Full Question & Answer Text (for Search Engines)
Question 1:
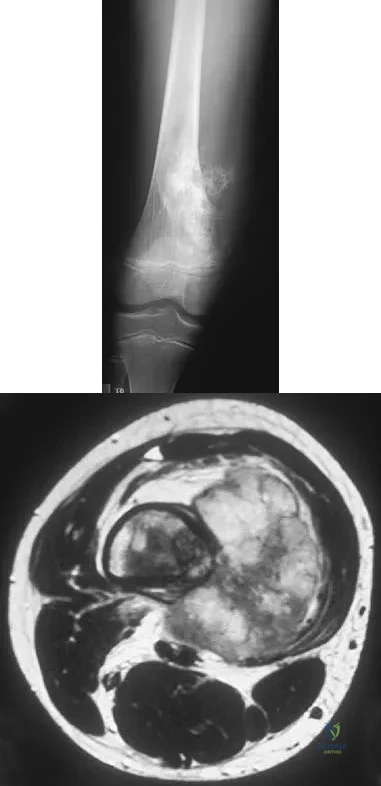
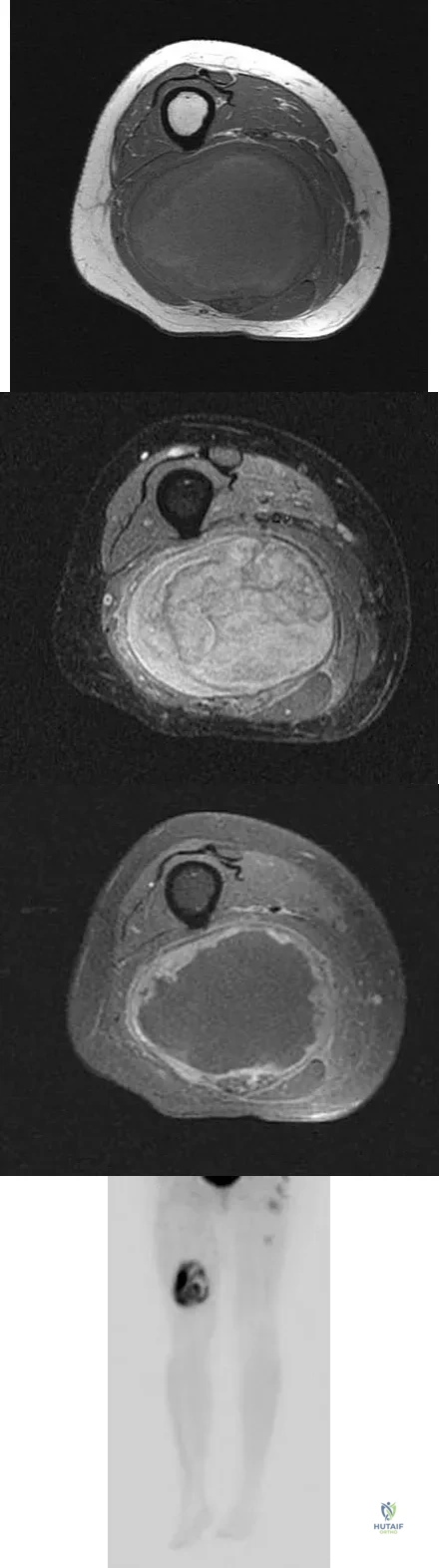
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Options:
- Osteosarcoma
- Osteochondroma
- Ewing's sarcoma
- Chondrosarcoma
- Periosteal chondroma
Correct Answer: Osteosarcoma
Explanation:
The most likely diagnosis is osteosarcoma. The imaging studies show an aggressive primary tumor of bone, and the histology slide shows a typical chondroblastic osteosarcoma, with osteoid deposited along the surface of bone trabeculae. Ewing's sarcoma histologically consists of small round blue cells. Osteochondroma and periosteal chondroma can occur near the knee but have different radiographic and histologic patterns. Chondrosarcoma rarely occurs in children. Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
References:
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 2:
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Options:
- close observation with frequent neurovascular checks.
- emergency angiography.
- emergency exploration of the brachial artery.
- removal of pin fixation and exploration of the brachial artery.
- thrombectomy.
Correct Answer: close observation with frequent neurovascular checks.
Explanation:
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
References:
Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 3:
What nerve is most likely to be injured during the anterior exposure of C2-3?
Options:
- Facial
- Superior laryngeal
- Vagus
- Hypoglossal
- Phrenic
Correct Answer: Hypoglossal
Explanation:
The hypoglossal nerve exits from the ansa cervicalis at approximately the C2-3 level and can be injured during retraction up to the C2 level. The superior laryngeal nerve lies at about C4-5. The facial nerve is much higher. The vagus nerve runs with the internal jugular and carotid much more laterally. The phrenic nerve exits posteriorly. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.
References:
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 4:
What is the main function of collagen found within articular cartilage?
Options:
- Compressive properties
- Tensile properties
- Proteoglycan synthesis
- Cartilage metabolism
- Joint lubrication
Correct Answer: Tensile properties
Explanation:
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
References:
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 5:
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Options:
- Before Risser 1 and menarche
- After Risser 1 and menarche
- Between Risser 1 and menarche
- After menarche but before Risser 1
- At Risser 2
Correct Answer: Before Risser 1 and menarche
Explanation:
PHV generally occurs while girls are still Risser 0; menarche typically occurs before Risser 1, which has a wide variation in its timing. The curve magnitude at the PHV is the best prognostic indicator available. Most untreated patients with curves greater than 30 degrees at PHV require surgery, while patients with smaller curves at that stage typically do not require surgery. Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
References:
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 6:
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include
Options:
- closed management of the medial condyle and humeral shaft fractures and open reduction and internal fixation of the both bones forearm fracture.
- closed management of the humeral shaft fracture and open reduction and internal fixation of the medial condyle and the both bones forearm fractures.
- open reduction and internal fixation of the humeral shaft, medial condyle, and the both bones forearm fractures.
- open reduction and internal fixation of the medial condyle and both bones forearm fractures, and external fixation of the humeral shaft fracture.
- delayed stabilization of all fractures after the open wound has healed.
Correct Answer: open reduction and internal fixation of the humeral shaft, medial condyle, and the both bones forearm fractures.
Explanation:
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
References:
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Question 7:
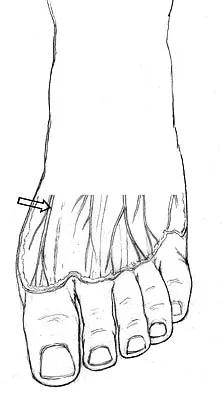
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
Options:
- Saphenous
- Medial branch of the superficial peroneal
- Deep peroneal
- Posterior tibial
- Sural
Correct Answer: Medial branch of the superficial peroneal
Explanation:
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
References:
Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea & Febiger, 2000, pp 963, 966.
Question 8:
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Options:
- deltoid.
- wrist flexor.
- wrist extensor.
- triceps.
- grip.
Correct Answer: wrist extensor.
Explanation:
A herniated cervical disk at C5-6 causes a C6 radiculopathy. There are eight cervical nerve roots and seven cervical vertebrae, and C8 exits between the C7 and T1 vertebrae. The C6 nerve root typically innervates the biceps and wrist extensor. The deltoid is predominantly innervated by C5. The wrist flexor and triceps are predominantly innervated by C7. Grip strength is predominantly a function of C8.
References:
Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 9:
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Options:
- Serum uric acid level studies and administration of indomethacin
- Administration of colchicine
- Administration of allopurinol
- Aspiration with evaluation of crystals, cell count, and culture
- Aspiration with evaluation of crystals and steroid injection
Correct Answer: Aspiration with evaluation of crystals, cell count, and culture
Explanation:
The patient's symptoms are typical for gouty arthropathy, and the diagnosis can only be confirmed with aspiration and visualization of the crystals. A concomitant infection also must be ruled out; therefore, it is important to obtain a cell count and culture. Colchicine may have a role in gouty management, but the diagnosis must be confirmed. Allopurinol is not effective in acute gouty arthropathy. Measurement of serum uric acid levels is often not helpful in making a definitive diagnosis. Steroid injections should be deferred until cell count and culture results indicate no accompanying infection. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
References:
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1712-1718.
Question 10:
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Options:
- Coracohumeral
- Superior glenohumeral
- Middle glenohumeral
- Anterior band of the inferior glenohumeral ligament complex
- Posterior band of the inferior glenohumeral ligament complex
Correct Answer: Anterior band of the inferior glenohumeral ligament complex
Explanation:
With the arm in the abducted, externally rotated position, the anterior band of the inferior glenohumeral ligament complex moves anteriorly, preventing anterior humeral head translation. Both the coracohumeral ligament and the superior glenohumeral ligament restrain the humeral head to inferior translation of the adducted arm, and to external rotation in the adducted position. The middle glenohumeral ligament is a primary stabilizer to anterior translation with the arm abducted to 45 degrees. The posterior band of the inferior glenohumeral ligament complex resists posterior translation of the humeral head when the arm is internally rotated. Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
References:
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 11:
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15 degrees of valgus, and forefoot supination can be corrected to 10 degrees from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Options:
- medial sliding calcaneal osteotomy with flexor digitorum longus (FDL) transfer.
- isolated subtalar arthrodesis.
- isolated talonavicular arthrodesis.
- triple arthrodesis.
- subtalar arthroereisis.
Correct Answer: triple arthrodesis.
Explanation:
The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7 degrees, an isolated subtalar fusion is a possible alternative.
References:
Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 12:
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?
Options:
- Closed reduction and application of a shoulder spica cast in the outpatient setting
- Closed reduction under fluoroscopy and application of a shoulder spica cast in the operating room
- No active reduction and placement of the upper extremity in a shoulder immobilizer
- Closed or open reduction and percutaneous pin stabilization
- Open reduction and internal fixation
Correct Answer: Closed or open reduction and percutaneous pin stabilization
Explanation:
The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient's age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement. Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
References:
Sarwark JF, King EC, Luhmann SJ: Proximal humerus, scapula, and clavicle, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 703-715.
Question 13:
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Options:
- Extensor digiti quinti
- Abductor pollicis longus
- Extensor pollicis longus
- Extensor carpi radialis brevis
- Extensor carpi ulnaris
Correct Answer: Extensor digiti quinti
Explanation:
The tendon most prone to rupture in a patient with rheumatoid arthritis of the wrist is the extensor digiti quinti. It can be a silent injury since the extensor digitorum communis can provide extension to the fifth finger. The extensor digiti quinti is at high risk since it is overlying the ulnar head where it is prone to attritional rupture (Vaughan-Jackson syndrome). Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
References:
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg 2006;14:65-77.
Question 14:
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Options:
- Reposition the harness to hold the hips in 70 degrees of abduction
- Closed reduction and arthrography under anesthesia
- Open reduction and a spica cast
- Continued harness treatment in the current position
- Spica cast
Correct Answer: Continued harness treatment in the current position
Explanation:
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
References:
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 15:
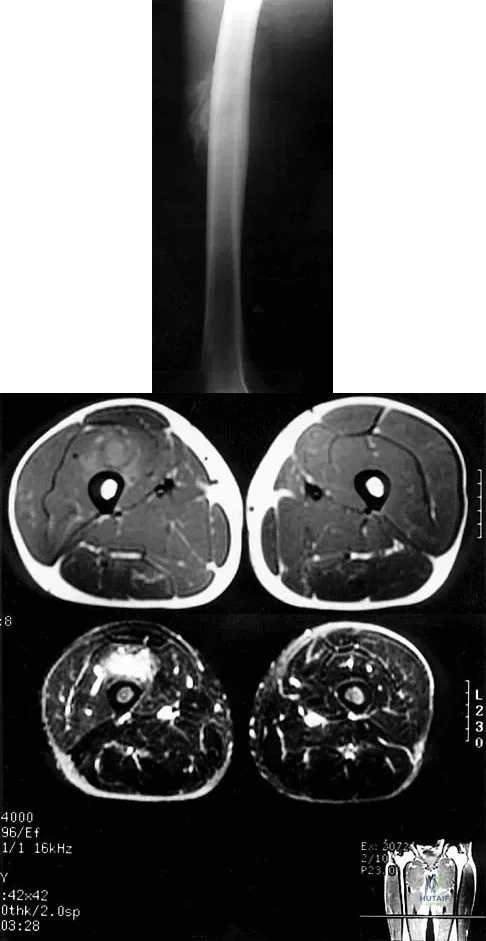
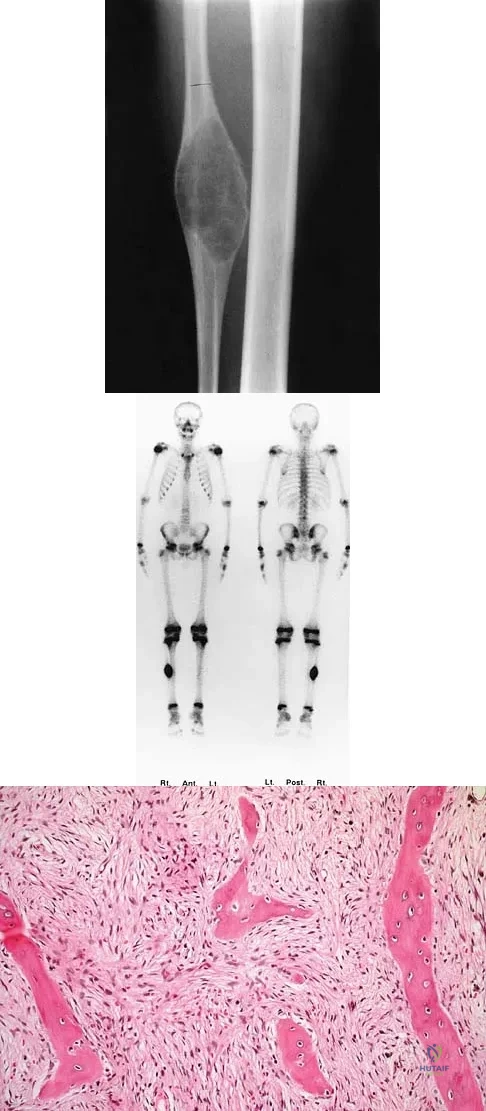
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of
Options:
- CT of the chest.
- a bone scan.
- a repeat radiograph in 6 to 8 weeks.
- repeat MRI in 6 to 8 weeks.
- an open biopsy.
Correct Answer: a repeat radiograph in 6 to 8 weeks.
Explanation:
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
References:
Wang SY, Lomasney LM, Demos TC, Hopkinson WJ: Radiologic case study: Traumatic myositis ossificans. Orthopedics 1999;22:991-995, 1000.
Question 16:
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Options:
- open reduction and plate fixation.
- a figure-of-8 bandage for 4 to 6 weeks.
- a sling for comfort, followed by physical therapy when pain-free.
- excision of the outer end of the clavicle.
- a tension band and Kirschner wires.
Correct Answer: a sling for comfort, followed by physical therapy when pain-free.
Explanation:
Displaced clavicular fractures lateral to the coracoid process (Neer type II and III) are best managed nonsurgically with sling immobilization and physical therapy, starting with pendulum exercises and progressing to active-assisted exercises when comfortable. Supervised therapy should be performed for 3 months or until full painless motion is achieved. In one study by Robinson and Cairns, this form of treatment provided patients with a 86% chance of avoiding a secondary reconstructive procedure. Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Scientific References
:
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 17:
Histologically, synovial chondromatosis is characterized by
Options:
- exuberant synovitis (Pannus).
- loose fragments of articular cartilage embedded in the synovium.
- ossified cartilage nodules embedded in the synovium.
- the presence of granulomas in the synovium.
- hemosiderin deposition in the synovium.
Correct Answer: ossified cartilage nodules embedded in the synovium.
Explanation:
Histologically, there is metaplastic cartilage arising from the synovium. These lobules of zonates hyaline cartilage are of variable size, are embedded within edematous synovium, and protrude into the joint. The lobules calcify and ossify, leading to the characteristic radiographic appearance. Inflammatory synovitis is not characteristic of synovial chondromatosis. The fluid is clear and serosanguin, not blood tinged. Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
References:
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 18:
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Options:
- Ankle
- Anterior knee
- Posterior knee
- Hip
- Elbow
Correct Answer: Anterior knee
Explanation:
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
References:
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 19:
Which of the following bearing materials is most resistant to scratching from third-body debris?
Options:
- Alumina
- Stainless steel
- Forged cobalt-chromium
- Ion bombarded and forged cobalt-chromium
- Oxidized titanium
Correct Answer: Alumina
Explanation:
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
References:
Cooper JR, Dowson D, Fisher J, Jobbins B: Ceramic bearing surfaces in total articular joints: Resistance to third body damage from bone cement particles. J Med Eng Technol 1991;15:63-67.
Question 20:
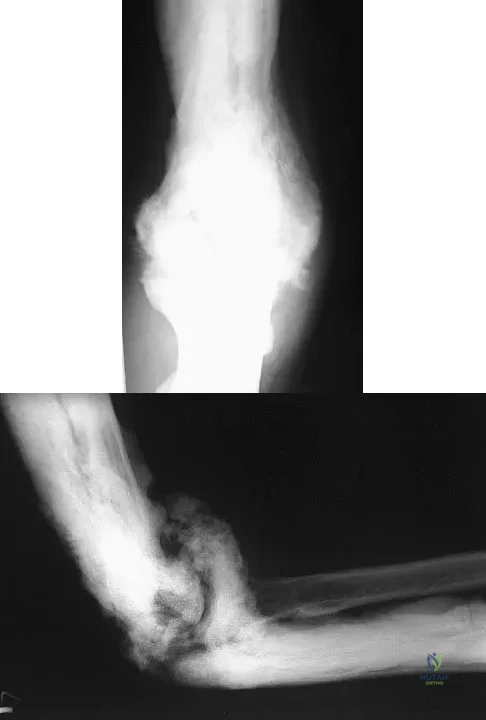
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
Options:
- Melorheostosis
- Ectopic bone formation
- Bone infarct
- Infection
- Juxacortical chondroma
Correct Answer: Melorheostosis
Explanation:
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
References:
Kawabata H, Tsuyuguchi Y, Kawai H, et al: Melorheostosis of the upper limb: A report of two cases. J Hand Surg Am 1984;9:871-876.
Question 21:
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Options:
- Cruciate paralysis
- Quadraplegia
- Normal function
- Absent bulbocavernosus reflex
- Greater occipital nerve dysesthesia
Correct Answer: Normal function
Explanation:
The radiographic findings are consistent with a type II Hangman's fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function. Levine AM: Traumatic spondylolisthesis of the axis (Hangman's fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
References:
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 22:
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Options:
- oral antibiotics and observation.
- IV antibiotics and observation.
- immediate arthroscopic debridement and lavage.
- blood cultures, oral antibiotics, and a reculture in 2 days.
- aspiration of the joint at his regular follow-up in 7 days if the symptoms increase.
Correct Answer: immediate arthroscopic debridement and lavage.
Explanation:
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
References:
Ward WG, Goldner RD: Shoulder pyarthrosis: A concomittant process. Orthopedics 1994;17:591-595.
Question 23:
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Options:
- triple arthrodesis.
- manipulation of the foot under general anesthesia.
- continued nonsurgical management until the synchondrosis ossifies.
- resection of the coalition and interposition with the extensor digitorum brevis.
- a medial closing wedge osteotomy of the calcaneus.
Correct Answer: resection of the coalition and interposition with the extensor digitorum brevis.
Explanation:
Surgical treatment is indicated for a symptomatic tarsal coalition that has failed to respond to nonsurgical management. In this patient, the radiographs reveal a calcaneonavicular coalition and no degenerative changes. The patient is symptomatic, and two attempts at use of a short leg walking cast have failed to provide relief. For calcaneonavicular coalitions, good results have been reported following resection and interposition of the extensor digitorum brevis. A retrospective study of this procedure achieved good to excellent results in 58 of 75 feet (77%). Degenerative arthritis or persistent pain following resection of a coalition is a reasonable indication for a triple arthodesis. A medial closing wedge osteotomy of the calcaneus may be indicated for a rigid flatfoot with severe valgus deformity. There are no studies documenting the long-term effectiveness of a manipulation under general anesthesia for this condition. Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
References:
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 24:
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Options:
- an orthosis and an immediate return to running.
- no running for 6 weeks and use of a bone stimulator at night.
- a University of California Biomechanics Laboratory (UCBL) orthosis and a gradual return to running.
- immobilization in a short leg cast with no weight bearing for 6 to 8 weeks.
- open reduction and internal fixation.
Correct Answer: immobilization in a short leg cast with no weight bearing for 6 to 8 weeks.
Explanation:
The patient has a nondisplaced stress fracture of the tarsal navicular. Weight bearing is associated with a high rate of nonunion; therefore, management should consist of immobilization and no weight bearing for 8 weeks. Delayed union or nonunion is treated by excision of sclerotic fracture margins and bone grafting, with or without internal fixation. Generally, CT should be repeated to document healing before permitting a return to sports. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
References:
Torg J, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-712.
Question 25:
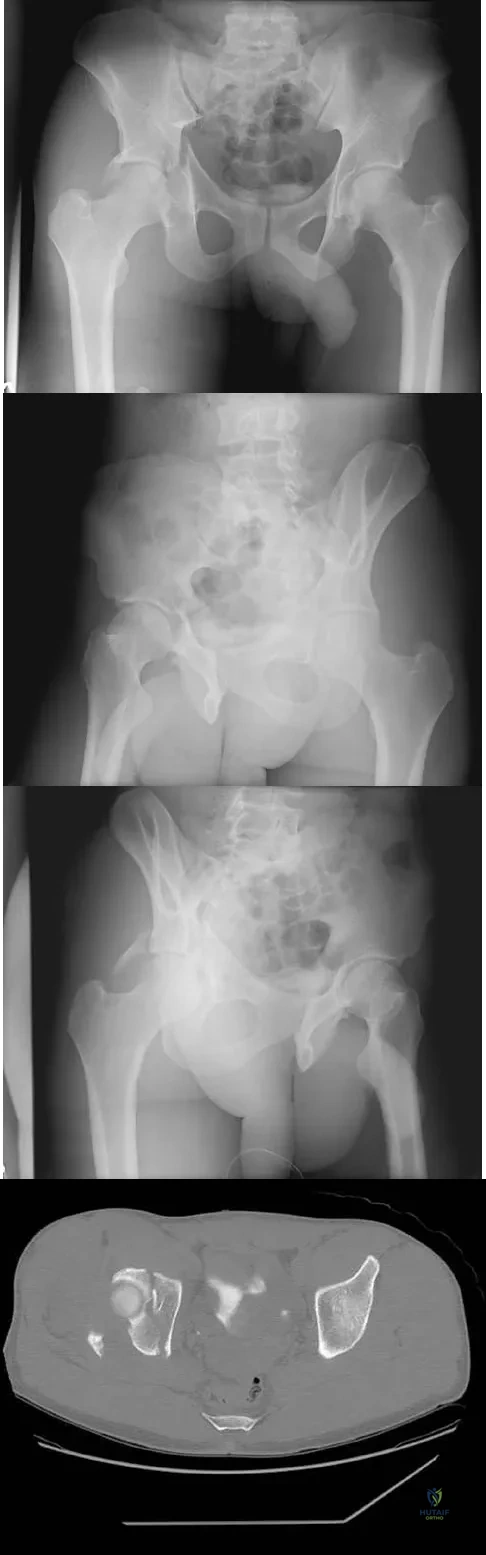
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Options:
- Transverse
- Transverse with posterior wall
- Both column
- Posterior wall anterior hemitransverse
- T-type
Correct Answer: Transverse with posterior wall
Explanation:
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
References:
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 26:
Examination of a 9-year-old girl who injured her left elbow in a fall reveals tenderness and swelling localized to the medial aspect of the elbow. Motor and sensory examinations of the hand are normal, and circulation is intact. A radiograph is seen in Figure 28. Management should consist of
Options:
- long arm cast immobilization.
- open reduction and internal fixation, followed by cast immobilization.
- closed reduction and percutaneous pin fixation.
- anterior transposition of the ulnar nerve.
- excision of the loose fragment and repair of the common flexor origin.
Correct Answer: long arm cast immobilization.
Explanation:
Avulsion fractures of the medial epicondyle are caused by a valgus stress applied to the immature elbow and usually occur in children between the ages of 9 and 14 years. Long-term studies have shown that isolated fractures of the medial epicondyle with between 5 to 15 mm of displacement heal well. Brief immobilization (1 to 2 weeks) in a long arm cast or splint yields results similar to open reduction and internal fixation. Fibrous union of the fragment is not associated with significant symptoms or diminished function. Surgical excision of the fragment yielded the worst results in one study and should be avoided. Open reduction is best reserved for those injuries in which the medial epicondylar fragment becomes entrapped in the elbow joint during reduction and cannot be extracted by closed manipulation. Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
References:
Josefsson PO, Danielsson LG: Epicondylar elbow fracture in children: 35-year follow-up of 56 unreduced cases. Acta Orthop Scand 1986;57:313-315.
Question 27:
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Options:
- Surgery on the wrong patient
- Surgery on the wrong side
- Incorrect procedure performed
- Intraoperative death
- Surgery on the wrong level
Correct Answer: Surgery on the wrong level
Explanation:
Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures. Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
References:
Wong DA: Spinal surgery and patient safety: A systems approach. J Am Acad Orthop Surg 2006;14:226-232.
Question 28:
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Options:
- Fifth metatarsal head lateral ostectomy
- Fifth metatarsal head excision
- Metatarsal osteotomy and fifth metatarsal head ostectomy
- Fifth metatarsal plantar condylectomy
- Fifth metatarsophalangeal Silastic implant arthroplasty
Correct Answer: Metatarsal osteotomy and fifth metatarsal head ostectomy
Explanation:
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
References:
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 29:
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Options:
- bone obtained through a knee arthrotomy with creation of a portal that will be used for retrograde femoral nailing.
- bone obtained by going through the mass.
- bone obtained through a posterior approach, dissecting out and protecting the sciatic nerve and popliteal artery.
- soft tissue obtained through a longitudinal incision centered over the mass.
- soft tissue obtained through a transverse incision on the medial thigh.
Correct Answer: soft tissue obtained through a longitudinal incision centered over the mass.
Explanation:
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
References:
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 30:
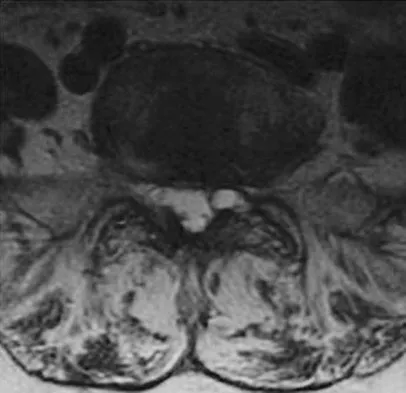
Examination of a 34-year-old man who has had left leg pain for the past 6 weeks reveals minimal weakness of the left extensor hallucis longus and normal ankle jerk and patellar reflexes. Figure 33 shows an axial MRI scan of the L4-5 disk. Based on these findings, the MRI scan results are consistent with compression of the
Options:
- traversing L4 nerve root and the patient's history and examination.
- traversing L4 nerve root but inconsistent with the patient's history and examination.
- traversing L5 nerve root and the patient's history and examination.
- traversing L5 nerve root but inconsistent with the patient's history and examination.
- exiting L5 nerve root and the patient's history and examination.
Correct Answer: traversing L5 nerve root and the patient's history and examination.
Explanation:
The patient has an L5 radiculopathy secondary to an L4-5 disk herniation that is compressing the traversing L5 nerve root.
References:
McCulloch JA, Young PH: Essentials of Spinal Microsurgery. Philadelphia, PA, Lippincott-Raven, 1998.
Question 31:
A 21-year-old collegiate scholarship football player has an episode of transient quadriplegia. An MRI scan of the cervical spine reveals cord edema and severe congenital spinal stenosis. The athlete has aspirations of playing on a professional level and demands that he be allowed to play. The team physician should give what recommendation to the college?
Options:
- Do not allow the athlete to return to football.
- Allow the athlete to participate.
- Allow the athlete to play only if he signs a waiver.
- Suggest that the college and athlete enter binding arbitration.
- Allow the athlete to play with special equipment.
Correct Answer: Do not allow the athlete to return to football.
Explanation:
Federal courts have ruled that a student-athlete does not have a constitutional right to participate in athletics against medical advice. As long as the student retains his scholarship, the college is under no legal or ethical obligation to allow the student to participate in sports. A waiver would not hold up in court and would not indemnify the college or the team physician against suit. No equipment has been shown to be effective in preventing transient quadriplegia. Mathias MB: The competing demands of sport and health: An essay on the history of ethics in sports medicine. Clin Sports Med 2004;23:195-214.
References:
Bernstein J, Perlis C, Bartolozzi AR: Ethics in sports medicine. Clin Orthop 2000;378:50-60.
Question 32:
Which of the following activities can improve posterior capsular contractures?
Options:
- Theraband exercises to strengthen the external rotator
- Latissimus pull-down exercises to the chest
- Seated rows
- Internal rotation stretch at 90 degrees abduction with scapular stabilization
- Bench press with wide grip
Correct Answer: Internal rotation stretch at 90 degrees abduction with scapular stabilization
Explanation:
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule. Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
References:
Kibler WB, McMullen J, Uhl J: Shoulder rehabilitation strategies, guidelines, and practice. Op Tech Sports Med 2000;8:258-267.
Question 33:
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Options:
- 5 mm
- 10 mm
- 15 mm
- 20 mm
- 25 mm
Correct Answer: 20 mm
Explanation:
Miller and associates reported the results of a cadaveric study of the vascular risk of a posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. The average distance from the screw to the popliteal artery was 21.1 mm (range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon's finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle. Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804. Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
References:
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 34:
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Options:
- Peroneus brevis
- Extensor digitorum longus
- Extensor hallucis
- Tibialis anterior
- Peroneus tertius
Correct Answer: Peroneus tertius
Explanation:
The appropriate placement of the anterolateral portal provides access to the lateral gutter of the joint while avoiding the superficial peroneal nerve. The safest location for the portal is approximately 4 mm lateral to the peroneus tertius tendon, the closest of the tendons listed to the anterolateral portal. Because the superficial peroneal nerve location is variable, attempts to visualize, palpate, or transilluminate the nerve are mandatory.
References:
Ogut T, Akgun I, Kesmezacar H, et al: Navigation for ankle arthroscopy: Anatomical study of the anterolateral portal with reference to the superficial peroneal nerve. Surg Radiol Anat 2004;26:268-274.
Question 35:
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Options:
- A 45-year-old woman with a hypermobile foot
- A 45-year-old man with a rigid hindfoot valgus deformity
- A thin 55-year-old woman with mild hemiparesis affecting the symptomatic foot from a previous stroke
- An active 55-year-old woman with a progressively worsening supple hindfoot valgus
- A moderately obese 70-year-old woman with a supple hindfoot
Correct Answer: An active 55-year-old woman with a progressively worsening supple hindfoot valgus
Explanation:
Transfer of the flexor digitorum longus tendon is a common technique combined with other procedures to treat patients with posterior tibial tendon insufficiency. However, it is contraindicated in patients with a fixed hindfoot deformity, hypermobility, or neuromuscular compromise. It is relatively contraindicated in patients who are obese, and those older than age 60 to 70 years. Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
References:
Mann RA: Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 167-296.
Question 36:
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Options:
- Surgical repair of the Bankart lesion
- Exploration of the axillary nerve
- MRI neurography
- Repeat EMG studies
- Continued observation and physical therapy
Correct Answer: Repeat EMG studies
Explanation:
Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months. Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36. Artico M, Salvati M, D'Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700. Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
References:
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 37:
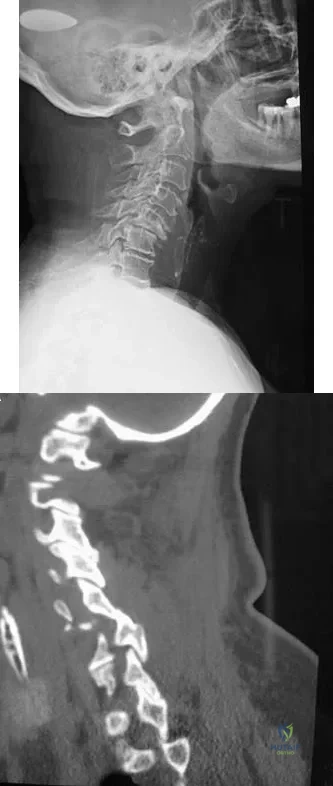
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Options:
- Degenerative spondylolisthesis
- Superior facet fracture
- Inferior facet fracture
- Perched unilateral facet dislocation
- Bilateral facet dislocation
Correct Answer: Perched unilateral facet dislocation
Explanation:
The radiograph shows a displacement of C5 on C6 of approximately 25%. The CT scan shows a perched facet at C5-6. There is no evidence of a facet fracture. A bilateral facet dislocation would show a displacement of more than 50%. Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
References:
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 38:
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Options:
- reconstruction of the sternoclavicular capsule.
- symptomatic nonsurgical treatment.
- medial clavicle excision.
- medial clavicle excision with capsular imbrication.
- medial clavicle excision and rhomboid ligament reconstruction.
Correct Answer: symptomatic nonsurgical treatment.
Explanation:
For the patient with an anterior sternoclavicular dislocation, the most appropriate initial treatment should be symptomatic. Surgical options are usually contraindicated because the incidence of intraoperative and postoperative complications is high. A deformity from an anterior sternoclavicular dislocation is usually well tolerated. Return to play is allowed when symptoms resolve. Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
References:
Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 39:
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Options:
- overgrowth of the distal radial epiphysis.
- premature closure of the distal radial physis.
- premature closure of the distal ulnar physis.
- a Salter-Harris type I fracture of the distal radius with a volar slip of the epiphysis.
- a Salter-Harris type I fracture of the distal radius with a dorsal slip of the epiphysis.
Correct Answer: premature closure of the distal radial physis.
Explanation:
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
References:
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
Question 40:
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?
Options:
- Closed reduction and casting for 4 weeks
- Closed reduction and bracing with immediate range of motion
- Open reduction, lateral collateral ligament repair, and open reduction and internal fixation or metallic replacement of the radial head
- Open reduction, radial head silastic arthroplasty, and lateral collateral ligament repair
- Open reduction, lateral collateral ligament repair, and radial head excision
Correct Answer: Open reduction, lateral collateral ligament repair, and open reduction and internal fixation or metallic replacement of the radial head
Explanation:
The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated. Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
References:
O'Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 41:
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Options:
- cheilectomy.
- extra-depth shoes.
- steroid injection.
- arthrodesis.
- joint replacement arthroplasty.
Correct Answer: extra-depth shoes.
Explanation:
Some patients have minimal symptoms associated with hallux rigidus despite significant radiographic evidence of osteoarthritis. This patient's symptoms are primarily related to shoe pressure from the exostosis and can be managed with extra-depth shoe wear. Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
References:
Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 42:
Using methylmethacrylate to fill a biopsy hole in the diaphysis of a femur theoretically achieves what purpose?
Options:
- Local tumor control by chemical cytotoxic effect
- Local tumor kill from heat generation
- Minimizes tumor contamination
- Decreases rate of wound infection
- Reinforces the bone to prevent fracture
Correct Answer: Minimizes tumor contamination
Explanation:
Placing cement over a bone biopsy site prevents tumor contamination by controlling hematoma. Even though the use of cement may impart some strength, the femur is still at significant risk for fracture. The use of bone cement in this manner has not been cleared by the FDA, but many physicians feel that it is appropriate when the patient's health status has been given careful consideration, and the physician has the necessary knowledge and training. The other options are not important reasons to use methylmethacrylate in biopsies. Simon MA, Springfield DS, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 55-65.
References:
Simon MA: Biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1982;64:1253-1257.
Question 43:
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Options:
- elbow flexion.
- shoulder flexion.
- shoulder internal rotation.
- shoulder abduction.
- forearm pronation.
Correct Answer: elbow flexion.
Explanation:
The musculocutaneous nerve travels through the conjoined tendon approximately 8 cm distal to the tip of the acromion. The musculocutaneous nerve innervates the biceps muscle and the bracialis muscle, both of which are responsible for elbow flexion. Shoulder flexion is facilitated by the anterior fibers of the deltoid muscle (axillary nerve) and the supraspinatus muscle (suprascapular nerve). The subscapular muscle facilitates internal rotation of the shoulder (upper and lower subscapularis nerve). Shoulder abduction is performed by the deltoid muscle (axillary nerve), and forearm pronation is facilitated by the pronator teres (median nerve). Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
References:
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 2-49.
Question 44:
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Options:
- Inflation of the abdominal portion of the PASG
- Application of a pelvic clamp
- Application of a pelvic external fixator
- Rapid infusion of 4 more units of blood
- Angiography and embolization
Correct Answer: Angiography and embolization
Explanation:
There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated. Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856. Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
References:
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 45:
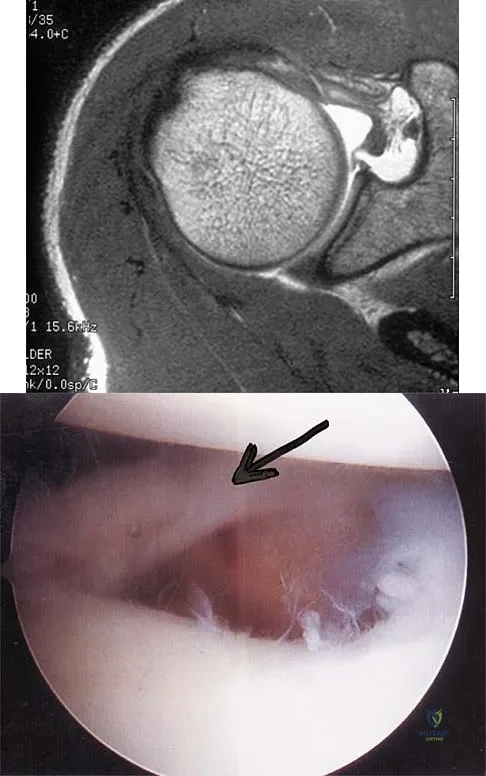
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Options:
- Normal anatomic variant (Buford complex)
- Glenoid labral tear (superior labrum anterior and posterior)
- Bankart lesion
- Avulsion of the biceps tendon
- Subscapularis tendinitis
Correct Answer: Normal anatomic variant (Buford complex)
Explanation:
The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Scientific References
:
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 46:
Chronic anterior donor site pain following the harvest of autologous iliac crest bone graft for use during anterior cervical diskectomy and fusion is reported by approximately what percent of patients?
Options:
- Less than 1%
- 5%
- 25%
- 50%
- 75%
Correct Answer: 25%
Explanation:
Four years after surgery, more than 90% of patients are satisfied with the cosmetic appearance of the iliac donor site scar. Approximately 25% still have pain and/or functional difficulty, including 12.7% who still report difficulty with ambulation, 11.9% difficulty with recreational activities, 7.5% with sexual intercourse, and 11.2% require pain medication for iliac donor site symptoms. Silber JS, Anderson DG, Daffner SD, et al: Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine 2003;28:134-139.
References:
Cockin J: Autologous bone-grafting complications at the donor site. J Bone Joint Surg Br 1971;49:153.
Question 47:
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Options:
- Tachycardia, hypertension, intact bulbocavernosus reflex
- Tachycardia, hypotension, intact bulbocavernosus reflex
- Tachycardia, hypotension, absent bulbocavernosus reflex
- Bradycardia, hypotension, absent bulbocavernosus reflex
- Bradycardia, hyperthermia, intact bulbocavernosus reflex
Correct Answer: Bradycardia, hypotension, absent bulbocavernosus reflex
Explanation:
The term 'spinal shock' applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
References:
Ditunno JF, Little JW, Tessler A, et al: Spinal shock revisited: A four-phase model. Spinal Cord 2004;42:383-395.
Question 48:
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of
Options:
- Z-plasty.
- a posterior interosseous fasciocutaneous flap.
- a reverse cross-finger flap from the index finger.
- excision of the contracture with placement of a full-thickness skin graft.
- excision of the contracture with placement of a split-thickness skin graft.
Correct Answer: a posterior interosseous fasciocutaneous flap.
Explanation:
The contracture is too large for a Z-plasty, which allows a 75% increase in length. Excision of the scar with placement of a skin graft is prone to contracture. A posterior interosseous fasciocutaneous flap will provide enough well-vascularized tissue and is well suited to reach the first dorsal web space. Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
References:
Brunelli F, Valenti P, Dumontier C, et al: The posterior interosseous reverse flap: Experience with 113 flaps. Ann Plast Surg 2001;47:25-30.
Question 49:
A 65-year-old man has a painful and often audible crepitus after undergoing a total knee arthroplasty 8 months ago. His symptoms are reproduced with active extension of about 30 degrees. Examination reveals no effusion or localized tenderness, a stable knee, and a range of motion of 5 degrees to 120 degrees. Radiographs are shown in Figures 37a and 37b. Management should consist of
Options:
- revision of all components to ensure patellar tracking.
- athroscopic debridement.
- arthrotomy and keloid excision.
- intra-articular corticosteroid injections.
- patellar component revision.
Correct Answer: athroscopic debridement.
Explanation:
This is a typical presentation of the patellar clunk syndrome. The syndrome usually follows implantation of a posterior stabilized prosthesis. It is thought to be the result of femoral component design and altered extensor mechanics. The condition usually resolves with arthroscopic debridement of the suprapatellar fibrous nodule. Arthrotomy or revision is seldom warranted. Beight JL, Yao B, Hozack WJ, Hearn SL, Booth RE Jr: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.
References:
Lintner DM, Bocell JR, Tullos HS: Arthroscopic treatment of intra-articular fibrous bands after total knee arthroplasty: A follow-up note. Clin Orthop 1994;309:230-233.
Question 50:
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Options:
- slow rewarming in cool 77 degrees F (25 degrees C) water.
- rapid rewarming in a footbath at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C).
- rewarming in 98.6 degrees F (37 degrees C) water.
- heated blankets at 100.4 degrees F (38 degrees C).
- a heating pad at 104.0 degrees F (40 degrees C).
Correct Answer: rapid rewarming in a footbath at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C).
Explanation:
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
References:
Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 51:
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Options:
- Long thoracic nerve
- Spinal accessory nerve
- Thoracodorsal nerve
- Lower trunk of the brachial plexus
- Posterior cord of the brachial plexus
Correct Answer: Long thoracic nerve
Explanation:
The long thoracic nerve, which innervates the serratus anterior, is prone to injury because of its superficial location along the chest wall. The long thoracic nerve is derived from the roots of C5, C6, and C7. The spinal accessory nerve innervates the trapezius, and the thoracodorsal nerve innervates the latissimus dorsi. The posterior cord of the brachial plexus provides the axillary and the radial nerves. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
References:
Marmor L, Bechtal CO: Paralysis of the serratus anterior due to electric shock relieved by transplantation of the pectoralis major muscle: A case report. J Bone Joint Surg Am 1983;45:156-160.
Question 52:
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Options:
- progressive increase in lumbar lordosis.
- load transfer to the superior adjacent vertebra.
- normalization of load transfer with working kyphosis.
- reduced strain at the occipito-cervical junction.
- reduced strain at the apex of the deformity.
Correct Answer: load transfer to the superior adjacent vertebra.
Explanation:
Kayanja and associates, in a number of biomechanical studies, showed that in a kyphotic spine the strain is located at the apex of the deformity, the force is transmitted to the superior adjacent vertebrae, and that realignment and cement augmentation effectively normalize the load transfer. Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87. Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63. Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
References:
Kayanja M, Evans K, Milks R, et al: The mechanics of polymethylmethacrylate augmentation. Clin Orthop Relat Res 2006;443:124-130.
Question 53:
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?
Options:
- Patient's age
- Patient's gender
- Number of prior surgical procedures
- Detachment of the deltoid
- Duration of the rotator cuff tear
Correct Answer: Detachment of the deltoid
Explanation:
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely. Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855. Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
References:
Neviaser RJ, Neviaser TJ: Operation for failed rotator cuff repair: Analysis of fifty cases. J Shoulder Elbow Surg 1992;1:283-286.
Question 54:
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?
Options:
- Osteoarthritis
- Rheumatoid arthritis
- Synovial chondromatosis
- Gout
- Osteonecrosis
Correct Answer: Osteonecrosis
Explanation:
The MRI scan shows near complete involvement of the femoral head with bone marrow changes and some collapse of the necrotic segment. This is most suggestive of osteonecrosis.
References:
Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997.
Question 55:
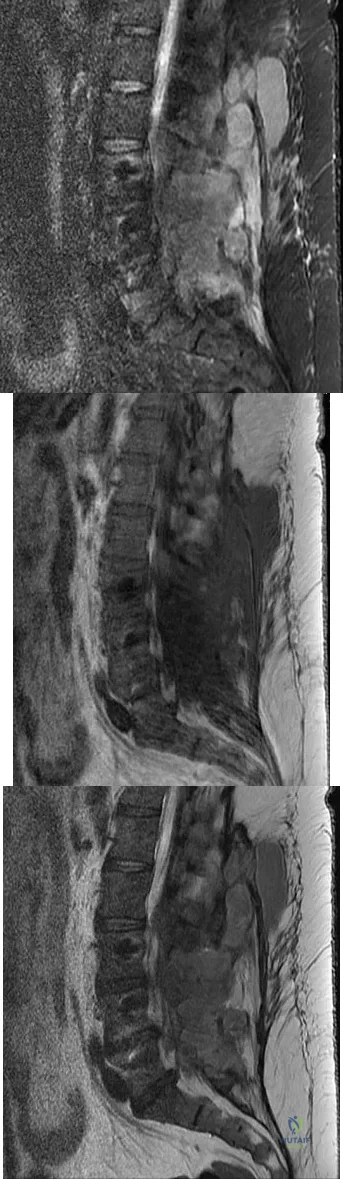
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?
Options:
- Physical therapy for functional rehabilitation
- CT/myelography of the spinal axis
- MRI with gadolinium
- Psychiatric consultation for possible malingering
- Lumbar puncture for analysis of cerebrospinal fluid
Correct Answer: MRI with gadolinium
Explanation:
The patient has had a clear and sudden onset of a profound neurologic deficit. The radiographic studies suggest a lesion in the conus medullaris that appears to be intradural and intramedullary. MRI, with and without contrast, will best evaluate this mass further. The addition of gadolinium allows further evaluation of vascularity and the extent of the lesion. Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
References:
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 81-87.
Question 56:
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Options:
- Infection
- Heterotopic ossification
- Dislocation
- Periprosthetic fracture
- Acetabular component loosening
Correct Answer: Acetabular component loosening
Explanation:
Acetabular component loosening has been reported as the most common mode of failure following total hip arthroplasty in patients with a previous acetabular fracture. Following acetabular fracture and subsequent open reduction and internal fixation, the bone quality and vascularity are compromised, thus reducing the success rate of acetabular component cementless fixation. Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
References:
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 57:
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Options:
- Pectoralis major tendon rupture
- Supraspinatus rupture
- Subscapularis rupture
- Bankart tear
- Humeral avulsion of the inferior glenohumeral ligament
Correct Answer: Subscapularis rupture
Explanation:
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
References:
Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 58:
What is the primary limiting membrane and mechanical support for the periphery of the physis?
Options:
- Perichondrial ring of La Croix
- Groove of Ranvier
- Zone of provisional calcification
- Last intact transverse septum
- Primary spongiosa
Correct Answer: Perichondrial ring of La Croix
Explanation:
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
References:
Asher MA (ed): Orthopaedic Knowledge Update 1. Chicago, IL, American Academy of Orthopaedic Surgeons, 1984, pp 15-28.
Question 59:
A 17-year-old man sustained a 5-mm laceration on the lateral aspect of the hindfoot while working on a farm. Examination in the emergency department revealed no fractures. Twenty-four hours later, he returns to the emergency department with increasing foot pain. Thin brown drainage is seen emanating from the wound. He has a temperature of 102.0 degrees F (38.9 degrees C), a pulse rate of 120, and a blood pressure of 80/40 mm Hg. Examination of the foot reveals diffuse swelling, ecchymosis, tenderness, and crepitus with palpation. Current radiographs are shown in Figures 40a and 40b. Management should now consist of
Options:
- intravenous antibiotics.
- hyperbaric oxygen therapy and intravenous antibiotics.
- surgical debridement, primary wound closure, and intravenous antibiotics.
- surgical debridement, closure of the wound over drains, and intravenous antibiotics.
- surgical debridement, leaving the wound open, and intravenous antibiotics.
Correct Answer: surgical debridement, leaving the wound open, and intravenous antibiotics.
Explanation:
The mechanism and environment in which the injury occurred, the clinical picture, and the radiographic findings of gas in the tissues suggest an anaerobic Gram-positive bacterial infection. This can be a life- and limb-threatening infection. Treatment should consist of wide debridement of all devitalized tissue, and intravenous antibiotics should be started. Wounds should be left open to allow bacterial effluent and increase oxygen tension in the wound. Hyperbaric oxygen may be used as an adjuvant but is no substitute for debridement. Pellegrini VD, Reid JS, Evarts CM: Complications, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 1, pp 458-463.
References:
Ayers DC, Murray DC: Complications of the treatment of fractures and dislocations: General considerations, in Epps Jr CH (ed): Complications in Orthopedic Surgery, ed 4. Philadelphia, PA, JB Lippincott, 1994, pp 3-48.
Question 60:
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Options:
- Disk degeneration
- Limbus fracture
- Degenerative retrolisthesis of L4-5
- Spondylolysis
- Osteoid osteoma
Correct Answer: Spondylolysis
Explanation:
The patient has a pars interarticularis defect of L5 without apparent listhesis. The other diagnoses are not present. Papanicolaou N, Wilkinson RH, Emmans JB, Treves S, Micheli LJ: Bone scintigraphy and radiography in young athletes with low back pain. Am J Roentgenol 1985;145:1039-1044.
References:
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 291-302.
Question 61:
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Options:
- cast immobilization.
- delayed fixation of the medial malleolus.
- immediate fixation of the medial malleolus and plating of the fibula.
- immediate fixation of the medial malleolus, plating of the fibula, and placement of a syndesmotic screw.
- immediate fixation of the medial malleolus and placement of a syndesmotic screw.
Correct Answer: immediate fixation of the medial malleolus, plating of the fibula, and placement of a syndesmotic screw.
Explanation:
The examination and radiographs reveal a closed fracture-dislocation of the ankle with tibiofibular diastasis. Immediate fixation of the medial malleolus and plating of the fibula are indicated. If residual tibiofibular diastasis occurs with lateral translation of the fibula after plating, a syndesmotic screw is placed to stabilize the syndesmosis. Ankle fracture-dislocations associated with a proximal fibular fracture (Maisonneuve fracture) require syndesmotic fixation, but the fibula is not plated. Unstable ankle fractures require surgical treatment. If swelling is severe (fracture blisters, loss of skin wrinkling), a compressive splint is applied and surgery is delayed for 5 to 7 days. Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
References:
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 62:
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Options:
- High volume diuresis with alkalinization of the urine
- Systemic heparinization of the patient for 72 hours
- Elevation of the extremity, with maintanence of the patient's room temperature at 80 degrees F (26.6 degrees C)
- Satellite ganglion continuous sympathetic block
- Daily IV administration of low-molecular-weight dextran
Correct Answer: High volume diuresis with alkalinization of the urine
Explanation:
After major limb replantation, the occurrence of ischemic rhabdomyonecrosis can result in lactic acidosis and myoglobulinemia. These complications can be limited by rapid repair of the arterial supply, potentially using a shunt before skeletal stability. Repair of the venous system should be performed after repair of the artery. High volume fluid replacement will maintain a diuresis, thus limiting the complications from myoglobulinemia. Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
References:
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
Question 63:
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Options:
- Moist dressings and continued observation
- Debridement of the necrotic tissue
- Amputation at the metatarsophalangeal level with open wound management
- Closed forefoot amputation
- Guillotine transtibial amputation
Correct Answer: Moist dressings and continued observation
Explanation:
The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement. McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective. Am J Orthop 1999;28:21-26.
References:
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 64:
What is the main function of collagen found within articular cartilage?
Options:
- Compressive properties
- Tensile properties
- Proteoglycan synthesis
- Cartilage metabolism
- Joint lubrication
Correct Answer: Tensile properties
Explanation:
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
References:
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 65:
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Options:
- Less elastic and less permeable
- Less elastic and more permeable
- Of the same elasticity and permeability
- More elastic and more permeable
- More elastic and less permeable
Correct Answer: More elastic and less permeable
Explanation:
The meniscal cartilage, like articular cartilage, possesses viscoelastic properties. The extracellular matrix is a biphasic structure composed of a solid phase (collagen, proteoglycan) that acts as a fiber-reinforced porous-permeable composite, and a fluid phase that may be forced through the solid matrix by a hydraulic pressure gradient. Although these properties are shared with articular cartilage, the meniscus is more elastic and less permeable than articular cartilage. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
References:
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, AAOS, 1999, pp 349-354.
Question 66:
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?
Options:
- Dislocation of the great toe MTP joint
- Rupture of the volar plate
- Fracture of the lateral sesamoid
- Fracture of the lateral sesamoid and rupture of the plantar plate
- Subluxation of the sesamoids
Correct Answer: Fracture of the lateral sesamoid and rupture of the plantar plate
Explanation:
Turf toe occurs in collision and contact sports in which the athlete pushes off to accelerate or change direction and there is hyperextension of the great toe MTP joint. Typically, there is also axial loading of the posterior hindfoot, which increases the hyperextension of the MTP joint. The most common presentation is pain and swelling of the MTP joint and inability to hyperextend the joint without significant symptoms. With significant force, fractures of the sesmoids and plantar soft tissues can occur. The radiographs do not show a dislocation of the great toe MTP joint because it is concentrically located on both radiographs. However, the radiographs show a fracture of the lateral sesamoid or a diastasis of a bipartite lateral sesamoid. The medial sesamoid is also proximal indicating a rupture of the plantar (volar) plate. Therefore, the most likely diagnosis is a fracture of the lateral sesamoid with rupture of the plantar plate leading to proximal migration of the proximal fragment of the lateral sesamoid and the medial sesamoid. Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
References:
Rodeo SA, O'Brien S, Warren RF, et al: Turf toe: An analysis of metatarsal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 67:
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the
Options:
- spinal accessory nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
- spinal accessory nerve, causing shoulder elevation with the scapula translated medially and the inferior angle rotated medially.
- long thoracic nerve, causing shoulder elevation with the scapula translated medially and the inferior angle rotated medially.
- long thoracic nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
- thoracodorsal nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
Correct Answer: spinal accessory nerve, causing shoulder depression with the scapula translated laterally and the inferior angle rotated laterally.
Explanation:
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
References:
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;108:15-18.
Question 68:
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Options:
- external fixation.
- plate fixation.
- skeletal traction for 5 weeks.
- immediate spica cast immobilization.
- flexible nailing with titanium nails.
Correct Answer: immediate spica cast immobilization.
Explanation:
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365. Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
References:
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
Question 69:
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of
Options:
- a three-phase bone scan.
- CT.
- MRI.
- a repeat examination in 6 weeks.
- a biopsy.
Correct Answer: a repeat examination in 6 weeks.
Explanation:
The plain radiographs reveal a pedunculated osteochondroma with a fracture. There is a bony growth in the metaphysis of a long bone, on a stalk that is directed away from the nearby epiphysis. On the AP view, the host cortical and medullary bone are shown as "blending" with lesional bone. There is also a fracture through the lesion. Based on these radiographic findings, the diagnosis is an osteochondroma; therefore, initial management of an acute fracture of an osteochondroma is symptomatic treatment alone. Additional imaging studies are not indicated in this patient. At times it may be difficult to distinguish a sessile osteochondroma from a parosteal osteosarcoma. In the latter case, the host medullary bone and lesion bone are not confluent. A CT scan may be helpful to distinguish if the host medullary and cortical bone are confluent with the lesion.
References:
Davids JR, Glancy GL, Eilert RE: Fracture through the stalk of pedunculated osteochondromas: A report of three cases. Clin Orthop 1991;271:258-264.
Question 70:
What is the most common pediatric soft-tissue sarcoma?
Options:
- Ewing's sarcoma
- Liposarcoma
- Rhabdomyosarcoma
- Malignant fibrous histiocytoma
- Fibrosarcoma
Correct Answer: Rhabdomyosarcoma
Explanation:
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
References:
Wexler LH, Helman LJ: Pediatric soft tissue sarcomas. CA Cancer J Clin 1994;44:211-247.
Question 71:
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Options:
- Lumbar laminectomy with synovial cyst excision
- Repeat epidural steroid injection
- Microdiskectomy at L4-5
- Nonsteroidal medication and outpatient physical therapy
- Left-sided facet blocks at L4-5 and L5-S1
Correct Answer: Lumbar laminectomy with synovial cyst excision
Explanation:
Lumbar spinal stenosis with lumbar radiculopathy can be commonly caused by a synovial cyst arising from the facet joints. Lyons and associates reported on the surgical treatment of synovial cysts in 194 patients. Of the 147 with follow-up data, 91% reported good pain relief and 82% had improvement of their motor deficits. Epstein reported a 58% to 63% incidence of good/excellent results and a 38 to 42 point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis. Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg 2000;93:53-57. Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Scientific References
:
Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Question 72:
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Options:
- Reamed intramedullary nailing
- Traction
- External fixation
- Open plating
- Mast suit
Correct Answer: External fixation
Explanation:
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome. Shafi S, Elliot AC, Gentilello L: Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma 2005;59:1081-1085. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
References:
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-454.
Question 73:
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Options:
- Abundance of basic calcium phosphate crystals
- Abundance of calcium pyrophosphate crystals
- Gout
- Rheumatoid arthritis
- Osteonecrosis
Correct Answer: Abundance of basic calcium phosphate crystals
Explanation:
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
References:
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 74:
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of
Options:
- additional physical therapy and home stretching exercises.
- closed reduction and immobilization in a spica cast.
- open reduction and transfer of the subscapularis and lesser tuberosity.
- humeral arthroplasty.
- total shoulder arthroplasty.
Correct Answer: humeral arthroplasty.
Explanation:
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
References:
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
Question 75:
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
Options:
- Conversion to cast immobilization for 6 weeks
- Application of an articulated external fixator
- Begin early motion as soon as pain resolves
- Open reduction
- MRI to assess ligament integrity
Correct Answer: Open reduction
Explanation:
Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment. Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
References:
Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.
Question 76:
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T1-weighted, STIR, and T1-weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Options:
- Peripheral nerve sheath tumor
- Malignant peripheral nerve sheath tumor
- Malignant fibrous histiocytoma
- Liposarcoma
- Synovial sarcoma
Correct Answer: Malignant peripheral nerve sheath tumor
Explanation:
The images reveal a large mass in the posterior thigh arising from the sciatic nerve. The lesion is edematous, and the gadolinium image reveals rim enhancement, suggesting necrosis, given that the STIR image is not uniformly bright as would be seen in a cystic lesion. The PET scan has increased uptake, in this case a standard unit value (SUV) of greater than 2.0. These findings are all very suggestive of a malignant process. The history of neurofibromatosis makes a malignant peripheral nerve sheath tumor, or neurofibrosarcoma, the most likely diagnosis. The term "peripheral nerve sheath tumor" has replaced neurolemmoma and schwannoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
References:
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 77:
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Options:
- Extensor carpi radialis brevis, extensor carpi radialis longus, extensor digitorum comminus, extensor indicis proprious
- Extensor carpi radialis brevis, extensor carpi radialis longus, extensor indicis proprious, extensor digitorum comminus
- Extensor carpi radialis longus, extensor carpi radialis brevis, extensor indicis proprious, extensor digitorum comminus
- Extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum comminus, extensor indicis proprious
- Extensor carpi radialis longus, extensor digitorum comminus, extensor carpi radialis brevis, extensor indicis proprious
Correct Answer: Extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum comminus, extensor indicis proprious
Explanation:
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
References:
Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 78:
Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
Options:
- Vocal cord paralysis is three times as likely with a right-sided approach as compared to a left-sided approach.
- Vocal cord paralysis is twice as likely with a right-sided approach as compared to a left-sided approach.
- Vocal cord paralysis is equally likely with either a right-sided or a left-sided approach.
- Vocal cord paralysis is three times as likely with a left-sided approach as compared to a right-sided approach.
- Vocal cord paralysis is twice as likely with a left-sided approach as compared to a right-sided approach.
Correct Answer: Vocal cord paralysis is equally likely with either a right-sided or a left-sided approach.
Explanation:
It has been traditionally taught that a left-sided approach to the anterior cervical spine is associated with a lower incidence of injury compared to the right-sided approach. This is due in part to the anatomic differences in the path the recurrent laryngeal nerve (RLN) takes on the right as compared to the left. Both nerves ascend in the tracheoesophageal groove after branching off the vagus nerve in the upper thorax. The left-sided RLN loops around the aortic arch and stays relatively medial as compared to the right-sided RLN which loops around the right subclavian artery and is somewhat more lateral at this point, and therefore is theoretically more vulnerable as it ascends toward the larynx before becoming protected in the tracheoesophageal groove. Furthermore, the variant of a nonrecurrent inferior laryngeal nerve branching directly off the vagus nerve at the level of the midcervical spine is much more common on the right than the left. Despite this reasoning, there has been no clinical evidence to suggest that laterality of approach for anterior cervical surgery makes any difference in the incidence of vocal cord paralysis. Furthermore, two recent studies have shown that the incidence of RLN injury and vocal cord paralysis is equal with either side of approach. Beutler WJ, Sweeney CA, Connolly PJ: Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 2001;26:1337-1342.
References:
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 79:
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Options:
- No pharmacologic intervention is recommended at this time
- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours
- Administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 48 hours
- Administration of naloxone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours
- Administration of naloxone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 48 hours
Correct Answer: No pharmacologic intervention is recommended at this time
Explanation:
The standard practice in the pharmacologic treatment of a spinal cord injury in the United States has been the administration of methylprednisolone with an initial bolus of 30 mg/kg followed by 5.4 mg/kg for 24 hours, in accordance with the findings of the second and third National Acute Spinal Cord Injury Studies (NASCIS). Although the studies have subsequently drawn criticism for their methodology and outcomes, it has been generally accepted that beneficial neurologic outcomes were anticipated in patients who were able to start the protocol within 8 hours of their initial injury. Further improvement was noted in patients receiving the methylprednisolone within 3 hours of their injury and continuing an infusion for 48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time. Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
References:
Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.
Question 80:
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
Options:
- closed reduction and a long arm cast.
- closed reduction, percutaneous pin fixation, and a long arm cast.
- closed reduction and an external fixator.
- open reduction and internal fixation and soft-tissue repair.
- proximal row carpectomy.
Correct Answer: open reduction and internal fixation and soft-tissue repair.
Explanation:
Open reduction and internal fixation is the treatment of choice for accurate reduction of the disrupted intercarpal ligaments. In addition, the displaced scaphoid fracture will require open reduction and internal fixation and possible bone grafting. Closed reduction and long arm casting will not allow accurate reduction of the dislocated intracarpal intervals, and it is unlikely to allow accurate reduction of the scaphoid. The maneuver required to effect closed reduction of a displaced scaphoid fracture will most likely cause the scaphoid lunate interval to displace. Closed reduction with percutaneous pin fixation or with an external fixator is unable to effect anatomic reduction of the injury. Proximal row carpectomy is used as a salvage procedure for a variety of degenerative and posttraumatic problems of the wrist. Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120. Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
References:
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
Question 81:
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Options:
- Radiographs, including anterior, lateral, and oblique views
- MRI of the lumbar spine and follow-up at the clinic in 1 week
- Caudal epidural steroid injection
- Reassurance, limited analgesics, and early range of motion as tolerated
- Immediate MRI of the lumbar spine and possible urgent surgical decompression
Correct Answer: Reassurance, limited analgesics, and early range of motion as tolerated
Explanation:
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
References:
Wong DA, Transfeldt E: Macnab's Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 82:
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Options:
- A long leg cast in 90 degrees of knee flexion for 6 weeks
- Open reduction and internal fixation with a transphyseal 6.5-mm screw and washer
- Arthroscopic anterior cruciate ligament reconstruction with hamstring tendons
- Arthroscopic debridement and staged anterior cruciate ligament reconstruction when skeletally mature
- Open reduction and internal fixation with suture or intra-epiphyseal screw placement
Correct Answer: Open reduction and internal fixation with suture or intra-epiphyseal screw placement
Explanation:
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 83:
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?
Options:
- Pedicled vascularized bone graft
- Long arm thumb spica cast
- Percutaneous screw fixation
- Corticocancellous bone grafting via a volar approach (Matti-Russe)
- Open reduction and differential pitch screw placement via a dorsal approach
Correct Answer: Open reduction and differential pitch screw placement via a dorsal approach
Explanation:
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
References:
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 84:
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Options:
- distal Chevron osteotomy.
- proximal metatarsal osteotomy with soft-tissue release.
- shoe wear modifications.
- dorsal cheilectomy with Moberg osteotomy.
- hallux metatarsophalangeal joint arthroplasty.
Correct Answer: shoe wear modifications.
Explanation:
Surgery is not indicated in a patient who has a mild deformity and no pain. Shoe wear modifications should be recommended.
References:
Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 85:
A 53-year-old man reports a 5-week history of worsening low back pain accompanied by bilateral knee and ankle pain and swelling. He also reports a lesser degree of neck and left elbow pain. He denies any history of trauma or provocative episodes. His medical history is significant for Reiter's syndrome more than 25 years ago, with no subsequent exacerbations. Furthermore, he has recently returned from a vacation in Costa Rica and noted the development of infectious gastroenteritis with diarrhea within 1 week of his return. This was treated with a 10-day course of oral antibiotics and has since resolved. He denies any significant bowel or urinary symptoms at this time. His neurologic examination is essentially within normal limits, but is somewhat limited by his low back and leg pain. What further investigation is most appropriate at this time?
Options:
- Radiographs of the lumbar spine and bilateral knees and ankles
- MRI of the lumbar spine with and without gadolinium contrast
- Synovial fluid analysis of the involved joints for crystals and bacteria
- Laboratory tests including a CBC count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)
- Laboratory tests including CBC count, rheumatoid factor (RF), antinuclear antibodies (ANA), and human leukocyte antigen-B27 (HLA-B27)
Correct Answer: Laboratory tests including a CBC count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)
Explanation:
The patient has pain involving the cervical and lumbar spine as well as pain and swelling in both the knees and ankles. As such, this can be classified as polyarticular arthritis. The presence of multiple joint symptoms in the lower extremities, the absence of a history of trauma, and the multiple joints involved direct attention away from the spine as the etiology of this patient's pain. Radiographs of the involved joints are not likely to yield much useful information to assist with a diagnosis. Likewise, an MRI scan of the lumbar spine is not likely to provide much information regarding the etiology of the patient's condition. When a rheumatologic illness is suspected, the selective use of confirmatory laboratory testing can aid in arriving at a correct diagnosis. A presumed case of gout or chondrocalcinosis can be confirmed by the presence of the appropriate crystals in a joint-fluid aspiration. Because of the patient's recent trip to Costa Rica and the subsequent gastroenteritis, a CBC count, ESR, and CRP should be ordered to rule out infectious and inflammatory versus noninflammatory conditions. Rheumatoid factor (RF) in general should only be ordered for patients with polyarticular joint inflammation for more than 6 weeks. The presence of rheumatoid factor does not indicate rheumatoid arthritis. Antinuclear antibodies (ANA) should be ordered when a connective tissue disease such as systemic lupus erythematosus (SLE) is suspected on the basis of specific history and physical examination findings, such as inflammatory arthritis. Human leukocyte antigen-B27 (HLA-B27) should be ordered only when the patient's history is compatible with ankylosing spondylitis or Reiter's syndrome and this patient had a history of Reiter's syndrome. Gardner GC, Kadel NJ: Ordering and interpreting rheumatologic laboratory tests. J Am Acad Orthop Surg 2003;11:60-67.
References:
Shojania K: Rheumatology: 2. What laboratory tests are needed? CMAJ 2000;162:1157-1163.
Question 86:
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Options:
- Middle glenohumeral
- Inferior glenohumeral
- Coracoacromial
- Coracoclavicular
- Coracohumeral
Correct Answer: Coracohumeral
Explanation:
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
References:
Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 87:
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?
Options:
- No additional consent needed
- Verbal approval
- Written approval
- Written approval with notarization
- Telephone consent witnessed by a nurse
Correct Answer: No additional consent needed
Explanation:
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Scientific References
:
Burrington-Brown J: Working smart: Does the privacy rule allow us to release patient information over the telephone without authorization? J AHIMA 2003;74:62.
Question 88:
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Options:
- humeral head replacement with rotator cuff repair.
- humeral head replacement without rotator cuff repair.
- arthrodesis of the shoulder.
- total shoulder replacement with rotator cuff repair.
- total shoulder replacement without rotator cuff repair.
Correct Answer: total shoulder replacement with rotator cuff repair.
Explanation:
Given the size of the rotator cuff tear, it is likely to be repaired; therefore, the treatment of choice is a total shoulder replacement with rotator cuff repair. Severe rotator cuff insufficiency can lead to early glenoid failure because of superior instability, and glenoid resurfacing should be avoided in those instances. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
References:
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 89:
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Options:
- Infection
- Lymphoma
- Paget's disease
- Massive bone infarct
- Old pelvic trauma
Correct Answer: Paget's disease
Explanation:
The radiograph shows enlargement of the bone, coarse trabeculation, a blastic appearance, and thickening of the cortex, revealing the classic appearance of Paget's disease in the sclerotic phase, the most common presentation. While lymphoma may present as a blastic lesion, it will not have the same enlargement, coarse trabeculation of bone, and the significant sclerosis seen here. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
References:
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 90:
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?
Options:
- Observation
- Oral antibiotics only
- IV antibiotics only
- Irrigation and debridement of the surgical site
- Irrigation and debridement of the surgical site with hardware removal
Correct Answer: Irrigation and debridement of the surgical site
Explanation:
The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal. Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
References:
Fang A, Hu SS, Endres N, et al: Risk factors for infection after spinal surgery. Spine 2005;30:1460-1465.
Question 91:
Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
Options:
- Increased blood loss
- Decreased range of motion of the knee
- Infection
- Hip pain
- Muscle weakness
Correct Answer: Hip pain
Explanation:
There is no difference between the rates of union, malunion, range of motion of the hip or knee, muscle weakness, or infection for the two types of femoral nail insertion. The only difference is the location of the morbidity, which is around the insertion point of the rod. The antegrade technique has more morbidity about the hip, and the retrograde insertion technique has more morbidity about the knee. Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169. Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
References:
Tornetta P III, Tiburzi D: Antegrade or retrograde reamed femoral nailing: A prospective, randomized trial. J Bone Joint Surg Br 2000;82:652-654.
Question 92:
A 25-year-old woman who fell on her outstretched hand reports chronic pain over the hypothenar eminence region and some dorsal ulnar wrist pain. She also notes difficulty playing golf and tennis. Plain radiographs of the hand and wrist are unremarkable. A CT scan is shown in Figure 36. What is the next most appropriate step in management?
Options:
- Ultrasound therapy
- MRI for further soft-tissue evaluation
- Open reduction and internal fixation of the hook of the hamate
- Excision of the hook of the hamate
- Electrodiagnostic evaluation
Correct Answer: Excision of the hook of the hamate
Explanation:
The CT scan reveals a hook of the hamate nonunion with irregular resorption at the fracture site, which is at the base of the hamate. Symptomatic relief of the pain and discomfort has been well documented after excision of the hook of the hamate. Ultrasound therapy will not provide long-term symptomatic relief or induce nonunion healing. MRI for further soft-tissue evaluation is inappropriate because this is a bony problem; the bony architecture of the wrist is best visualized by CT. Open reduction and internal fixation of the hook of the hamate does not provide the symptomatic relief that is found with excision of the hook of the hamate. In addition, the technical difficulties and relative risk of persistent nonunion after open reduction and internal fixation are not merited when hamate excision can be effected easily and causes no long-term untoward effects. Electrodiagnostic evaluation is inappropriate because there is no history of the persistent numbness and tingling that is found in peripheral compression neuropathies. Stark HH, Chao EK, Zemel NP, Rickard TA, Ashworth CR: Fracture of the hook of the hamate. J Bone Joint Surg Am 1989;71:1206-1207. Failla JM: Hook of hamate vascularity: Vulnerability to osteonecrosis and nonunion. J Hand Surg Am 1993;18:1075-1079. Carter PR, Easton RG, Littler JW: Ununited fracture of the hook of the hamate. J Bone Joint Surg Am 1977;59:583-588.
References:
Egawa M, Asai T: Fracture of the hook of the hamate: Report of six cases and the suitability of computerized tomography. J Hand Surg Am 1983;8:393-398.
Question 93:
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of
Options:
- observation.
- proximal tibial osteotomy.
- proximal tibial hemiepiphyseodesis.
- a long leg brace with a varus-producing strap.
- MRI to map the extent of the osseous physeal bridge.
Correct Answer: observation.
Explanation:
Although fractures of the proximal tibial metaphysis in young children appear innocuous, development of a progressive valgus deformity is possible despite adequate and appropriate treatment. When treating a child with this injury, it is prudent to warn the parents that a valgus deformity of the tibia may develop. The most likely cause is asymmetric growth of the proximal tibial physis. Because spontaneous angular improvement can be expected in most patients, surgery to correct these deformities should be delayed at least 2 to 3 years and should be limited to patients who have symptoms. There are no studies that document the efficacy of bracing for this deformity. Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
References:
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 94:
A patient who was involved in a motor vehicle accident 2 days ago now reports neck pain. He denies any other symptoms. Radiographs reveal a type II odontoid fracture that is 2 mm anteriorly displaced. Management consists of halo vest immobilization in extension, and repeat radiographs reveal that the fracture is completely reduced. The patient is discharged to home, but later that evening he notes difficulty swallowing while trying to eat dinner. What is the most likely cause of this difficulty?
Options:
- Injury to the recurrent laryngeal nerve
- Injury to the superior laryngeal nerve
- Esophageal trauma at the time of the fracture or at the time of the reduction
- Retropharyngeal edema or hematoma from the fracture
- Halo vest placement
Correct Answer: Halo vest placement
Explanation:
If the neck is immobilized in excessive extension, it can be difficult for the patient to swallow. If the patient had injured the recurrent or superior laryngeal nerve at the time of the accident, it is likely to have manifested itself earlier on. Esophageal trauma or retropharyngeal edema or hematoma from the fracture also should have manifested itself earlier. Because the fracture was completely reduced, it is unlikely that moving the small fragment posteriorly would have injured the esophagus. Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
References:
Glaser JA, Whitehill R, Stamp WG, Jane JA: Complications associated with the halo-vest: A review of 245 cases. J Neurosurg 1986;65:762-769.
Question 95:
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Options:
- Parosteal osteosarcoma
- Unicameral bone cyst
- Aneurysmal bone cyst
- Eosinophilic granuloma
- Fibrous dysplasia
Correct Answer: Fibrous dysplasia
Explanation:
The ground glass appearance on the radiograph, the hot bone scan, and histologic findings of bony spicules without osteoblastic rimming in a background of bland fibrous tissue all suggest fibrous dysplasia. Stress-related pain is common with activity because of the dysplastic bone. Parosteal osteosarcomas are surface lesions. Simple cysts, aneurysmal bone cysts, and eosinophilic granuloma are all possible radiographically; however, the histology is most consistent with fibrous dysplasia. Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
References:
Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 96:
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Options:
- Broad-spectrum parenteral antibiotics
- Repeat aspirations
- Irrigation and debridement
- Hyperbaric oxygen
- Resection of the sternoclavicular joint
Correct Answer: Resection of the sternoclavicular joint
Explanation:
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
References:
Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 97:
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Options:
- Cast immobilization for 6 weeks
- Hinged brace with early range of motion in supination
- Hinged brace with early range of motion in pronation
- Primary ligament repair
- Lateral collateral ligament reconstruction with tendon graft
Correct Answer: Hinged brace with early range of motion in pronation
Explanation:
Most closed simple dislocations are best managed with early range of motion. Posterior dislocation typically occurs through a posterolateral rotatory mechanism. When placed in pronation, the elbow has greater stability when the medial ligamentous structures are intact. In traumatic dislocations, MRI rarely provides additional information that will affect treatment. In elbows that remain unstable, primary repair is preferred over ligament reconstruction. Cast immobilization increases the risk of arthrofibrosis.
References:
O'Driscoll SW, Morrey BF, Korinek S, et al: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 98:
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?
Options:
- Thorough history and physical examination
- CBC count, electrolytes, and serum protein electrophoresis
- Bone scan
- CT of the brain
- Radiograph and CT of the chest
Correct Answer: CT of the brain
Explanation:
The work-up for a patient with an unknown primary lesion that is metastatic to bone includes a search for the primary tumor and other sites of metastasis. This involves conducting a thorough history and physical examination, appropriate laboratory studies, bone scan, chest radiograph, and CT of the chest, abdomen, and pelvis. In women, a mammogram may be indicated. CT of the brain is not necessary in the early stages of a metastatic work-up. Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
References:
Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 99:
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Options:
- lateral placement, directly within the temporalis muscle.
- lateral to the medial third of the orbit.
- lateral to the lateral aspect of the orbit.
- above the medial third of the orbit.
- lateral between the temporalis muscle and zygomatic temporal nerve.
Correct Answer: lateral to the medial third of the orbit.
Explanation:
Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable. Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Scientific References
:
Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.
Question 100:
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Options:
- an elevated thyroid-stimulating hormone level.
- an elevated estrogen level.
- elevated blood urea nitrogen and creatinine levels.
- a growth hormone deficiency.
- normal laboratory values.
Correct Answer: normal laboratory values.
Explanation:
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
References:
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.