Suprascapular Nerve Decompression: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for an immersive masterclass on suprascapular nerve decompression. We'll meticulously explore both open and arthroscopic techniques, detailing critical anatomy, precise intraoperative steps, neurovascular considerations, and strategies for managing potential complications. From preoperative planning to postoperative rehabilitation, this guide provides a comprehensive overview for orthopaedic fellows.
Comprehensive Introduction and Patho-Epidemiology
Suprascapular nerve (SSN) entrapment represents a fascinating, intricate, and historically underappreciated etiology of shoulder pain and profound upper extremity dysfunction. Initially codified in the orthopedic literature by Koppel and Thompson, this compressive neuropathy demands a meticulous anatomical understanding and precise surgical execution that transcends routine shoulder arthroscopy or open rotator cuff repair. The clinical presentation is notoriously insidious, frequently masquerading as primary glenohumeral pathology, cervical radiculopathy, or intrinsic rotator cuff disease. Consequently, a high index of suspicion is paramount for the operating surgeon. The entrapment typically manifests at one of two critical anatomical choke points: the suprascapular notch or the spinoglenoid notch. Patients present with a heterogeneous spectrum of symptoms, ranging from a diffuse, deep-seated, nagging posterior shoulder ache to profound motor weakness and clinically obvious atrophy of the supraspinatus and infraspinatus muscle bellies.
The pathogenesis of SSN neuropathy is intimately tied to its etiology, which dictates both the natural history and the urgency of surgical intervention. When a space-occupying lesion—most classically a paralabral ganglion cyst—is the primary culprit, the pathology tends to be progressive. These cysts almost universally arise from posterosuperior or posterior labral tears, functioning via a one-way ball-valve mechanism that permits synovial fluid extravasation into the paralabral tissues while precluding backflow. As the cyst expands within the unyielding confines of the spinoglenoid or suprascapular notch, it exerts direct ischemic compression on the vasa nervorum of the SSN, leading to focal demyelination and, ultimately, Wallerian degeneration. While rare instances of spontaneous cyst rupture or resolution have been documented, expectant management in the presence of documented motor deficits is generally ill-advised due to the risk of irreversible muscle fibrosis and fatty infiltration.

Beyond discrete space-occupying lesions, the nerve is acutely vulnerable to dynamic traction and microtrauma. The suprascapular notch is the most frequent site of primary entrapment, where the nerve is tethered beneath a thickened, hypertrophic, or even ossified transverse scapular ligament (TSL). This relative anatomical confinement renders the nerve highly susceptible to traction injuries, particularly during repetitive overhead activities that combine extreme external rotation and abduction—a biomechanical pattern ubiquitous in overhead athletes such as volleyball attackers, tennis servers, and baseball pitchers. Furthermore, the modern shoulder surgeon must recognize "functional" traction neuropathy secondary to massive, retracted posterosuperior rotator cuff tears. As the supraspinatus tendon retracts medially, it dynamically alters the vector of the SSN, effectively bowstringing the nerve against the unyielding medial edge of the suprascapular notch.
Iatrogenic injury to the SSN remains a persistent threat that requires vigilant situational awareness during both open and arthroscopic procedures. The nerve is at risk during distal clavicle resections if dissection strays excessively posterior and inferior. It can be compromised by aggressive transglenoid drilling during posterior instability repairs, or by errant retractor placement during open posterior approaches to the glenohumeral joint. Even patient positioning for prolonged spine surgery in the prone position has been implicated in traction neurapraxia. Therefore, mastery of the nerve's anatomical course is not merely an academic exercise; it is the fundamental prerequisite for safe shoulder surgery.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional command of the regional anatomy is the bedrock of safe and effective suprascapular nerve decompression. The SSN is a mixed motor and sensory peripheral nerve, originating primarily from the upper trunk of the brachial plexus. It derives its dominant contributions from the C5 and C6 ventral rami, with a variable, albeit clinically significant, contribution from C4 in approximately 50% of the population. As it departs the upper trunk, it courses laterally and posteriorly through the posterior triangle of the neck, running deep to the trapezius and the omohyoid muscle before arriving at the superior border of the scapula.
Origin and Course of the Suprascapular Nerve
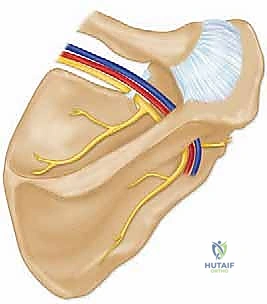
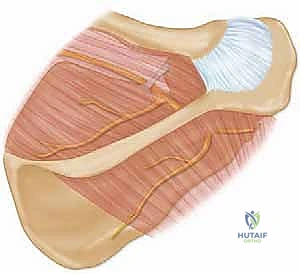
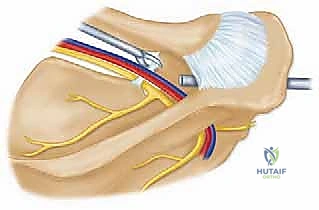
The nerve's trajectory through the scapular topography involves navigating two distinct, potentially constricting fibro-osseous portals. The first is the suprascapular notch, located on the superior border of the scapula, immediately medial to the base of the coracoid process. From a surgical landmark perspective, this notch lies approximately 4.5 cm medial to the posterolateral corner of the acromion and 3 cm medial to the supraglenoid tubercle. The notch is roofed by the transverse scapular ligament (TSL). The classic anatomical axiom "Army over Navy" dictates that the suprascapular artery courses over the TSL, while the suprascapular nerve passes under the ligament, directly against the periosteum of the notch. However, anatomical variants exist wherein the artery, or a significant venous plexus, accompanies the nerve beneath the ligament, necessitating meticulous blunt dissection prior to ligamentous release.
After exiting the suprascapular notch, the SSN provides two critical motor branches to the supraspinatus muscle and sensory articular branches to the coracoclavicular ligament, the acromioclavicular joint, and the superior capsule of the glenohumeral joint. The main trunk of the nerve then continues its descent, wrapping around the lateral margin of the scapular spine to enter the spinoglenoid notch. This second potential choke point is located approximately 1.8 cm medial to the posterior glenoid rim and 2.5 cm inferomedial to the supraglenoid tubercle.
At the spinoglenoid notch, the nerve is accompanied by the suprascapular artery and vein, which have rejoined the nerve's course. The neurovascular bundle is bounded medially by the base of the scapular spine and laterally by the glenoid neck. A distinct fascial band, the spinoglenoid ligament (or inferior transverse scapular ligament), roofs this notch in a variable percentage of individuals (ranging from 15% to 80% in cadaveric studies). When present, this ligament becomes taut during cross-body adduction and internal rotation, potentially compressing the nerve against the underlying bone and leading to isolated infraspinatus denervation.
Muscular Intervals and Neurovascular Risks
Navigating the muscular intervals to access these notches requires precision to avoid collateral iatrogenic damage. The traditional open approach to the suprascapular notch utilizes a trapezius-splitting technique. The trapezius, innervated by the spinal accessory nerve (Cranial Nerve XI), is generally forgiving of a longitudinal split in line with its muscle fibers. However, the surgeon must remain hyper-vigilant; excessive medial or aggressive blunt retraction can stretch or transect the accessory nerve or its arborizing branches, leading to catastrophic trapezius palsy and scapular winging.

Conversely, accessing the spinoglenoid notch openly necessitates a deltoid-splitting approach. This interval is fraught with danger due to the proximity of the axillary nerve. The axillary nerve exits the quadrangular space and courses transversely across the deep surface of the deltoid, typically 5 to 7 cm distal to the lateral edge of the acromion. A deltoid split that propagates too far inferiorly places this nerve at imminent risk. It is an absolute surgical imperative to place a heavy, non-absorbable stay suture at the distal apex of the deltoid split (no more than 4-5 cm from the posterior acromion) to physically prevent inadvertent distal extension during retraction.
Exhaustive Indications and Contraindications
The decision to proceed with surgical decompression of the suprascapular nerve must be rooted in a rigorous clinical evaluation, advanced imaging, and electrodiagnostic confirmation. Surgery is rarely the first line of treatment for idiopathic or traction-related SSN neuropathy without a discrete mass. However, strict adherence to evidence-based indications ensures optimal patient outcomes and mitigates the risk of operating on confounding pathologies such as Parsonage-Turner syndrome or cervical radiculopathy.
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Paralabral Ganglion Cyst with Motor Deficit: MRI-confirmed cyst at the spinoglenoid or suprascapular notch accompanied by weakness or EMG changes. | Space-occupying lesions cause direct mechanical compression and ischemia. Decompression (and labral repair) halts Wallerian degeneration and promotes reinnervation. |
| Failure of Conservative Management: Persistent, debilitating shoulder pain and weakness refractory to 6-12 months of structured physical therapy, NSAIDs, and activity modification (in the absence of a cyst). | Indicates irreversible structural tethering (e.g., ossified TSL) or dynamic compression that cannot be overcome by scapular stabilization exercises. | |
| Massive Retracted Rotator Cuff Tear with SSN Neuropathy: Severe medial retraction of the supraspinatus causing bowstringing of the SSN. | Releasing the TSL prior to or during cuff repair mobilizes the nerve, reduces traction neuropraxia, and may improve the excursion of the supraspinatus muscle unit. | |
| Progressive Muscle Atrophy: Documented, worsening visible atrophy of the supraspinatus and/or infraspinatus fossa. | Time is muscle. Prolonged denervation leads to irreversible fatty infiltration (Goutallier stage 3 or 4), precluding functional recovery even if the nerve is eventually decompressed. | |
| Relative Contraindications | Asymptomatic Ganglion Cysts: Incidental finding on MRI without pain, weakness, or EMG abnormalities. | Many small cysts are self-limiting or asymptomatic. Surgical intervention exposes the patient to unnecessary operative risks. |
| Mild, Early Traction Neuropathy: Athletes with acute onset pain but normal strength and minimal EMG changes. | Often resolves with rest, scapular dyskinesia correction, and posterior capsule stretching. | |
| Absolute Contraindications | Parsonage-Turner Syndrome (Acute Brachial Neuritis): Sudden, severe shoulder pain followed by patchy weakness, often viral or autoimmune in origin. | This is a medical, inflammatory condition. Surgical decompression provides zero benefit and exposes the patient to surgical morbidity. |
| Cervical Radiculopathy (C5/C6): Compression at the neural foramen mimicking SSN entrapment. | Requires cervical spine intervention. Operating on the shoulder for cervical pathology is a classic diagnostic failure (Double-crush syndrome must be carefully evaluated). |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for SSN decompression is an exhaustive process that relies heavily on advanced diagnostic modalities. The clinical examination provides the initial clues: a deep, aching pain localized to the posterior or posterolateral shoulder, often exacerbated by cross-body adduction or internal rotation. Atrophy of the supraspinatus and infraspinatus (suprascapular notch entrapment) or isolated infraspinatus atrophy (spinoglenoid notch entrapment) is a late but definitive sign.

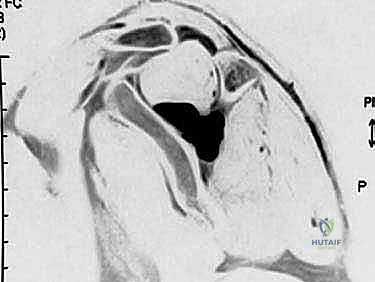
Magnetic Resonance Imaging (MRI) is the undisputed gold standard for preoperative templating. A non-contrast MRI is typically sufficient to identify paralabral ganglion cysts, which appear as multilobulated, well-circumscribed masses demonstrating low signal intensity on T1-weighted sequences and brilliantly high signal intensity on T2-weighted fluid-sensitive sequences. Crucially, the MRI must be scrutinized to identify the underlying intra-articular pathology—almost universally a superior labrum anterior-to-posterior (SLAP) tear or a posterior labral tear. The surgeon must plan to address both the cyst and the labral defect; decompressing the cyst without repairing the labral "valve" results in unacceptably high recurrence rates. Furthermore, MRI allows for the assessment of muscle viability via the Goutallier classification system, which helps set realistic postoperative expectations regarding strength recovery.
Electromyography (EMG) and Nerve Conduction Studies (NCS) are essential adjuncts, particularly in cases without a discrete mass on MRI. These studies confirm the diagnosis, localize the exact level of the lesion (suprascapular vs. spinoglenoid notch), and quantify the severity of axonal loss. Findings such as positive sharp waves, fibrillation potentials, and prolonged motor latencies confirm active denervation and solidify the indication for surgical release.
Patient Positioning Considerations
The choice of patient positioning—Beach Chair versus Lateral Decubitus—is dictated by surgeon preference, the planned approach (open vs. arthroscopic), and the necessity for concurrent intra-articular procedures.
The Beach Chair Position is highly versatile and favored for open approaches. The patient is secured at a 60- to 70-degree incline. This orientation provides an intuitive, upright anatomical perspective of the shoulder girdle. It allows for seamless conversion from an arthroscopic evaluation to an open posterior or superior approach without the need for repositioning. The arm is free-draped, enabling the surgeon to dynamically manipulate the limb through a full range of motion, which is invaluable for testing nerve tension post-release and for accessing different muscular windows. The primary anesthetic consideration is the risk of cerebral hypoperfusion; meticulous blood pressure monitoring is mandatory.
The Lateral Decubitus Position is frequently preferred by surgeons executing a purely arthroscopic decompression, particularly when extensive labral repair is anticipated. The patient is placed in the lateral position with the operative arm suspended in 10 to 15 pounds of balanced traction at approximately 45 degrees of abduction and 15 degrees of forward flexion. This traction significantly distracts the glenohumeral joint, dramatically expanding the intra-articular working space and facilitating visualization of the posterior labrum and the spinoglenoid notch via an intra-articular or subacromial perspective. However, the surgeon must be acutely aware of the risk of traction-induced neurapraxia to the brachial plexus and ensure that traction time is minimized and pressure points are rigorously padded.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of SSN decompression demands a bloodless field, precise anatomical knowledge, and meticulous tissue handling. While arthroscopic techniques have gained immense popularity for their minimally invasive nature, the open approach remains the gold standard for complex, revision, or heavily ossified cases, and serves as the foundational anatomical lesson for all shoulder surgeons.
Open Decompression of the Suprascapular Notch
With the patient in the beach chair position, the anatomical landmarks—the scapular spine, acromion, and distal clavicle—are demarcated. A saber-type skin incision is utilized, following Langer's lines to optimize the cosmetic outcome. The incision begins at the distal third of the scapular spine, coursing anteriorly over the superior aspect of the shoulder to a point roughly 2 cm medial to the acromioclavicular (AC) joint.

Following sharp dissection through the subcutaneous tissues, the thick fascia overlying the trapezius muscle is identified. A longitudinal split is made in the trapezius, strictly in line with its oblique fibers, centered over the anticipated location of the suprascapular notch (approximately 4.5 cm medial to the acromial angle). Blunt dissection using the surgeon's fingers or a periosteal elevator is employed to gently separate the muscle fibers, taking extreme care not to extend the split excessively medial, which endangers the spinal accessory nerve.

Upon retracting the trapezius, the underlying supraspinatus muscle fascia is encountered. The supraspinatus muscle belly is gently mobilized and retracted posteriorly and inferiorly using a blunt retractor (such as a Richardson or a dull Chandler retractor). Deep to the supraspinatus, a layer of fibrofatty tissue obscures the superior border of the scapula. Careful blunt dissection through this fat pad reveals the suprascapular artery, which typically runs transversely over the TSL. The artery is mobilized and protected.

The TSL is now visualized as a dense, taut band bridging the suprascapular notch. A blunt nerve hook is carefully passed beneath the TSL to definitively identify and protect the underlying suprascapular nerve. Once the nerve is visually and tactilely confirmed to be safe, the TSL is sharply transected using a #15 blade or a Kerrison rongeur if the ligament is heavily ossified. The release must be complete; the surgeon should be able to freely pass an instrument through the notch without resistance. Hemostasis is meticulously obtained, and the trapezius split is closed loosely with absorbable sutures.

Open Decompression of the Spinoglenoid Notch
For isolated spinoglenoid notch entrapment, a posterior approach is utilized. A longitudinal or slightly oblique incision is made directly over the posterior aspect of the glenohumeral joint, centered over the muscular interval between the posterior deltoid and the teres minor.
The deltoid fascia is incised, and a blunt split is created in the posterior deltoid in line with its fibers. Crucially, a stay suture is placed at the inferior apex of this split, exactly 4 cm distal to the posterior acromion, to absolutely prevent distal propagation and catastrophic injury to the axillary nerve.
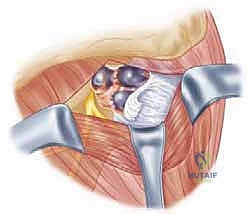
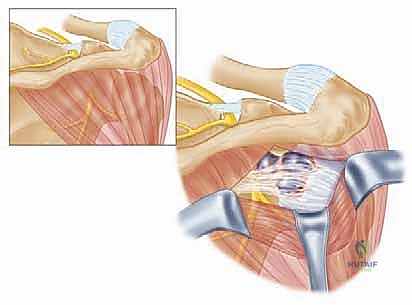
Once the deltoid is retracted, the deep fascia overlying the infraspinatus and teres minor is exposed. The interval between the infraspinatus (superiorly) and the teres minor (inferiorly) is developed. Retracting the infraspinatus superiorly exposes the posterior capsule of the glenohumeral joint and the base of the scapular spine. The spinoglenoid notch is palpated at the lateral margin of the scapular spine. If a spinoglenoid ligament is present and taut, it is carefully isolated and released. If a ganglion cyst is the source of compression, it is meticulously dissected. The cyst wall is excised, and its stalk, which invariably leads to a capsulolabral defect, is traced to the joint line. The labral tear must be repaired, often requiring the placement of suture anchors into the posterior glenoid rim to seal the one-way valve and prevent cyst recurrence.
Complications, Incidence Rates, and Salvage Management
While suprascapular nerve decompression is highly effective, it is a technically demanding procedure fraught with potential pitfalls. Complications, though relatively infrequent in experienced hands, can be devastating to shoulder function. The surgeon must be prepared to identify and manage these intraoperatively and postoperatively.
| Complication | Estimated Incidence | Mechanism & Presentation | Salvage & Management Strategy |
|---|---|---|---|
| Iatrogenic Nerve Injury (SSN) | < 1% | Direct laceration during TSL release or aggressive retraction. Presents as immediate, profound weakness post-op. | Intraoperative: Immediate microsurgical primary epineural repair. Postoperative: Observe with serial EMGs; if no recovery by 3-6 months, consider nerve grafting or tendon transfers (e.g., lower trapezius transfer). |
| Iatrogenic Axillary Nerve Injury | 1 - 2% (Open Post. Approach) | Distal extension of the deltoid split > 5cm from the acromion. Presents as deltoid atony and lateral shoulder numbness. | Prevention is key (stay sutures). If injured, early exploration and primary repair or nerve grafting within 3 months is mandated. |
| Vascular Injury / Hematoma | 2 - 5% | Laceration of the suprascapular artery or vein during notch dissection. Can lead to compressive hematoma. | Immediate intraoperative control with bipolar electrocautery, surgical clips, or suture ligation. Post-op hematomas causing acute nerve compression require immediate surgical evacuation. |
| Incomplete Decompression / Recurrence | 5 - 10% | Failure to completely transect an ossified TSL, or failure to repair the labral tear feeding a ganglion cyst. | Revision surgery. If a cyst recurs, a combined arthroscopic labral repair and open/arthroscopic cyst excision is required. Ensure complete visualization of the notch during revision. |
| Spinal Accessory Nerve Injury | < 1% | Overly aggressive medial retraction during the trapezius split. Presents as scapular winging and inability to shrug. | Difficult to repair primarily due to branching. Often requires delayed salvage procedures such as the Eden-Lange muscle transfer procedure. |

Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following SSN decompression is as critical as the surgical execution itself. The protocol must be meticulously phased to protect the surgical repair (particularly if a concurrent labral repair was performed) while preventing adhesive capsulitis and facilitating neuromuscular re-education of the chronically denervated musculature.
Phase 1: Protection and Passive Motion (Weeks 0-4)
The primary goal in the immediate postoperative period is to protect the healing tissues. If an isolated nerve decompression was performed, the patient is placed in a standard sling for comfort and may begin early passive range of motion (PROM) within 48 hours. However, if a labral repair was performed to address a ganglion cyst, the shoulder is immobilized in a sling for 4 weeks. During this phase, only restricted PROM is permitted, strictly avoiding positions that stress the labral repair (e.g., avoiding internal rotation and cross-body adduction for posterior labral repairs). Cryotherapy and non-steroidal anti-inflammatory drugs (NSAIDs) are utilized to manage inflammation.
Phase 2: Active-Assisted and Active Motion (Weeks 4-8)
As soft tissue healing progresses, the sling is discontinued. The focus shifts to restoring full, symmetric passive and active-assisted range of motion (AAROM). Scapular mobilization is initiated to correct any underlying scapular dyskinesia, which is frequently present in patients with chronic SSN neuropathy. Aquatic therapy can be highly beneficial in this phase to reduce the effects of gravity. Active range of motion (AROM) is gradually introduced as tolerated, ensuring that the patient does not develop compensatory shrug mechanics.
Phase 3: Strengthening and Neuromuscular Re-education (Weeks 8-16)
Once full, painless AROM is achieved, progressive isotonic strengthening commences. This phase is heavily focused on the rotator cuff and the periscapular stabilizers (rhomboids, levator scapulae, serratus anterior, and trapezius). Because the supraspinatus and infraspinatus may have suffered chronic denervation, strengthening must be highly specific and initiated at low resistance with high repetitions to encourage motor unit recruitment without causing fatigue-induced substitution patterns. Biofeedback and electrical stimulation may be used as adjuncts to facilitate muscle activation.
Phase 4: Return to Sport and Advanced Function (Months 4-6+)
The final phase bridges the gap between clinical rehabilitation and the functional demands of the patient's occupation or sport. Plyometric exercises, advanced proprioceptive drills, and sport-specific kinetic chain activities are integrated. Overhead athletes undergo a rigorous, interval throwing or hitting program. Return to full, unrestricted activity is permitted only when the patient demonstrates symmetric strength (at least 90% of the contralateral side on isokinetic testing), full dynamic stability, and an absence of pain during sport-specific maneuvers. It is critical to counsel patients that maximal recovery of muscle bulk and strength following severe denervation may take up to 12 to 18 months, and in cases of severe preoperative fatty infiltration, complete recovery may never be achieved.

Summary of Landmark Literature and Clinical Guidelines
The evolution of suprascapular nerve decompression is chronicled through several seminal publications that have shaped modern orthopedic practice. Koppel and Thompson (1959) provided the foundational anatomical and clinical description of suprascapular nerve entrapment at the suprascapular notch, establishing the theoretical framework for surgical release.
Ferretti et al. (1987) were instrumental in highlighting the unique vulnerability of the SSN in overhead athletes, specifically detailing the traction neuropathy seen in elite volleyball players. Their work underscored the biomechanical reality that extreme external rotation and abduction dynamically tether the nerve, leading to insidious infraspinatus atrophy.
The advent of advanced imaging revolutionized the diagnosis of space-occupying lesions. Tirman et al. (1994) definitively correlated the presence of paralabral ganglion cysts on MRI with underlying SLAP and posterior labral tears, establishing the modern paradigm that the intra-articular pathology must be addressed to prevent cyst recurrence.
More recently, the shift toward minimally invasive techniques was championed by Lafosse et al. (2007), who described a reproducible, entirely arthroscopic technique for releasing the transverse scapular ligament. This landmark paper demonstrated that arthroscopic decompression yields clinical outcomes equivalent to open techniques while significantly reducing surgical morbidity, minimizing deltoid and trapezius dissection, and allowing for concurrent management of intra-articular pathology.
