Masterclass: Precision Surgical Correction of Bunionette Deformity

Key Takeaway
Step into the operating theater for a comprehensive masterclass on bunionette deformity correction. This guide details preoperative planning, precise intraoperative techniques including condylectomy, chevron, and oblique metatarsal osteotomies, complete with anatomical considerations, critical pearls, and complication management. Learn to navigate neurovascular risks and achieve optimal patient outcomes with this immersive, step-by-step surgical breakdown.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are addressing a ubiquitous yet frequently underestimated source of lateral forefoot pathology: the bunionette deformity, historically and colloquially known as a tailor's bunion. While often perceived by the uninitiated as a minor cosmetic ailment or a simple hyperkeratotic lesion, a poorly managed bunionette can significantly compromise a patient's ambulatory capacity and overall quality of life. Our objective in this masterclass is not merely the mechanical correction of the deformity, but the instillation of the meticulous technical precision and critical biomechanical reasoning required to achieve consistent, excellent, and durable outcomes.
The bunionette is essentially a painful osseous and soft-tissue prominence on the lateral aspect of the fifth metatarsal head. However, this simplistic definition belies a complex patho-anatomical spectrum. The etiology is multifactorial, representing a confluence of intrinsic anatomical predispositions and extrinsic mechanical forces. Intrinsically, variations in the morphology of the fifth ray dictate the specific type of deformity. These include a congenitally prominent or hypertrophic lateral metatarsal condyle, a structural bowing or lateral deviation of the fifth metatarsal shaft in the transverse plane, or a divergent articulation at the fifth tarsometatarsal joint leading to a pathologically increased intermetatarsal angle between the fourth and fifth metatarsals.
Extrinsic factors act as the catalyst for symptomatology. Chronic extrinsic pressure, predominantly from constrictive, narrow-toebox footwear, exacerbates the underlying anatomical prominence. Historically, the occupational posture of tailors sitting cross-legged applied direct, unyielding pressure to the lateral aspect of the fifth metatarsal head, giving rise to the eponym. This repetitive microtrauma and frictional shear stress precipitate a cascade of localized inflammatory responses. The skin hypertrophies, forming painful, intractable plantar or lateral keratoses (IPK). The underlying adventitial bursa becomes acutely inflamed, thickened, and occasionally infected, while the joint capsule itself undergoes fibrotic changes due to chronic mechanical overload.
Understanding the epidemiology of the bunionette deformity is crucial for anticipating patient demographics and tailoring treatment expectations. It is overwhelmingly more prevalent in the female population, a demographic disparity largely attributed to the biomechanical constraints of modern fashionable footwear. Furthermore, bunionette deformities rarely exist in a vacuum; they are frequently concomitant with other complex forefoot pathologies, such as hallux valgus, splayfoot deformities, and lesser toe contractures (hammer or claw toes). A comprehensive surgical strategy must account for these concurrent deformities, as isolated correction of the fifth ray in the presence of global forefoot biomechanical failure will inevitably lead to suboptimal outcomes, transfer metatarsalgia, or rapid recurrence.
Detailed Surgical Anatomy and Biomechanics
Mastery of the intricate anatomy of the lateral forefoot is the absolute prerequisite for executing precise surgical correction and avoiding devastating iatrogenic complications. The fifth ray is a dynamically unique structure, functioning not as a rigid lever, but as a mobile, adaptive column during the terminal stance phase of the gait cycle. Osteologically, the fifth metatarsal is the most lateral and structurally independent of the metatarsals. Its proximal base articulates with the cuboid, forming a highly mobile tarsometatarsal articulation that allows for independent triplanar motion—specifically, pronation and supination—essential for accommodating uneven terrain. The metatarsal shaft possesses a natural lateral curvature, and the distal head articulates with the proximal phalanx of the fifth toe, forming the fifth metatarsophalangeal (MTP) joint.
The soft-tissue envelope surrounding the fifth MTP joint is highly specialized. The joint capsule is inherently thin dorsally but heavily reinforced plantarly by the plantar plate, a robust fibrocartilaginous structure that resists dorsal subluxation of the proximal phalanx and protects the metatarsal head from direct vertical weight-bearing forces. Medial and lateral collateral ligaments provide coronal plane stability. The musculotendinous anatomy must be respected and preserved during exposure. The extensor digiti minimi and extensor digitorum longus tendons cross the joint dorsally, while the flexor digiti minimi brevis and the flexor digitorum longus tendons traverse plantarly. The abductor digiti minimi, originating from the calcaneus, inserts onto the lateral base of the proximal phalanx, contributing significantly to the lateral soft-tissue bulk and functioning as an active dynamic stabilizer of the lateral column.
Neurovascular preservation is the most critical aspect of the superficial dissection, fellows. The lateral dorsal digital nerve, a terminal branch of the superficial fibular (peroneal) nerve, courses distally along the dorsolateral aspect of the fifth metatarsal shaft and head. It is remarkably superficial, lying just beneath the subdermal adipose layer, making it highly susceptible to transection, traction neuropraxia, or entrapment within scar tissue during the initial skin incision and capsular exposure. Injury to this nerve results in painful neuromas and debilitating lateral toe numbness. Plantarly, the lateral plantar digital nerve runs deep to the plantar fascia; while less directly exposed during a standard lateral approach, aggressive plantar retractor placement can induce neuropraxia.
The vascular supply to the fifth metatarsal head is equally critical, particularly when planning osteotomies. The primary blood supply derives from the lateral metatarsal arteries, which form a rich extraosseous anastomotic network before penetrating the metatarsal neck and head via small capsular vessels. Excessive periosteal stripping, particularly aggressive circumferential dissection at the metatarsal neck, disrupts this delicate vascular plexus. This iatrogenic devascularization drastically increases the risk of avascular necrosis (AVN) of the metatarsal head and delayed union or nonunion of distal osteotomies. Therefore, dissection must remain strictly subperiosteal only where necessary for the osteotomy cuts, preserving the soft-tissue attachments dorsally and plantarly.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a bunionette deformity must be predicated on a rigorous evaluation of the patient's symptoms, functional limitations, and failure of comprehensive non-operative management. Surgery is never indicated for purely cosmetic concerns or asymptomatic radiographic abnormalities. The primary indication is recalcitrant lateral forefoot pain localized to the fifth metatarsal head that significantly impairs activities of daily living and persists despite at least 3 to 6 months of conservative therapy. Conservative measures must include aggressive footwear modification (wide toe-box shoes, seamless uppers), custom or over-the-counter orthoses with lateral offloading pads, padding of the bony prominence, and judicious use of non-steroidal anti-inflammatory drugs (NSAIDs) or localized corticosteroid injections for acute bursitis.
When conservative measures are exhausted, the specific surgical indication is dictated by the precise anatomical nature of the deformity, as defined by the Coughlin classification. A Type 1 deformity (prominent lateral condyle) warrants a lateral condylectomy. A Type 2 deformity (lateral bowing of the metatarsal shaft) necessitates a distal metatarsal osteotomy, such as a chevron or transverse sliding osteotomy, to medialize the articular surface. A Type 3 deformity (widened 4-5 intermetatarsal angle) requires a proximal metatarsal osteotomy or a diaphyseal osteotomy to correct the severe angular divergence. Furthermore, the presence of a painful, intractable plantar keratosis (IPK) directly beneath the fifth metatarsal head may indicate the need for an osteotomy that incorporates a dorsal closing wedge to elevate the metatarsal head, alleviating plantar pressure.
Contraindications to bunionette surgery must be carefully respected to prevent catastrophic outcomes. Active local or systemic infection is an absolute contraindication. Severe peripheral vascular disease (PVD) characterized by absent pedal pulses, delayed capillary refill, or a low ankle-brachial index (ABI) precludes any elective forefoot surgery due to the unacceptably high risk of wound dehiscence, infection, and subsequent amputation. Similarly, poorly controlled diabetes mellitus with significant peripheral neuropathy presents a relative to absolute contraindication; these patients are at extreme risk for Charcot neuroarthropathy, unrecognized postoperative trauma, and chronic ulceration.
Furthermore, patients with unrealistic expectations, profound psychiatric comorbidities, or those who are non-compliant and cannot adhere to strict postoperative weight-bearing restrictions are poor surgical candidates. In the setting of severe, end-stage osteoarthritis of the fifth MTP joint, isolated corrective osteotomies will fail to relieve pain; these cases may require joint arthroplasty, resection arthroplasty, or, rarely, arthrodesis. The surgeon must also carefully evaluate the entire lower extremity kinetic chain; operating on a bunionette in the presence of an unaddressed, severe equinus contracture or profound pes planovalgus will likely result in rapid recurrence due to persistent, uncorrected deforming forces.
| Category | Specific Condition | Indication / Contraindication | Clinical Rationale |
|---|---|---|---|
| Indications | Recalcitrant Pain | Absolute Indication | Failure of 3-6 months of conservative care (shoe modification, padding). |
| Indications | Type 1 Deformity | Indication for Condylectomy | Hypertrophic lateral condyle causing localized pressure without angular deviation. |
| Indications | Type 2/3 Deformity | Indication for Osteotomy | Structural bowing or widened IMA requiring osseous realignment. |
| Contraindications | Severe PVD | Absolute Contraindication | High risk of wound necrosis, non-healing, and potential amputation. |
| Contraindications | Active Infection | Absolute Contraindication | Risk of osteomyelitis and systemic spread; must resolve prior to elective surgery. |
| Contraindications | Severe Neuropathy | Relative/Absolute | Inability to protect the surgical site; high risk of Charcot arthropathy or ulceration. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Radiographic Assessment
Before we even consider making an incision, comprehensive patient assessment and meticulous preoperative planning are paramount. Our patient presents with classic symptoms: pain and tenderness localized over the lateral aspect of the fifth metatarsal head, exacerbated by activity and enclosed footwear. They often describe seasonal variations, with symptoms improving in less restrictive summer footwear. As we examine the patient, we must observe both feet simultaneously in a standing, weight-bearing position. Note any obvious lateral prominence, a palpable hard or soft callus over the fifth metatarsal head, or an inflamed bursa. Skin integrity is critical; carefully inspect for any ulceration over the callus or between the fourth and fifth toes, which could indicate neuropathy or severe pressure.
Standing plain radiographs are indispensable for classifying the bunionette and guiding our surgical strategy. We require weight-bearing Anteroposterior (AP), lateral, and oblique views. On the AP view, we evaluate for joint space narrowing, subchondral sclerosis, or osteophyte formation suggestive of arthritis. Crucially, we measure the intermetatarsal angle (IMA) between the fourth and fifth metatarsals. A normal 4-5 IMA is typically less than 8 degrees; an angle exceeding this indicates a Type 3 deformity. We also measure the lateral deviation angle of the fifth metatarsal to identify a Type 2 deformity. The oblique view often provides the clearest visualization of the lateral metatarsal head, allowing us to identify a prominent lateral condyle (Type 1). The lateral view is essential to assess for any sagittal plane deformities, such as plantarflexion of the metatarsal head causing an IPK, or concurrent lesser toe deformities.
Operating Room Setup and Positioning
For distal metatarsal osteotomies and condylectomies, intraoperative fluoroscopy is absolutely essential to confirm our osteotomy cuts, assess intra-articular alignment, and verify hardware placement. The C-arm must be positioned to allow for immediate AP, lateral, and oblique views of the forefoot without requiring the surgical team to break scrub or reposition the patient. This usually entails placing the image intensifier on the contralateral side of the patient, with the X-ray tube positioned below the radiolucent operating table. Ensuring the table is fully radiolucent at the foot of the bed is a non-negotiable requirement for this procedure.
The patient is positioned supine. A critical, often overlooked step is the placement of a small, rolled blanket or gel bolster under the ipsilateral buttock. This maneuver internally rotates the hip, bringing the foot out of its natural externally rotated resting posture and into a neutral position. This provides the surgeon with direct, ergonomic access to the lateral aspect of the foot, preventing intraoperative fatigue and ensuring precise instrument trajectory. Finally, a sterile Esmarch tourniquet is applied tightly above the ankle, or a pneumatic thigh tourniquet is utilized based on surgeon preference. We will inflate our ankle tourniquet to 250 mmHg immediately prior to incision to ensure a completely bloodless surgical field, which is vital for identifying the delicate neurovascular structures.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
"Alright team, let's begin. We've prepped and draped, and our tourniquet is inflated. The first step is our skin incision."
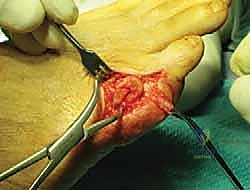
Using a #15 scalpel blade, we make a longitudinal incision approximately 3-4 cm in length, centered precisely over the palpable prominence of the fifth metatarsal head. It is crucial to place this incision directly lateral—midway between the dorsal and plantar margins of the foot—to avoid the extensor tendons dorsally and the weight-bearing plantar skin.

Remember, fellows, caution is paramount to avoid the digital nerves. The lateral dorsal digital nerve is a superficial structure lying just beneath the dermis. A best practice is to score the epidermis with the scalpel, then deepen through the subcutaneous tissue using strictly blunt dissection or by gently spreading with small Metzenbaum scissors, always orienting the instrument parallel to the anticipated course of the nerve fibers.

Once the subdermal layer is breached, we utilize careful blunt and sharp dissection to mobilize the soft-tissue flaps, freeing the skin from the underlying joint capsule. This exposes the lateral aspect of the metatarsal head and any associated adventitial bursa. Meticulous hemostasis is achieved using bipolar electrocautery; monopolar cautery should be avoided near the skin edges to prevent thermal necrosis. If a thickened, inflamed bursa is present, we must carefully and completely excise it at this stage, as leaving fibrotic bursal tissue can lead to persistent postoperative swelling and pain.

Capsulotomy and Joint Exposure
With the bursa excised and the capsule exposed, we proceed to enter the joint. I prefer a V-shaped or L-shaped capsulotomy over the lateral aspect of the fifth MTP joint. For the V-capsulotomy, the apex of the 'V' is directed proximally toward the metatarsal shaft, while the diverging arms extend distally toward the base of the proximal phalanx.
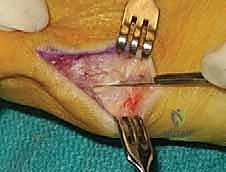
This specific geometric design is highly advantageous; it allows for robust, multi-directional plication and tightening of the capsule during closure. By advancing the V-flap proximally, we can effectively correct mild medial deviation of the toe and restore lateral collateral tension. Ensure your capsulotomy is precise, utilizing a #15 blade, and take exceptional care not to score the underlying articular cartilage of the metatarsal head.

Once the capsule is incised and reflected, we achieve full visualization of the enlarged lateral condyle of the fifth metatarsal head. My assistant will now carefully place small, blunt Hohmann or mini-Senn retractors—one dorsally and one plantarly. This maneuver is critical to protect the extensor digiti minimi tendon dorsally and the flexor digiti minimi brevis tendon and plantar plate plantarly. Excellent visualization and soft-tissue protection are the cornerstones of a safe osteotomy.
Lateral Metatarsal Condylectomy (Type 1 Deformity)
For a pure Type 1 deformity, where the pathology is isolated to a hypertrophic lateral condyle without shaft bowing or an increased IMA, a lateral condylectomy is the procedure of choice.

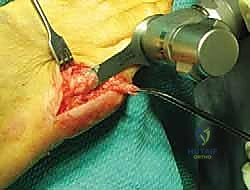
Using a micro-sagittal saw, we align the blade parallel to the lateral cortex of the metatarsal shaft. The cut begins distally at the parasagittal groove of the articular cartilage and exits proximally at the metaphyseal-diaphyseal junction.

It is imperative not to resect too much bone; aggressive resection can destabilize the MTP joint, leading to medial subluxation of the fifth toe, while insufficient resection will fail to relieve the patient's symptoms.

Following the primary saw cut, the excised bony fragment is removed. We then utilize a rongeur and a fine bone rasp to meticulously smooth the remaining lateral cortical margin.

Any sharp osseous edges left behind will act as a stress riser beneath the skin, causing recurrent pain and potentially deep tissue ulceration. Copious irrigation with sterile saline is performed to remove all bone debris, which could otherwise cause heterotopic ossification or severe postoperative inflammation.
Distal Metatarsal Osteotomy (Chevron) (Type 2 Deformity)
When encountering a Type 2 deformity characterized by lateral bowing of the metatarsal shaft, a condylectomy alone is insufficient; we must medialize the metatarsal head via a distal osteotomy. The distal chevron osteotomy is highly effective for this indication.

After performing the initial lateral eminence resection (as described above), we mark the apex of our chevron cut centrally within the metatarsal head, approximately 1 cm proximal to the articular surface.
The arms of the chevron are directed proximally at an angle of roughly 60 degrees. Using a fine micro-sagittal saw, the dorsal and plantar limbs of the osteotomy are executed.

Once the osteotomy is complete, the capital fragment is manually translated medially by 3 to 5 millimeters, depending on the severity of the deformity. It is crucial to avoid excessive medial translation, which can lead to lateral instability or loss of bony apposition resulting in nonunion.

Following medial translation, the osteotomy is provisionally fixated using a smooth 0.045-inch Kirschner wire (K-wire) driven from dorsal-distal to plantar-proximal.

Intraoperative fluoroscopy is immediately utilized to confirm the precise medialization of the head, the integrity of the MTP joint articulation, and the trajectory of our provisional fixation.
Once alignment is radiographically confirmed, definitive fixation is achieved. While K-wires can be left in place, I prefer rigid internal fixation using a single, low-profile 2.0mm or 2.4mm headless compression screw or a standard cortical screw.

The screw is introduced over the guidewire (if cannulated) or via a newly drilled path, ensuring it crosses the osteotomy site perpendicularly to maximize interfragmentary compression.

After the screw is fully seated, the prominent medial cortical overhang of the proximal metatarsal shaft is resected flush with the newly medialized metatarsal head using the sagittal saw.

This step is vital to prevent a new medial bony prominence that could impinge on the fourth metatarsal.

Final fluoroscopic images are obtained in AP, lateral, and oblique planes to document the final hardware placement and joint congruency.
The wound is then thoroughly irrigated. The V-shaped capsulotomy is meticulously repaired using 3-0 or 4-0 absorbable suture in a "pants-over-vest" or simple interrupted fashion, pulling the apex of the V proximally to tighten the lateral capsule and stabilize the toe.

The subcutaneous tissues are closed with buried interrupted sutures, and the skin is approximated with a running subcuticular closure or simple nylon sutures, ensuring no tension on the skin edges.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following bunionette correction can and do occur. The surgeon must be acutely aware of these risks, employ rigorous preventative strategies, and possess the knowledge to execute effective salvage management. One of the most common and frustrating complications is injury to the lateral dorsal digital nerve. The incidence of transient neuropraxia or permanent nerve injury ranges from 2% to 10% in the literature. Prevention relies entirely on meticulous, blunt superficial dissection and avoiding aggressive retraction. If a painful neuroma develops postoperatively, initial management includes targeted corticosteroid injections and desensitization therapy; recalcitrant cases may require surgical excision of the neuroma and burying the proximal nerve stump into the adjacent intrinsic musculature or bone.
Avascular necrosis (AVN) of the fifth metatarsal head is a devastating complication, particularly associated with distal osteotomies. While the reported incidence is relatively low (1-3%), the functional consequences are severe, leading to joint collapse, severe arthritis, and intractable pain. AVN is primarily prevented by minimizing periosteal stripping at the metatarsal neck and avoiding aggressive capsular dissection that disrupts the lateral metatarsal artery anastomotic network. If AVN occurs and progresses to joint collapse, conservative management involves offloading and orthotics. Surgical salvage typically necessitates an interpositional arthroplasty, resection of the metatarsal head, or, in severe cases, a fifth MTP joint arthrodesis.
Nonunion and delayed union of the osteotomy site are risks inherent to any bone-cutting procedure, with incidence rates hovering around 1-5%. Risk factors include inadequate internal fixation, thermal necrosis from the saw blade, excessive periosteal stripping, and patient non-compliance with postoperative weight-bearing restrictions. Prevention involves utilizing a sharp saw blade with copious irrigation to prevent thermal injury, ensuring rigid internal fixation (preferably with a compression screw), and strict adherence to postoperative protocols. Asymptomatic nonunions may be observed; however, painful nonunions require revision surgery, which involves debridement of the nonunion site, application of autologous bone graft, and revision rigid internal fixation.
Recurrence of the deformity or the development of transfer metatarsalgia are biomechanical failures. Recurrence (up to 10% in some series) often results from choosing an inadequate procedure (e.g., performing a simple condylectomy for a severe Type 3 deformity with a wide IMA) or failing to address concomitant forefoot pathology. Transfer metatarsalgia occurs when the fifth metatarsal is excessively elevated or shortened during the osteotomy, shifting the weight-bearing burden to the fourth metatarsal head. Prevention requires precise preoperative templating and intraoperative fluoroscopic confirmation to ensure the metatarsal head is medialized without unintentional dorsal translation or excessive shortening. Salvage for transfer metatarsalgia may involve custom orthotics or, surgically, a Weil osteotomy of the overloaded lesser metatarsal.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Nerve Injury (Neuroma) | 2% - 10% | Blunt superficial dissection; avoid aggressive lateral retraction. | Corticosteroid injections; surgical excision and burying of proximal stump. |
| **Avascular Necrosis ( |
