Supramalleolar Osteotomy with External Fixation: A Masterclass in Distal Tibial Deformity Correction

Key Takeaway
Join us in the OR for a masterclass on supramalleolar osteotomy (SMO) with external fixation. This immersive guide covers meticulous preoperative planning, critical surgical anatomy, and a granular, real-time breakdown of percutaneous osteotomy and circular fixator application for complex distal tibial deformities. We emphasize neurovascular protection, precise technique, and managing potential pitfalls for optimal patient outcomes.
The management of distal tibial deformities represents one of the most mechanically and biologically demanding challenges in orthopedic surgery. This masterclass chapter explores the Supramalleolar Osteotomy (SMO) combined with circular external fixation, an advanced technique designed to restore anatomical alignment, preserve the native ankle joint, and optimize long-term biomechanical function. Unlike acute corrections utilizing internal fixation, which are often limited by the soft tissue envelope and the magnitude of the deformity, external fixation leverages the principles of distraction osteogenesis and gradual tissue adaptation. This approach is particularly indispensable when addressing complex, multiplanar deformities in the presence of compromised soft tissues, osteopenia, or active infection.
Comprehensive Introduction and Patho-Epidemiology
The evolution of the supramalleolar osteotomy is deeply intertwined with the pioneering work of Gavriil Ilizarov and the subsequent development of hexapod circular external fixators. Historically, distal tibial malunions and congenital deformities were managed with closing or opening wedge osteotomies stabilized by plates and screws. While effective for mild, uniplanar deformities in patients with pristine soft tissues, these techniques frequently fall short in the post-traumatic setting. The advent of the Ilizarov method introduced the concept of the "tension-stress effect," allowing for the simultaneous correction of angular, translational, and rotational deformities while lengthening the limb. Modern hexapod systems, such as the Taylor Spatial Frame (TSF), have further revolutionized this process by utilizing computer software to precisely manage six degrees of freedom, transforming complex 3D deformity correction into a highly reproducible, mathematically driven science.

The patho-epidemiology of distal tibial deformities is predominantly post-traumatic, stemming from malunited pilon fractures, distal third tibial shaft fractures, or physeal arrest following pediatric trauma. Metabolic bone diseases (such as rickets), congenital anomalies (like clubfoot sequelae), and neuromuscular disorders also contribute to the patient population requiring SMO. Regardless of the etiology, the mechanical consequence is a shift in the mechanical axis deviation (MAD). The ankle joint, possessing a relatively small surface area compared to the knee or hip, is exquisitely sensitive to asymmetric loading. A varus or valgus malalignment of even a few degrees significantly decreases the contact area within the tibiotalar joint, exponentially increasing peak contact stresses. This biomechanical cascade inevitably leads to early-onset, asymmetric osteoarthritis if left uncorrected.


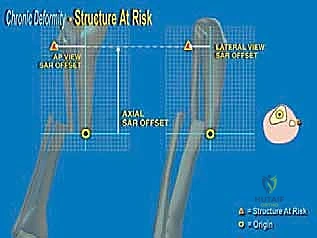
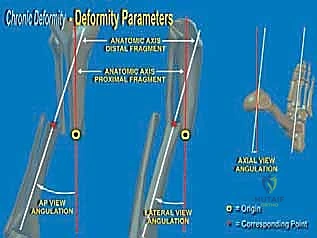
A core philosophical tenet of this procedure revolves around the strategic placement of the osteotomy relative to the Center of Rotation and Angulation (CORA). While geometric principles dictate that an osteotomy at the true CORA allows for pure angular correction without translation, biological realities often necessitate a different approach. In chronic post-traumatic deformities, the bone at the CORA is frequently highly sclerotic, avascular, and biologically inert due to chronic stress shielding and microtrauma. Performing an osteotomy through this dense bone drastically increases the risk of delayed union or nonunion. Therefore, we advocate for executing the SMO at the metaphyseal-diaphyseal junction—typically 5 cm proximal to the ankle joint—where the bone is highly vascularized and possesses robust osteogenic potential. This offset osteotomy requires calculated translation to realign the mechanical axis, a task effortlessly managed by hexapod external fixators.


Furthermore, the utilization of a percutaneous, minimally invasive approach preserves the periosteal and endosteal blood supply, which is the lifeblood of distraction osteogenesis. The external fixator acts not only as a rigid stabilization device but also as a dynamic biological tool. By allowing for gradual correction, we mitigate the risk of acute neurovascular compromise and skin necrosis—complications that frequently plague open, acute corrections. This philosophy prioritizes biological preservation and mechanical precision, ensuring that we not only correct the radiographic parameters but also optimize the host tissue's healing capacity.
Detailed Surgical Anatomy and Biomechanics
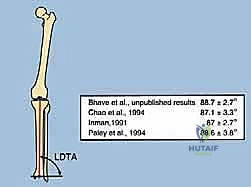
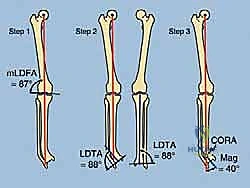
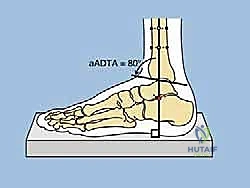
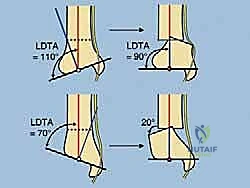
A profound mastery of distal tibial and ankle anatomy is the absolute prerequisite for safely executing a supramalleolar osteotomy and applying a circular frame. Osteologically, the distal tibia flares into the metaphysis, forming the robust medial malleolus and the tibial plafond, which articulates with the talar dome. The normal Lateral Distal Tibial Angle (LDTA) is approximately 89 degrees, and the Anterior Distal Tibial Angle (ADTA) is approximately 80 degrees. Deviations from these normative values dictate our correction parameters. The fibula, securely bound to the tibia by the distal tibiofibular syndesmosis, plays a critical role in lateral column stability. Any correction of the tibia must be accompanied by an appropriate fibular osteotomy; failure to release the fibula will result in a tethering effect, preventing tibial correction and potentially causing syndesmotic diastasis or subluxation of the talus.


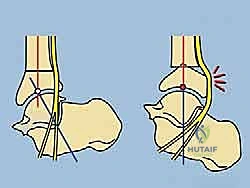
Navigating the muscular and tendinous intervals requires meticulous attention to cross-sectional anatomy. The anterior compartment houses the tibialis anterior, extensor hallucis longus (EHL), and extensor digitorum longus (EDL). Our preferred percutaneous approach for the tibial osteotomy utilizes a safe zone medial to the tibialis anterior tendon. This specific interval avoids direct injury to the muscle bellies and keeps the surgeon safely away from the anterior neurovascular bundle (deep peroneal nerve and anterior tibial artery), which lies lateral to the tibialis anterior and EHL. During wire and half-pin insertion, strict adherence to established cross-sectional safe zones is mandatory to avoid transfixing these tendinous structures, which would severely restrict postoperative range of motion and cause debilitating pain.

Neurovascular considerations are paramount, particularly regarding the tibial nerve and the posterior tibial artery, which course through the deep posterior compartment and enter the tarsal tunnel posteromedially. The tibial nerve is at extreme risk during the correction of significant varus or procurvatum (apex anterior) deformities. These deformities chronically shorten the nerve; acute correction can induce severe stretch neuropraxia. The gradual correction afforded by external fixation allows for biological adaptation (neurogenesis) of the nerve. However, prophylactic tarsal tunnel release must be considered if the preoperative deformity is severe or if acute intraoperative translation is planned. Additionally, the superficial peroneal nerve, exiting the lateral compartment to provide dorsal foot sensation, is highly vulnerable during the placement of anterolateral half-pins and must be actively protected through careful blunt dissection down to the bone.


Finally, the soft tissue envelope of the distal third of the leg is notoriously tenuous, lacking robust muscular coverage and relying on a delicate fascial-cutaneous blood supply defined by specific angiosomes. In post-traumatic scenarios, this envelope is often further compromised by previous incisions, skin grafts, free flaps, or chronic venous stasis. The presence of adherent, scarred skin dictates that large, open approaches for internal fixation are fraught with the risk of catastrophic wound breakdown and deep infection. The percutaneous osteotomy technique, utilizing multiple small drill holes and a narrow osteotome or Gigli saw, respects this fragile envelope. By minimizing surgical trauma to the soft tissues, we preserve the critical extrinsic blood supply to the healing osteotomy site, drastically reducing the incidence of infection and nonunion.
Exhaustive Indications and Contraindications
The decision to proceed with a supramalleolar osteotomy utilizing external fixation requires a nuanced understanding of both the mechanical deformity and the patient's biological and psychological capacity to tolerate a prolonged reconstructive process. The primary indication is a symptomatic malalignment of the distal tibia that alters the mechanical axis of the lower extremity, threatening the longevity of the ankle and subtalar joints. This includes post-traumatic malunions presenting with multiplanar deformities (varus/valgus, procurvatum/recurvatum, translation, and internal/external rotation). It is also highly indicated for patients with concomitant limb length discrepancies (LLD) exceeding 1.5 to 2.0 cm, as circular frames allow for simultaneous angular correction and distraction osteogenesis.

Another critical indication is the presence of an infected nonunion or a deformity combined with active osteomyelitis. In these complex limb salvage scenarios, internal fixation is absolutely contraindicated due to the presence of biofilm-producing bacteria. External fixation allows for aggressive debridement of necrotic bone, acute shortening to close soft tissue defects if necessary, and subsequent bone transport or gradual correction away from the zone of infection. Furthermore, SMO is indicated as a joint-preserving procedure in patients with early, asymmetric ankle osteoarthritis. By realigning the mechanical axis to shift weight-bearing forces away from the damaged cartilage and onto the preserved articular surfaces, surgeons can significantly delay or eliminate the need for total ankle arthroplasty or arthrodesis.
Despite its versatility, several absolute and relative contraindications must be respected. Absolute contraindications include severe, uncorrectable peripheral vascular disease that precludes adequate healing of the osteotomy or pin tracts. Profound peripheral neuropathy, such as advanced Charcot neuroarthropathy with total loss of protective sensation, is a strong relative contraindication; these patients are at high risk for catastrophic pin tract infections, unrecognized fractures, and rapid frame loosening. Psychological instability, active substance abuse, or a demonstrated inability to comply with the rigorous postoperative demands of pin care and frame adjustments also serve as definitive contraindications. The success of this procedure relies heavily on the patient's active participation in their own care.
| Category | Indications | Contraindications |
|---|---|---|
| Mechanical | Multiplanar distal tibial malunions; MAD > 10mm; LDTA/ADTA deviations > 5°; LLD > 1.5cm. | Severe, unbraceable knee instability proximal to the deformity. |
| Biological | Infected nonunions; compromised soft tissue envelope (flaps/grafts); early asymmetric ankle OA. | Severe peripheral vascular disease (ABI < 0.5); active systemic sepsis. |
| Patient Factors | Motivated patient capable of daily pin care and strut adjustments; limb salvage candidates. | Advanced Charcot neuropathy; non-compliance; severe psychiatric illness. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which successful deformity correction is built. The clinical evaluation must be exhaustive, beginning with a detailed gait analysis to observe dynamic compensatory mechanisms, such as subtalar valgus compensating for tibial varus. Limb length discrepancy must be quantified clinically using calibrated blocks under the shorter limb until the pelvis is level. The rotational profile is assessed with the patient prone, measuring the thigh-foot axis to quantify internal or external tibial torsion. A rigorous neurovascular examination is mandatory; documenting baseline sensory or motor deficits is crucial, as is evaluating the quality of pedal pulses. The soft tissue envelope must be mapped, noting the location of all previous surgical scars, skin grafts, and areas of adherent skin, which will dictate optimal pin and wire placement.
The radiographic protocol is standardized and non-negotiable. It begins with a 51-inch bipedal erect leg radiograph (hips to ankles) with the patellae oriented strictly forward. This allows for the calculation of the Mechanical Axis Deviation (MAD) and the joint orientation angles. Orthogonal, weight-bearing AP, lateral, and mortise views of the affected ankle provide localized detail of the joint space and the deformity apex. A Saltzman alignment view is critical to evaluate hindfoot compensation. Advanced imaging is frequently employed; a fine-cut CT scan with 3D reconstructions is invaluable for mapping complex rotational deformities, assessing the extent of sclerotic bone at a nonunion site, and planning the precise trajectory of the osteotomy. MRI may be indicated if there is suspicion of deep infection, osteomyelitis, or significant chondral defects within the tibiotalar joint.


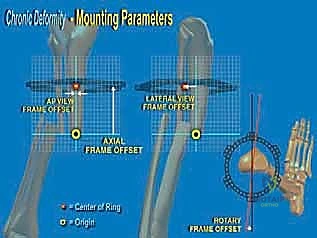
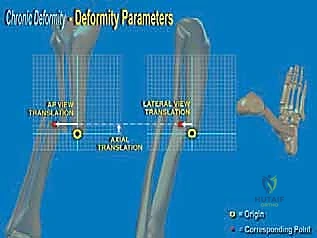
Deformity analysis and templating transition the clinical data into a surgical blueprint. On the AP and lateral radiographs, the proximal and distal anatomical axes are drawn. The intersection of these lines identifies the Center of Rotation and Angulation (CORA). The surgeon must then decide whether to perform the osteotomy directly at the CORA or at an offset location (e.g., the metaphyseal-diaphyseal junction). If an offset osteotomy is chosen, the required translation to realign the mechanical axis must be mathematically calculated. Using hexapod software, the surgeon inputs the bone parameters, deformity parameters, and frame mounting parameters to generate a preliminary correction schedule. Ring sizes are selected to allow at least 2 fingerbreadths (approx. 3 cm) of clearance circumferentially around the leg to accommodate postoperative edema without causing skin necrosis.


Patient positioning in the operating room is designed to facilitate unrestricted fluoroscopic access and precise limb alignment. The patient is placed supine on a fully radiolucent Jackson or OSI flat table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring that the patella points directly toward the ceiling. This neutral rotation is critical for establishing accurate AP and lateral fluoroscopic views without constantly rotating the C-arm. The limb is prepped and draped freely from the toes to the proximal thigh. A sterile tourniquet may be applied but is rarely inflated, as the continuous assessment of distal perfusion is vital during wire placement and osteotomy execution. The C-arm is brought in from the contralateral side, positioned to easily swing between orthogonal views.
Step-by-Step Surgical Approach and Fixation Technique
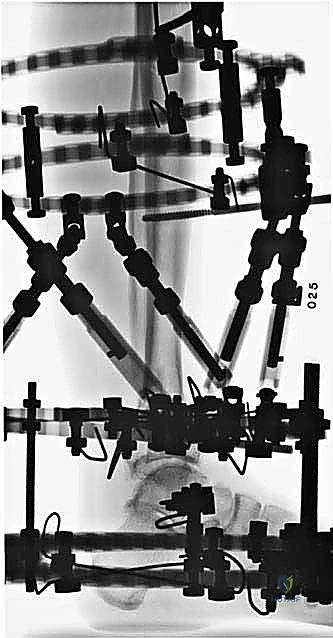
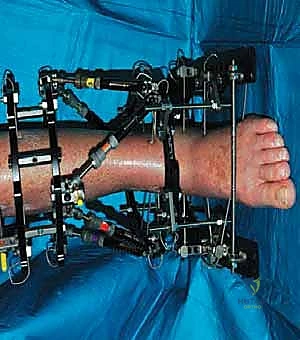
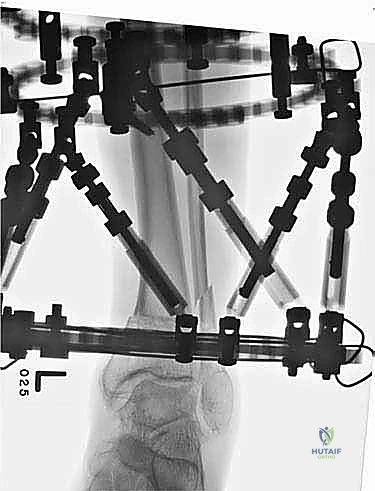
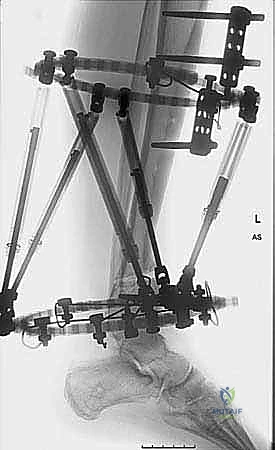
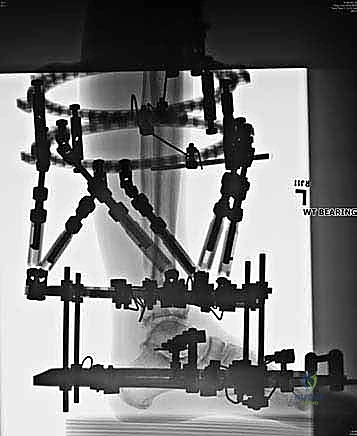
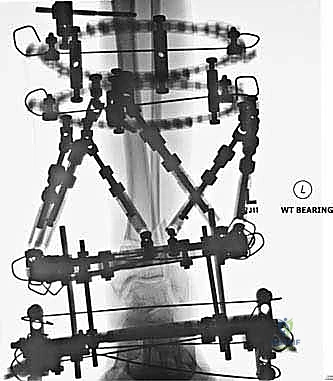
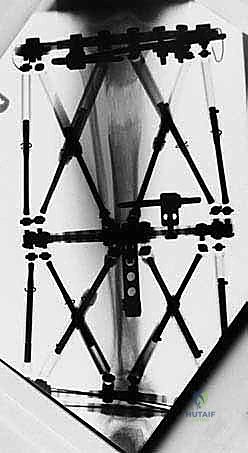
The surgical execution begins with the application of the circular external fixator, prioritizing stability and adherence to safe zones. The pre-assembled frame is passed over the limb. The distal reference ring is applied first, oriented parallel to the ankle joint line in both the coronal and sagittal planes. A smooth 1.8 mm Ilizarov wire is driven transversely across the distal tibia, starting from the lateral side (anterior to the fibula) and exiting medially, strictly avoiding the anterior neurovascular bundle and the posterior tarsal tunnel structures. This wire is tensioned to 130 kg. A second, olive wire is placed from posterolateral to anteromedial to provide multiplanar stability. The proximal ring is then secured to the tibial diaphysis, orthogonal to the proximal mechanical axis, utilizing a combination of tensioned wires and hydroxyapatite-coated 5.0 mm or 6.0 mm half-pins placed strictly in the anterior or anteromedial safe zones.

Following rigid frame application, attention turns to the fibular osteotomy. The fibula must be addressed to prevent tethering during tibial correction. The level of the fibular osteotomy depends on the apex of the tibial deformity but is typically performed in the middle or distal third of the fibular shaft. A 3 cm longitudinal incision is made over the posterolateral border of the fibula, carefully identifying and protecting the superficial peroneal nerve anteriorly. The periosteum is incised and elevated. We prefer a multiple drill-hole technique followed by a narrow osteotome to complete the cut, minimizing thermal necrosis and preserving the periosteal sleeve. The fibular ends must be demonstrably mobile; any residual tethering will severely compromise the subsequent tibial correction and generate excessive forces on the frame.
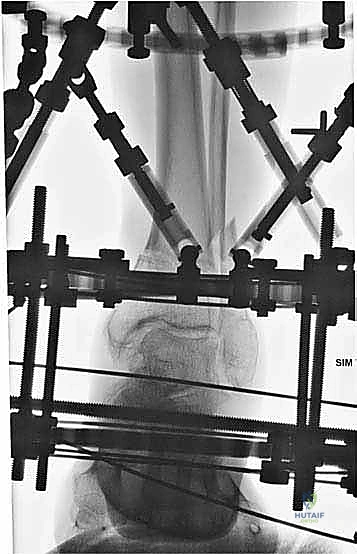

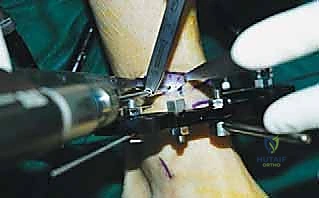
The percutaneous supramalleolar tibial osteotomy is the most critical step. A 1 cm vertical incision is made directly over the tibial crest, approximately 5 cm proximal to the ankle joint, staying medial to the tibialis anterior tendon. Blunt dissection is carried down to the periosteum. A periosteal elevator is used to create a subperiosteal tunnel medially and laterally. Using a 4.8 mm drill bit under fluoroscopic guidance, multiple contiguous holes are drilled across the tibial metaphysis in a single plane, creating a "postage stamp" effect. It is imperative to internally rotate the foot during the posteromedial drilling to protect the tibial nerve and posterior tibial artery from the drill bit. Alternatively, a Gigli saw can be passed subperiosteally to perform the osteotomy, which provides a remarkably clean and biologically friendly cut.


The osteotomy is completed by passing a sharp, 10 mm osteotome through the drill holes, gently twisting to fracture the remaining cortical bridges. The surgeon must feel a distinct "clunk" and visually confirm translational mobility of the distal fragment on fluoroscopy to ensure a complete corticotomy. Incomplete osteotomies will result in premature consolidation or failure of the frame struts during the distraction phase. Once complete, the surgical wounds are irrigated and closed loosely with nylon sutures. If an acute correction is planned, the frame struts are adjusted in the OR to achieve the desired alignment. If gradual correction is planned (our preferred method for large deformities), the frame is locked in its neutral, uncorrected position. Sterile dressings are applied around the pin sites, utilizing compressive sponges to minimize hematoma formation and prevent skin tethering.

Complications, Incidence Rates, and Salvage Management
Complications in supramalleolar osteotomy with external fixation are not uncommon, but the vast majority are minor and entirely manageable if identified early. Pin tract infection is the most ubiquitous complication, occurring in up to 80% of patients during the lifespan of the frame. These are typically superficial, presenting with localized erythema, serous drainage, and mild pain. Management relies on the Checketts-MacDonald classification. Grade 1 and 2 infections are treated aggressively with local pin care optimization (chlorhexidine washes, tension-free skin releases) and short courses of oral antibiotics (e.g., cephalexin or doxycycline). Deep infections (Grade 3 or higher) involving osteolysis or ring sequestrum require immediate intravenous antibiotics, pin removal, debridement, and re-insertion of a new pin at a safe, adjacent site to maintain construct stability.


Neurovascular compromise, particularly tibial nerve stretch neuropraxia, is a severe complication associated with the rapid correction of chronic varus or procurvatum deformities. The nerve, having adapted to a shortened path, becomes acutely ischemic when stretched. Patients will report burning pain radiating into the plantar aspect of the foot, followed by sensory blunting and potentially motor weakness (loss of toe flexion). The immediate salvage management is to halt the correction schedule and potentially reverse the struts by a few millimeters to relieve tension. The correction is then resumed at a much slower rate (e.g., 0.25 mm/day instead of 1 mm/day). If symptoms persist or if a massive acute correction is mandatory, a prophylactic or therapeutic surgical release of the tarsal tunnel is required to decompress the nerve.

Delayed union and nonunion at the osteotomy site occur in approximately 5-10% of cases, heavily correlated with patient factors such as smoking, poorly controlled diabetes, or executing the osteotomy through
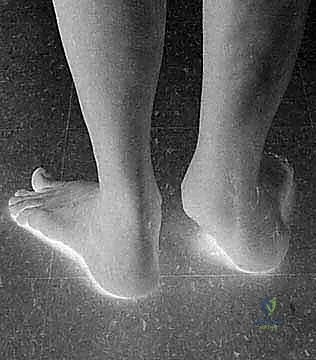
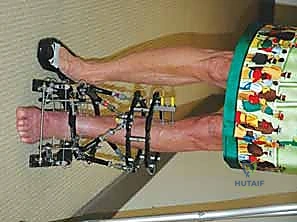
Clinical & Radiographic Imaging Archive