

Anterior Hip Mastery: Navigating Latae & Sart...
00:00
Start Quiz
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?

Explanation
Findings in patients with McCune-Albright syndrome include polyostotic fibrous dysplasia, multiple cafe-au-lait spots, and precocious puberty. The bone changes in NF-1 resemble nonossifying fibromas, not fibrous dysplasia. NF-2 has little bony change with typical ocular abnormalities. Paget's disease occurs in older individuals and does not present with cafe-au-lait spots. Ollier's disease (multiple enchondromatosis) may show bone changes but not the other findings. Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746. Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
- Taleisnik J: Carpal instability. J Bone Joint Surg Am 1988;70:1262-1268.
Question 3High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
Explanation
25b The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
References:
- Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 4High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 5High Yield
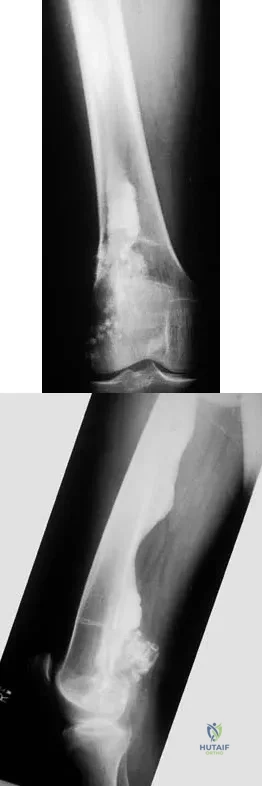
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?
Explanation
Explanation
59b 59c 59d This classic case of osteosarcoma illustrates the typical radiographic and histologic characteristics of this disease. The radiographs show an aggressive-appearing lesion of the distal femur. The lesion has both lytic and blastic areas. Periosteal reaction is present in the form of a Codman's triangle. The radiographs are highly suggestive of osteosarcoma. The photomicrographs show malignant spindle cells that produce osteoid, thus confirming the diagnosis of osteosarcoma. Treatment of osteosarcoma is multimodal including multi-agent chemotherapy and surgery (wide resection or amputation). Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
References:
- Mankin HJ, Hornicek FJ, Rosenberg AE, et al: Survival data for 648 patients with osteosarcoma treated at one institution. Clin Orthop Relat Res 2004;429:286-291.
Question 6High Yield
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 7High Yield
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Explanation
Multiple cytokines (inflammatory mediators) are released following trauma, and their levels can be measured in serum. Persistent elevated levels of IL-6 (> 800 pg/mL) indicate an exaggerated systemic inflammatory response to trauma and have been associated with the development of MODS. Recent work has shown that extensive surgical procedures should be avoided when IL-6 levels remain elevated to prevent the precipitation of MODS. In the future, it is likely that this mediator and possibly others will be used to determine timing and techniques of future treatment. Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429. Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
References:
- Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 8High Yield
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
The risk of infection in a 3B open tibia fracture is most directly related to the timing of the soft-tissue coverage and less related to the size or location of the wound. The wound VAC does not lower or raise the risk of infection in open fractures. It does appear to increase the window of time to obtain coverage without increasing the risk of infection. Additionally, the wound VAC may decrease the probability of needing free tissue coverage. Intramedullary nailing has not been shown to lower the risk of infection in 3B fractures. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292. Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Question 9High Yield
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?

Explanation
The radiographs reveal osteoarthritis and proximal humeral head migration. Integrity of the rotator cuff must be questioned based on these radiographic changes. The status of the rotator cuff is the most influential factor affecting postoperative function in shoulder hemiarthroplasty. The coracoacromial ligament provides a barrier to humeral head proximal migration in the face of a rotator cuff tear. The radiographs do not indicate significant humeral head or glenoid erosion. Acromioclavicular arthritis is often asymptomatic. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 10High Yield
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of
Explanation
Explanation
26b In a patient with inflammatory arthritis, advanced hallux valgus deformity in conjunction with lesser metatarsophalangeal joint destruction and subluxation warrants fusion of the first metatarsophalangeal joint and lesser metatarsal head resections. Hallux valgus correction will fail because of incompetent soft tissues. A Keller resection arthroplasty is not indicated in this age group. Synovectomy is contraindicated because of evidence of erosive changes of the lesser metatarsophalangeal joints. Ouzounian T: Rheumatoid arthritis of the foot & ankle, in Myerson MS (ed): Foot & Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 2, pp 1189-1204. Mann RA, Thompson FM: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg Am 1984;66:687-692.
References:
- Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term followup study. J Bone Joint Surg Am 2000;82:322-341.
Question 11High Yield
An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?
Explanation
Explanation
37b The patient has a well-established nonunion in a very porotic bone. Electrical stimulation has been found effective in treating tibial nonunions, but there is very little data on humeral nonunions, especially chronic well-established ones. Ultrasound stimulation is effective in accelerating fracture healing, but there is little data concerning the treatment of nonunions. Intramedullary nailing with bone graft is an option, but it maybe difficult to obtain a rigid construct in a very porotic bone. An Ilizarov-type external fixator would be an alternative, but there is little clinical data for the humerus and it may be poorly tolerated. A plate and screw construct with bone graft combines rigidity with the biologic advantage of the bone graft. A recent series reported on the use of a plate combined with onlay allograft for recalitrant nonunions. Cement augmentation for screw fixation either in the canal or added to the screw holes may be helpful in select cases. Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
References:
- Jupiter JB: The treatment of complex non-unions of the humeral shaft with a combination of surgical techniques. J Bone Joint Surg Am 1990;72:701-707.
Question 12High Yield
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
Explanation
Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
References:
- McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 13High Yield
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must

Explanation
While it is recommended that a patient gain full range of motion, pain-free function, and symmetric strength prior to returning to vigorous activities, it is absolutely essential that radiographs of the fracture site reveal a circumferential external bridging callus to prevent refracture. This is particularly important for comminuted femoral fractures with various sized fragments. It is also recommended that a return to rodeo riding be postponed for at least 1 year. Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112. Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am 1991;73:1561-1566.
Question 14High Yield
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of
Explanation
Dislocation of the long head of the biceps tendon is the result of a defect in the region of the rotator cuff interval, coracohumeral ligament-superior glenohumeral ligament pulley, or an associated tear of the medial insertion of the subscapularis tendon. In the case of an intra-articular dislocation of the long head of the biceps tendon associated with a tear of the subscapularis tendon, stabilization of the biceps tendon is difficult in this situation; therefore, biceps release or tenodesis and repair of the subscapularis tendon is the treatment of choice. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Question 15High Yield
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of

Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 16High Yield
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?

Explanation
Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis. Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765. Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Question 17High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 18High Yield
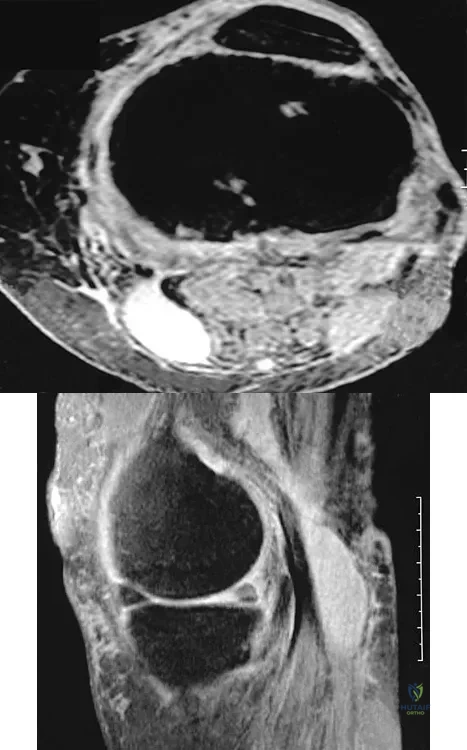
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
References:
- Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 19High Yield
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
Explanation
The patient has a classic Erb's palsy with weakness of the muscles innervated by the fifth and sixth cervical roots. Horner syndrome, a poor prognostic indicator for recovery, is absent in this infant. All infants with brachial plexus birth palsies initially should be monitored for spontaneous recovery during the first 3 to 6 months of life. During this period of observation, glenohumeral motion, especially external rotation, should be maintained. Many infants will begin to show recovery within the first 6 to 8 weeks after birth and continue on to normal function. The timing of microsurgery is controversial. A recent study found that the outcome of microsurgical repair in patients who had no recovery of biceps function within 3 months after birth was similar compared to those who had recovery of biceps function between 3 and 6 months and no microsurgical repair. The author concluded that microsurgical repair was effective in improving function in those infants who had no evidence of recovery of biceps function within the first 6 months of life. Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
References:
- Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 20High Yield
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of
Explanation
The radiographs show localized diffuse cortical thickening that is characteristic of melorheostosis. The condition may be monostotic or it may involve many bones in one extremity (monomelic) in the distribution of a sclerotome. Bone scans will show increased uptake at the site or sites of skeletal involvement. Long tubular bones are most commonly involved. Melorheostosis is usually asymptomatic and requires no treatment. On rare occasions, there may be associated soft-tissue contractures. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 21High Yield
Which of the following findings best describes the effects of increasing conformity of a fixed tibial bearing component and femoral component in total knee arthroplasty?
Explanation
Explanation
In the design of tibial and femoral components, a compromise must be made between contact stresses and constraint. Increased conformity increases constraint, limits motion, and potentially increases stress on the knee-cement interface. By increasing conformity, the surface area over which force is applied is increased, resulting in decreased peak contact stresses and decreased component wear rates. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
References:
- Bartel DL, Rawlinson JJ, Burstein AH, Ranawat CS, Flynn WF Jr: Stresses in polyethylene components of contemporary total knee replacements. Clin Orthop 1995;317:76-82.
Question 22High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?
Explanation
Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
References:
- Mann RA, Reynolds JC: Interdigital neuroma: A critical clinical analysis. Foot Ankle 1983;3:238-243.
Question 23High Yield
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm3. Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of
Explanation
Explanation
This clinical situation requires careful analysis because some data suggest infection and some a noninfectious inflammatory process. Bilateral hip involvement, the absence of significant fluid collection or fever, the streptozyme level, and the history of upper respiratory infection all suggest poststreptococcal toxic synovitis as the most likely cause for the clinical presentation. In the first 24 hours, this type of presentation might warrant incision and drainage given uncertainty of the diagnosis and the risks associated with missing an infection. However, 5 days after onset, surgery is not warranted, especially given that the patient remains afebrile and her symptoms are improving. Cardiology consultation would be appropriate. There is no evidence to suggest slipped capital femoral epiphysis. Treatment with antibiotics is not advised because there is no bacteriologic data on which to base treatment. De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
References:
- Haueisen DC, Weiner DS, Weiner SD: The characterization of "transient synovitis of the hip" in children. J Pediatr Orthop 1986;6:11-17.
Question 24High Yield
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?

Explanation
Lumbar spinal stenosis with lumbar radiculopathy can be commonly caused by a synovial cyst arising from the facet joints. Lyons and associates reported on the surgical treatment of synovial cysts in 194 patients. Of the 147 with follow-up data, 91% reported good pain relief and 82% had improvement of their motor deficits. Epstein reported a 58% to 63% incidence of good/excellent results and a 38 to 42 point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis. Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg 2000;93:53-57. Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Question 25High Yield
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?

Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 26High Yield
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
The patient has a burst fracture with probable unilateral entrapment of the cauda equina within the elements of the fractured lamina. A dural tear is likely in this scenario as well. It is recommended that this type of burst fracture be treated surgically with laminectomy, freeing of the entrapped nerve roots, and dural repair followed by stabilization of the fracture by either a posterior or combined approach. The degree of kyphosis and the extent of anterior canal compromise does not warrant corpectomy in this patient. Therefore, after completing the laminectomy and dural repair, posterior fusion and instrumentation should be sufficient to stabilize the fracture. Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 27High Yield
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?
Explanation
Explanation
50b 50c 50d 50e The pathology demonstrates a very cellular chondroid matrix with multinucleated forms, atypia, and myxomatous regions. This is most consistent with a myxoid chondrosarcoma. The radiograph shows a well-circumscribed lesion in the superior and medial aspect of the right acetabulum. The CT and MRI scans confirm these same findings with no evidence of matrix mineralization or significant surrounding edema. Unfortunately, in this location with this appearance, the radiographic differential diagnosis includes all the diagnoses listed. Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
References:
- Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 28High Yield
Figure 15 shows possible locations of anterior pin sites for halo fixation. What location is considered most ideal?
Explanation
Explanation
The anterior pin should be placed just above and lateral to the eyebrow at the site labeled A. At site B, the supraorbital nerve can be damaged. At site C, the supratrochlear nerve or the frontal sinus can be damaged. The site labeled D is over the temporalis muscle; in this location the temple bone is thin and there is the risk of perforation. Site E is above the equator of the forehead; at this location there is a risk that the halo ring will slip off the head altogether. Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
References:
- Garfin SR, Botte MJ, Centeno RS, Nickel VL: Osteology of the skull as it affects halo pin placement. Spine 1985;10:696-698.
Question 29High Yield
Which of the following best characterizes bone mineralization?
Explanation
Mineralization occurs at the site of hole zones between the collagen fibrils. Crystals begin from the necessary ions of the lattice that come together with the correct orientation to form the first stable crystal. Formation of this critical nucleus is the most energy-demanding step of crystallization. Enzymes within the extracellular matrix vesicles degrade inhibitors such as adenosine triphosphate, pyrophosphate, and proteoglycans found in the surrounding extracellular matrix. Bone mineral consists of numerous impurities (carbonate, magnesium) that are more soluble, allowing the bone to act as a reservoir for calcium, phosphate, and magnesium ions. Crystals may form by addition of ions or ion clusters to the critical nucleus in many directions, with 'kink' sites forming to branch and exponentially proliferate the crystals. Macromolecules facilitate formation of the critical nucleus and increasing local concentrations of necessary ions. Once the crystals are formed and proliferating, macromolecules bind to the surface and block the growth of the crystal, regulating size, shape, and number of crystals. Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Question 30High Yield
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of
Explanation
Explanation
The patient has a chronic ingrown nail on his great toe, which is not an uncommon occurrence in teenagers because of improper nail care. There is local infection and a foreign body reaction because of the nail. Continued conservative management with soaks and antibiotics will not improve the clinical situation. In the presence of local chronic infection, nail matrix ablation is contraindicated. Additionally, in the absence of a history of an ingrown nail, a nail matrix ablation is not medically indicated. The appropriate treatment is partial removal of the nail plate. With nail plate removal, the inflammation and local infection will resolve rapidly. Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
References:
- Coughlin MJ, Mann RA: Toenail abnormalities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1033-1070.
Question 31High Yield
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
Explanation
TCP is resorbed more rapidly, at a rate of 10 to 20 times faster than hydroxyapatite, partially because its larger pore size makes it a weaker substance. It provides significantly less compressive strength than hydroxyapatite. It does partially convert to hydroxyapatite, thus slowing its resorption rate. The absorbing cell of hydroxyapatite is the foreign body giant cell, not the osteoclast. Optimum pore size appears to be between 150 and 500 um. Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
References:
- Walsh WR, Chapman-Sheath PJ, Cain S, et al: A resorbable porous ceramic composite bone graft substitute in a rabbit metaphyseal defect model. J Orthop Res 2003;21:655-661.
Question 32High Yield
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?

Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 33High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 34High Yield
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings?
Explanation
Explanation
Os acromiale represents a failure of fusion of the anterior acromial apophysis and has been reported in approximately 8% of the population. Patients with a symptomatic os acromiale often report impingement-type symptoms with pain over the superior acromion, especially with overhead activities or sleeping. When nonsurgical management is unsuccessful, surgical options include excision, open reduction and internal fixation, and arthroscopic decompression. Kurtz CA, Humble BJ, Rodosky MW, et al: Symptomatic os acromiale. J Am Acad Orthop Surg 2006;14:12-19.
References:
- Ortiguera CJ, Buss DD: Surgical management of the symptomatic os acromiale. J Shoulder Elbow Surg 2002;11:521-528.
Question 35High Yield
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?

Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 36High Yield
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
Explanation
Laminoplasty or any posterior decompressive procedure is contraindicated in patients with cervical spondylotic myelopathy and cervical kyphosis. The residual kyphotic posture of the cervical spine results in persistent spinal cord compression. The other choices are not contraindications for laminoplasty. Concomitant cervical radiculopathy can be addressed at the time of laminoplasty with a keyhole foraminotomy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 37High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 38High Yield
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
Explanation
Dense pods of ingrowth into the porous coating of cementless ingrowth sockets are seen. Channels through the non-ingrown portion allow access to the trabecular bone of the ilium. Polyethylene wear debris can enter these areas through screw holes. Expansile, lytic lesions can result, which can become large without compromising implant fixation. Loosening is late and results from catastrophic loss of bone. A well-fixed acetabular component with a modular design, a well-designed locking mechanism, and a good survivorship history is a candidate for exchange of the liner and grafting of the osteolytic lesion. Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265. Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
References:
- Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 39High Yield
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 40High Yield
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
Explanation
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
References:
- Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 41High Yield
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
Explanation
35b 35c The patient has an open fracture of the physis of the distal phalanx with a portion of the nail bed interposed in the physis. Seymour initially described this injury in the distal phalanges of fingers. Optimal treatment consists of removing the interposed tissue, irrigating the fracture, and a short course of antibiotics. The nail should be preserved to provide stability. Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34. Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
References:
- Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 42High Yield
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include

Explanation
Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Question 43High Yield
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
Explanation
64b 64c 64d 64e The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Question 44High Yield
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
Explanation
15b The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five "P's" of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease. Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998, pp 1826-1844.
Question 45High Yield
What is the most common foot deformity associated with myelomeningocele?
Explanation
Explanation
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
References:
- Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 622-628.
Question 46High Yield
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
Explanation
45b 45c 45d Giant cell tumors typically occur in a juxta-articular location involving the epiphysis and metaphysis of long bones, usually eccentric in the bone. The radiographs show a destructive process within the distal tibia and an associated soft-tissue mass. The histology shows multinucleated giant cells in a bland matrix with a few scattered mitoses. Osteosarcoma can have a similar destructive appearance but a very different histologic pattern with osteoid production. Ewing's sarcoma also can have a diffuse destructive process in the bone. The histologic pattern of Ewing's sarcoma is diffuse round blue cells. Aneurysmal bone cysts typically are seen as a fluid-filled lesion on imaging studies and have only a scant amount of giant cells histologically. Metastatic adenocarcinoma does not demonstrate the pattern shown in the patient's histology specimen. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
References:
- Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 47High Yield
A 12-year-old girl has painless bowing of the tibia. Radiographs and a biopsy specimen are shown in Figures 35a through 35c. What is the most likely diagnosis?
Explanation
Explanation
35b 35c The patient has osteofibrous dysplasia. The radiographic differential diagnosis includes osteofibrous dysplasia, fibrous dysplasia, and adamantinoma. Histology shows a fibro-osseous lesion with prominent osteoblastic rimming but a lack of epithelial nests. Adamantinoma is a low-grade malignancy that typically is located in the anterior tibial cortex and has a soap bubble appearance. Histologically, it is similar to osteofibrous dysplasia but includes epithelial nests of cells. Treatment requires resection. Fibrous dysplasia usually does not require biopsy; however, in this patient the radiographs do not distinguish it from adamantinoma. The radiographic findings are not typical of Ewing's sarcoma or osteosarcoma. Repeat biopsy should be considered if clinical or radiographic features change.
References:
- Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 48High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
References:
- Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 49High Yield
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
Explanation
15b 15c The biopsy specimen shows a wavy collagenous matrix with elongated cells; this is most consistent with neurofibroma. The patient has a mass in the region of the sciatic nerve. Imaging characteristics, homogeneous and very low signal on T1-weighted and very high signal on the T2-weighted sequences, are consistent with a myxoid-type lesion. These include myxoma, myxoid sarcomas, and nerve sheath tumors. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
References:
- Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 50High Yield
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?
Explanation
Explanation
Transphyseal fractures of the proximal femur at birth are more likely to occur in large newborns after a difficult delivery. At rest, the patients are comfortable and show a pseudoparalysis; however, passive motion of the lower extremity results in discomfort. Teratologic hip dislocations will have a positive Galeazzi sign, but are not painful. Development of a septic hip would be unlikely within 12 hours postpartum. Congenital coxa vara is typically painless. Postpartum ligamentous laxity might account for a positive Ortolani sign, but is painless. Weinstein JN, Kuo KN, Millar EA: Congenital coxa vara: A retrospective review. J Pediatr Orthop 1984;4:70-77.
References:
- Beaty JH: Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 409-425.
Question 51High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
References:
- Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 52High Yield
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
Explanation
The child has a near complete central physeal arrest of the distal femur and worsening limb-length discrepancy will develop. She is growing at the average rate for the population. The distal femoral physis grows at a rate of roughly 9 mm per year. Girls finish their growth at approximately age 14 years. Thus, at maturity the left leg will be 6.4 cm longer than the right. An angular deformity has not developed at this point and her arrest is central; therefore, angular deformity is unlikely to develop in any plane. Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
References:
- Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 53High Yield
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?
Explanation
Explanation
The risk of synostosis is imminent with any technique for repairing a distal biceps tendon rupture. However, the risk is quite low for all approaches that avoid exposure of the ulna, including the muscle-splitting two-incision technique.
References:
- Norris TR: Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, p 342.
Question 54High Yield
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a lobular mass that is below the vitamin E tablet marker taped to the skin. This is juxtaposed to the tibialis anterior tendon. It is slightly more enhanced than the surrounding subcutaneous fat and is consistent with a ganglion. Osteosarcoma, aneurysmal bone cyst, or unicameral bone cyst all would demonstrate enhancement or pathology in the bone. This is clearly a well-defined soft-tissue mass. Gouty tophi show low to intermediate signal on T1- and T2-weighted images. Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547. Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
References:
- Gerster JC, Landry M, Dufresne L, Meuwly JY: Imaging of tophaceous gout: Computed tomography provide specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis 2002;61:52-54.
Question 55High Yield
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
Explanation
The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
References:
- Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 56High Yield
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type

Explanation
The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 57High Yield
Which of the following best describes heat stroke?
Explanation
Heat stroke consists of hyperthermia (greater than 105.8 degrees F [41 degrees C]), central nervous system dysfunction, and cessation of sweating with hot, dry skin. It is a medical emergency that results from failure of the thermoregulatory mechanisms of the body. It has a high death rate and requires rapid reduction in body core temperature. Heat syncope is characterized by a transient loss of consciousness with peripheral vasodilation and decreased cardiac output with normal body temperature. Heat cramps involve painful contractions of large muscle groups because of decreased hydration and a decrease of serum sodium and chloride. Heat exhaustion is distinguished by a core temperature of less than 102.2 degrees F (39 degrees C) and an absence of central nervous system dysfunction. Hypernatremic heat exhaustion results from inadequate water replacement. Knochel JP: Environmental heat illness: An eclectic review. Arch Intern Med 1974;133:841-864. Hubbard RW, Gaffin SL, Squire DL: Heat related illness, in Wilderness Medicine, ed 3. St Louis, MO, Mosby, 1995, p 167.
Question 58High Yield
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0 degrees. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of

Explanation
Because the patient's shoulders are overtensioned anteriorly, premature osteoarthritis may develop. This may create obligate translation posteriorly and increase the interarticular pressure of the humeral head against the glenoid. Patients should achieve 20 degrees to 30 degrees of external rotation with the elbow at the side. Late degenerative arthritis following a Putti-Platt procedure is associated with significant restriction of external rotation. This patient's shoulder has a reduced risk of anterior instability, rotator cuff tear, and internal impingement because of the limitation of motion. Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 59High Yield
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
Explanation
46b 46c Nodular fasciitis is a benign soft-tissue lesion that usually arises from the fascia and is often misdiagnosed as a sarcoma. Desmoid tumors (aggressive fibromatosis) are also benign tumors with a greater tendency for local recurrence. Desmoid tumors have more spindle-shaped fibroblasts in an abundant collagenous matrix. Malignant fibrous histiocytoma is a hypercellular pleomorphic sarcoma more commonly found in adults. The histology is not consistant with a fatty tumor.
References:
- Bernstein KE, Lattes R: Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-1678.
Question 60High Yield
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?

Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 61High Yield
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?
Explanation
Explanation
In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation. Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
References:
- Aschauer E, Resch H: Four-part proximal humeral fractures: ORIF, in Warner JP, Iannotti JP, Flatow EL (eds): Complex and Revision Problems in Shoulder Surgery, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 289-309.
Question 62High Yield
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
References:
- Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 63High Yield
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 64High Yield
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
Explanation
15b 15c The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
References:
- Hensinger RN, DeVito PD, Ragsdale CG: Changes in the cervical spine in juvenile rheumatoid arthritis. J Bone Joint Surg Am 1986;68:189-198.
Question 65High Yield
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 66High Yield
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of
Explanation
Explanation
The history, physical examination, and radiographs indicate that the patellofemoral pain is most likely caused by excessive lateral patellar pressure and patellar maltracking. Because the radiographs reveal the lateral tilt of the patella and lateral subluxation, the treatment of choice is bilateral lateral releases with anteromedialization of the tibial tubercles. This procedure corrects not only the excessive lateral patellar pressure, but also the lateral subluxation. The use of patella-stabilizing braces or taping may provide temporary relief, but these implements are not well-tolerated and they will not change the underlying biomechanics of the knee. Simple lateral release is indicated for isolated lateral tilt, but it does not correct the lateral subluxation. The use of thermal capsular shrinkage for the medial retinaculum has not been proven to provide long-term correction of the deformity. Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
References:
- Fulkerson JP: Patellofemoral pain disorders: Evaluation and management. J Am Acad Orthop Surg 1994;2:124-132.
Question 67High Yield
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Explanation
Explanation
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
References:
- Dellon AL, Mackinnon SE: Injury to the medial antebrachial cutaneous nerve during cubital tunnel surgery. J Hand Surg Br 1985;10:33-36.
Question 68High Yield
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?

Explanation
The grading of response to chemotherapy for osteosarcoma was introduced by Huvos and associates. Patients with tumors that show more than 90% necrosis after neoadjuvant chemotherapy are considered to have had a good response and have better survival rates than those with less than 90% necrosis. However, it should be noted that survival rates for patients with a poor response are still better than in patients who do not receive neoadjuvant chemotherapy. More recently, similar results have been reported in patients with Ewing's sarcoma. Chemotherapy is not typically used for giant cell tumor of bone. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Question 69High Yield
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
Explanation
25b 25c The patient has a displaced burst fracture. Fusion with instrumentation has shown better results than casting alone. Posterior fusion with instrumentation, with sagittal plane correction, yields the best results. Decompression occurs indirectly with correction of the kyphosis. Anterior decompression is unnecessary. Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120. Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
References:
- Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 70High Yield
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?

Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 71High Yield
What type of nerve palsy is most common following elbow arthroscopy?

Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 72High Yield
Which of the following ligaments are the primary static restraints to inferior translation of the arm when the shoulder is in 0 degrees of abduction and neutral rotation?
Explanation
Explanation
Biomechanical ligament sectioning studies have implicated both the superior glenohumeral and coracohumeral ligaments as restraints to inferior translation when the shoulder is in 0 degrees of abduction and neutral rotation. Although there is controversy over the significance of each ligament, both are involved to some degree. The middle glenohumeral ligament is more important in the midranges of abduction, and the inferior ligament is more important at 90 degrees of abduction. The coracoacromial and coracoclavicular ligaments play no role in glenohumeral restraint. Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
References:
- Jost B, Koch PP, Gerber C: Anatomy and function of the rotator interval. J Shoulder Elbow Surg 2000;9:336-341.
Question 73High Yield
A 5-year-old girl sustained a comminuted Salter-Harris type IV fracture of the left distal tibia 2 years ago. The AP radiograph shown in Figure 54a reveals a growth arrest and a 1.4-cm limb-length discrepancy. The ankle is in approximately 20 degrees of varus. Figure 54b shows a coronal reconstruction image of the distal tibial physis, and Figure 54c shows a sagittal reconstruction image of the same area. On the sagittal reconstruction image, the bar extends from the 9-mm mark to the 24-mm mark in 3-mm increments. On the coronal image, the bar extends from the 9-mm mark to the 24-mm mark, also in 3-mm increments. A map of the physeal bar based on these measurements is shown in Figure 54d. Initial treatment should consist of
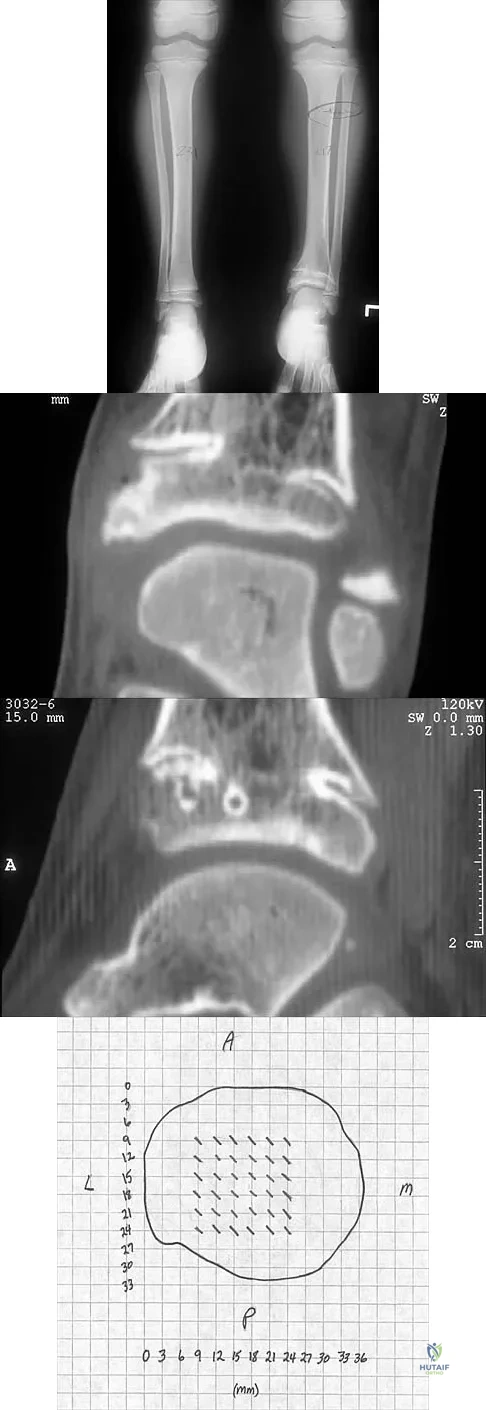
Explanation
Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 74High Yield
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
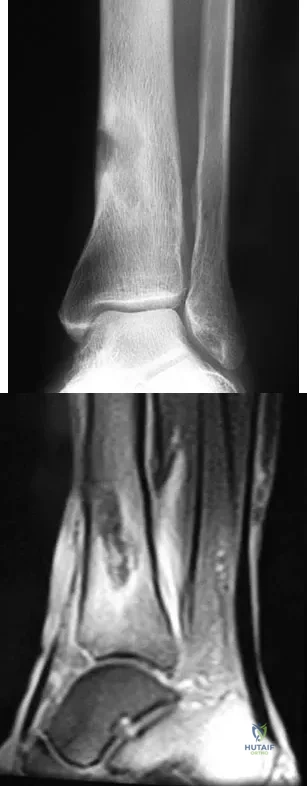
Explanation
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful. Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Question 75High Yield
During the implantation of a cementless acetabular component in total hip arthroplasty, placement of a screw in the anterior superior quadrant puts which of the following structures at risk for damage?
Explanation
Explanation
A knowledge of the safe quadrants for screw placement for acetabular component implantation is essential when performing total hip arthroplasty. The external iliac vessels are on the inner wall of the pelvis, corresponding to the anterior superior quadrant of the acetabulum. Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws. J Bone Joint Surg Am 1990;72:509-511.
References:
- Wasielewski RC, Cooperstein L, Kruger MP, Rubash HE: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508.
Question 76High Yield
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
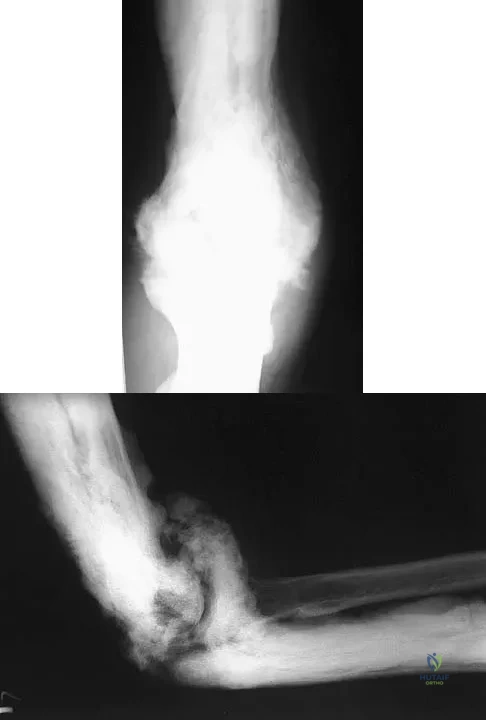
Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 77High Yield
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a transection of the biceps muscle. The underlying brachialis is intact. This injury can occur as a result of a cord wrapped around the upper arm. Care should be taken to ensure that there is no concurrent vascular injury. A posterior subcutaneous lipoma appears as a well-encapsulated mass on T2-weighted images. Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
References:
- Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 78High Yield
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
Explanation
Foot deformity and decreased joint motion have been associated with increased plantar pressures and an increased risk of ulceration. In a partial-thickness ulcer without exposed bone or tendon, total contact casting is highly effective. Concomitant Achilles tendon lengthening increases the likelihood that healing of the ulcer can be obtained and perhaps more importantly, maintained. Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
References:
- Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 79High Yield
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
Explanation
The most common finding at exploration of an inappropriately placed pedicle screw is displacement of the nerve. Pedicle breach is common, ranging from 2% to 20%, but most are asymptomatic. All of the choices are possible, but in a large series conducted by Lonstein and associates, the authors reported that displacement of the root, most often medial, was the most common finding. Laceration, contusion, or transfixion usually was not seen. Spinal fluid leakage occurs less frequently and is not expected in the minimal broach illustrated. Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238. Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
References:
- Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 80High Yield
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
Explanation
Polyethylene wear debris can result in significant synovitis and subsequent cloudy appearing synovial fluid. Typically, laboratory studies show a WBC of less than 30,000/mm3 no left shift. Cytologic examination can reveal intra-articular polyethylene particles. Infected total knee arthroplasty is extremely uncommon in a healthy, immune-competent patient who has a normal preoperative erythrocyte sedimentation rate and C-reactive protein level.
References:
- Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 81High Yield
What anatomic site is considered at highest risk for pathologic fracture?
Explanation
Explanation
The subtrochanteric femur has been identified as an anatomic site that is particularly prone to pathologic fracture. An avulsion fracture of the lesser trochanter is a sign of impending femoral fracture. While the other anatomic locations are also frequently involved in metastatic bone disease, pathologic fractures occur less commonly. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
References:
- Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1055.
Question 82High Yield
A 15-year-old boy with epilepsy who is treated with phenytoin sustains a vertebral compression fracture during a breakthrough seizure. Radiographs of the spine reveal generalized osteopenia. What is the most likely cause of the osteopenia?
Explanation
Explanation
As a side effect of treatment, phenytoin induces osteomalacia, or rickets, in growing children, through interference with metabolism of vitamin D. Oral supplementation of vitamin D can minimize this effect in patients who are undergoing prolonged treatment with phenytoin.
References:
- Chung S, Ahn C: Effects of anti-epileptic drug therapy on bone mineral density in ambulatory epileptic children. Brain Dev 1994;16:382-385.
Question 83High Yield
Radiographs of a 15-year-old girl with knee pain reveal a radiopaque lesion of the distal femoral metaphysis and epiphysis with a small associated soft-tissue mass. A biopsy specimen shows osteoid and pleomorphic cells with multiple mitotic figures. Staging studies show no other sites of disease. Treatment should consist of
Explanation
Explanation
Based on the location and extent of the tumor, most patients are candidates for limb salvage surgery. The patient has an osteosarcoma; therefore, the treatment of choice is preoperative chemotherapy, wide resection, and reconstruction. There is no difference in survival rates between patients who undergo limb salvage surgery and those who undergo amputation. Curettage and placement of methylmethacrylate is used to treat benign lesions of bone and would not be appropriate in this patient.
References:
- Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Osteosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 265-274.
Question 84High Yield
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?

Explanation
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Question 85High Yield
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
Anteromedial displacement of the tibial tubercle unloads the distal and lateral facets of the patella and shifts the forces to the proximal and medial facets. Therefore, if findings indicate arthrosis predominately in the medial and proximal areas of the patella, this is considered a relative contraindication because it may accentuate arthritic symptoms. Fulkerson JP: Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop 1983;177:176-181. Bellemans J, Cauwenberghs F, Witvrouw E, et al: Anteromedial tibial tubercle transfer in patients with chronic anterior knee pain and a subluxation-type patellar malalignment. Am J Sports Med 1997;25:375-381.
Question 86High Yield
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
Explanation
Acute posterior dislocations occur rarely, accounting for less than 5% of acute dislocations. They are most often the result of falls on an outstretched hand. Reduction can be accomplished with flexion of the arm to 90 degrees and adduction to disimpact the humeral head from the glenoid rim. The arm is then externally rotated until the head has cleared the glenoid rim. Following brace immobilization in neutral to 5 to 10 degrees of external rotation and slight abduction, it is critical to avoid internal rotation for 4 to 6 weeks. Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1986;68:724-731.
References:
- Pollock RG, Bigliani LU: Recurrent posterior shoulder instability: Diagnosis and treatment. Clin Orthop 1993;291:85-96.
Question 87High Yield
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?

Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 88High Yield
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 89High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 90High Yield
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain?
Explanation
Explanation
McCune-Albright syndrome is the combination of polyostotic fibrous dysplasia, café-au-lait lesions, and endocrine dysfunction. The most common endocrine presentation is precocious development of secondary sexual characteristics. Compared with bone lesions in patients without polyostotic disease, the skeletal lesions in patients with the syndrome tend to be larger, more persistent, and associated with more complications. Bisphosphonate therapy has been shown in several studies to decrease the pain associated with the skeletal lesions of fibrous dysplasia. DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation and treatment. J Bone Joint Surg Am 2005;87:1848-1864.
References:
- Zacharin M, O'Sullivan M: Intravenous pamidronate treatment of polyostotic fibrous dysplasia associated with McCune Albright syndrome. J Pediatr 2000;137:403-409.
Question 91High Yield
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
Explanation
Clearance of the cervical spine can be difficult in the obtunded or unresponsive patient. Various trauma series have been reported to detect up to 95% of cervical fractures but only when ideal imaging views have been obtained, which is not often possible in the unresponsive or uncooperative patient. Passively performed cervical flexion-extension under live fluoroscopy has been suggested but is not without inherent risk in the potentially unstable cervical spine. CT of the cervical spine has gained acceptance for the evaluation of these patients given the excellent evaluation of the osseous anatomy and for the common availability in most emergency departments. Sanchez and associates, using a protocol to evaluate for cervical spine injuries after blunt trauma, were able to detect 99% of cervical fractures with 100% specificity. Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463. Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.
Question 92High Yield
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
Explanation
53b Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggest that intramedullary nails done acutely with avoidance of intraoperative hypotension did not compromise the outcome related to the head injury. This was especially true for high-level GCS scores. A GCS score of lower than 8 and intraoperative hypotension have been associated with worsening outcomes following acute intramedullary nailing of the femur. Skin traction and distal femur skeletal traction in a young adult man with a femoral fracture is not well tolerated secondary to spasm and pain. External fixation is an option but an unnecessary step in the treatment of this patient. Ventriculostomy is not necessary in stable patients with no significant bleeding on a CT scan of the head. Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45. Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369. McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Question 93High Yield
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
References:
- Ross PD, Davis JW, Epstein RS, Wasnich RD: Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114:919-923.
Question 94High Yield
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?

Explanation
The child has an up-to-date tetanus; therefore, a booster is not recommended. Pseudomonas coverage is most likely not needed because the child was barefoot. It is too early to evaluate for abscess or osteomyelitis with MRI, and a formal debridement is rarely indicated without signs of an abscess or a retained foreign body. Radiographs with soft-tissue penetration should be obtained to check for a retained foreign body. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
Question 95High Yield
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 255-264.
Question 96High Yield
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
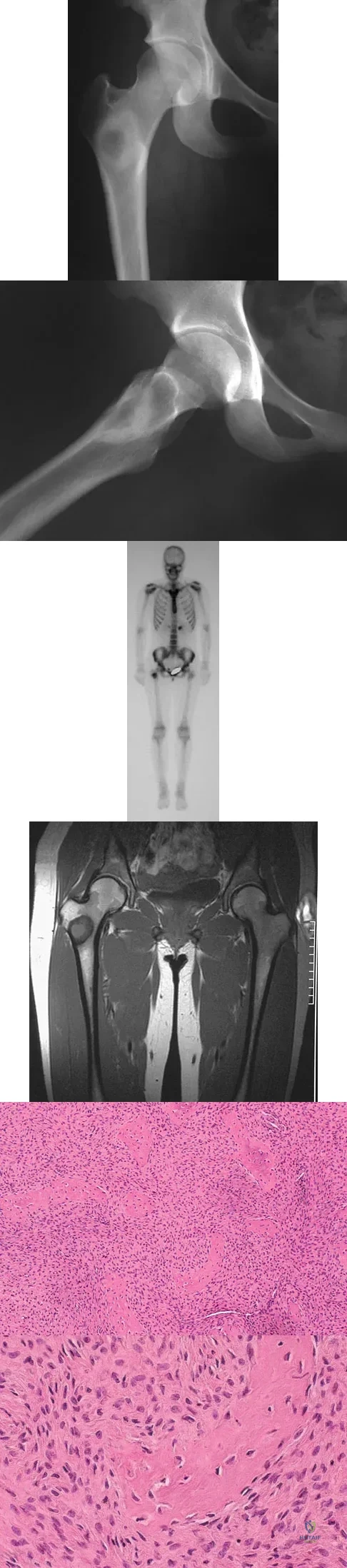
Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 97High Yield
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
Explanation
41b Open reduction and internal fixation of distal humeral fractures in elderly patients often fails. These fractures characteristically have a very small distal segment and poor bone quality, resulting in failure of fixation and nonunion. Nonunion is often painful and functionally debilitating. Total elbow arthroplasty provides good results when used for distal humeral fractures in elderly patients with osteopenic bone and fracture patterns thought to be irreconstructable. Long arm casting may result in union, but the resulting stiffness is unacceptable for an active patient. Elbow arthrodesis has few indications. A sling and range-of-motion exercises will often result in a painful and debilitating nonunion at the fracture site. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
References:
- Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 98High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 99High Yield
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
Explanation
The history, examination, and surgical findings are most consistent with plantar fibromatosis. Plantar fibromatosis is a benign tumor of the plantar fascia that consists chiefly of fibromyoblasts. These cells produce excessive collagen and are similar to the cells found in the palmar fascia of patients with Dupuytren's contracture of the hand. The myocyte, synovial cell, and osteocyte all produce their respective individual tissue types but do not contribute to the formation of a plantar fibromatosis. The T-cell is an important immunologic cell that is most affected in patients with HIV.
References:
- Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 100High Yield
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?
Explanation
Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
References:
- Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding anterior-approach-to-the-hip