Supramalleolar Osteotomy: An Intraoperative Masterclass for Ankle Deformity Correction

Key Takeaway
This masterclass provides an immersive, step-by-step guide to supramalleolar osteotomy. We cover preoperative planning, patient positioning, comprehensive surgical anatomy, and meticulous intraoperative execution, including fibular and tibial osteotomies. Learn critical pearls, potential pitfalls, and strategies for optimal fixation and postoperative rehabilitation to correct ankle malalignment and restore joint congruity.
Comprehensive Introduction and Patho-Epidemiology
Supramalleolar osteotomy (SMOT) represents a precise, technically demanding, and joint-preserving surgical intervention designed to normalize altered load distribution across the tibiotalar articulation. Unlike the knee or hip, where primary osteoarthritis is predominantly driven by intrinsic cartilaginous degeneration and genetic predispositions, osteoarthritis of the ankle is overwhelmingly post-traumatic in etiology. It frequently manifests secondary to malunited fractures of the tibial plafond, distal tibial shaft, or fibula, as well as chronic ligamentous instability leading to asymmetric loading. The primary objective of SMOT is not merely the mechanical realignment of osseous structures, but the restoration of biomechanical harmony, the mitigation of progressive cartilage degradation, and the alleviation of debilitating pain, thereby delaying or entirely circumventing the need for end-stage salvage procedures such as ankle arthrodesis or total ankle arthroplasty (TAA).

The patho-epidemiology of ankle osteoarthritis dictates that even minor angular deviations in the coronal or sagittal planes drastically reduce the tibiotalar contact area. The ankle joint, characterized by its highly congruent mortise and relatively thin but dense articular cartilage, is exceptionally sensitive to mechanical axis deviations. A shift of the mechanical axis by merely a few millimeters can increase peak focal contact stresses by over 50%. Long-standing varus or valgus malalignment generates abnormal stress concentrations on specific, localized regions of the tibiotalar joint. Over time, this asymmetric loading overwhelms the chondrocytes' reparative capacity, leading to accelerated, unicompartmental cartilage wear. If left untreated, the mechanical axis deviation creates a self-propagating cycle: asymmetric wear leads to further deformity, which in turn exacerbates the focal loading, ultimately resulting in pan-articular destruction.
By definition, a supramalleolar osteotomy is executed at the metaphyseal level of the distal tibia, frequently accompanied by a concomitant fibular osteotomy, to correct angular deformities situated juxta-articularly. This intervention is primarily indicated in cases of asymmetric osteoarthritis where a viable portion of articular cartilage remains in the unloaded compartment. By shifting the mechanical axis toward the preserved cartilage—often aiming for a slight overcorrection of 3 to 5 degrees—the surgeon redistributes the weight-bearing forces. This offloading of the degenerated compartment not only provides profound symptomatic relief but can also facilitate the fibrocartilaginous resurfacing of eburnated bone, making SMOT a cornerstone in the modern orthopedic surgeon's armamentarium for joint preservation.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy of the distal lower extremity is an absolute prerequisite for the safe and efficacious execution of a supramalleolar osteotomy. The distal tibia expands into a metaphyseal flare, characterized by a thin cortical shell enveloping a dense cancellous bone network. This robust cancellous bed provides an excellent environment for osteotomy healing, particularly in opening wedge configurations. However, the anteromedial surface of the distal tibia is notoriously devoid of robust muscular coverage, lying directly deep to the subcutaneous tissue and skin. This precarious soft tissue envelope necessitates meticulous handling to prevent wound dehiscence and deep infection. The vascular supply to the distal tibia is primarily derived from the anterior tibial, posterior tibial, and peroneal arteries, with the periosteal network playing a critical role in cortical perfusion. Consequently, subperiosteal dissection must be strictly limited to the planned osteotomy site to preserve the osteogenic potential of the bone.
The fibula and the distal tibiofibular syndesmosis are integral to ankle biomechanics and must be meticulously managed during SMOT. The syndesmosis—comprising the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the interosseous ligament, and the transverse ligament—maintains the integrity of the ankle mortise. When correcting significant coronal plane deformities, particularly valgus deformities requiring a lateral closing wedge tibial osteotomy, the fibula acts as a lateral strut that will tether the correction if not addressed. Therefore, a fibular osteotomy is frequently mandatory to allow the distal tibial articular surface to tilt into the desired alignment without disrupting the syndesmotic relationship or causing subluxation of the talus within the mortise.
Neurologically, several critical structures traverse the operative field. The superficial peroneal nerve pierces the deep fascia in the middle to distal third of the lateral leg and bifurcates into the medial and intermediate dorsal cutaneous nerves, crossing the anterolateral aspect of the ankle. During anterior or lateral approaches, these branches are highly susceptible to iatrogenic injury, either from direct transection or aggressive retraction. The sural nerve and the short saphenous vein course posterolaterally and must be protected during fibular osteotomies. Biomechanically, the surgeon must accurately identify the Center of Rotation of Angulation (CORA). If the osteotomy is performed exactly at the CORA, pure angular correction is achieved without translation. However, anatomical constraints often dictate that the osteotomy be performed proximal to the CORA (e.g., at the metaphyseal flare rather than intra-articularly). In such instances, the surgeon must calculate and execute an intentional translation of the distal fragment to ensure the mechanical axis is accurately restored to the center of the ankle joint.
Exhaustive Indications and Contraindications
The success of a supramalleolar osteotomy is entirely predicated on rigorous patient selection. The ideal candidate is a physiologically young, active patient presenting with symptomatic, unicompartmental ankle osteoarthritis secondary to a juxta-articular angular deformity. The presence of at least 50% preserved cartilage in the contralateral compartment (e.g., preserved lateral cartilage in a varus ankle) is the sine qua non for this procedure. The osteotomy serves to transfer the mechanical load from the arthritic compartment to the preserved compartment. Furthermore, SMOT is highly effective for correcting post-traumatic malunions of the distal tibia and fibula prior to the onset of frank osteoarthritis, acting as a prophylactic measure against future joint degeneration.
Conversely, symmetric or pan-articular, end-stage osteoarthritis is an absolute contraindication to SMOT, as there is no healthy cartilage available to accept the transferred load. In such scenarios, arthrodesis or total ankle arthroplasty are the appropriate interventions. Systemic conditions that severely compromise bone healing or soft tissue viability, such as uncontrolled diabetes mellitus, profound peripheral vascular disease, or active osteomyelitis, preclude the use of osteotomies. Neuropathic arthropathy (Charcot joint) is a strict contraindication due to the high risk of nonunion, hardware failure, and progressive deformity. Additionally, uncorrectable hindfoot or midfoot deformities that drive the ankle pathology must be addressed; an isolated SMOT will fail if the primary deforming force originates distally (e.g., a rigid, forefoot-driven hindfoot varus).
| Category | Indications for Supramalleolar Osteotomy | Contraindications for Supramalleolar Osteotomy |
|---|---|---|
| Articular Status | Asymmetric (unicompartmental) ankle osteoarthritis; Preserved cartilage in the compartment to be loaded. | Symmetric, pan-articular, or end-stage osteoarthritis (Kellgren-Lawrence Grade IV globally). |
| Deformity Type | Post-traumatic malunion of the distal tibia/fibula; Congenital angular deformities; Juxta-articular varus or valgus. | Severe, uncorrectable multiplanar deformities requiring intra-articular osteotomy; Forefoot-driven deformities not addressed concomitantly. |
| Bone & Soft Tissue | Good bone stock capable of supporting internal fixation; Adequate soft tissue envelope for incisional healing. | Severe osteoporosis; Active local or systemic infection; Compromised soft tissue envelope (e.g., severe venous stasis, prior radiation). |
| Systemic/Patient Factors | Physiologically young, active patients; Compliant with non-weight-bearing protocols. | Neuropathic arthropathy (Charcot); Uncontrolled diabetes mellitus; Severe peripheral vascular disease; Active tobacco use (relative/absolute depending on severity). |
| Joint Stability | Stable or correctable ligamentous instability (can be addressed simultaneously). | Uncorrectable, profound neuromuscular imbalance (e.g., severe spasticity or flaccid paralysis). |
Pre-Operative Planning, Templating, and Patient Positioning
Before an incision is made, meticulous preoperative planning and templating are paramount. The surgeon must define the problem, quantify the magnitude of the deformity in all three planes, and mathematically design the surgical solution. Clinical examination begins with a comprehensive assessment of the entire lower extremity mechanical axis, ruling out ipsilateral knee or hip deformities that could masquerade as, or contribute to, ankle malalignment. Ligamentous stability is evaluated via anterior drawer and talar tilt tests; chronic lateral ligamentous instability frequently accompanies long-standing varus deformities and may require concomitant lateral ligament reconstruction (e.g., Modified Broström-Gould) to ensure the longevity of the osteotomy. The Coleman block test is indispensable for evaluating varus hindfoot deformities; it differentiates a flexible, forefoot-driven varus (which corrects when the first ray is allowed to plantarflex off the block) from a rigid, structural hindfoot varus.


Imaging is the cornerstone of templating. Standard, bilateral, full weight-bearing anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory. A Saltzman hindfoot alignment view is critical for quantifying the relationship between the tibial axis and the calcaneal tuberosity. Full-length standing lower extremity radiographs are essential if there is any clinical suspicion of proximal mechanical axis deviation. Advanced imaging, such as CT or SPECT-CT, is highly recommended to assess the precise location and extent of osteochondral lesions, the presence of subchondral cysts, and the true three-dimensional geometry of the deformity. SPECT-CT, in particular, provides a functional metabolic map of the joint, highlighting areas of active subchondral stress and guiding the surgeon in determining the exact degree of offloading required.

Templating involves measuring the Tibiotalar Angle (TAS) and the Tibial Lateral Surface Angle (TLS). To determine the exact size of the wedge to be inserted (opening wedge) or excised (closing wedge), the surgeon utilizes the trigonometric formula: $/tan(/theta) = H/W$, where $/theta$ is the desired angle of correction, $H$ is the height of the wedge base in millimeters, and $W$ is the width of the tibia at the planned osteotomy level. For asymmetric osteoarthritis, clinical evidence strongly supports planning for an overcorrection of 3 to 5 degrees into the opposite alignment (e.g., correcting a varus ankle to 3-5 degrees of valgus) to ensure adequate mechanical offloading of the diseased cartilage.
Patient positioning is entirely dictated by the planned surgical approach. For a medial opening wedge osteotomy (typically utilized for varus deformities), the patient is positioned supine on a radiolucent operating table. A small bump is placed under the ipsilateral hip to prevent external rotation, and a sandbag is placed under the calf to slightly flex the knee, thereby relaxing the gastrocnemius-soleus complex and presenting the medial tibia optimally. Conversely, for a lateral closing wedge osteotomy (frequently employed for substantial valgus deformities), the patient may be positioned in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg, providing unimpeded access to the lateral fibula and anterolateral tibia. A pneumatic tourniquet is routinely applied to the proximal thigh to ensure a bloodless surgical field.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a supramalleolar osteotomy demands precision, respect for soft tissues, and rigorous adherence to the preoperative template. The technique varies significantly depending on whether a lateral closing wedge or a medial opening wedge is selected.
Lateral Closing Wedge Osteotomy for Valgus Deformity
For valgus deformities, a lateral closing wedge osteotomy of the tibia is often preferred, particularly when the deformity exceeds 10 degrees, as an excessively large medial opening wedge can lead to soft tissue tensioning issues and delayed union.
Fibular Osteotomy and Syndesmotic Management:
The procedure typically begins with the fibula. An incision is made along the anterior margin of the distal fibula. Meticulous dissection is required to identify and protect the superficial peroneal nerve anteriorly and the sural nerve posteriorly. The fibula must be shortened to accommodate the lateral closing wedge of the tibia and prevent tethering of the correction. A Z-shaped osteotomy is biomechanically superior to a simple transverse cut, as it provides innate rotational stability and a larger surface area for healing.


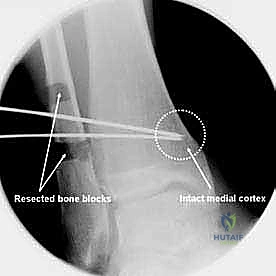
Kirschner wires are placed to mark the planned transverse cuts, typically 2 to 3 cm in length, starting just proximal to the anterior syndesmosis. The proximal transverse cut is directed anteriorly, and the distal cut posteriorly, to avoid the dense syndesmotic ligaments. After completing the longitudinal connecting cut with an oscillating saw, precisely measured bone blocks (calculated from the preoperative template) are resected from both ends of the Z. The fibula is not immediately fixed; it is left mobile to allow for the tibial correction.
Tibial Osteotomy Execution:
Attention is then turned to the lateral tibia. An anterolateral approach is utilized, developing the interval between the tibialis anterior and the extensor hallucis longus. Two Kirschner wires are placed under fluoroscopic guidance to define the osteotomy planes. The wires are directed from the lateral cortex, converging exactly at the medial cortex, which will serve as the intact plastic hinge.
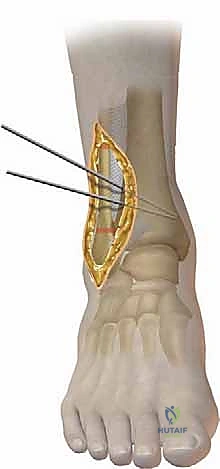
The angle between these wires corresponds exactly to the planned wedge angle. Using a saw, the bone between the wires is carefully resected. The medial cortex must be meticulously preserved to maintain stability and act as a fulcrum. Once the wedge is removed, the osteotomy is slowly closed by applying varus force to the foot. The fibular osteotomy is then reduced, and both the tibia and fibula are rigidly fixed using anatomically contoured locking plates.
Medial Opening Wedge Osteotomy for Varus Deformity
For varus deformities, the medial opening wedge osteotomy is highly favored due to its relative simplicity, avoidance of limb shortening, and excellent healing rates in the metaphyseal cancellous bone.
Surgical Approach and Osteotomy:
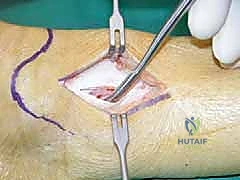
A longitudinal incision is made over the medial aspect of the distal tibia, taking care to protect the saphenous vein and nerve. The periosteum is incised longitudinally and elevated minimally to expose the planned osteotomy site, typically 3 to 4 cm proximal to the tibial plafond. A guide wire is drilled from medial to lateral, aiming for the lateral cortex just proximal to the syndesmosis. A second wire can be placed parallel to the first to guide the saw blade.


The osteotomy is initiated with an oscillating saw and completed with sharp osteotomes to prevent thermal necrosis and ensure the lateral cortical hinge remains intact. The osteotomy is then gradually and carefully opened using a combination of osteotomes and a specialized lamina spreader. Rapid or forceful opening can result in a catastrophic fracture of the lateral hinge, converting a stable osteotomy into an unstable construct requiring significantly more robust fixation.


Internal Fixation Strategies and Bone Grafting
Once the desired correction is achieved and verified via multi-planar intraoperative fluoroscopy (confirming the mechanical axis now passes through the desired portion of the talar dome), the defect must be stabilized and filled.


For structural support in opening wedges, a tricortical iliac crest autograft is the gold standard, though structurally sound allografts (e.g., femoral head or precisely milled allograft wedges) are increasingly utilized to avoid donor site morbidity. The graft is tamped into the defect, ensuring it sits flush with the medial cortex.


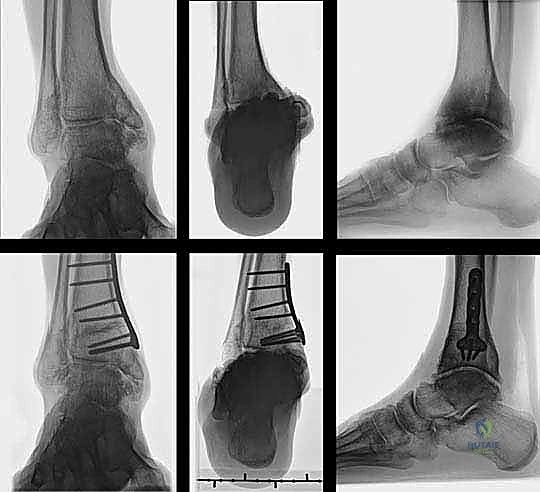
Fixation is achieved utilizing a pre-contoured, low-profile medial distal tibia locking plate. The plate functions as an internal fixator, neutralizing bending and torsional forces while the osteotomy heals. Locking screws are placed in the distal fragment (the epiphysis/metaphysis) and the proximal diaphyseal fragment. Compression across the osteotomy is generally not desired in an opening wedge; rather, the plate acts in a bridging capacity to maintain the structural integrity of the graft and the corrected alignment.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and execution, supramalleolar osteotomies carry a distinct complication profile. The surgeon must be prepared to identify and manage these issues promptly to prevent catastrophic failure of the joint preservation effort. The most critical intraoperative complication is the inadvertent fracture of the contralateral cortical hinge. If the lateral hinge fractures during a medial opening wedge, the construct loses its inherent stability, risking translation, rotation, and loss of the coronal correction. This necessitates immediate intraoperative revision, typically requiring the addition of a lateral plate or the use of a more robust, multi-planar external fixator to stabilize the now-complete osteotomy.
Postoperatively, delayed union and nonunion are the most concerning osseous complications, particularly in opening wedge osteotomies where a large gap must be bridged by bone graft. The incidence of nonunion ranges from 2% to 7%, heavily influenced by patient factors such as smoking, diabetes, and the use of allograft versus autograft. Soft tissue complications, including wound dehiscence and superficial infection, are relatively common (up to 10%) due to the tenuous vascularity of the anteromedial distal tibia. Deep infections are rare but devastating, often requiring hardware removal, aggressive debridement, and conversion to external fixation.

Under-correction or over-correction represents a failure of preoperative planning or intraoperative execution. Under-correction fails to offload the arthritic compartment, leading to persistent pain and continued joint degeneration. Severe over-correction can induce iatrogenic arthritis in the previously healthy compartment. In cases of progressive, symptomatic failure of the osteotomy, salvage management is required. The primary salvage options are ankle arthrodesis or total ankle arthroplasty (TAA). Notably, a prior SMOT does not necessarily preclude a subsequent TAA; in fact, by restoring the mechanical axis, a well-healed SMOT may optimize the local anatomy for a future joint replacement, making the primary osteotomy a valuable "buying time" procedure.
| Complication Type | Specific Complication | Estimated Incidence | Management / Salvage Strategy |
|---|---|---|---|
| Intraoperative | Cortical Hinge Fracture | 5% - 10% | Immediate stabilization with contralateral plating or robust external fixation; conversion to complete osteotomy rules. |
| Intraoperative | Neurovascular Injury (e.g., Superficial Peroneal Nerve) | 1% - 3% | Primary micro-surgical repair if recognized; post-op management with neuromodulators; prevention via meticulous dissection is key. |
| Postoperative (Early) | Wound Dehiscence / Superficial Infection | 5% - 10% | Local wound care, oral or IV antibiotics; rarely requires surgical debridement if hardware is not exposed. |
| Postoperative (Late) | Delayed Union / Nonunion | 2% - 7% | Prolonged non-weight-bearing; bone stimulators; revision surgery with autogenous bone grafting and hardware exchange. |
| Postoperative (Late) | Under-correction / Recurrent Deformity | 3% - 8% | Revision osteotomy if cartilage remains viable; conversion to Ankle Arthrodesis or Total Ankle Arthroplasty (TAA) if joint is destroyed. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a supramalleolar osteotomy is a protracted and meticulously phased process, requiring strict patient compliance to ensure optimal osseous union and functional recovery. The protocol must balance the need for early mobilization to prevent joint stiffness with the absolute necessity of protecting the osteotomy site from premature mechanical loading.
Phase I: Immediate Postoperative Period (Weeks 0-2)
Immediately following surgery, the patient is placed in a bulky, well-padded posterior splint and maintained in a strict non-weight-bearing (NWB) status. Elevation of the limb above the level of the heart is critical during the first 72 to 96 hours to mitigate edema, which is a primary driver of early wound complications. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk factors. At the two-week mark, sutures are removed, and the surgical wounds are assessed.
Phase II: Early Mobilization and Protection (Weeks 2-6)
If the wounds are healing satisfactorily, the patient is transitioned to a removable controlled ankle motion (CAM) boot. The patient remains strictly non-weight-bearing. However, they are instructed to remove the boot multiple times daily to perform active and active-assisted range of motion (ROM) exercises for the ankle and subtalar joints. This early mobilization is vital for cartilage nutrition, preventing capsular contracture, and optimizing the gliding planes of the extensor and flexor tendons.
Phase III: Progressive Weight-Bearing (Weeks 6-12)
At the six-week postoperative milestone, weight-bearing radiographs are obtained to assess the progression of osseous union. If radiographic evidence of bridging callus is present, and the patient is clinically non-tender at the osteotomy site, a progressive weight-bearing protocol is initiated. The patient begins with partial weight-bearing (e.g., 25% of body weight) in the CAM boot, utilizing crutches. Weight-bearing is advanced by 25% weekly, as tolerated, until full weight-bearing is achieved. Physical therapy is intensified during this phase, focusing on proprioception, intrinsic foot muscle strengthening, and normalization of the gait cycle.
Phase IV: Advanced Rehabilitation and Return to Activity (Weeks 12+)
By 12 weeks, most patients demonstrate solid clinical and radiographic union. The CAM boot is discontinued, and the patient transitions to supportive athletic footwear. Rehabilitation focuses on advanced strengthening, eccentric loading of the Achilles and peroneal tendons, and sport-specific or occupation-specific functional drills. Maximum medical improvement and final functional outcomes may not be fully realized until 12 to 18 months postoperatively, as the subchondral bone undergoes continuous remodeling in response to the newly restored mechanical axis.
Summary of Landmark Literature and Clinical Guidelines
The clinical efficacy and long-term survivorship of supramalleolar osteotomies have been rigorously validated through decades of orthopedic literature. The foundational principles of SMOT were largely established by Takakura et al. in the 1990s, who demonstrated that realigning the mechanical axis in early-stage ankle osteoarthritis could halt disease progression and stimulate fibrocartilage regeneration. Takakura's classification system for ankle osteoarthritis remains a critical tool for predicting osteotomy success; patients with stage II or IIIa disease (partial joint space narrowing with preserved cartilage in one compartment) demonstrate the highest success rates.
More contemporary, landmark prospective studies by Hintermann and Pagenstert have further refined the indications and techniques. Hintermann's long-term follow-up studies revealed that in properly selected patients, the survivorship of the native ankle joint following SMOT exceeds 85% at 10 years and approaches 75% at 15 years. These studies underscore the critical importance of achieving a slight overcorrection (3-5 degrees) to ensure adequate offloading of the degenerated compartment. Furthermore, literature highlights that concomitant procedures, such as lateral ligament reconstruction for chronic instability or gastrocnemius recession for equinus contractures, are often mandatory to achieve durable, long-term success.
Current clinical guidelines from major orthopedic foot and ankle societies strongly advocate for joint-preserving
