Arthroscopic Management of Biceps Tendinopathy: An Intraoperative Masterclass
Key Takeaway
This masterclass provides a comprehensive guide to arthroscopic biceps tendon treatment, from diagnosis to advanced surgical techniques. Fellows will gain insights into detailed anatomy, preoperative planning, intraoperative execution of débridement, tenotomy, and tenodesis, including critical pearls and complication management for superior patient care.
Comprehensive Introduction and Patho-Epidemiology
The management of long head of the biceps (LHB) tendinopathy represents one of the most frequently debated and dynamically evolving paradigms in contemporary orthopedic sports medicine. Historically relegated to the status of a vestigial structure—often colloquially termed the "appendix of the shoulder"—the LHB is now universally recognized as a potent pain generator and a critical component of anterior shoulder pathology. This intraoperative masterclass is designed to transcend basic surgical technique; it is a comprehensive exposition on understanding the intricate biomechanics, recognizing subtle pathoanatomy, and executing surgical interventions that optimize long-term functional outcomes for our patients.
Epidemiologically, isolated LHB pathology is a rare clinical entity, accounting for a mere fraction of shoulder presentations. The vast majority of biceps tendinopathy occurs concomitantly with broader shoulder derangements, most notably rotator cuff disease and superior labrum anterior-posterior (SLAP) lesions. The incidence of LHB pathology increases linearly with age, closely mirroring the epidemiological curve of degenerative rotator cuff tears. In the athletic population, particularly overhead throwers, LHB pathology frequently manifests as a consequence of repetitive microtrauma, subtle glenohumeral instability, or internal impingement syndromes, necessitating a highly nuanced diagnostic and therapeutic approach.
The pathophysiology of LHB tendinopathy exists along a continuum, initiating with acute tenosynovitis characterized by robust inflammatory infiltrates within the bicipital sheath, progressing to chronic tendinosis marked by mucoid degeneration, collagen disorganization, and tenocyte apoptosis. This degenerative cascade is frequently exacerbated by mechanical entrapment within the bicipital groove or instability secondary to pulley complex incompetence. Vascular studies have identified a critical watershed zone within the intra-articular portion of the tendon, predisposing this specific segment to ischemic degeneration and subsequent mechanical failure. Understanding this continuum is paramount, as the histopathological state of the tendon directly dictates the optimal surgical intervention.
Furthermore, the concept of the "hidden lesion" of the biceps cannot be overstated. A significant portion of the LHB resides extra-articularly within the intertubercular groove, rendering it invisible to standard intra-articular arthroscopic visualization. Pathology localized to this concealed segment—such as distal tendinosis, partial tearing, or entrapment—can easily be missed if the surgeon fails to dynamically evaluate the tendon by actively pulling it into the glenohumeral joint during diagnostic arthroscopy. Failure to address these hidden lesions is a primary etiology of persistent postoperative anterior shoulder pain following otherwise successful rotator cuff repairs.
Detailed Surgical Anatomy and Biomechanics
Origin, Course, and the Biceps Pulley Complex
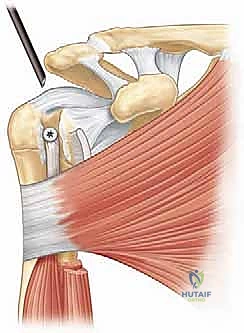
The anatomical journey of the long head of the biceps brachii is uniquely complex, dictating its susceptibility to varied pathological states. The LHB originates from the supraglenoid tubercle and the superior aspect of the glenoid labrum. Anatomical studies demonstrate significant variability in this origin, with the tendon frequently bifurcating to attach to both the anterior and posterior aspects of the superior labrum. From its origin, the tendon courses intra-articularly but extrasynovially, traversing an oblique path across the humeral head for an average distance of 35 to 55 millimeters before exiting the glenohumeral joint and entering the bicipital groove.

At the critical juncture where the LHB exits the joint, it is stabilized by the biceps pulley complex, a highly sophisticated capsuloligamentous sling. This complex is primarily composed of the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the superior-most fibers of the subscapularis tendon. The SGHL and CHL form a U-shaped sling that envelopes the biceps tendon, providing vital medial and anterior stability. The deep fibers of the CHL intertwine with the supraspinatus and subscapularis, creating a dynamic tensioning system. Disruption of this pulley complex, frequently associated with subscapularis or supraspinatus tears, inevitably leads to medial subluxation or frank dislocation of the LHB, precipitating severe mechanical attrition and tendinopathy.
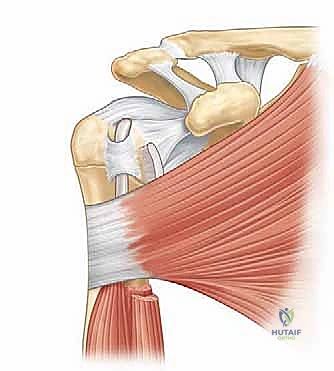
The Intertubercular Groove and Biomechanical Function
The bicipital groove, bordered medially by the lesser tuberosity and laterally by the greater tuberosity, serves as the extra-articular conduit for the LHB. The morphometry of this groove is highly variable and clinically significant. Averaging approximately 5 centimeters in length, the groove is widest at its proximal entrance (9-12 mm) but narrows significantly in its midportion (mean width 6.2 mm). This morphological bottleneck is the anatomical basis for the "hourglass biceps" phenomenon, wherein a hypertrophic, degenerated intra-articular tendon becomes mechanically incarcerated at the proximal groove entrance during arm elevation, causing distinct mechanical popping and severe pain.

The biomechanical role of the LHB remains a subject of intense academic scrutiny. While its function as an elbow flexor and forearm supinator is well established, its contribution to glenohumeral kinematics is fiercely debated. Electromyographic and cadaveric studies suggest that the LHB acts as a dynamic humeral head depressor, particularly in the setting of rotator cuff deficiency, and provides subtle anterior stability to the glenohumeral joint during the late cocking phase of throwing. However, other in vivo kinematic studies argue that its stabilizing role is negligible in the presence of an intact rotator cuff. Despite this debate, the consensus remains that a pathologically altered LHB loses any beneficial biomechanical function and transitions purely into a source of nociception and mechanical dysfunction.
Exhaustive Indications and Contraindications
The decision matrix for managing LHB pathology requires a meticulous synthesis of patient demographics, functional demands, structural pathology, and concomitant shoulder derangements. The fundamental surgical debate centers on the choice between biceps tenotomy and biceps tenodesis. Both procedures yield high rates of patient satisfaction and pain relief, yet they possess distinct biomechanical and cosmetic implications that must be tailored to the individual patient.
Simple debridement of the LHB is rarely indicated as a standalone procedure. It is generally reserved for minor fraying (less than 25% of the tendon diameter) in the setting of a stable pulley complex. Once structural compromise exceeds 25% to 50% of the tendon cross-sectional area, or if there is overt instability, subluxation, or a clear "hourglass" entrapment, definitive management via tenotomy or tenodesis is mandated. Leaving a significantly diseased tendon in situ, even after extensive debridement, is a well-documented cause of surgical failure and persistent postoperative pain.
Biceps tenotomy is highly effective, technically straightforward, and avoids the risks associated with implant fixation. It is generally the procedure of choice for elderly, low-demand patients, those with massive, irreparable rotator cuff tears, or patients with significant medical comorbidities where minimizing operative time is critical. However, tenotomy carries a known risk of the "Popeye" deformity (distal migration of the biceps muscle belly), subjective fatigue cramping in the biceps during repetitive use, and a mild, often subclinical, decrease in peak supination strength.
Conversely, biceps tenodesis aims to restore the resting length-tension relationship of the biceps muscle, thereby mitigating the risk of cosmetic deformity and fatigue cramping. Tenodesis is strongly indicated in younger, active patients, manual laborers, athletes, and individuals who express significant concern regarding postoperative cosmesis. Contraindications to tenodesis include active local or systemic infection, profound osteopenia that precludes secure implant fixation, or a patient who is unable or unwilling to comply with the requisite postoperative rehabilitation protocol.
| Surgical Intervention | Primary Indications | Relative Contraindications | Key Advantages | Key Disadvantages |
|---|---|---|---|---|
| Biceps Tenotomy | Elderly patients (>65 yrs); Low functional demand; Massive irreparable cuff tears; Non-compliance with rehab; Severe osteopenia. | Young, active patients; Manual laborers; High cosmetic concern; Pre-existing biceps cramping. | Technically simple; No implant cost/risk; Rapid recovery; Excellent pain relief. | High rate of "Popeye" deformity; Risk of fatigue cramping; Slight loss of supination strength. |
| Suprapectoral Tenodesis | Active patients (<65 yrs); Concomitant arthroscopic procedures; Desire to maintain cosmesis and strength. | Severe groove comminution; Distal biceps pathology extending past the groove. | Maintains length-tension; Avoids Popeye deformity; All-arthroscopic technique. | Risk of persistent groove pain; Implant-related complications; Technically demanding. |
| Subpectoral Tenodesis | Revision tenodesis; Extensive distal tendon pathology; "Hourglass" biceps with severe groove stenosis. | High risk of neurovascular injury (if anatomy distorted); Bleeding diathesis. | Removes tendon entirely from groove; Excellent biomechanical fixation. | Requires open incision; Risk to musculocutaneous nerve; Longer surgical time. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Advanced Imaging
Meticulous preoperative planning begins with a comprehensive clinical evaluation. Patients typically present with insidious, poorly localized anterior shoulder pain that frequently radiates distally along the anterior brachium. The pain is characteristically exacerbated by overhead activities, lifting, and resisted supination. While physical examination maneuvers such as Speed's test, Yergason's test, and the active compression (O'Brien's) test are routinely utilized, the astute clinician must recognize their inherent limitations. The sensitivity and specificity of these tests are notoriously variable, largely due to the high prevalence of concomitant rotator cuff and labral pathology that confounds the clinical picture.

Advanced imaging is critical for definitive preoperative templating. Magnetic Resonance Imaging (MRI), particularly non-contrast high-resolution 3-Tesla scans, provides unparalleled soft tissue detail. Axial and oblique sagittal sequences are paramount for evaluating the integrity of the biceps pulley complex, assessing for LHB subluxation, and identifying tenosynovitis or peritendinous effusion within the bicipital groove. Furthermore, MRI allows for the critical assessment of concomitant subscapularis and supraspinatus tears, which directly dictate the surgical approach.
Ultrasound has emerged as a highly valuable, dynamic imaging modality in the hands of an experienced musculoskeletal ultrasonographer. It allows for real-time assessment of LHB stability during active internal and external rotation of the shoulder. Ultrasound is exquisitely sensitive for detecting peritendinous fluid, tendon subluxation, and complete ruptures. Furthermore, ultrasound-guided diagnostic injections of local anesthetic into the bicipital sheath can definitively isolate the LHB as the primary pain generator, providing invaluable diagnostic clarity prior to surgical intervention.
Patient Positioning and Operating Room Setup
The choice of patient positioning—beach-chair versus lateral decubitus—is largely dictated by surgeon preference and the nature of concomitant procedures, but both require exactness to optimize visualization and minimize complications. For arthroscopic LHB management, the beach-chair position is frequently preferred as it provides an anatomical orientation that facilitates both intra-articular evaluation and seamless conversion to an open subpectoral approach if required.

When utilizing the beach-chair position, the patient is secured in a semi-recumbent posture at approximately 45 to 60 degrees of elevation. Meticulous attention must be paid to head and neck positioning to prevent catastrophic neurological complications. The cervical spine must be maintained in a neutral position, avoiding excessive flexion, extension, or lateral deviation, which can precipitate brachial plexus traction injuries or compromise cerebral perfusion. The operative arm is placed in a pneumatic or mechanical articulating arm holder, allowing the surgeon to dynamically control rotation, forward flexion, and traction throughout the procedure.
If the lateral decubitus position is selected, the patient is secured with a vacuum beanbag, and the operative arm is suspended utilizing a sterile traction apparatus. Typically, 10 to 15 pounds of traction is applied at an angle of 45 degrees of abduction and 15 degrees of forward flexion. While this position provides excellent distraction of the glenohumeral joint for labral work, it distorts the normal anatomical relationship of the anterior shoulder structures, making evaluation of LHB tracking and subpectoral exposures slightly more challenging. Regardless of the position chosen, all bony prominences must be rigorously padded, and a thorough examination under anesthesia (EUA) should be performed prior to sterile draping to assess baseline range of motion and glenohumeral stability.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Tendon Evaluation
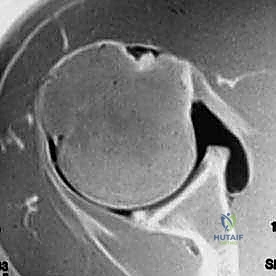
The surgical execution commences with a systematic diagnostic arthroscopy. A standard posterior viewing portal is established, and a 30-degree arthroscope is introduced into the glenohumeral joint. A thorough, reproducible sweep of the joint is mandatory, evaluating the articular cartilage, labrum, capsular ligaments, and the articular surface of the rotator cuff. The LHB is identified at its origin on the supraglenoid tubercle.
Crucially, the intra-articular portion of the LHB visible from the posterior portal represents only a fraction of the tendon. To evaluate for "hidden lesions," an anterior working portal (typically an anterosuperior or mid-anterior portal) is established under direct localization. A calibrated arthroscopic probe is introduced, and the LHB is actively grasped and pulled intra-articularly. This maneuver allows the surgeon to inspect the portion of the tendon that normally resides within the proximal bicipital groove. The tendon is meticulously evaluated for erythema, severe fraying, partial tearing, or the classic hourglass hypertrophy. Concurrently, the integrity of the superior subscapularis and the SGHL/CHL pulley complex is probed to assess for occult instability.

Execution of Biceps Tenotomy
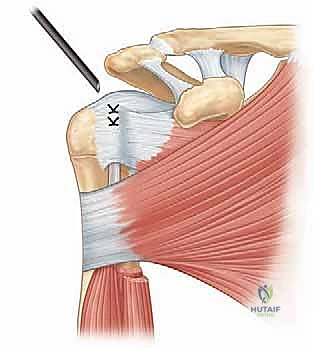
If the preoperative plan and intraoperative findings dictate a biceps tenotomy, the procedure is executed rapidly and efficiently. Utilizing the anterior working portal, an arthroscopic basket punch, motorized shaver, or radiofrequency ablation wand is introduced. The LHB is transected as close to its superior labral origin as possible to minimize the residual stump, which can act as a mechanical irritant.
It is imperative to ensure a clean, complete release of the tendon. Following transection, the proximal stump is carefully debrided back to a stable rim using a motorized shaver to prevent postoperative catching or impingement against the humeral head. The distal portion of the transected tendon typically retracts distally into the bicipital groove. In cases of severe groove stenosis, the tendon may not retract fully; in such instances, pushing the tendon distally into the groove with a probe ensures it clears the intra-articular space.
Arthroscopic Suprapectoral Tenodesis Technique
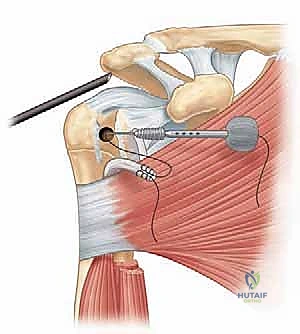
For patients requiring tenodesis, the arthroscopic suprapectoral technique offers robust fixation while maintaining an all-arthroscopic environment. After diagnostic evaluation, the LHB is tagged intra-articularly to maintain control. A spinal needle is utilized to percutaneously localize the ideal trajectory for an accessory anterolateral portal, aiming directly at the bicipital groove.

Once the portal is established, the transverse humeral ligament is released utilizing a radiofrequency wand, unroofing the proximal bicipital groove. The LHB is exteriorized or mobilized, and a high-strength suture is passed through the tendon utilizing a penetrator or lasso technique. The tendon is then transected proximally at the labral origin.
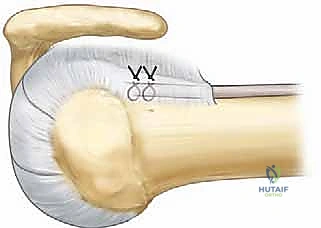
Preparation of the bony bed is a critical step. The bicipital groove is decorticated using a motorized burr to expose a bleeding cancellous bone bed, optimizing the biological environment for tendon-to-bone healing. A pilot hole is drilled at the apex of the groove, typically utilizing a reamer that matches the diameter of the chosen interference screw (commonly 7 to 9 mm).
The tagged LHB is then reduced into the prepared bony socket. Maintaining appropriate tension on the traction sutures, a bio-composite or PEEK interference screw is advanced over a guide pin, securing the tendon within the socket. The surgeon must meticulously monitor the tension of the tendon during screw insertion to ensure the physiological length-tension relationship is restored. Once secure fixation is achieved, the excess proximal tendon is excised flush with the articular margin using a shaver or radiofrequency device.
Complications, Incidence Rates, and Salvage Management
While arthroscopic management of LHB tendinopathy is generally highly successful, it is not devoid of complications. A profound understanding of these potential pitfalls is essential for both preoperative patient counseling and intraoperative risk mitigation. The most frequently cited complication following simple tenotomy is the "Popeye" deformity, a cosmetic alteration resulting from the distal retraction of the biceps muscle belly. The incidence of this deformity is highly variable in the literature, ranging from 3% to 70%, largely dependent on patient body habitus and the specific criteria used for evaluation. While often asymptomatic, it can be a source of significant dissatisfaction in cosmetically sensitive individuals.
Following tenodesis, the most common complication is persistent pain at the bicipital groove. This can occur in up to 10% to 15% of suprapectoral tenodesis cases and is often attributed to residual tenosynovitis of the tendon segment remaining within the distal groove, or inadequate resection of the proximal tendon stump. Implant-related complications, including interference screw pullout, fracture of the proximal humerus (particularly if the cortical socket is oversized), and foreign body reactions to bioabsorbable materials, are rare but devastating when they occur.
Neurovascular injury is a critical concern, particularly when converting to an open subpectoral approach. The musculocutaneous nerve, which innervates the biceps and brachialis muscles, courses dangerously close to the medial border of the biceps muscle belly. Aggressive medial retraction during a subpectoral exposure can cause neuropraxia or structural injury to this nerve. Similarly, aberrant portal placement during arthroscopic suprapectoral techniques can endanger the axillary nerve or the cephalic vein.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| "Popeye" Deformity | 10% - 40% (Tenotomy); <2% (Tenodesis) | Distal retraction of muscle belly; Failure of tenodesis implant. | Reassurance (if asymptomatic); Revision open subpectoral tenodesis (if symptomatic/acute). |
| Persistent Groove Pain | 5% - 15% (Suprapectoral) | Retained diseased tendon in groove; Inadequate decortication; Implant reaction. | Corticosteroid injection; Revision to open subpectoral tenodesis (removing tendon from groove). |
| Fatigue Cramping | 15% - 25% (Tenotomy) | Loss of physiological length-tension relationship. | Physical therapy; Activity modification; Rarely requires surgical revision. |
| Hardware Failure / Pullout | 1% - 3% | Poor bone quality (osteopenia); Undersized interference screw; Aggressive early rehab. | Revision tenodesis utilizing a cortical button or dual-fixation technique. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be meticulously tailored to the specific surgical intervention performed—tenotomy versus tenodesis—as well as any concomitant procedures, such as rotator cuff repair. The primary objective of rehabilitation following a tenodesis is to protect the structural integrity of the tendon-to-bone repair during the initial phases of biological healing, while sequentially restoring range of motion and functional strength.
Phase I: Protection and Early Motion (Weeks 0-4)
Following a tenodesis, the patient is placed in a standard shoulder sling for 4 weeks. The paramount restriction during this phase is the absolute avoidance of active elbow flexion and active forearm supination, as these motions generate direct tensile forces across the repair site. Rehabilitation focuses on passive range of motion (PROM) of the shoulder to prevent adhesive capsulitis. Pendulum exercises, passive forward elevation, and passive external rotation are initiated immediately. Active hand, wrist, and cervical spine motion are encouraged to promote vascular flow and prevent distal stiffness.
Phase II: Active-Assisted and Active Motion (Weeks 4-8)
At the 4-week mark, the sling is discontinued. The patient transitions from passive to active-assisted range of motion (AAROM) and subsequently to active range of motion (AROM) of the shoulder. Gentle, active elbow flexion and supination are introduced, but strictly without resistance. The focus is on normalizing scapulohumeral rhythm and achieving full, symmetrical active elevation. Submaximal, pain-free isometric exercises for the rotator cuff and periscapular stabilizers are initiated.
Phase III: Progressive Strengthening (Weeks 8-12)
Once full, pain-free AROM is achieved and initial biological healing of the tenodesis site is established (typically around 8 weeks), progressive resistive exercises are introduced. Isotonic strengthening of the biceps and brachialis begins with light weights and high repetitions. Rotator cuff strengthening is advanced using resistance bands and light dumbbells. Closed kinetic chain exercises are incorporated to enhance proprioception and dynamic stability.
Phase IV: Return to Sport and High-Level Function (Weeks 12+)
The final phase focuses on sport-specific or occupation-specific functional training. Plyometric exercises, advanced dynamic stabilization drills, and progressive interval throwing programs (for overhead athletes) are implemented. Return to unrestricted heavy lifting, manual labor, or contact sports is generally permitted between 4 and 6 months postoperatively, contingent upon the patient achieving at least 90% strength symmetry compared to the contralateral limb and demonstrating an absence of pain with provocative testing. For patients who underwent a simple tenotomy without concomitant repair, the protocol is significantly accelerated, with active motion and strengthening initiated as tolerated by pain, often returning to full activity within 6 to 8 weeks.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of LHB tendinopathy is supported by a robust, albeit sometimes conflicting, body of orthopedic literature. The foundational debate between tenotomy and tenodesis has been the subject of numerous prospective
