Full Question & Answer Text (for Search Engines)
Question 1:
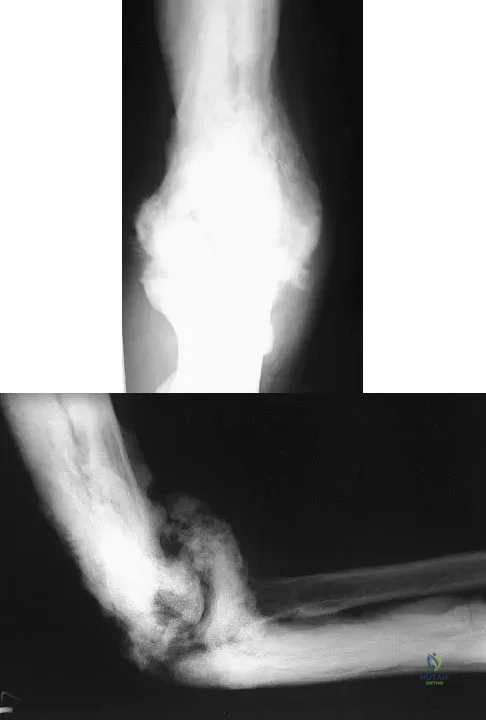
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Options:
- semiconstrained total elbow arthroplasty.
- ulnohumeral arthroplasty and anterior and posterior capsular releases.
- closed reduction and external fixation.
- open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a hinged elbow fixator.
- open reduction, heterotopic excision, anterior and posterior capsular releases, and pin fixation across the joint for 3 weeks.
Correct Answer: open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a hinged elbow fixator.
Explanation:
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition. Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
References:
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 2:
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Options:
- splinting for 5 weeks.
- active range-of-motion exercises after 1 to 3 days.
- delayed passive stretching at 2 weeks.
- open medial collateral ligament reconstruction.
- open lateral collateral ligament reconstruction.
Correct Answer: active range-of-motion exercises after 1 to 3 days.
Explanation:
The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation. Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
References:
O'Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 3:
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Options:
- Immediately
- In three games
- After anterior plate removal
- Next season
- Cannot return
Correct Answer: Immediately
Explanation:
The radiograph shows that the two-level anterior cervical diskectomy and fusion has healed. In addition, the patient has good range of motion and the neurologic examination is normal. Based on these findings, the patient can return to play immediately. Patients with one- or two-level anterior cervical diskectomies and fusions that have healed fully can return to play. Any loss of motion, persistent neurologic deficit, or significant adjacent segment degeneration may preclude a player from returning. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
Torg JS, Ramsey-Emrhein JA: Management guidelines for participation in collision activities with congenital, developmental, or post-injury lesions involving the cervical spine. Clin Sports Med 1997;16:501-530.
Question 4:
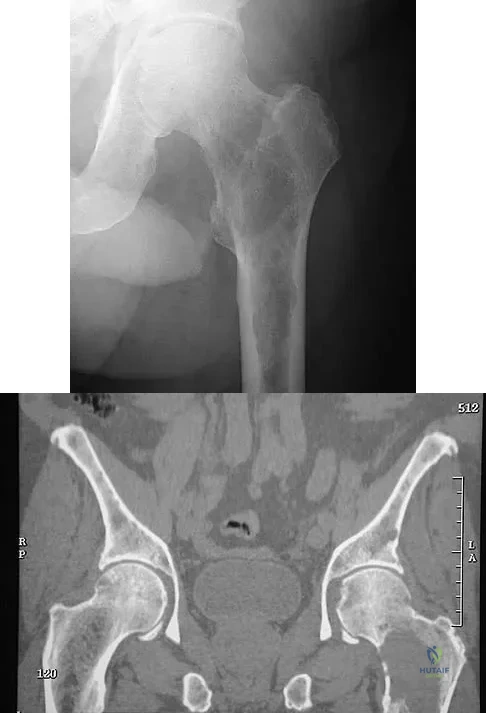
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Options:
- chemotherapy, wide resection, and endoprosthetic reconstruction.
- radiation therapy only.
- chemotherapy only.
- prophylactic internal fixation with a locked intramedullary rod.
- open curettage, bone grafting, dynamic hip screw fixation, and radiation therapy.
Correct Answer: prophylactic internal fixation with a locked intramedullary rod.
Explanation:
The underlying diagnosis is multiple myeloma. Because the patient has a large lucent lesion in the peritrochanteric region of the left proximal femur, the risk of pathologic fracture is high. Consideration should be given to prophylactic internal fixation with a locked intramedullary rod. The lesion does not appear to be a sarcoma requiring wide resection and endoprosthetic reconstruction. Neither chemotherapy nor radiation therapy alone is likely to result in long-term stabilization of the proximal femur. Postoperative treatment with bisphosphonates and radiation therapy is indicated to decrease the risk of future pathologic fractures. The patient should also be referred to a medical oncologist for medical management. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
References:
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 5:
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Options:
- No pharmacologic intervention is recommended at this time
- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours
- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 48 hours
- Administration of naloxone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours
- Administration of naloxone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 48 hours
Correct Answer: No pharmacologic intervention is recommended at this time
Explanation:
The standard practice in the pharmacologic treatment of a spinal cord injury in the United States has been the administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours, in accordance with the findings of the second and third National Acute Spinal Cord Injury Studies (NASCIS). Although the studies have subsequently drawn criticism for their methodology and outcomes, it has been generally accepted that beneficial neurologic outcomes were anticipated in patients who were able to start the protocol within 8 hours of their initial injury. Further improvement was noted in patients receiving the methylprednisolone within 3 hours of their injury and continuing an infusion for 48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time. Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
References:
Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.
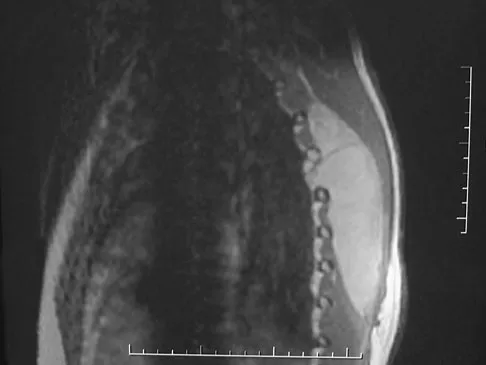
Question 6:
What is the most likely type of pathology seen in Figure 16?
Options:
- Tumor
- Infection
- Inflammatory
- Congenital
- Trauma
Correct Answer: Tumor
Explanation:
The figure shows the missing pedicle or "winking owl" sign that is characteristic of tumor involvement of the cortical bone of the pedicle. None of the other pathologic processes commonly gives this radiographic picture. Thinned, but not missing pedicles, have been described as a normal variant. McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
References:
Charlton OP, Martinez S, Gehweiler JA Jr: Pedicle thinning at the thoracolumbar junction: A normal variant. Am J Roentgenol 1980;134:825-826.
Question 7:
The pathophysiology of a claw toe deformity includes muscular imbalance caused by which of the following relatively strong structures?
Options:
- Intrinsics overpowering a relatively weak extensor digitorum longus
- Plantar plate overpowering a relatively weak extensor digitorum brevis
- Lumbricals overpowering relatively weak intrinsics
- Extensor digitorum longus overpowering relatively weak intrinsics
- Extensor digitorum longus overpowering a relatively weak extensor digitorum brevis
Correct Answer: Extensor digitorum longus overpowering relatively weak intrinsics
Explanation:
The dynamic forces acting to maintain the position of the proximal phalanx at the head of the metatarsal are a balance between the extensor digitorum longus and the weaker intrinsic muscles. With hyperextension at the metatarsophalangeal joint, the intrinsic muscles become less efficient as plantar flexors. Consequently, the hyperextension deformity progresses in the metatarsophalangeal joint as the opposition of the intrinsic muscles to the extensor tendon lessens. This is in contrast to the situation in the interphalangeal joints, where the stronger flexors overpower the weaker intrinsic muscles, which act as the extensors. This combination of events leads to hyperextension at the metatarsophalangeal joint and flexion deformities at the interphalangeal joints, resulting in claw toe. Mizel MS, Yodlowski ML: Disorders of the lesser metatarsophalangeal Joints. J Am Acad Orthop Surg 1995;3:166-173.
References:
Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed. 7. St Louis, MO, Mosby, 1999, pp 325-328.
Question 8:
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?
Options:
- A 2-year-old with spastic diplegia and a flexible equinovarus foot
- A 5-year-old with spastic quadriplegia and athetosis
- A 6-year-old with spastic hemiplegia, a flexible equinovarus foot, and out-of-phase posterior tendon activity on electromyography
- A 6-year-old with spastic hemiplegia, a flexible equinovarus foot, and continuous posterior tibial tendon activity on electromyography
- A 10-year-old with spastic quadriplegia and a rigid equinovarus foot
Correct Answer: A 6-year-old with spastic hemiplegia, a flexible equinovarus foot, and continuous posterior tibial tendon activity on electromyography
Explanation:
Isolated split posterior tendon transfer alone is best performed in a patient with cerebral palsy who is between the ages of 4 and 7 years and has a flexible equinovarus foot. Rigid deformities often must be managed with a combination of soft-tissue and bony procedures. Patients with out-of-phase activity may be best managed with a transfer of the posterior tibialis to the dorsum of the foot, while those with continuous activity are better candidates for an isolated split posterior tendon transfer. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
References:
Kling TF Jr, Kaufer H, Hensinger RN: Split posterior tibial-tendon transfers in children with cerebral spastic paralysis and equinovarus deformity. J Bone Joint Surg Am 1985;67:186-194.
Question 9:
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Options:
- Unicameral bone cyst
- Aneurysmal bone cyst
- Giant cell tumor
- Chondromalacia
- Ewing's sarcoma
Correct Answer: Ewing's sarcoma
Explanation:
Although the imaging studies are consistent with a unicameral bone cyst, aneurysmal bone cyst, or giant cell tumor, the histology shows small round blue cells that are typical of Ewing's sarcoma. Although Ewing's sarcoma frequently occurs in the diaphysis, it can occur in the metaphysis.
References:
Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 10:
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Options:
- Plate and screw fixation
- Fluted intramedullary rods
- Interlocking intramedullary rods
- Cemented intramedullary rods
- Step-cut osteotomies and interlocking intramedullary rods
Correct Answer: Plate and screw fixation
Explanation:
Plate and screw fixation of allograft is associated with the highest incidence of union but also the highest prevalence of allograft fracture. Conversely, intramedullary fixation is associated with a higher incidence of nonunion but fewer fractures. Step-cut osteotomies are not associated with a higher incidence of union.
References:
Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 11:
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Options:
- Loosening of the prosthesis
- Modulus mismatch
- Chronic infection
- Osteoporosis
- Metastatic tumor
Correct Answer: Loosening of the prosthesis
Explanation:
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
References:
Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.
Question 12:
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Options:
- Ulnar nerve
- Radial nerve
- Posterior interosseous nerve
- Superficial radial nerve
- Median nerve
Correct Answer: Radial nerve
Explanation:
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
References:
Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 13:
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Options:
- Neurofibroma of the suprascapular nerve
- Ganglion cyst of the suprascapular notch
- Ganglion cyst of the spinoglenoid notch
- Lipoma of the suprascapular notch
- Lipoma of the spinoglenoid notch
Correct Answer: Ganglion cyst of the spinoglenoid notch
Explanation:
Compression of the suprascapular nerve by a ganglion cyst is a well-documented cause of pain and weakness in the shoulder. Isolated involvement of the infraspinatus indicates that the area of entrapment is at the spinoglenoid notch and not the suprascapular notch. The majority of ganglion cysts found in the shoulder are related to tears of the labrum. When such a compressive lesion is found, decompression can be accomplished through either an open or arthroscopic approach. Several authors have shown the value of arthroscopy in the treatment of this condition. It has been shown that it is technically possible to decompress a paralabral ganglion cyst using arthroscopy; this method is usually followed by repair of the torn labrum. Alternatively, arthroscopic repair of the labrum can be performed and the cyst may be aspirated at the time of surgery. Open cyst excision through a posterior approach is also an acceptable method of treatment. Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114. Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
References:
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 14:
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?
Options:
- Development of arthritic changes at 1 year
- Restoration of full elbow range of motion
- Loss of approximately 25% of elbow flexion strength
- Posterolateral rotatory instability
- Olecranon nonunion
Correct Answer: Loss of approximately 25% of elbow flexion strength
Explanation:
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%. McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
References:
Ring D, Jupiter JB, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
Question 15:
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Options:
- Anterior border of the tibia
- Anterior border of the posterior cruciate ligament (PCL)
- Posterior border of the tibia
- Posterior border of the anterior horn of the lateral meniscus
- Posterior border of the anterior horn of the medial meniscus
Correct Answer: Anterior border of the posterior cruciate ligament (PCL)
Explanation:
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL. Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
References:
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 16:
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Options:
- observation.
- rehabilitation.
- immobilization.
- primary repair.
- reconstruction.
Correct Answer: primary repair.
Explanation:
The MRI scan shows a rupture of the patellar tendon. This injury is most appropriately addressed with primary repair. For athletic individuals, the results of nonsurgical management are suboptimal. Reconstructive procedures are not necessary. Matava MJ: Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-296.
References:
Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307.
Question 17:
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?
Options:
- Percutaneous pinning of the fracture with Kirschner wires
- Open reduction and pinning with Kirschner wires
- Arthroscopic in situ compression screw fixation
- Reduction and compression screw fixation via a volar approach
- Reduction and compression screw fixation via a dorsal approach
Correct Answer: Reduction and compression screw fixation via a dorsal approach
Explanation:
Displaced fractures of the scaphoid are best treated with compression screw fixation. Proximal third fractures (as in this patient) are optimally approached via a dorsal approach to ensure proper reduction and compression. Fractures of the scaphoid waist can be approached either by a volar or a dorsal approach. Kirschner wire fixation is limited to proximal pole fractures that are too small to accommodate the trailing head of a compression screw. Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.
References:
Filan SK, Herbert TJ: Herbert screw fixation of scaphoid fractures. J Bone Joint Surg Br 1996;78:519-529.
Question 18:
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?
Options:
- Metastatic focus
- Bony island
- Intravertebral disk herniation
- Osteoporosis
- Hemangioma
Correct Answer: Hemangioma
Explanation:
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
References:
Garfin SR, Vaccaro AR(eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 235-256.
Question 19:
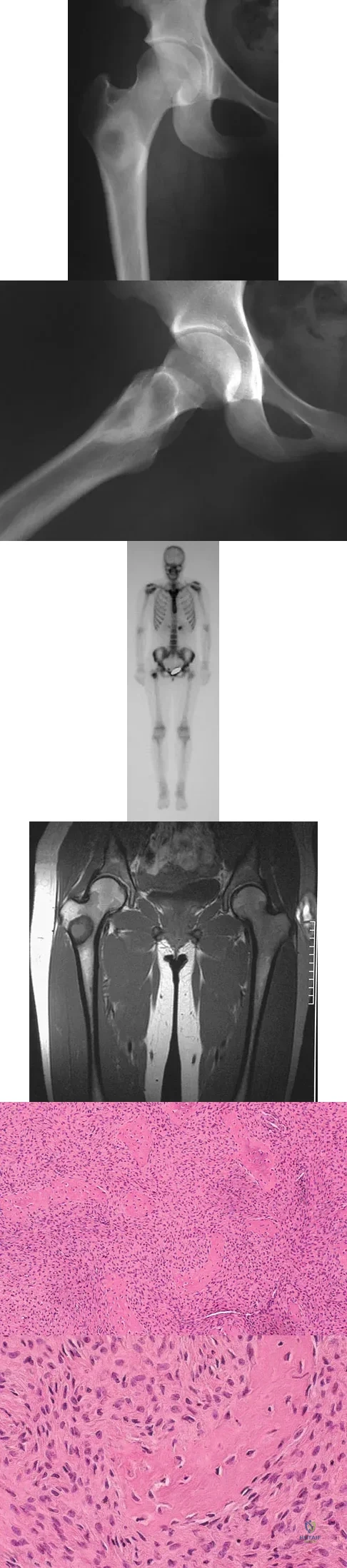
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
Options:
- Osteosarcoma
- Fibrous dysplasia
- Osteoblastoma
- Ossifying fibroma
- Osteomyelitis
Correct Answer: Fibrous dysplasia
Explanation:
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
References:
DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am 2005;87:1848-1864.
Question 20:
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient's ability to heal the wound postoperatively?
Options:
- Absolute toe pressures of 55 mm Hg
- Transcutaneous oxygen level of 20 mm Hg
- Arterial brachial indices (ABI) of 1.2 at the level of surgery
- ABI 0.3 at the level of surgery
- Albumin level of 2.5
Correct Answer: Absolute toe pressures of 55 mm Hg
Explanation:
Absolute toe pressures greater than 40 to 50 mm Hg are a good sign of healing potential. An ABI of greater than 0.45 favors healing, but indices greater than 1 are falsely positive due to calcifications in the vessels. Normal albumin is an overall indication of nutritional status. A transcutaneous oxygen level should be greater than 40 mm Hg for healing. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
References:
Pinzur MS, Stuck R, Sage R: Benchmark analysis on diabetics at high risk for lower extremity amputation. Foot Ankle Int 1996;17:695-700.
Question 21:
A characteristic genetic translocation has been noted in which of the following tumors?
Options:
- Ewing's sarcoma
- Chondrosarcoma
- Neurofibrosarcoma
- Osteosarcoma
- Epithelioid sarcoma
Correct Answer: Ewing's sarcoma
Explanation:
There have been no characteristic gene translocations or rearrangements noted in osteosarcoma, chondrosarcoma, neurofibrosarcoma, or epithelioid sarcoma. In contrast, Ewing's sarcoma has been noted to have a consistent genetic translocation t(11:22). Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
References:
Simon MA, Springfield DS, et al: Management of Surgical Specimens: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 67-75.
Question 22:
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Options:
- Sciatic nerve
- Cluneal nerves
- Inferior gluteal artery
- Superior gluteal artery
- Sacroiliac joint
Correct Answer: Superior gluteal artery
Explanation:
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
References:
Shin AY, Moran ME, Wenger DR: Superior gluteal artery injury secondary to posterior iliac crest bone graft harvesting: A surgical technique to control hemorrhage. Spine 1996;21:1371-1374.
Question 23:
A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
Options:
- core decompression.
- biopsy of the femoral head.
- protected weight bearing and observation.
- total hip arthroplasty.
- percutaneous cannulated pin fixation of the femoral neck.
Correct Answer: protected weight bearing and observation.
Explanation:
Transient osteoporosis of the hip is an uncommon problem, usually affecting women in the last trimester of pregnancy and middle-aged men. Symptoms include pain in the involved hip with temporary osteopenia; however, there is no joint space involvement. In this patient, the imaging findings are consistent with transient osteoporosis. Short TR/TE (repetition time/echo time) images reveal diffusely decreased signal intensity in the femoral head and intracapsular region of the femoral neck. Increased signal intensity is seen with increased T2-weighting. Within a few months, the pain, as well as the imaging findings, will completely resolve without intervention. Distinguishing the diffuse features of transient osteoporosis of the hip from the segmental findings of osteonecrosis is essential. Unlike transient osteoporosis of the hip, osteonecrosis will have a double-density signal on MRI and may progress radiographically. Surgical intervention and oral corticosteriods are not indicated for treatment. Protected weight bearing until the pain resolves may decrease symptoms while the transient osteoporosis resolves. Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229. Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.
References:
Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.
Question 24:
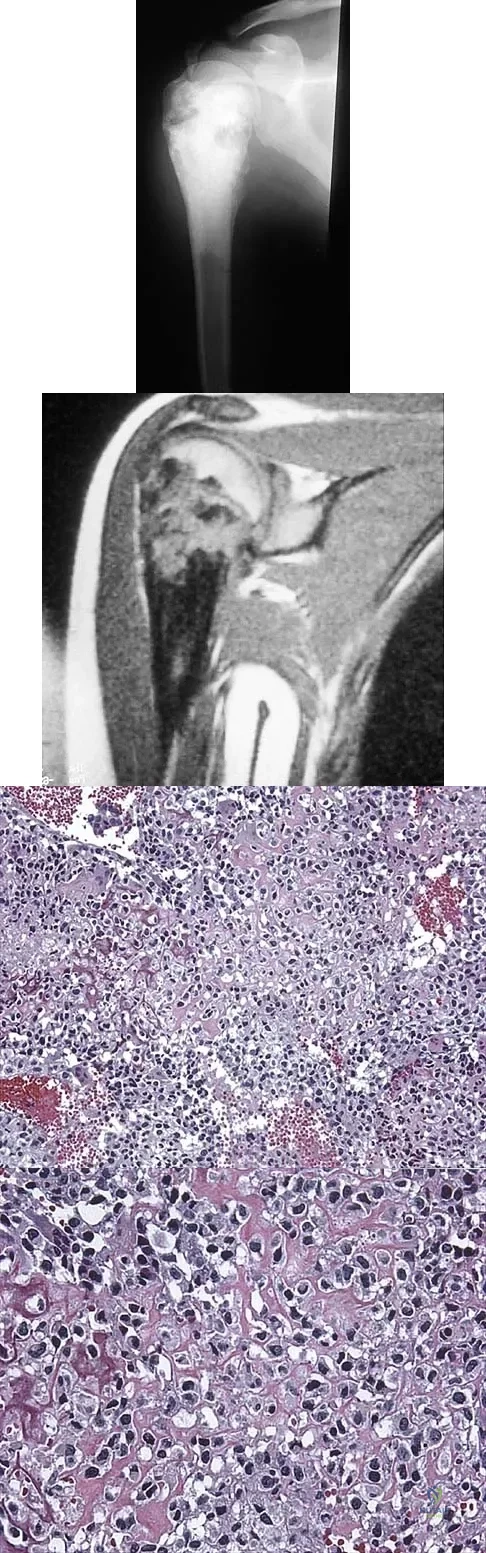
A 13-year-old girl has had a firm mass and pain in her right shoulder for the past several weeks. She denies any history of trauma. A radiograph and MRI scan are shown in Figures 31a and 31b. Biopsy specimens are shown in Figures 31c and 31d. What is the most likely diagnosis?
Options:
- Osteosarcoma
- Ewing's sarcoma
- Osteochondroma
- Chondrosarcoma
- Periosteal chondroma
Correct Answer: Osteosarcoma
Explanation:
The patient has osteosarcoma. The radiograph suggests an aggressive primary tumor of bone, and the histology shows malignant cells surrounded by osteoid, classic for osteosarcoma. Ewing's sarcoma histologically consists of small round blue cells. Osteochondroma and periosteal chondroma occur in the shoulder but have a different histologic pattern and a less aggressive radiographic appearance. Chondrosarcomas rarely occur in children. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
References:
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 25:
The inheritance of the deformity shown in Figure 1 is most commonly
Options:
- autosomal-recessive.
- autosomal-dominant.
- x-linked dominant.
- mitochondrial.
- sporadic.
Correct Answer: autosomal-dominant.
Explanation:
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
Scientific References
:
Kay SPJ: Cleft hand, in Green DP (ed): Green's Operative Hand Surgery. Philadelphia, Pa, Churchill Livingston, 1999, pp 402-414.
Question 26:
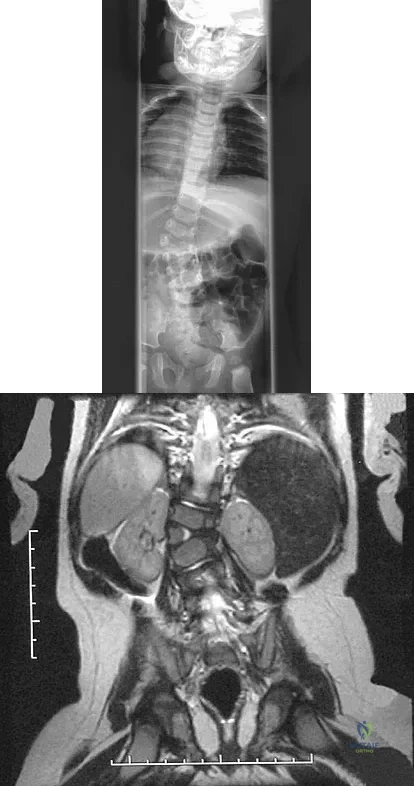
Figures 31a and 31b show the radiograph and MRI scan of an otherwise normal 3-month-old infant who has a spinal deformity. MRI reveals no intraspinal anomalies. What is the next step in management?
Options:
- Posterior spinal fusion with instrumentation
- Anterior-posterior hemiepiphysiodesis
- Brace management
- Cardiac and renal evaluation
- Hemivertebrectomy and fusion
Correct Answer: Cardiac and renal evaluation
Explanation:
Congenital scoliosis in an infant warrants evaluation of the renal, cardiac, and neurologic systems because frequently there is concurrent pathology. Progression in this instance is possible but not certain; therefore, progression must be documented prior to any surgical intervention. Close observation with serial radiographs every 4 to 6 months is appropriate. All of the surgical options listed may be reasonable choices in the future, but cardiac evaluation is the most important issue at this time. Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
References:
Hedequist D, Emans J: Congenital scoliosis. J Am Acad Orthop Surg 2004;12:266-275.
Question 27:
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6 degrees F (37 degrees C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Options:
- Continued resuscitation with fluids and blood
- Ongoing resuscitation and pelvic angiography
- Application of an external fixator in the emergency department
- A pelvic binder and continued resuscitation
- A pelvic binder, skeletal traction, and continued resuscitation
Correct Answer: A pelvic binder, skeletal traction, and continued resuscitation
Explanation:
The patient is at risk for a pelvic vascular injury and major hemorrhage. This type of complication of pelvic trauma is highest in motorcyclists. Once it is recognized that the pelvic ring has opened, it is important to close that ring to tamponade any venous bleeding with a pelvic binder and to add a skeletal traction pin to the limb on the involved side. This will correct any translational displacement. The noninvasive pelvic binders or sheets are easy to apply and are very effective. They do not compromise future care and allow the surgeons access to the abdomen. External fixation or pelvic resuscitation clamps require a certain amount of skill to apply and are not always available. If the pelvic stabilization does not improve the hemodynamic parameters in 10 to 15 minutes, angiography is necessary.
References:
Mayo K, Kellam JK: Pelvic ring disruptions, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1052-1108.
Question 28:
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?
Options:
- Stress radiographs to evaluate the ankle ligaments
- MRI to evaluate possible ligamentous injury
- CT to evaluate possible osteochondral injury
- Functional brace treatment
- Surgical repair of the ankle ligaments
Correct Answer: Functional brace treatment
Explanation:
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
References:
Hamilton WG: Sprained ankles in ballet dancers. Foot Ankle 1982;3:99-102.
Question 29:
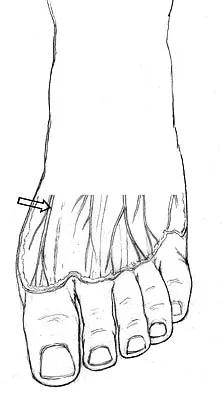
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Options:
- Saphenous
- Medial branch of the superficial peroneal
- Deep peroneal
- Posterior tibial
- Sural
Correct Answer: Medial branch of the superficial peroneal
Explanation:
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
References:
Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger, 2000, pp 963, 966.
Question 30:
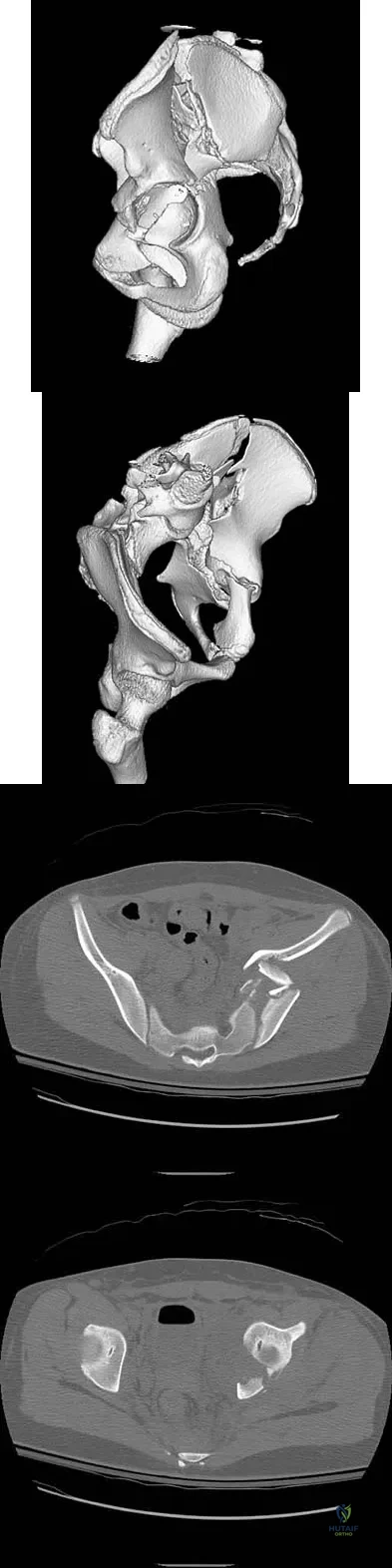
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Options:
- T-type
- Anterior column
- Both-column
- Anterior column posterior hemitransverse
- Posterior column
Correct Answer: Both-column
Explanation:
The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction of displacement. Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
References:
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 31:
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of
Options:
- in situ posterior fusion.
- hemivertebral resection and fusion.
- convex hemiepiphyseodesis.
- observation with follow-up in 6 months.
- thoracolumbosacral orthosis bracing.
Correct Answer: hemivertebral resection and fusion.
Explanation:
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
References:
Lazar RD, Hall JE: Simultaneous anterior and posterior hemivertebra excision. Clin Orthop 1999;364:76-84.
Question 32:
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Options:
- greater sciatic notch and passing between the inferior gemellus and the obturator externus.
- greater sciatic notch and passing between the piriformis and the superior gemellus.
- obturator foramen and passing between the obturator internus and the obturator externus.
- lesser sciatic notch and passing between the piriformis and the superior gemellus.
- lesser sciatic notch and passing between the superior gemellus and the inferior gemellus.
Correct Answer: greater sciatic notch and passing between the piriformis and the superior gemellus.
Explanation:
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
References:
Hollingshead WH: Anatomy for Surgeons: The Back and Limbs, ed 2. Hagerstown, MD, Harper & Row, 1969, pp 607-609.
Question 33:
Which of the following muscles attaches to the coracoid process of the scapula?
Options:
- Subscapularis
- Supraspinatus
- Pectoralis minor
- Long head of the biceps brachii
- Serratus anterior
Correct Answer: Pectoralis minor
Explanation:
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
References:
Jobe CM: Gross anatomy of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 49-66.
Question 34:
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Options:
- Surgical fixation with percutaneous pins
- Surgical fixation with a hemiarthroplasty with tuberosity repair
- Surgical fixation with a total shoulder arthroplasty
- Sling immobilization for 6 weeks followed by active range of motion
- Sling immobilization with daily pendulum exercises
Correct Answer: Surgical fixation with a hemiarthroplasty with tuberosity repair
Explanation:
The patient has a displaced four-part proximal humerus fracture. Given her age and the presence of osteopenia, a cemented hemiarthroplasty is the treatment of choice. The glenoid is uninjured so a total shoulder arthroplasty is not indicated. Percutaneous pinning in younger individuals with good bone quality may be indicated but not in an 82-year-old woman with osteopenia. Sling immobilization and immediate pendulum exercises will lead to a nonunion. Sling immobilization for 6 weeks followed by active range of motion will result in a nonunion or malunion with unacceptable functional results. Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
References:
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 352-354.
Question 35:
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have
Options:
- an increased need for revision.
- a greater limb-length discrepancy.
- a decreased rate of postoperative instability.
- a decreased rate of wear.
- a decreased rate of peroneal nerve palsy.
Correct Answer: an increased need for revision.
Explanation:
The rate of revision has been found to be significantly increased in patients with a dislocated hip preoperatively compared with patients with a subluxated hip. This may be the result of compromised acetabular bone stock. The rate of nerve palsy may be increased because of the greater degree of lengthening required to reduce the reconstructed hip. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
References:
Schmalzried TP, Noordin S, Amstutz HC: Update on nerve palsy associated with total hip replacement. Clin Orthop 1997;344:188-206.
Question 36:
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
Options:
- Physical therapy
- Hardware removal
- Repeat placement of a syndesmotic screw
- Deltoid ligament reconstruction
- Revision ORIF with exploration of the syndesmosis and medial ankle
Correct Answer: Revision ORIF with exploration of the syndesmosis and medial ankle
Explanation:
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction. Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.
References:
Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 37:
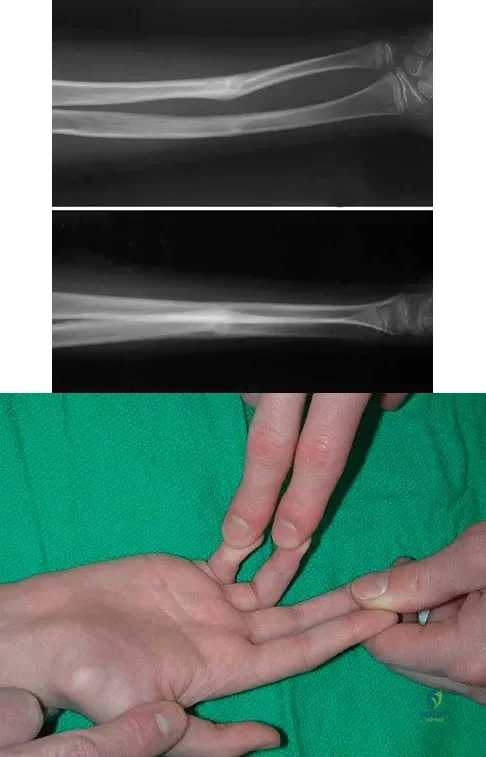
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?
Options:
- Unrecognized laceration of the extensor tendon to the ring and little fingers
- Unrecognized compartment syndrome
- Entrapment of the flexor digitorum profundus to the ring and little fingers
- Triggering at the A1 pulleys
- Ulnar nerve injury below the elbow
Correct Answer: Entrapment of the flexor digitorum profundus to the ring and little fingers
Explanation:
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
References:
Hendel D, Aner A: Entrapment of the flexor digitorum profundus of the ring finger at the site of an ulnar fracture: A case report. Ital J Orthop Traumatol 1992;18:417-419.
Question 38:
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?
Options:
- Arthroscopic debridement
- Arthrodesis
- Resection arthroplasty
- Hemiarthroplasty
- Cortisone injection
Correct Answer: Hemiarthroplasty
Explanation:
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
References:
Loebenberg MI, Plate AM, Zuckerman JD: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 39:
A 32-year-old football coach has had a 4-month history of increasing right wrist pain, particularly during blocking exercises, and he reports significant pain with range of motion and gripping activities. He denies any history of trauma. Examination reveals dorsal wrist tenderness and boggy fullness over the dorsum of the wrist. No erythema is noted. Grip strength is 60% compared with the opposite side. Radiographs are shown in Figures 5a and 5b. What is the most likely diagnosis?
Options:
- Scapholunate dissociation
- Triangular fibrocartilage tear
- Scaphoid fracture
- Perilunate dislocation
- Kienbock's disease
Correct Answer: Kienbock's disease
Explanation:
The patient has Kienbock's disease (osteonecrosis of the lunate), which presents with boggy synovitis of the wrist, decreased range of motion, and often normal radiographs. The patient's radiographs reveal small fragments from the lunate, with increased density in the lunate body. While a traumatic event may precede the patient's pain, often an insidious increase in pain is found. Repetitive trauma has been suggested as a possible cause. This disease process is classically associated with an ulnar-negative variant. An MRI scan, revealing a low-intensity signal in the lunate, is the best diagnostic tool for early Kienbock's disease. Green DP, Hotchkiss RN, Pederson WC: Green's Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
References:
Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
Question 40:
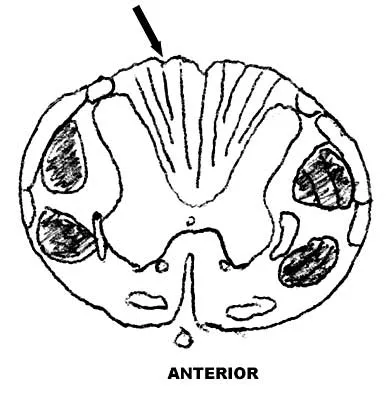
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
Options:
- Complete paraplegia
- Contralateral weakness below the level of the injury
- Ipsilateral weakness below the level of the injury
- Unilateral loss of position sense, proprioception, and vibratory sense below the level of the injury
- Loss of pain and temperature sensation below the level of the injury
Correct Answer: Unilateral loss of position sense, proprioception, and vibratory sense below the level of the injury
Explanation:
The arrow is pointing to the posterior columns of the spinal cord that transmit position sense, vibratory sense, and proprioception. There are no motor tracts in the posterior columns. Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
References:
Northrup B: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 545.
Question 41:
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
Options:
- triple arthrodesis.
- lateral column lengthening with flexor digitorum longus tendon transfer.
- medial calcaneal displacement osteotomy, flexor digitorum longus transfer, and gastrocnemius recession.
- midfoot arthrodesis.
- subtalar arthroereisis with a Maxwell-Brancheau Arthroereisis titanium implant.
Correct Answer: midfoot arthrodesis.
Explanation:
The patient has a degenerative collapse of the midfoot through the tarsometatarsal joints with significant forefoot abduction; therefore, a midfoot arthrodesis is required to address the arthritic joints and deformity at the tarsometatarsal articulation. All of the other procedures correct hindfoot deformities and therefore would not be appropriate treatment. Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
References:
Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am 1996;78:1376-1385.
Question 42:
During primary total knee arthroplasty, the trial components are in place. The extensor space is tight, but the flexion space is normal. What is the best gap balancing solution?
Options:
- Decrease the thickness of the tibial insert.
- Upsize the femoral component and distally augment the femur.
- Resect additional distal femoral bone.
- Resect additional distal femoral bone and proximal tibial bone.
- Resect the proximal tibial bone and distally augment the femoral component.
Correct Answer: Resect additional distal femoral bone.
Explanation:
The first rule of total knee arthroplasty is to restore the joint line to its original location. This will ensure optimal patellofemoral biomechanics and will facilitate ligament balancing. Changes on the tibial side affect both the flexion and extension gaps equally. Changes in femoral component sizing or position affect the flexion gap only. Tibial changes affect both the flexion and extension gaps. To convert a tight extension gap to a normal flexion gap, more distal femur needs to be resected. Vince KG: Revision knee arthroplasty technique. Instr Course Lect 1993;42:325-339.
References:
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 513-536.
Question 43:
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Options:
- Biceps femoris
- Lateral gastrocnemius
- Semimembranosus
- Semitendinosus
- Popliteus
Correct Answer: Lateral gastrocnemius
Explanation:
The radiograph shows a fabella, a sesamoid bone that is usually found within the tendon of the lateral head of the gastrocnemius. It can be confused with a loose body on radiographs. It occurs in 18% of patients and is often bilateral. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, pp 4-69.
Scientific References
:
Weissman BNW, Sledge CB (ed): Orthopaedic Radiology. Philadelphia, PA, WB Saunders, 1986, p 514.
Question 44:
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Options:
- Esophagus
- Trachea
- Superior laryngeal nerve
- Recurrent laryngeal nerve
- Sympathetic chain
Correct Answer: Recurrent laryngeal nerve
Explanation:
Although any of these structures can be injured by pressure from the medial blade of a self-retaining retractor, the recurrent laryngeal nerve runs cephalad in the interval between the esophagus and trachea and is vulnerable to pressure if caught between the retractor and an inflated endotracheal tube balloon. Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
References:
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 45:
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
Options:
- Melorheostosis
- Ectopic bone formation
- Bone infarct
- Infection
- Juxacortical chondroma
Correct Answer: Melorheostosis
Explanation:
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
References:
Kawabata H, Tsuyuguchi Y, Kawai H, et al: Melorheostosis of the upper limb: A report of two cases. J Hand Surg Am 1984;9:871-876.
Question 46:
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Options:
- MRI of the lesion, CT of the chest
- MRI of the lesion, chest, and abdomen, CT of the pelvis
- MRI of the lesion, chest, and abdomen, CT of the pelvis, bone scan
- MRI of the lesion, CT of the chest, sentinel node biopsy
- CT of the lesion and chest, bone scan
Correct Answer: MRI of the lesion, CT of the chest
Explanation:
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
References:
Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 47:
Which of the following is considered an important component in treating the lesion shown in Figure 56?
Options:
- Excision of the skin in addition to the cyst
- Resection of the nail plate
- Excision of bony osteophytes from the distal interphalangeal (DIP) joint
- Injection of corticosteroid into the DIP joint
- Resection of part of the collateral ligament and extensor mechanism
Correct Answer: Excision of bony osteophytes from the distal interphalangeal (DIP) joint
Explanation:
Mucoid cysts are commonly associated with DIP joint arthritis. Two treatment options are commonly used: (1) aspiration/drainage and injection of corticosteroid and (2) surgical excision. When performing the surgery, excision of the bony osteophytes about the DIP joint is helpful in achieving a cure. There are no reports of significant benefit with nail removal or partial ligament or extensor tendon resection. Some authors have advocated skin excision and rotational flaps for wound coverage, but this is somewhat controversial. Rizzo M, Beckenbaugh RD: Treatment of mucous cysts of the fingers: Review of 134 cases with minimum 2-year follow-up evaluation. J Hand Surg Am 2003;28:519-524.
References:
Eaton RG, Dobranski AI, Littler JW: Marginal osteophyte excision in treatment of mucous cysts. J Bone Joint Surg Am 1973;55:570-574.
Question 48:
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Options:
- Aseptic loosening
- Mortality
- Infection
- Bleeding
- Limited motion requiring manipulation
Correct Answer: Mortality
Explanation:
Parvizi and associates studied the 30-day mortality rate after more than 22,000 total knee arthroplasties and found that the rate after bilateral total knee arthroplasty was significantly higher than after unilateral total knee arthroplasty. Aseptic loosening, bleeding, and range of motion have not been shown to be statistically different between patients who had unilateral and simultaneous bilateral total knee arthroplasty.
References:
Parvizi J, Sullivan TA, Trousdale RT, Lewallen DG: Thirty-day mortality after total knee arthroplasty. J Bone Joint Surg Am 2001;83:1157-1161.
Question 49:
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Options:
- distal chevron bunionectomy.
- proximal first metatarsal osteotomy with distal soft-tissue realignment.
- double osteotomy of the first metatarsal with distal soft-tissue realignment.
- arthrodesis of the first metatarsophalangeal joint.
- Keller bunionectomy.
Correct Answer: arthrodesis of the first metatarsophalangeal joint.
Explanation:
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
References:
Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 50:
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Options:
- Involvement of the vertebral body and posterior elements
- Involvement of the thoracic vertebrae
- Involvement of the lumbar vertebrae
- Age of the patient
- Pretreatment degree of kyphosis
Correct Answer: Involvement of the vertebral body and posterior elements
Explanation:
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
References:
Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 51:
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of
Options:
- greater trochanter detachment.
- femoral stem loosening.
- wear.
- osteolysis.
- infection.
Correct Answer: wear.
Explanation:
Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability. Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
References:
Parvizi J, Wade FA, Rapuri VR, et al: Revision hip arthroplasty for late instability secondary to polyethylene wear. Clin Orthop 2006, in press.
Question 52:
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Options:
- external fixation with a circular frame.
- open reduction and internal fixation with screws.
- closed reduction and percutaneous pinning.
- closed reduction and cast immobilization.
- amputation.
Correct Answer: open reduction and internal fixation with screws.
Explanation:
The displaced talar neck fracture should be treated with open reduction and internal fixation using screws. Closed reduction and casting will not maintain position, and percutaneous pinning is not able to maintain reduction to allow union. External fixation and amputation are not necessary for this injury unless there is severe soft-tissue loss.
References:
Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 53:
The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
Options:
- Patients have the same likelihood of receiving disability whether treated with or without surgery.
- Sixty percent of surgically treated patients undergo at least one more operation within 5 years.
- Only 20% of patients treated with surgery report improved symptoms of back and/or leg pain.
- A smaller portion of surgical patients, compared to nonsurgically treated patients, report improvement.
- Fifty percent of patients treated nonsurgically seek surgery within 5 years.
Correct Answer: Patients have the same likelihood of receiving disability whether treated with or without surgery.
Explanation:
Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.
References:
Atlas SJ, Keller RB, Chang Y, et al: Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine 2001;26:1179-1187.
Question 54:
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?
Options:
- It may be difficult to obtain informed consent, even with an interpreter.
- The husband may be unwilling to allow his wife to have the appropriate surgery.
- Associated comorbidities in the patient increase the risk of surgical intervention.
- There is the potential of not being able to obtain a satisfactory CT scan because of claustrophobia.
- Postsurgical care may be jeopardized by the patient's role as caretaker for her children, thus compromising her ability to comply with weight-bearing restrictions.
Correct Answer: Postsurgical care may be jeopardized by the patient's role as caretaker for her children, thus compromising her ability to comply with weight-bearing restrictions.
Explanation:
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
References:
Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 55:
What is the main function of collagen found within articular cartilage?
Options:
- Compressive properties
- Tensile properties
- Proteoglycan synthesis
- Cartilage metabolism
- Joint lubrication
Correct Answer: Tensile properties
Explanation:
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
References:
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 56:
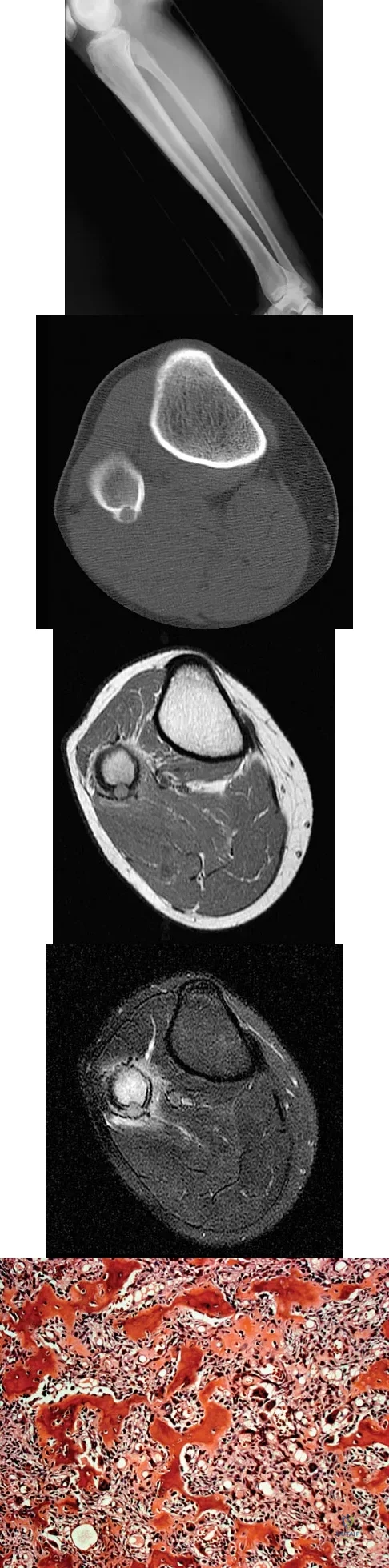
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Options:
- Osteoid osteoma
- Brodie's abscess
- Osteoblastoma
- Chondroblastoma
- Osteosarcoma
Correct Answer: Osteoid osteoma
Explanation:
The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
References:
Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 57:
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Options:
- Fewer complications
- Lower infection rate
- Evaluation of the glenohumeral joint
- Preservation of the inferior acromioclavicular ligament
- Decreased surgical time
Correct Answer: Evaluation of the glenohumeral joint
Explanation:
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
References:
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 58:
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Options:
- Ruptured biceps tendon
- Subscapularis tear
- Anterior subluxation
- Internal impingement syndrome
- Locked posterior dislocation
Correct Answer: Subscapularis tear
Explanation:
A positive lift-off test and increased passive external rotation are diagnostic of a subscapularis tear or detachment. Although a similar injury could produce anterior instability, this will test the integrity of the subscapularis. A locked dislocation has limited passive movement. A ruptured biceps tendon will most likely produce ecchymosis and findings similar to supraspinatus trauma. Internal impingement is not associated with subscapularis weakness. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 59:
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?
Options:
- Medial cord
- Lateral cord
- Posterior cord
- Upper trunk
- Lower trunk
Correct Answer: Posterior cord
Explanation:
From proximal to distal, the brachial plexus is divided into roots, trunks, divisions, and cords before forming specific peripheral nerve branches. The structure marked Q is called the posterior cord because it lies posterior to the axially artery at the level of the cords. Its terminal branches are the upper subscapular (V), thoracodorsal (W), lower subscapular (X), axillary (F), and radial (G) nerves. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-24.
References:
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 63.
Question 60:
Examination of a hand with compartment syndrome is most likely to reveal which of the following?
Options:
- Clenched fist
- Intrinsic minus posturing
- Pain with passive stretch
- Compression of the superficial arch
- Pallor
Correct Answer: Intrinsic minus posturing
Explanation:
In a study of 19 patients with compartment syndrome of the hand, all had tense swollen hands with elevated compartment pressures. Most patients were neurologically compromised so pain with passive stretch may be difficult to illicit. Arterial inflow is present in the arch and thus pallor is not present. The typical posture of the hand is not clenched, rather it is an intrinsic minus posture of metacarpophalangeal joint extension and flexion of the proximal and distal interphalangeal joints. Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
References:
Dellaero DT, Levin LS: Compartment syndrome of the hand: Etiology, diagnosis, and treatment. Am J Orthop 1996;25:404-408.
Question 61:
What is the function of the rotator cuff during throwing?
Options:
- Limits humeral head translation in the transverse plane but not in the sagittal plane
- Limits superior migration but not anterior and posterior translation
- Limits superior migration and anterior and posterior translation
- Provides little control of superior anterior and posterior translation
- Creates inferior migration with maximal contraction during acceleration
Correct Answer: Limits superior migration and anterior and posterior translation
Explanation:
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
References:
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 62:
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Options:
- external traction.
- open reduction and internal stabilization.
- repeat closed reduction under general anesthesia.
- open reduction.
- percutaneous pin fixation in the current position.
Correct Answer: open reduction.
Explanation:
The radiographs show a complex dislocation of the little finger metacarpophalangeal joint. This is characterized by obvious dislocation on the AP and lateral views and a type of bayonet apposition best visualized on the lateral view. Irreducibility of this injury is caused by displacement of the volar plate that has been traumatically avulsed from its origin on the metacarpal, with subsequent displacement into the metacarpophalangeal joint. This abnormal position of the volar plate causes irreducibility that can be corrected only by open reduction. This can be effected either by dorsal or palmar approaches. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
References:
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 63:
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Options:
- Diminished revascularization of cancellous bone graft
- Increased activity of osteoblasts
- Increased activity of osteocytes
- Antibody-induced necrosis
- Inhibition of prostaglandins
Correct Answer: Diminished revascularization of cancellous bone graft
Explanation:
Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.
References:
Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 64:
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Options:
- volar open reduction and pinning.
- open reduction, ligament repair, and pinning.
- closed reduction and splinting.
- closed reduction and pinning.
- dorsal open reduction and pinning.
Correct Answer: closed reduction and splinting.
Explanation:
The radiograph shows a volarly dislocated lunate. Initial emergent treatment of perilunate dislocations should consist of closed reduction and splinting, especially if the patient exhibits median nerve compression. Open reduction and pinning or ligament repair are necessary but are not emergent. A dorsal approach is sometimes required for ligament repair or bony visualization; however, this can be done in a more semi-elective manner. Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
References:
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 65:
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?
Options:
- Subluxation of more than 3.5 mm at one or more motion segments
- Dynamic angulation of more than 11 degrees at one or more motion segments
- Subaxial cervical lordosis of more than 25 degrees (as measured from C2 to C7)
- Fixed kyphosis of more than 10 degrees
- Anteroposterior spinal canal diameter of less than 8 mm
Correct Answer: Fixed kyphosis of more than 10 degrees
Explanation:
Although cervical instability is a contraindication to posterior decompression alone, segmental instability in the myelopathic cervical spine can be addressed with concomitant posterior fusion with instrumentation. Cervical lordosis represents the ideal scenario for posterior decompressive procedures for myelopathy (laminectomy and laminoplasty) because compression from anterior osteophytes, if present, is relieved as the spinal cord migrates posteriorly. The anteroposterior diameter of the spinal canal does not have an impact on the selection of surgical approach. Posterior unroofing-type procedures in kyphotic cervical spines, however, are ineffective because anterior impingement on the spinal cord will remain; therefore, kyphosis of more than 10 degrees is considered a contraindication for posterior decompression. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
References:
Malone DG, Benzel EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-823.
Question 66:
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing's sarcoma. Following induction chemotherapy, local control typically consists of
Options:
- radiation therapy only.
- curettage and bone grafting.
- wide resection.
- below-knee amputation.
- observation.
Correct Answer: wide resection.
Explanation:
The current treatment regimen for Ewing's sarcoma typically involves induction chemotherapy followed by local control and further chemotherapy. Local control consists of surgery only, radiation therapy only, or a combination of the two. In bones that are easily resectable (expendable) with wide margins, surgery is usually recommended. For areas that cannot be resected (ie, large bulky pelvic tumors), radiation therapy alone is sometimes the preferred method of local control. If surgery is chosen and the margins are close, radiation therapy can be used as an adjuvant treatment. Amputation is rarely required for an isolated fibular lesion. Observation without adequate local control results in local recurrence. Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing's sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
References:
Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 67:
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Options:
- observation.
- wide resection.
- radiation therapy.
- extended curettage.
- chemotherapy.
Correct Answer: extended curettage.
Explanation:
An aneurysmal bone cyst is a benign, locally destructive lesion of bone. Most are seen in patients in the second decade of life. The clinical presentation varies, but most patients have pain, tenderness, swelling, and/or pathologic fracture. Radiographs show a radiolucent lesion sometimes with expansile remodeling of the cortex. MRI best detects the commonly seen fluid-fluid levels associated with this lesion. Histologic findings include blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute). Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
References:
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 68:
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Options:
- Bone scan
- Curettage and bone grafting of the cyst
- Cast immobilization
- Observation with reduced activity
- Skeletal survey
Correct Answer: Observation with reduced activity
Explanation:
The most likely diagnosis is Sever's disease, which is considered either an apophysitis or a para-apophyseal stress fracture. It is common in athletic children and is associated with a tight Achilles tendon. Cast immobilization may be necessary if activity reduction fails. Calcaneal cysts are quite common and do not require any further diagnostic testing or treatment unless they occupy the full width of the calcaneus or one third of the length of the calcaneus. Ogden JA, Ganey TM, Hill JD, et al: Sever's injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
References:
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 69:
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Options:
- A Pavlik harness with the hips in 90 degrees of flexion and 60 degrees of abduction
- A spica cast with the hips in 100 degrees of flexion and 70 degrees of abduction
- Observation with range-of-motion exercises to minimize contractures
- Open reduction through an anterior hip approach
- Open reduction through a medial hip approach
Correct Answer: Observation with range-of-motion exercises to minimize contractures
Explanation:
The status of the hips (located or dislocated) in children with thoracic-level myelomeningocele has no effect on the functional outcome of these patients. Management of unstable hips in this population should be limited to treatment of the contractures that may lead to poor limb positioning in either braces or a wheelchair. The use of the Pavlik harness and/or spica cast is contraindicated because they would promote flexion and abduction contractures. In the past, open reduction either through an anterior or medial approach had been performed with a high incidence of redislocation and other complications, with little functional gain for the child. Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
References:
Schoenecker PL: Surgical management of hip problems in children with myelomeningocele, in Sarwark KR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 117-131.
Question 70:
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of
Options:
- open release of the posterior capsule.
- arthroscopic release of the rotator cuff interval.
- arthroscopic release of the anteroinferior capsule.
- open subscapularis lengthening.
- open extra-articular release.
Correct Answer: arthroscopic release of the rotator cuff interval.
Explanation:
When external rotation at the side is limited, the most likely diagnosis is contracture of the rotator cuff interval, including the superior glenohumeral and coracohumeral ligaments. Therefore, the treatment of choice is arthroscopic release of the rotator cuff interval.
References:
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 71:
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of
Options:
- spinal accessory nerve exploration with repair.
- long thoracic nerve exploration with repair.
- a sling for comfort, followed by shoulder strengthening exercises.
- scapulothoracic arthrodesis.
- split pectoralis major transfer.
Correct Answer: a sling for comfort, followed by shoulder strengthening exercises.
Explanation:
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis. Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
References:
Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 72:
What is the function of the rotator cuff during throwing?
Options:
- Limits humeral head translation in the transverse plane but not in the sagittal plane
- Limits superior migration but not anterior and posterior translation
- Limits superior migration and anterior and posterior translation
- Provides little control of superior anterior and posterior translation
- Creates inferior migration with maximal contraction during acceleration
Correct Answer: Limits superior migration and anterior and posterior translation
Explanation:
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
References:
Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 73:
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Options:
- mobilization in a kinetic therapy bed for 8 weeks.
- initiation of a steroid protocol.
- immediate laminectomy of T7, T8, and T9.
- application of a total contact orthosis.
- open reduction and posterior segmental stabilization and grafting.
Correct Answer: open reduction and posterior segmental stabilization and grafting.
Explanation:
With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
References:
Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
Question 74:
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Options:
- observation and splinting.
- local wound drainage under local anesthesia.
- incision and drainage, deep wound cultures, removal of the plates and screws, and cast application.
- incision and drainage, deep wound cultures, and removal of the fixation only if it is loose.
- incision and drainage, deep wound cultures, and bone grafting.
Correct Answer: incision and drainage, deep wound cultures, and removal of the fixation only if it is loose.
Explanation:
Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63. Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
References:
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Question 75:
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Options:
- Flexion contracture of 5 degrees
- Subchondral cyst in the medial tibial condyle
- Lateral meniscal degeneration seen in an MRI scan
- Rheumatoid arthropathy
- Previous medial meniscectomy
Correct Answer: Rheumatoid arthropathy
Explanation:
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
References:
Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 76:
Figures 40a and 40b show the pre- and postoperative radiographs of an 82-year-old woman with bilateral hip pain who has had staged total hip arthroplasties. To minimize potential injury to the sciatic nerve at the time of surgery, the surgeon should
Options:
- perform a femoral shortening.
- perform a sciatic neurolysis.
- release the piriformis tendon.
- avoid use of posterior acetabular retractors.
- apply postoperative abduction bracing.
Correct Answer: perform a femoral shortening.
Explanation:
To improve hip biomechanics and secure more suitable bone for acetabular fixation, the true acetabulum is often resurfaced in patients who have developmental dysplasia of the hip, thus lowering the hip center and lengthening the leg. Acute lengthening of more than 3 cm will place excessive tension on the sciatic nerve and require a femoral shortening to avoid sciatic nerve injury. The other maneuvers will not relieve sciatic nerve tension because of limb lengthening. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 430-431.
References:
Sanchez-Sotelo J, Berry DJ, Trousdale RT, et al: Surgical treatment of developmental dysplasia of the hip in adults: II. Arthroplasty options. J Am Acad Orthop Surg 2002;10:334-344.
Question 77:
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
Options:
- Synovial sarcoma
- Infection
- Pigmented villonodular synovitis
- Malignant fibrous histiocytoma
- Synovial chondromatosis
Correct Answer: Pigmented villonodular synovitis
Explanation:
Pigmented villonodular synovitis often presents with intermittent swelling and minimal pain. It often occurs around joints but may be found around tendon sheaths and bursal linings. Periarticular erosions involving both sides of joints are typical, and multiple joint involvement has been described. Portions of low-signal intensity on T1- and T2-weighted images are characteristic of hemosiderin-laden processes. High-signal content is suggestive of high water content. The combination of low-signal intensity areas in intra-articular lesions with or without osseous destruction is diagnostic of pigmented villonodular synovitis. Aspiration reveals bloody or brownish fluid. The treatment of choice is synovectomy performed arthroscopically or open. Recurrence is common. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
References:
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 36.
Question 78:
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Options:
- Superior labrum anterior and posterior lesion, type III
- Isolated traumatic dislocation
- Axillary nerve disruption
- Subscapularis rupture
- Internal impingement
Correct Answer: Subscapularis rupture
Explanation:
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
References:
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 79:
What is the most common anatomic location for chondrosarcoma?
Options:
- Hand
- Distal femur
- Proximal humerus
- Spine
- Pelvis
Correct Answer: Pelvis
Explanation:
The most common anatomic location of chondrosarcoma is the pelvis (30%), followed by the proximal femur (20%). Chondrosarcomas appear in the shoulder girdle in 15% of patients but rarely affect the spine or hands. Marcove RC, Mike V, Hutter RV, et al: Chondrosarcoma of the pelvis and upper end of the femur: An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am 1972;54:561-572.
References:
Simon MA, Springfield DS, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 80:
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Options:
- Immediate MRI of the brain
- Physical therapy and observation
- Subacromial injection
- Decompression of the suprascapular nerve at the suprascapular notch
- Decompression of the infraspinatus branch of the suprascapular nerve at the spinoglenoid notch
Correct Answer: Physical therapy and observation
Explanation:
Suprascapular nerve injuries are more commonly seen in athletes who participate in overhead activities. When a patient is evaluated for posterior shoulder pain and infraspinatus muscle weakness or atrophy, electrodiagnostic studies are an essential part of the evaluation. In addition, imaging studies are indicated to exclude other diagnoses that can mimic a suprascapular nerve injury. Initial management should consist of cessation of the aggravating activity along with an organized shoulder rehabilitation program. If nonsurgical management fails to provide relief within 6 months to 1 year, surgical exploration of the suprascapular nerve should be considered. Release of the spinoglenoid ligament with resultant suprascapular nerve decompression may result in pain relief and a return of normal shoulder function. In this patient, who has a chronic neuropathy and mild symptoms, surgery is indicated only if nonsurgical management fails to provide relief and he is unable to perform at his position. Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
References:
Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 81:
In the most common condition causing a winged scapula, which of the following nerves is affected?
Options:
- Long thoracic nerve
- Spinal accessory nerve
- Suprascapular nerve
- Dorsal scapular nerve
- Thoracodorsal nerve
Correct Answer: Long thoracic nerve
Explanation:
A winged scapula is most often associated with Parsonage-Turner syndrome, a condition thought to be due to an inflammatory or immune-mediated mechanism. Certain muscles are predisposed, particularly the serratus anterior muscle innervated by the long thoracic nerve. Other less common nerve lesions (eg, the spinal accessory and dorsal scapular nerves) may also cause winged scapulae. Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995.
References:
van Alfen N, van Engelen BG: The clinical spectrum of neuralgic amyotrophy in 246 cases. Brain 2006;129:438-450.
Question 82:
What is the most common reason for reoperation in total knee arthroplasty?
Options:
- Polyethylene insert failure
- Malalignment of the knee
- Ligamentous instability
- Perioperative infection
- Patellar-related complications
Correct Answer: Patellar-related complications
Explanation:
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
References:
Wilson MG, Kelley K, Thornhill TS : Infection as a complication of total knee-replacement arthroplasty: Risk factors and treatment in sixty-seven cases. J Bone Joint Surg Am 1990;72:878-883.
Question 83:
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Options:
- Neurophysiologic test to evaluate the posterior interosseous nerve
- Transfer of the extensor indicis proprius to the extensor pollicis longus tendon
- Interphalangeal joint arthrodesis of the thumb
- Extension splinting of the thumb
- Fine cut CT of the distal radius to evaluate Lister's tubercle
Correct Answer: Transfer of the extensor indicis proprius to the extensor pollicis longus tendon
Explanation:
Extensor pollicis longus tendon rupture can occur after a fracture of the distal radius, even a minimally displaced one. Poor vascularity of the tendon within the third dorsal compartment is the suspected etiology, not the displaced fracture fragments. Tendon transfer will suitably restore active extension of the thumb interphalangeal joint. Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
References:
Hove LM: Delayed rupture of the thumb extensor tendon: A 5-year study of 18 consecutive cases. Acta Orthop Scand 1994;65:199-203.
Question 84:
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Options:
- Cemented polyethylene socket
- Cemented metal-backed socket
- Cementless hydroxyapatite-coated smooth metal-backed socket
- Cementless threaded metal-backed socket
- Cementless porous-coated metal-backed socket
Correct Answer: Cementless porous-coated metal-backed socket
Explanation:
Poor survivorship of cemented sockets in young patients has lead to the development of a variety of cementless designs. Of these, smooth metal-backed sockets have not performed as well as porous-coated designs. Threaded metal-backed sockets showed a 6% to 25% revision rate secondary to aseptic loosening at a mean follow-up of 4.5 to 6 years. Despite some early failed designs, cementless porous-coated metal-backed sockets have shown the best survivorship in long-term studies. Smith SE, Harris WH: Total hip arthroplasty performed with insertion of the femoral component with cement and the acetabular component without cement: Ten to thirteen-year study. J Bone Joint Surg Am 1997;79:1827-1833.
References:
Pellicci PM, Tria AJ Jr, Garvin KL, (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 195-206.
Question 85:
Split posterior tibial tendon transfer is used in the treatment of children with cerebral palsy. Which of the following patients is considered the most appropriate candidate for this procedure?
Options:
- A 6-year-old child with athetosis and a flexible equinovarus deformity of the foot
- A 6-year-old child with spastic hemiplegia and a rigid equinovarus deformity of the foot
- A 6-year-old child with spastic hemiplegia and a flexible equinovarus deformity of the foot
- A 10-year-old child with spastic quadriplegia and rigid valgus deformities of the feet
- A 15-year-old child with spastic diplegia and rigid equinovalgus deformities of the feet
Correct Answer: A 6-year-old child with spastic hemiplegia and a flexible equinovarus deformity of the foot
Explanation:
Split posterior tibial tendon transfers are best performed in patients with spastic cerebral palsy who are between the ages of 4 and 7 years and have flexible equinovarus deformities. Rigid deformities typically require bony reconstruction procedures. Tendon transfers in patients with athetosis are unpredictable. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in spastic cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
References:
Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 2, pp 1142-1152.
Question 86:
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the
Options:
- superior gluteal nerve laterally and the obturator nerve medially.
- superior gluteal nerve laterally and the femoral nerve medially.
- superior gluteal nerve medially and the femoral nerve laterally.
- superior gluteal nerve medially and the inferior gluteal nerve laterally.
- femoral nerve laterally and the obturator nerve medially.
Correct Answer: superior gluteal nerve laterally and the femoral nerve medially.
Explanation:
In the Smith-Petersen approach to the hip, dissection is carried out between the tensor fascia lata laterally (supplied by the superior gluteal nerve) and the sartorius and rectus femoris medially (both supplied by the femoral nerve). Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 82-85.
References:
Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 638-639.
Question 87:
A 63-year-woman has an elbow flexion contracture. History reveals that she underwent three previous surgeries to remove a malignant fibrous histiocytoma of the forearm. An MRI scan reveals a locally recurrent tumor at the site of the previous surgery. Which of the following is considered the most predictive factor for local recurrence?
Options:
- Tumor grade
- Tumor size
- Surgical margin
- Anatomic site of the tumor
- Histologic subtype of the tumor
Correct Answer: Surgical margin
Explanation:
The greatest risk factor for local recurrence is an inadequate surgical margin. The tumor grade, histologic subtype, and size are predictive of systemic relapse. Sarcomas that arise in some anatomic sites, such as the forearm or retroperitoneum, may be more difficult to completely resect compared with other sites. The optimum margin is generally considered to be a cuff of normal tissue beyond the tumor. Bell RS, O'Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375. Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J: Preoperative radiation, surgical margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;52:223-230.
References:
Wilson AN, Davis A, Bell RS, et al: Local control of soft tissue sarcoma of the extremity: The experience of a multidisciplinary sarcoma group with definitive surgery and radiotherapy. Eur J Cancer 1994;30:746-751.
Question 88:
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Options:
- Injury to the anterior band of the medial collateral ligament
- Injury to the radial nerve
- Injury to the lateral ulnar collateral ligament
- Injury to the lateral radial collateral ligament
- Excessive dissection of the extensor carpi radialis brevis origin
Correct Answer: Injury to the lateral ulnar collateral ligament
Explanation:
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
References:
O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 89:
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Options:
- Fracture comminution
- Displacement of 1 mm at the fracture site
- Involvement of the ischial facet
- Femoral head subluxation during fluoroscopic examination
- Presence of a bilateral pneumothorax
Correct Answer: Femoral head subluxation during fluoroscopic examination
Explanation:
Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized. Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
References:
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
Question 90:
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Options:
- Major long tubular bones
- Flat bones of the pelvis
- Fibula
- Metacarpals
- Vertebral bodies
Correct Answer: Major long tubular bones
Explanation:
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
References:
Wold LA, et al: Ewing's Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 91:
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Options:
- Partial tear of the patellar tendon
- Osteochondral fracture of the femur
- Anterior cruciate ligament (ACL) tear
- Posterior cruciate ligament (PCL) tear
- Patella fracture
Correct Answer: Posterior cruciate ligament (PCL) tear
Explanation:
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
References:
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 92:
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Options:
- There is a linear relationship between biosynthetic activity and the number of chondrocytes seeded.
- Osteochondral lesions of 12 mm in size may be treated with chondrocyte transplantation alone.
- Mesenchymal stem cells are harvested and allowed to differentiate to chondrocytes ex vivo.
- The cellular carrier has no effect on biosynthetic activity.
- In animal studies using fluorescent-labeled articular chondrocytes, donor cells are found to persist for up to 5 years.
Correct Answer: There is a linear relationship between biosynthetic activity and the number of chondrocytes seeded.
Explanation:
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
References:
Caplan AI, Elyaderani M, Mochizuki Y, et al: Principles of cartilage repair and regeneration. Clin Orthop 1997;342:254-269.
Question 93:
Examination of a 34-year-old man who has had left leg pain for the past 6 weeks reveals minimal weakness of the left extensor hallucis longus and normal ankle jerk and patellar reflexes. Figure 33 shows an axial MRI scan of the L4-5 disk. Based on these findings, the MRI scan results are consistent with compression of the
Options:
- traversing L4 nerve root and the patient's history and examination.
- traversing L4 nerve root but inconsistent with the patient's history and examination.
- traversing L5 nerve root and the patient's history and examination.
- traversing L5 nerve root but inconsistent with the patient's history and examination.
- exiting L5 nerve root and the patient's history and examination.
Correct Answer: traversing L5 nerve root and the patient's history and examination.
Explanation:
The patient has an L5 radiculopathy secondary to an L4-5 disk herniation that is compressing the traversing L5 nerve root.
References:
McCulloch JA, Young PH: Essentials of Spinal Microsurgery. Philadelphia, PA, Lippincott-Raven, 1998.
Question 94:
What is the most common foot deformity associated with myelomeningocele?
Options:
- Talipes equinovarus
- Congenital vertical talus
- Calcaneus valgus
- Calcaneus varus
- Cavus
Correct Answer: Talipes equinovarus
Explanation:
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
References:
Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001, pp 622-628.
Question 95:
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Options:
- increased bone turnover in the cortical area.
- inhibition of osteoclast-mediated bone resorption.
- improved mineralization of cortical bone.
- improved osteoblast organic matrix production.
- improved organization of collagen matrix.
Correct Answer: inhibition of osteoclast-mediated bone resorption.
Explanation:
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
References:
Glorieux FH, Bishop NJ, Plotkin H, et al: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1998;339:947-952.
Question 96:
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Options:
- increased abduction.
- pronation.
- flexion.
- flexion and pronation.
- extension.
Correct Answer: flexion and pronation.
Explanation:
The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
References:
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 97:
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?
Options:
- Hemangioma
- Ewing's sarcoma
- Clear cell sarcoma
- Malignant fibrous histiocytoma
- Synovial sarcoma
Correct Answer: Synovial sarcoma
Explanation:
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
References:
Bullough PG: Atlas of Orthopedic Pathology with Clinical and Radiologic Correlations, ed 2. New York, NY, Gower, 1992, p 17.23.
Question 98:
What preoperative factor correlates best with the outcome of rotator cuff repair?
Options:
- Size of the tear
- Age of the patient
- Arm dominance
- Rupture of the long head of the biceps
- Preoperative pain score
Correct Answer: Size of the tear
Explanation:
The size of the rotator cuff tear in both anteroposterior and mediolateral dimensions has been found to correlate best with outcome. Older patient age and rupture of the long head of the biceps tend to be associated with larger tears and, therefore, may be associated indirectly with a poorer outcome. Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 99:
The mother of a healthy 8-month-old boy reports that her son refuses to use his left arm. Examination reveals that the arm hangs limp at his side in an adducted and internally rotated position, and the affected shoulder subluxates posteriorly. Passive external rotation measures 15 degrees. Management should consist of
Options:
- release of the latissimus dorsi and teres major.
- release of the subscapularis and pectoralis major.
- passive range-of-motion exercises.
- exploration of the brachial plexus.
- functional bracing.
Correct Answer: passive range-of-motion exercises.
Explanation:
Injury to the upper trunk of the brachial plexus during birth (Erb's palsy) occurs in approximately 1 in 3,000 births. In a complete lesion, paralysis of the deltoid, supraspinatus, infraspinatus, teres minor, biceps, and brachioradialis results in the findings described above. Spontaneous recovery may occur for up to 2 years. Passive exercises administered daily by the parents are the initial recommended treatment at this age. If significant contracture results in posterior dislocation, surgical correction may be considered. Neer CS: Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 452-454. Pearl ML: Arthroscopy release of shoulder contracture secondary to birth palsy: An early report on findings and surgical technique. Arthroscopy 2003;19:577-582.
References:
Pearl ML, Edgerton BW, Kon DS, et al: Comparison of arthroscopic findings with MRI and arthrography in children with GH deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 2003;85:890-898.
Question 100:
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
Options:
- Osteonecrosis
- Transient osteoporosis
- Loose chondral fragment
- Labral tear
- Femoral neck stress fracture
Correct Answer: Labral tear
Explanation:
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
References:
McCarthy JC: The diagnosis and treatment of labral and chondral injuries. Instr Course Lect 2004;53:573-577.