course along the anterior surface of the muscle belly. The upper subscapular nerve typically innervates the superior portion, while the lower subscapular nerve innervates the inferior portion. During mobilization of a chronically retracted subscapularis, extreme caution must be exercised; excessive traction or blind dissection along the anterior muscle belly can lead to devastating iatrogenic denervation.
The musculocutaneous nerve (C5-C6) is another critical structure at risk. It innervates the biceps and brachialis muscles, typically entering the coracobrachialis muscle 5 to 8 cm distal to the tip of the coracoid process. During the deltopectoral approach, this nerve is highly vulnerable when retracting the conjoined tendon medially. Prolonged or heavy-handed retraction using rigid instruments can cause a traction neuropraxia. Furthermore, the axillary nerve (C5-C6) wraps around the surgical neck of the humerus, running closely with the posterior circumflex humeral artery. It is primarily at risk during inferior capsular releases at the 6 o'clock position of the glenoid. Finally, the cephalic vein, running in the deltopectoral groove, serves as our primary superficial landmark and must be carefully preserved or formally ligated to prevent obscuring hemorrhage.
Muscular and Ligamentous Anatomy
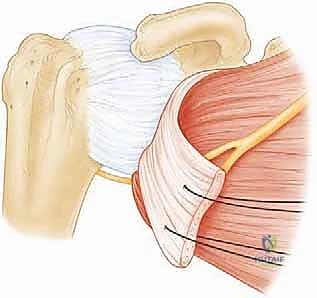
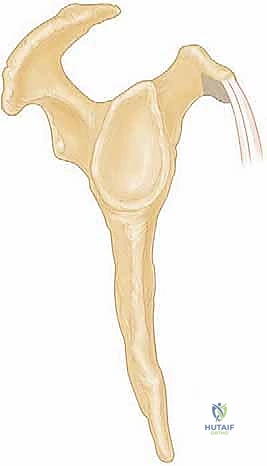
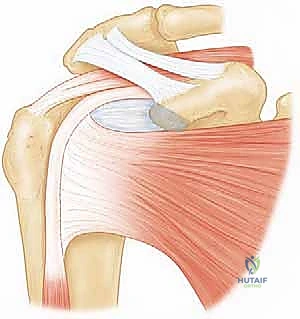
The subscapularis muscle originates from the broad subscapular fossa of the scapula. Its tendinous insertion is unique: the upper two-thirds insert as a distinct tendon onto the lesser tuberosity, while the inferior third inserts directly onto the humeral metaphysis as a muscular attachment. The superior border of the subscapularis intimately blends with the anterior fibers of the supraspinatus and the coracohumeral ligament (CHL) to form the rotator interval. This complex three-dimensional structure is bounded superiorly by the supraspinatus, inferiorly by the subscapularis, and medially by the coracoid process.
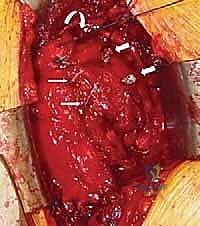
The biceps reflection pulley is a crucial anatomical sling that stabilizes the LHB at the proximal entrance of the bicipital groove. It is composed of the superior glenohumeral ligament (SGHL), the CHL, and the most superior fibers of the subscapularis tendon. When the subscapularis tears and retracts, it often takes the SGHL and CHL with it, creating a distinct anatomical landmark known as the "comma sign." Identifying this comma-shaped arc of tissue is essential for locating the superolateral corner of a retracted subscapularis tendon during surgical exploration.
Osteology and the Footprint
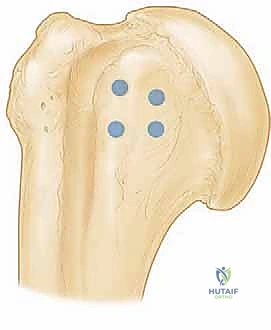
The lesser tuberosity is the primary insertion site for the subscapularis tendon and represents the critical footprint that must be restored. The footprint is broad and trapezoidal, measuring approximately 25 mm in superior-inferior length and 18 mm in medial-lateral width. Preparing this bony bed to a bleeding, decorticated surface is vital for optimal tendon-to-bone healing. The bicipital groove lies immediately lateral to the lesser tuberosity, housing the LHB. Its morphology must be assessed, as a shallow groove or osteophytic spurs can contribute to biceps instability. Finally, the coracoid process projects anteriorly and laterally; its posterolateral prominence is the primary culprit in subcoracoid impingement and is the target for our coracoid recession.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful outcomes in complex anterior shoulder reconstruction. The decision to proceed with a combined subscapularis repair, coracoplasty, and biceps tenodesis must be based on a synthesis of clinical symptoms, physical examination findings, and advanced imaging.
Surgical intervention is highly indicated for acute, traumatic subscapularis tears in active patients, as early repair prevents rapid muscle atrophy and fatty infiltration, which occur more aggressively in the subscapularis than in other rotator cuff muscles. Chronic, symptomatic tears that have failed a dedicated course of conservative management (including physical therapy focusing on periscapular stabilization and compensatory cuff strengthening) are also prime indications. The addition of a coracoid recession is indicated when preoperative imaging demonstrates a coracohumeral interval of less than 6 mm, or when intraoperative dynamic evaluation reveals frank impingement of the repaired tendon against the coracoid during internal rotation. Biceps tenodesis is indicated for almost all cases of complete subscapularis tears due to the inherent destruction of the biceps pulley, as well as in cases of severe LHB tenosynovitis, partial tearing (>25%), or subluxation.
Contraindications must be strictly respected to avoid catastrophic surgical failures. Advanced fatty infiltration of the subscapularis muscle (Goutallier Grade 3 or 4) is a strong relative, if not absolute, contraindication to primary repair, as the muscle has lost its contractile capability and the tendon tissue is often poor, leading to high re-tear rates. Fixed anterior-superior humeral escape, indicating a massive, irreparable anterosuperior cuff tear with loss of the coracoacromial arch, is another contraindication. Furthermore, advanced glenohumeral osteoarthritis (Hamada Grade 4 or 5) precludes isolated soft tissue repair; these patients are better served by arthroplasty options, such as a reverse total shoulder arthroplasty.
| Indication Category | Specific Clinical Scenarios | Contraindications |
|---|---|---|
| Acute Trauma | Traumatic avulsion in active patients; forced external rotation injuries; associated lesser tuberosity fractures. | Active systemic infection; severe medical comorbidities precluding anesthesia. |
| Chronic Pathology | Failure of >3 months conservative care; persistent pain and internal rotation weakness; positive belly-press/lift-off tests. | Advanced fatty infiltration (Goutallier Grade 3 or 4); fixed glenohumeral stiffness (frozen shoulder) requiring prior release. |
| Concomitant Lesions | LHB subluxation/dislocation (requires tenodesis); coracohumeral interval < 6mm (requires coracoplasty). | Severe glenohumeral arthritis (Hamada 4/5); irreparable massive cuff tears with anterosuperior escape (consider RTSA). |
| Revision Surgery | Failed prior arthroscopic repair with intact muscle belly; persistent subcoracoid impingement. | Deltoid paralysis (axillary nerve palsy); active local joint infection (Propionibacterium acnes). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning ensures a smooth, predictable surgical course and minimizes intraoperative surprises. This begins with a meticulous review of the patient's clinical examination and advanced imaging studies.
Advanced Imaging Review
Magnetic Resonance Imaging (MRI) or MR Arthrography is the gold standard for evaluating subscapularis pathology. We systematically assess axial, coronal, and sagittal sequences. Axial cuts are critical for evaluating the coracohumeral distance, identifying medial subluxation of the LHB, and assessing the degree of subscapularis tendon retraction. Sagittal Y-views are utilized to evaluate the muscle belly for fatty degeneration using the Goutallier classification, which directly correlates with tendon quality and postoperative healing potential. Coronal views help identify associated supraspinatus tears and superior labral pathology. Plain radiographs (True AP, Scapular Y, and Axillary views) are mandatory to rule out chronic bony changes, lesser tuberosity avulsion fractures, and anterior subluxation of the humeral head.
Examination Under Anesthesia (EUA)
Performed immediately prior to skin preparation, the EUA is a critical diagnostic adjunct. We assess for multi-directional instability, noting any abnormal anterior, posterior, or inferior translation. A key indicator of a complete subscapularis rupture is significantly increased passive external rotation compared to the contralateral shoulder, as the primary internal rotation restraint has been lost. We also carefully document the baseline Range of Motion (ROM) to differentiate a true mechanical block from pain-inhibited motion, which will guide our intraoperative capsular release and postoperative rehabilitation protocols.
Patient Positioning
For an open or mini-open subscapularis repair, the low beach chair position is preferred, offering excellent anterior exposure, anatomical orientation, and ergonomic advantages for the surgical team. The patient is positioned on a standard operating table articulated into a beach chair configuration, with the torso elevated to approximately 60 degrees and knees flexed to prevent distal sliding.

The head must be securely supported in a neutral position using a dedicated headrest to prevent cervical hyperextension, lateral flexion, or rotation, which can cause devastating brachial plexus traction injuries. The affected arm is draped free, allowing full manipulation throughout the case. We utilize a mechanical arm holder (e.g., McConnell or Spider arm positioner) to maintain various arm positions—such as internal rotation and varying degrees of abduction—without causing fatigue to the surgical assistant. Meticulous padding of all pressure points, including the occiput, elbows, heels, and sacrum, is critical to prevent peripheral nerve palsies and skin breakdown.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped and draped, we proceed with the surgical execution. This requires a systematic, layered approach, respecting the neurovascular boundaries while achieving adequate exposure for a tension-free repair.
1. The Deltopectoral Approach
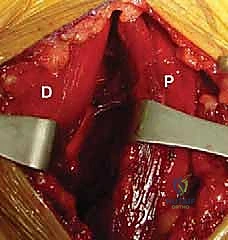
A curvilinear incision is made starting just proximal to the coracoid process, extending distally 8 to 10 cm toward the deltoid tuberosity, following Langer's lines. The subcutaneous tissue is divided using electrocautery. We identify the deltopectoral interval, marked by the cephalic vein and the distinct fascial plane between the laterally running deltoid fibers and the medially running pectoralis major fibers.
The cephalic vein is typically retracted laterally with the deltoid to preserve its major venous tributaries, though medial retraction is acceptable if the anatomy dictates. Self-retaining retractors are placed to maintain the interval, exposing the underlying clavipectoral fascia.
2. Deep Exposure and Subscapularis Mobilization
The clavipectoral fascia is divided lateral to the conjoined tendon. A broad, blunt retractor (such as a Richardson or a Kolbel) is placed medially to retract the conjoined tendon. Surgeon's Note: Extreme care must be taken here to avoid excessive medial traction, which places the musculocutaneous nerve at high risk of neuropraxia.
The subscapularis tendon is often found retracted medially beneath the coracoid process. If the tendon cannot be easily reduced to the lesser tuberosity, a systematic 360-degree release is mandatory. We begin with a superior release, dividing the rotator interval and the coracohumeral ligament to free the superior border. Next, an anterior release is performed, separating the subscapularis muscle belly from the overlying coracoid and conjoined tendon fascia.
An inferior release involves carefully detaching the inferior capsule from the subscapularis, staying strictly on the tendon to avoid the axillary nerve. Finally, a posterior capsular release (separating the tendon from the underlying anterior glenohumeral capsule) provides maximum lateral excursion.
3. Coracoid Recession (Coracoplasty)
Once the subscapularis is mobilized, we assess the subcoracoid space. If impingement is evident or the coracohumeral interval was narrow preoperatively, a coracoplasty is performed. Using a motorized burr or a sharp osteotome, the posterolateral 5 to 8 mm of the coracoid process is resected.
This resection must be beveled to create a smooth, concave surface that accommodates the lesser tuberosity during internal rotation. Care is taken not to compromise the origin of the conjoined tendon or the coracoclavicular ligaments superiorly. Bleeding from the cancellous bone of the coracoid is controlled with bone wax or electrocautery.
4. Biceps Tenodesis and Subscapularis Repair
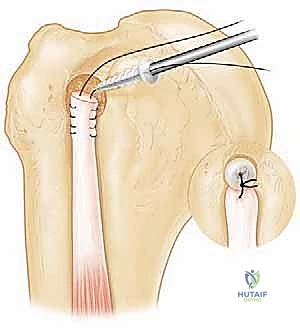
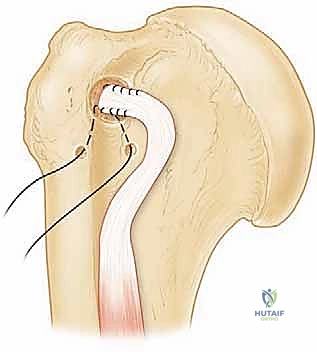
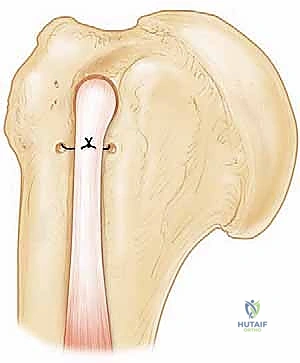
The LHB is identified, tagged, and tenotomized at its origin on the superior labrum. A suprapectoral or subpectoral tenodesis is then performed based on surgeon preference and the extent of biceps pathology. For a suprapectoral tenodesis, the tendon is whipstitched and secured into the bicipital groove using a biocomposite interference screw or suture anchors.
Attention is then turned to the subscapularis repair. The lesser tuberosity footprint is decorticated to a bleeding bone bed using a curette or burr. Depending on the tear size, a single or double-row suture anchor construct is utilized.
Anchors (typically 4.5mm to 5.5mm) are placed at the medial articular margin. High-strength sutures are passed through the tendon using a self-retrieving tissue penetrator, utilizing horizontal mattress or Mason-Allen configurations for optimal tissue grip.
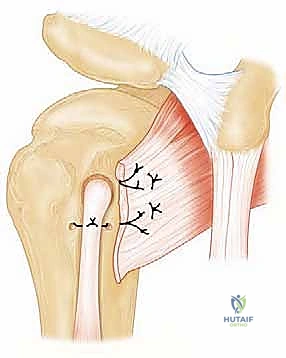
The arm is placed in approximately 20 to 30 degrees of internal rotation to remove tension from the repair, and the knots are tied sequentially from inferior to superior. A knotless lateral row can be added to compress the tendon against the footprint, maximizing the healing surface area.
Complications, Incidence Rates, and Salvage Management
Even with meticulous technique, complications in complex anterior shoulder reconstruction can occur. Anticipation, early recognition, and appropriate management are critical for mitigating long-term morbidity.
Neurologic injury is a devastating complication. Musculocutaneous nerve palsy occurs in approximately 1% to 2% of open anterior shoulder procedures, almost exclusively due to aggressive or prolonged medial retraction of the conjoined tendon. Symptoms include weakness in elbow flexion and numbness over the lateral forearm. Most cases are traction neuropraxias that resolve spontaneously over 3 to 6 months, managed with observation and supportive physical therapy. Axillary nerve injury is less common but can occur during aggressive inferior capsular releases. Prevention relies on keeping dissection instruments strictly on the tendinous insertion of the subscapularis and avoiding blind electrocautery at the 6 o'clock position.
Structural failure and re-tear of the subscapularis tendon remain significant concerns, with incidence rates reported between 5% and 15% depending on the initial tear size and tissue quality. Failures are often due to inadequate mobilization leading to a high-tension repair, poor biological healing (especially in patients with high Goutallier grades), or patient non-compliance with postoperative lifting restrictions. Salvage management for a failed repair in a young patient may involve a revision repair with allograft augmentation or a pectoralis major tendon transfer. In older, lower-demand patients, or those with concomitant arthritis, a reverse total shoulder arthroplasty is the salvage procedure of choice.
Postoperative stiffness, particularly an internal rotation contracture, is another common complication, occurring in up to 10% of patients. This is often an intentional trade-off to protect the repair, but excessive stiffness can limit function. Management begins with aggressive, phased physical therapy. If stiffness persists beyond 6 to 9 months and significantly impairs activities of daily living, an arthroscopic capsular release may be indicated. Infection, particularly involving indolent organisms like Cutibacterium acnes (formerly Propionibacterium acnes), must always be considered in cases of insidious postoperative pain and stiffness, requiring aggressive irrigation, debridement, and prolonged targeted antibiotic therapy.
| Complication | Estimated Incidence | Prevention and Intraoperative Avoidance | Salvage / Management Strategy |
|---|---|---|---|
| ** |
Clinical & Radiographic Imaging Archive
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding subscapularis-repair-coracoid-recession-and-biceps-tenodesis