Full Question & Answer Text (for Search Engines)
Question 1:
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include
Options:
- repair of the posterior interosseous nerve.
- repair of the median nerve at the elbow.
- neurolysis of the anterior interosseous nerve.
- observation of the nerve palsy.
- immediate electromyography and nerve conduction velocity studies.
Correct Answer: observation of the nerve palsy.
Explanation:
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
References:
Sood MK, Burke FD: Anterior interosseous nerve palsy: A review of 16 cases. J Hand Surg Br 1997;22:64-68.
Question 2:
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?
Options:
- Distal soft-tissue realignment
- Distal first metatarsal osteotomy with distal soft-tissue realignment
- Proximal first metatarsal osteotomy with distal soft-tissue realignment
- Proximal and distal first metatarsal osteotomy
- Osteotomy of the proximal phalanx
Correct Answer: Proximal and distal first metatarsal osteotomy
Explanation:
The radiograph reveals an increased first-second intermetatarsal angle and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular angle. Correction of both of these abnormalities requires a proximal and distal first metatarsal osteotomy. Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Scientific References
:
Peterson HA, Newman SR: Adolescent bunion treated with double osteotomy and longitudinal pin fixation of the first ray. J Pediatr Orthop 1993;13:80-84.
Question 3:
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?
Options:
- No immobilization, no time off from work, and instructions to go about normal activities
- Part-time soft collar immobilization and modified duty at work for 1 to 2 weeks
- Full-time soft collar immobilization and modified duty at work for 1 to 2 weeks
- Full-time rigid collar immobilization and time off from work for 1 to 2 weeks
- Repeat MRI to assess for occult disk or ligamentous injury
Correct Answer: No immobilization, no time off from work, and instructions to go about normal activities
Explanation:
Early mobilization and resumption of normal activities immediately after neck sprain has been shown to improve functional outcome and decrease subjective symptoms as measured 6 months after injury. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
References:
Mealy K, Brennan H, Fenelon GC: Early mobilization of acute whiplash injuries. Br Med J 1986;292:656-657.
Question 4:
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Options:
- intralesional.
- marginal.
- wide.
- wide contaminated.
- radical.
Correct Answer: intralesional.
Explanation:
Surgical margins are classified according to the plane of dissection in relation to the tumor. An intralesional procedure is where the plane of dissection passes through the tumor. A marginal resection involves a resection where the plane of dissection is through the reactive zone of the tumor. A wide resection is through completely normal tissue outside of the reactive zone. A radical resection removes all of the muscles and/or bone of the compartment that are involved by the tumor.
References:
Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120.
Question 5:
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?
Options:
- Multiple myeloma
- Metastatic neuroblastoma
- Polyostotic fibrous dysplasia
- Hodgkin's lymphoma
- Metastatic prostate cancer
Correct Answer: Metastatic prostate cancer
Explanation:
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
Scientific References
:
Sartor O: Radioisotopic treatment of bone pain from metastatic prostate cancer. Curr Oncol Rep 2003;5:258-262.
Question 6:
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Options:
- High histologic grade
- Tumor size greater than 8 cm
- Extracompartmental growth
- Solitary pulmonary metastasis
- Solitary bone metastasis
Correct Answer: Solitary bone metastasis
Explanation:
Distant bone metastasis is associated with an extremely poor prognosis for patients with osteosarcoma (5-year survival rate of less than 10%). Most osteosarcomas are high grade and extracompartmental, and approximately half are greater than 8 cm at presentation. The 5-year survival rate for these patients is approximately 70%. Patients with a solitary pulmonary metastasis have a prognosis worse than patients without detectable metastases but not as bad as those with bone metastases. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790. Heck RK, Stacy GS, Flaherty MJ, et al: A comparison study of staging systems for bone sarcomas. Clin Orthop Relat Res 2003;415:64-71.
References:
Kager L, Zoubeck A, Potschger U, et al: Primary metastatic osteosarcoma: Presentation and outcome of patients treated on neoadjuvant Cooperative Osteosarcoma Study Group protocols. J Clin Oncol 2003;21:2011-2018.
Question 7:
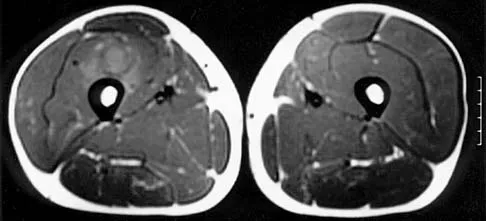
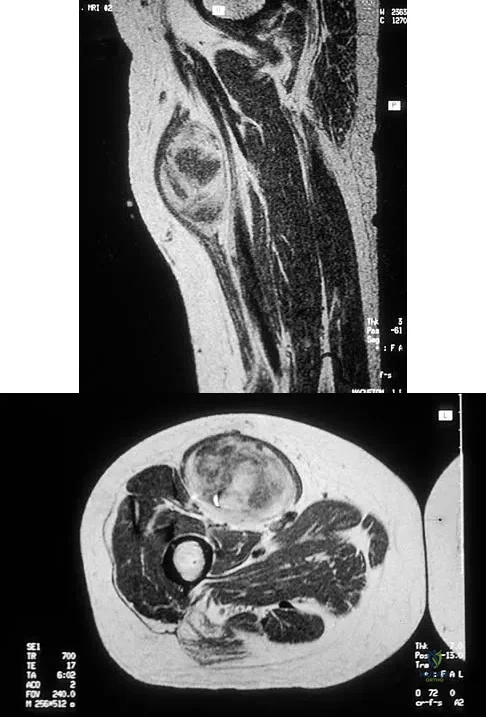
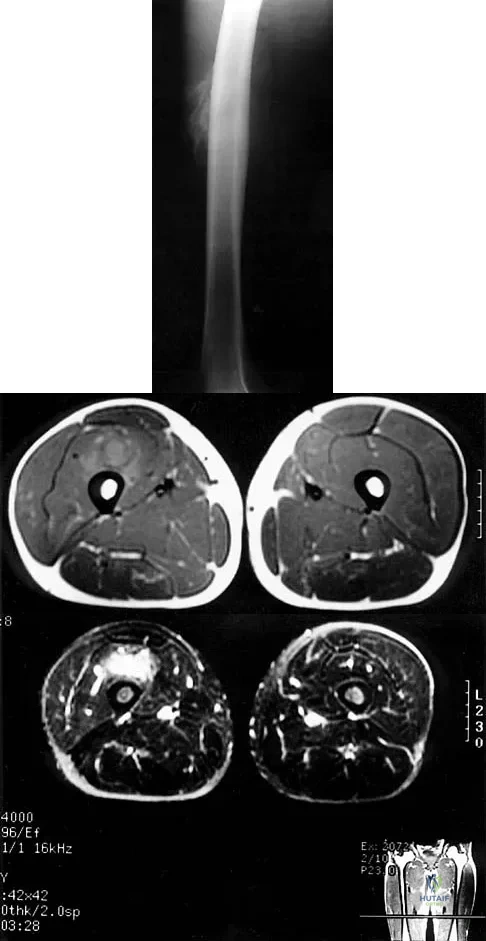
Figures 30a and 30b show the MRI scans of a 51-year-old woman who has had an enlarging soft-tissue mass in her right thigh for the past 18 months. Examination reveals no inguinal adenopathy. Results of a biopsy show a high-grade sarcoma. A bone scan is unremarkable, and a CT scan of the chest shows no evidence of pulmonary metastasis. According to the Musculoskeletal Tumor Society (MSTS) staging system, the tumor should be classified as what stage?
Options:
Correct Answer: IIA
Explanation:
According to the MSTS staging system, soft-tissue sarcomas are staged according to the following factors: grade, site, and metastasis. Roman numerals are used to designate malignant tumors, and Arabic numerals are used for benign tumors. Low-grade malignant tumors are staged as I while intermediate- and high-grade tumors are staged as II. Site is defined as intracompartmental (A) or extracompartmental (B). Any metastasis is staged as III. This patient has a high-grade tumor (II), and the MRI scans show that it is confined to a single compartment; therefore, it is staged as IIA. There is no evidence of metastatic disease. Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF: Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996;14:1679-1689.
References:
Wunder JS, Healey JH, Davis AM, Brennan MF: A comparison of staging systems for localized extremity soft tissue sarcoma. Cancer 2000;88:2721-2730.
Question 8:
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Options:
- Long arm cast for 2 weeks, followed by range of motion
- Early range of motion
- Metallic radial head arthroplasty
- Silastic radial head arthroplasty
- Excision of the radial head
Correct Answer: Metallic radial head arthroplasty
Explanation:
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
References:
Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Question 9:
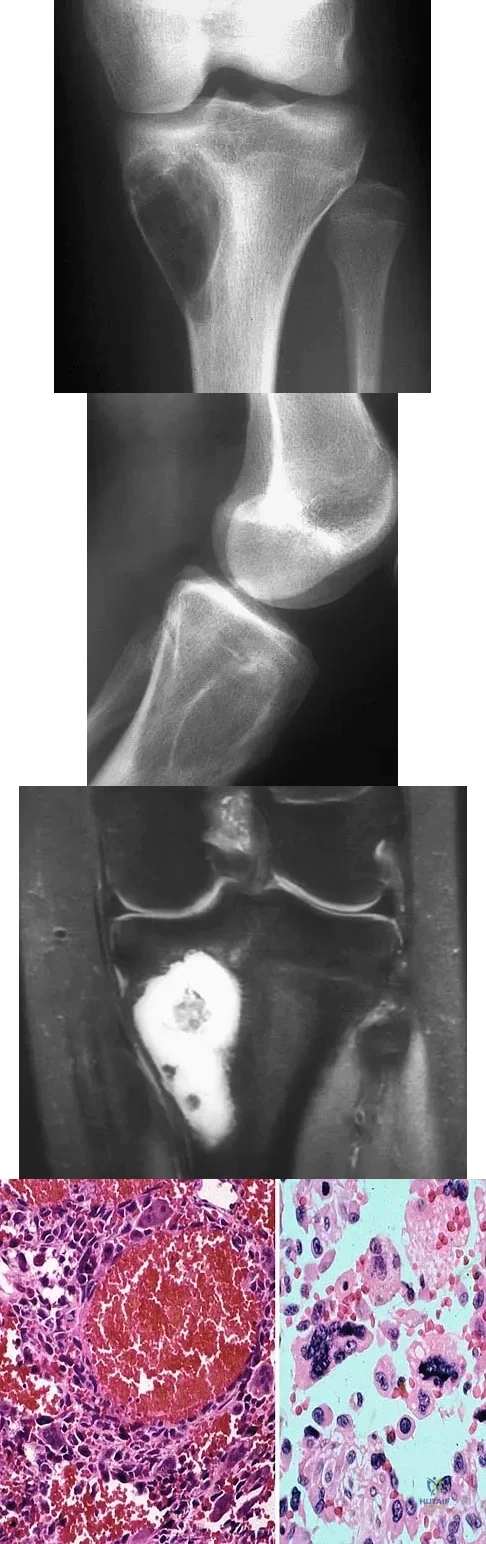
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?
Options:
- Giant cell tumor
- Infection
- Chondrosarcoma
- Osteosarcoma
- Chondroblastoma
Correct Answer: Osteosarcoma
Explanation:
The radiographs reveal a blastic lesion of the proximal tibial metaphysis with cortical destruction, mineralization extending into the soft tissue laterally, indistinct margins, and destruction of the normal trabecular pattern. In this age group, with this aggressive appearance, osteosarcoma is the most likely diagnosis. Chondroblastoma and giant cell tumor are generally geographic and lytic. Chondrosarcoma is rare in this age group and would likely be a secondary lesion from an underlying chondroid tumor that is not present here. Whereas infection can have a wide variety of appearances, it tends to be more lytic in the acute presentation. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
References:
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 10:
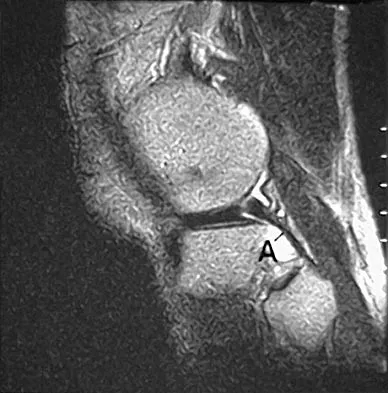
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Options:
- Anterior superior iliac spine
- Sciatic buttress
- A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
- The most superior portion of the roof of the acetabulum
- Iliopectineal line
Correct Answer: A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
Explanation:
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
References:
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 11:
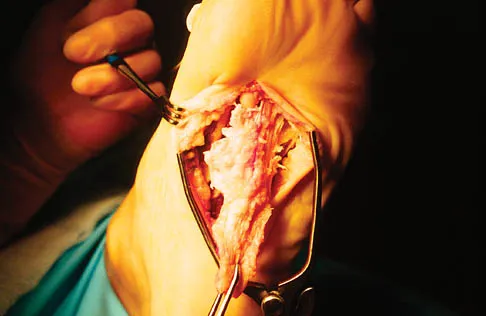
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Options:
- Myocyte
- T-cell
- Synovial cell
- Osteocyte
- Fibromyoblast
Correct Answer: Fibromyoblast
Explanation:
The history, examination, and surgical findings are most consistent with plantar fibromatosis. Plantar fibromatosis is a benign tumor of the plantar fascia that consists chiefly of fibromyoblasts. These cells produce excessive collagen and are similar to the cells found in the palmar fascia of patients with Dupuytren's contracture of the hand. The myocyte, synovial cell, and osteocyte all produce their respective individual tissue types but do not contribute to the formation of a plantar fibromatosis. The T-cell is an important immunologic cell that is most affected in patients with HIV.
References:
Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 12:
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Options:
- Technetium Tc 99m bone scan
- Intravenous antibiotics
- Oral antibiotics
- CT of the hips
- Aspiration of the left hip
Correct Answer: Aspiration of the left hip
Explanation:
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
References:
Kocher MS, Zurakowski D, Kasser JR: Differentiating between septic arthritis and transient synovitis of the hip in children: An evidence-based clinical prediction algorithm. J Bone Joint Surg Am 1999;81:1662-1670.
Question 13:
Which of the following are considered characteristic features of degeneration of a disk?
Options:
- Reduced water and glycosaminoglycan content and increased noncollagen glycoprotein
- Reduced water and glycosaminoglycan content and reduced noncollagen glycoprotein
- Reduced water content, increased glycosaminoglycan content, and increased noncollagen glycoprotein
- Increased water and glycosaminoglycan content and increased noncollagen glycoprotein
- Increased water and glycosaminoglycan content and reduced noncollagen glycoprotein
Correct Answer: Reduced water and glycosaminoglycan content and increased noncollagen glycoprotein
Explanation:
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
References:
Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 14:
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Options:
- in situ subtalar fusion.
- tibiotalocalcaneal arthrodesis using an intramedullary rod.
- ankle arthroscopy with debridement of osteophytes.
- subtalar distraction bone block arthrodesis.
- lateral wall ostectomy of the calcaneus.
Correct Answer: subtalar distraction bone block arthrodesis.
Explanation:
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Scientific References
:
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 15:
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Options:
- Ascending branch of the lateral femoral circumflex
- Superior gluteal
- Femoral
- Profunda femoris
- Medial femoral circumflex
Correct Answer: Ascending branch of the lateral femoral circumflex
Explanation:
The ascending branch of the lateral femoral circumflex artery crosses the gap between the tensor fascia lata and the sartorious and must be identified and ligated or coagulated. The other vessels are out of the field of dissection. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
References:
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 16:
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Options:
- cementless fixation.
- suction drains.
- general anesthesia.
- preoperative erythropoietin injections.
- low-molecular-weight heparin.
Correct Answer: preoperative erythropoietin injections.
Explanation:
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
References:
Feagan BG, Wang CJ, Kirkley A, et al: Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty: A randomized, controlled, trial. Ann Intern Med 2000;133:845-854.
Question 17:
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Options:
- septic arthritis.
- slipped capital femoral epiphysis.
- femoral head fracture (Pipkin I).
- developmental dysplasia of the hip.
- Legg-Calve-Perthes disease.
Correct Answer: Legg-Calve-Perthes disease.
Explanation:
Radiographic abnormalities such as coxa magna, coxa breva secondary to growth arrest, and coxa plana and acetabular deformities are associated with healed Legg-Calve-Perthes disease. Femoral heads that were flat yet congruent with the acetabulum are at risk for disabling arthritis in the sixth decade of life in 50% of these untreated patients. As the normal ball-and-socket joint deforms to a flattened cylinder, the hip loses abduction and rotation capability, while retaining flexion and extension potential. If the femoral head is flat and is not concentric with the acetabulum, early severe arthritis occurs. Hinge abduction and anterior impingement are known sequelae of a flat, incongruent femoral head.
References:
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 18:
A favorable outcome following nonsurgical management of a partial tear of the posterior cruciate ligament (PCL) is best associated with
Options:
- hamstring strength.
- quadriceps strength.
- a body mass index of less than 30.
- anterior cruciate ligament stability.
- compliance with brace use.
Correct Answer: quadriceps strength.
Explanation:
Rehabilitation of the quadriceps muscle following a partial tear of the PCL has been associated with a favorable outcome. The quadriceps acts an antagonist to the PCL because its contraction results in anterior tibial translation, which reduces the tensile stress on the injured ligament. Strengthening of the hamstring musculature increases posterior tibial translation and is contraindicated during the early rehabilitative phase following a PCL injury. Brace use has not been found to significantly alter the outcome following nonsurgical management of PCL tears. Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-38.
References:
Griffin JR, Annunziata CC, Harner CD: Posterior cruciate ligament injuries in the adult, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2083-2106.
Question 19:
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Options:
- closed reduction of the ulna and transcapitellar pinning of the radial head.
- closed reduction of the ulna and radial head dislocation.
- closed reduction of the ulna and annular ligament repair.
- open reduction of the radius and plating of the ulna.
- open reduction of the ulna and immobilization in an extension cast.
Correct Answer: closed reduction of the ulna and radial head dislocation.
Explanation:
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
References:
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 20:
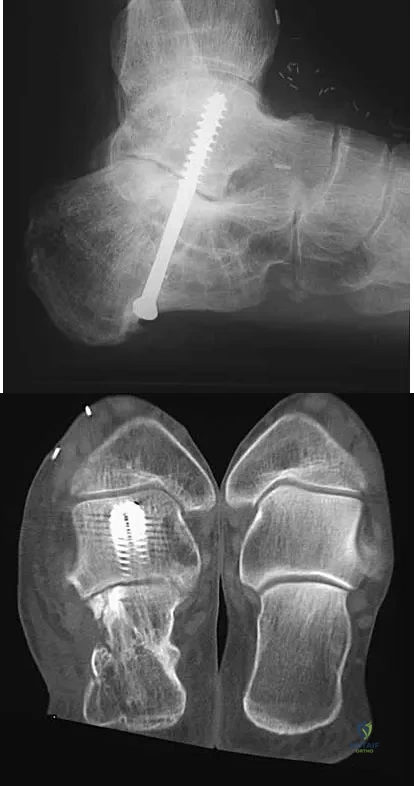
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Options:
- casting with an external bone stimulator.
- ankle arthrodesis.
- revision subtalar arthrodesis.
- conversion to triple arthrodesis without revision of the subtalar arthrodesis.
- conversion to triple arthrodesis with revision of the subtalar arthrodesis.
Correct Answer: conversion to triple arthrodesis with revision of the subtalar arthrodesis.
Explanation:
The patient has a nonunion at the subtalar joint because of poor preparation of the arthrodesis site with incomplete removal of the articular cartilage. Clinically, he has arthritis at the transverse tarsal joint. Casting with a bone stimulator is not expected to result in a union of the subtalar arthrodesis. To address both the subtalar nonunion and the transverse tarsal joint arthritis, revision of the subtalar arthrodesis and conversion to a triple arthrodesis is the preferred option. Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362. Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499. Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307. Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
References:
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 21:
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Options:
- serial injection of steroids into the area of discomfort.
- custom orthotics with a second metatarsal pad.
- physical therapy for transcutaneous electrical nerve stimulation and desensitization.
- plantar condylectomy of the second and third metatarsal heads.
- plantar exploration and revision neurectomy to a more proximal level.
Correct Answer: plantar exploration and revision neurectomy to a more proximal level.
Explanation:
Most patients with a significant recurrent neuroma will not obtain relief with conservative methods. Pain results from a stump neuroma at the weight-bearing area from too short of a resection of the nerve or from regrowth of the remaining nerve end. Although steroid injection may be helpful in localizing symptoms or providing temporary relief, it rarely cures a stump neuroma. Orthotics with a metatarsal pad will likely increase pressure and pain at the neuroma site. Physical therapy could temporize the symptoms but will not address the underlying problem. Similarly, bone decompression alone will not alter the location of the neuroma stump. Revision of the nerve to a more proximal level off of the weight-bearing area is the most likely method to succeed. A plantar approach facilitates identification and ability to revise the nerve to a more proximal level. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657. Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
References:
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton's neuroma excision. Foot Ankle 1992;13:153-156.
Question 22:
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Options:
- observation.
- physical therapy.
- ulnohumeral arthroplasty.
- ulnohumeral arthroplasty and ulnar nerve decompression.
- semiconstrained elbow arthroplasty.
Correct Answer: ulnohumeral arthroplasty and ulnar nerve decompression.
Explanation:
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis. Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
References:
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
Question 23:
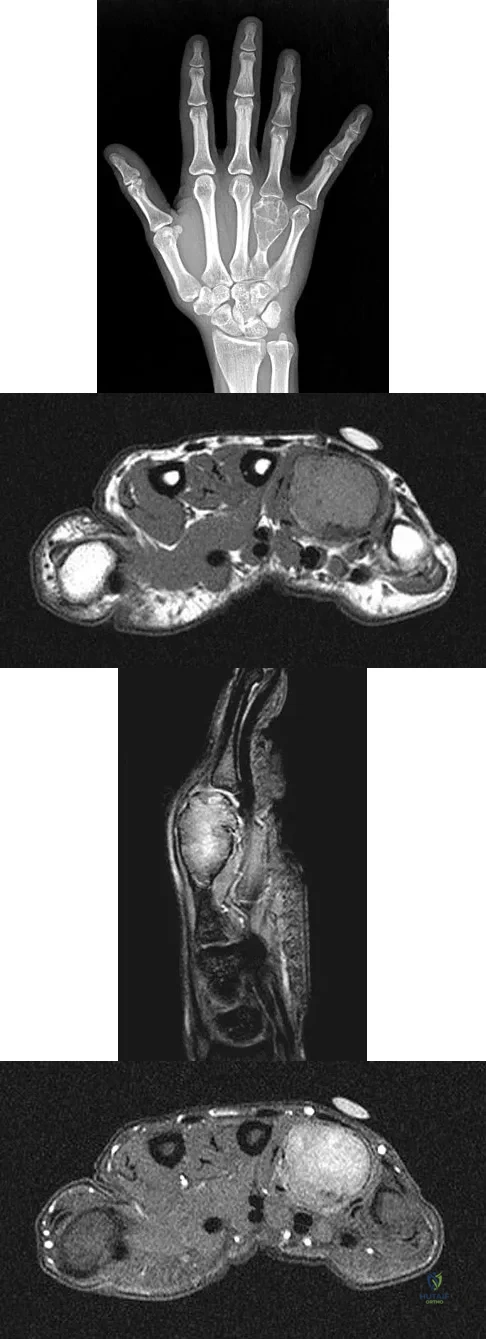
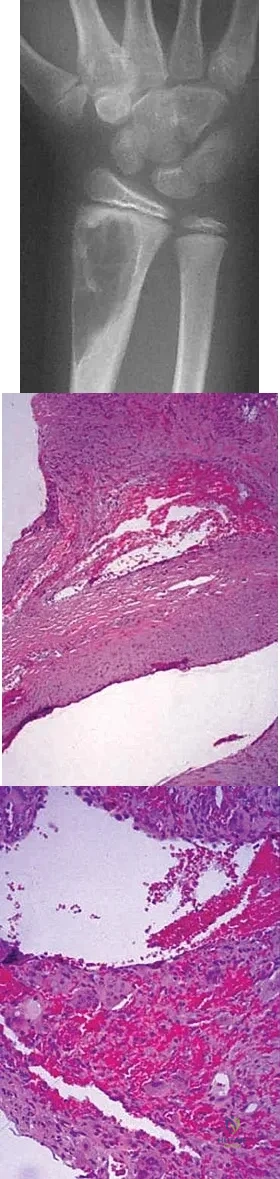
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?
Options:
- Infection
- Giant cell tumor
- Nonossifying fibroma
- Enchondroma
- Osteosarcoma
Correct Answer: Giant cell tumor
Explanation:
The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
References:
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 24:
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Options:
- bone obtained through a knee arthrotomy with creation of a portal that will be used for retrograde femoral nailing.
- bone obtained by going through the mass.
- bone obtained through a posterior approach, dissecting out and protecting the sciatic nerve and popliteal artery.
- soft tissue obtained through a longitudinal incision centered over the mass.
- soft tissue obtained through a transverse incision on the medial thigh.
Correct Answer: soft tissue obtained through a longitudinal incision centered over the mass.
Explanation:
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
References:
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 25:
Figure 21 shows the radiograph of an 18-year-old man who was brought to the emergency department with shoulder pain following a rollover accident on an all-terrain vehicle. Examination reveals a fracture with massive swelling; however, the skin is intact and not tented over the fracture. Based on these findings, initial management should consist of
Options:
- closed reduction of the displaced clavicular fracture.
- a figure-of-8 clavicular brace to stabilize the clavicular fracture.
- arteriography to evaluate for vascular injury.
- electromyography to evaluate for a brachial plexus injury.
- CT to evaluate for a scapular fracture.
Correct Answer: arteriography to evaluate for vascular injury.
Explanation:
The radiographic and clinical findings suggest a scapulothoracic dissociation with a widely displaced clavicular fracture and a laterally displaced scapula. These injuries have a high association with neurovascular injuries to the brachial plexus and subclavian artery. Emergent vascular evaluation with arteriography and possible vascular repair are indicated. This repair can be combined with open reduction and internal fixation of the clavicle to improve stability. Delay in treatment of these vascular injuries can be devastating. Iannotti JP, Williams GR (eds): Disorders of the Shoulder. Philadelphia, PA, Lippincott, 1999, pp 632-635.
References:
Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432.
Question 26:
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15 degrees of valgus, and forefoot supination can be corrected to 10 degrees from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Options:
- medial sliding calcaneal osteotomy with flexor digitorum longus (FDL) transfer.
- isolated subtalar arthrodesis.
- isolated talonavicular arthrodesis.
- triple arthrodesis.
- subtalar arthroereisis.
Correct Answer: triple arthrodesis.
Explanation:
The most important determining factor for correction of an adult flatfoot without an arthrodesis is the flexibility of the subtalar and transverse tarsal joints. Rigid deformities cannot be corrected with a medial sliding calcaneal osteotomy with FDL transfer or a subtalar arthroereisis. Isolated subtalar or talonavicular arthrodesis does not correct the deformities entirely. If the patient has forefoot supination that can be corrected to less than 7 degrees, an isolated subtalar fusion is a possible alternative.
References:
Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 27:
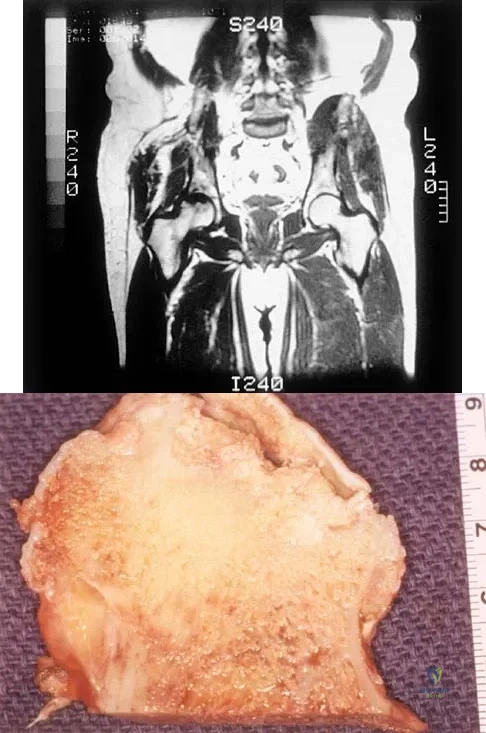
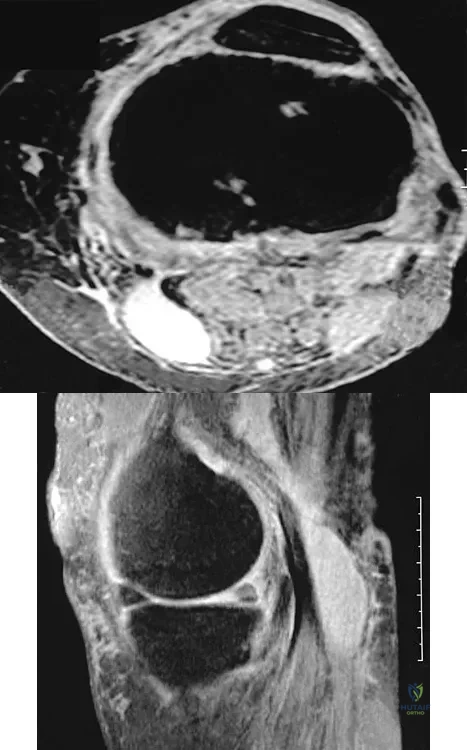
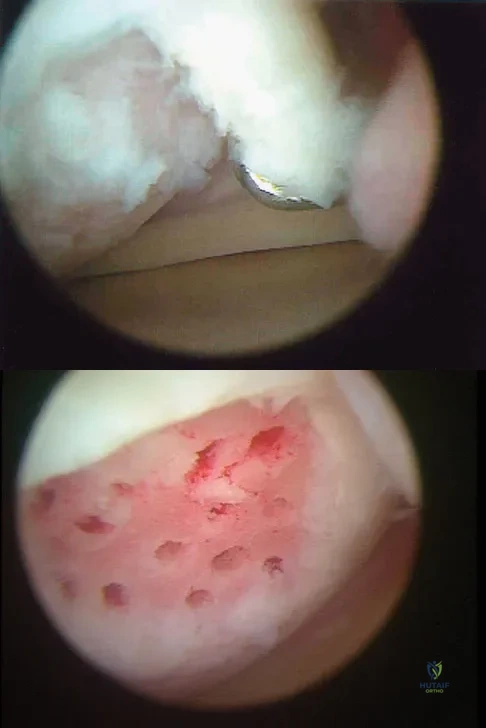
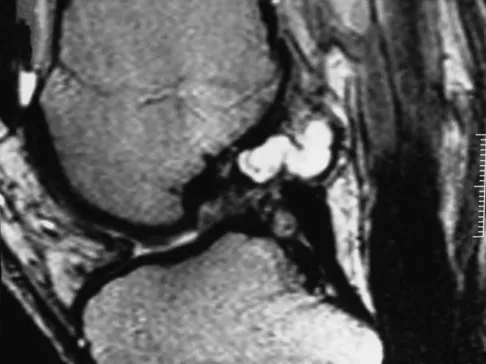
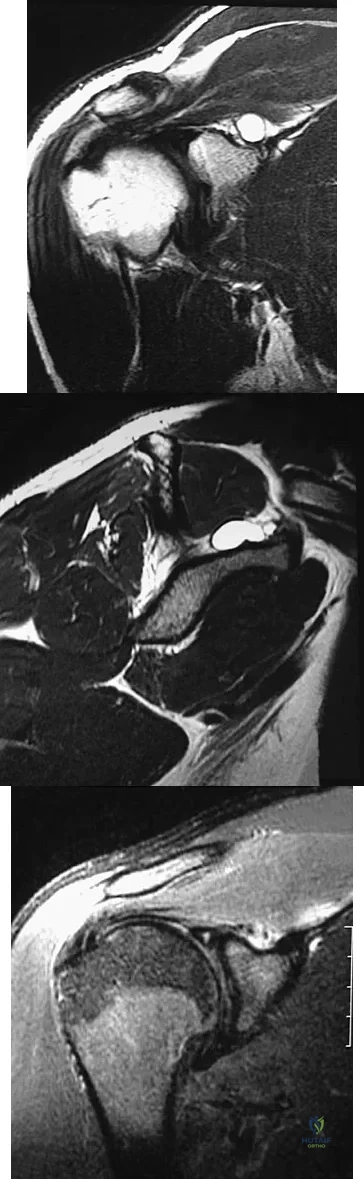
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of
Options:
- synovectomy.
- local excision with arthroplasty.
- radiation synovectomy.
- radiation therapy.
- radical resection.
Correct Answer: synovectomy.
Explanation:
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
References:
Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 28:
The spread of malignant cells to the vertebrae is often through
Options:
- epidural extension.
- Batson's vertebral plexus.
- the lymphatic system.
- direct tumor extension.
- arterial circulation including the artery of Adamkiewicz.
Correct Answer: Batson's vertebral plexus.
Explanation:
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
References:
Batson OV: The function of the vertebral veins and their role in the spread of metastases. Ann Surg 1940;112:138-149.
Question 29:
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Options:
- observation.
- serial casting.
- flexion osteotomy of the distal humerus.
- posterior soft-tissue elbow release and anterior triceps transfer.
- adaptive equipment.
Correct Answer: posterior soft-tissue elbow release and anterior triceps transfer.
Explanation:
Elbow release and triceps transfer to restore motion can be performed in children who are age 4 years and older. The ability to flex the elbow either actively or passively is of great assistance in activities of daily living. Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
References:
Caroll RE, Hill NA: Triceps transfer to restore elbow flexion: A study of fifteen patients with paralytic lesions and arthrogryposis. J Bone Joint Surg Am 1970;52:239-244.
Question 30:
A 54-year-old woman underwent prophylactic intramedullary fixation for an impending fracture of her right femur secondary to metastatic breast cancer. A bone scan revealed a second lesion in her inferior pubic ramus. Her oncologist has recommended that she receive the intravenous bisphosphonate, zoledronic acid, because the medication would
Options:
- result in increased bone density.
- accelerate healing of the femoral fracture.
- lower the serum phosphate level.
- reduce processing of future bone metastases.
- heal other impending fractures.
Correct Answer: reduce processing of future bone metastases.
Explanation:
Bisphosphonates have been reported to reduce the incidence of new osseous lesions and prevent an increase in size of existing lesions. Zoledronic acid has been reported in clinical trials to decrease the skeletal complications of patients with multiple myeloma and with bone metastases from solid tumors. Results also have demonstrated that zoledronic acid delays the initial onset of bone complications by more than 2 months in patients with non-small-cell lung cancer and other solid tumors. In two placebo-controlled clinical studies of zoledronic acid conducted in patients with bone metastases from prostate cancer or other solid tumors, there was a decrease in the number of patients with skeletal-related events compared to placebo, and the time to the first skeletal-related event was delayed. Mundy GR, Yoneda T: Bisphosphonates as anticancer drugs. N Engl J Med 1998;339:398-400.
References:
Rosen LS, Gordon D, Kaminski M, et al: Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: A phase III, double-blind, comparative trial. Cancer J 2001;7:377-387.
Question 31:
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
Options:
- immediate hospital admission and surgery because of the risk of paralysis.
- surgery within 24 hours.
- surgery within the next several days.
- elective surgery at the next available surgical date.
- additional nonsurgical management.
Correct Answer: additional nonsurgical management.
Explanation:
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
References:
Komori H, Shinomiya K, Nakai O, Yamaura I, Takeda S, Furuya K: The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996;21:225-229.
Question 32:
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Options:
- use of a sling for 3 weeks followed by a gradual return to activities.
- physical therapy.
- arthroscopy with removal of the loose fragment.
- arthroscopy with in situ drilling of the fragment.
- internal fixation of the fragment.
Correct Answer: arthroscopy with removal of the loose fragment.
Explanation:
Osteochondritis dissecans of the capitellum is seen most commonly in adolescent athletes. It should be distinguished from osteochondrosis of the capitellum (Panner's disease), a self-limiting condition seen in younger patients. Lesions are graded I through V based on radiographic and arthroscopic appearance. Grade I lesions show intact but soft cartilage. Grade II lesions show fissuring of the overlying cartilage. Grade III lesions show exposed bone or an attached osteoarticular flap that is not loose. Grade IV lesions show a loose but nondisplaced osteoarticular flap. Grade V lesions show a displaced fragment. Simple excision of the loose osteoarticular flap is the treatment of choice for grade IV and V lesions. More complex procedures such as drilling of the in situ lesion, bone grafting, or internal fixation are associated with significantly worse results. While some authors advocate abrasion chondroplasty, the long-term benefits of the procedure are yet to be proven. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
References:
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
Question 33:
The attachments of the transverse carpal ligament include which of the following structures?
Options:
- Scaphoid and the ulna
- Trapezium and the hook of the hamate
- Trapezium and the triquetrum
- Trapezoid and the hook of the hamate
- Trapezoid and the pisiform
Correct Answer: Trapezium and the hook of the hamate
Explanation:
The transverse carpal ligament is the volar boundary of the carpal tunnel. It attaches to the scaphoid and trapezium radially and the pisiform and the hook of the hamate ulnarly. The ulna and trapezoid do not receive attachments of the transverse carpal ligament. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
References:
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 168-170.
Question 34:
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of
Options:
- observation.
- bilateral adductor and iliopsoas releases, with nighttime abduction bracing.
- proximal femoral varus osteotomy with internal fixation.
- proximal femoral varus osteotomy with volume-reducing periacetabular osteotomy.
- proximal femoral varus osteotomy with shelf acetabular augmentation.
Correct Answer: observation.
Explanation:
Observation is the treatment of choice. Hip subluxation and dislocation are not uncommon in patients with SMA type II who are unlikely to be ambulatory. Scoliosis occurs in these patients 100% of the time and frequently creates pelvic obliquity. However, in long-term follow-up, patients with SMA type II and hip dislocations had little associated pain or functional limitations because of hip instability. In addition, recurrent hip subluxation after surgical treatment has been documented. Given the rarity of symptoms from hip instability in long-term follow-up, and the possibility of recurrent dislocation, surgical intervention for hip instability may expose SMA type II patients to undue surgical risk for minimal if any functional gain. Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
References:
Thompson CE, Larsen LJ: Recurrent hip dislocation in intermediate spinal atrophy. J Pediatr Orthop 1990;10:638-641.
Question 35:
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?
Options:
- Repeat trial of epidural steroid injections
- Pain management referral for narcotic management of symptoms
- Lumbar laminectomies at L4-5
- Lumbar laminectomies and fusion at L4-5
- Bilateral lumbar laminotomies at L3-4 and L4-5
Correct Answer: Lumbar laminectomies and fusion at L4-5
Explanation:
Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients. Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
References:
Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 36:
In a patient with a soft-tissue sarcoma treated by wide excision and radiation therapy, the risk of subsequent fracture is probably most influenced by
Options:
- location of the sarcoma in the lower extremity.
- excision of cortical bone with en bloc resection.
- a radiation dose of 60 Gy (6,000 cGy) versus 50 Gy (5,000 cGy).
- the addition of adjuvant chemotherapy.
- excision of the periosteum.
Correct Answer: excision of cortical bone with en bloc resection.
Explanation:
While most pathologic fractures are in the lower extremity in patients treated for soft-tissue sarcomas by wide excision and adjuvant radiation therapy, risk factors for such fractures are bone resection associated with excision of the tumor and soft-tissue sarcomas of the thigh that require periosteal stripping at the time of resection. Such fractures can occur late, often more than 6 months after surgery, are difficult to treat, and often result in nonunion. Bell RS, O'Sullivan B, Nguyen C, et al: Fractures following limb-salvage surgery and adjuvant irradation for soft-tissue sarcoma. Clin Orthop 1991;271:265-271.
References:
Lin PP, Boland PJ, Healey JH: Treatment of femoral fractures after irradiation. Clin Orthop 1998;352:168-178.
Question 37:
Figure 17 shows the radiograph of an 11-year-old boy with Duchenne muscular dystrophy who has been nonambulatory for the past 2 years. Management of the spinal deformity should consist of
Options:
- wheelchair modifications and custom-molded inserts.
- posterior fusion with instrumentation.
- anterior and posterior fusion.
- observation and reexamination in 6 months.
- thoracolumbosacral orthosis bracing.
Correct Answer: posterior fusion with instrumentation.
Explanation:
The presence of any curve greater than 20 degrees in a nonambulatory patient with Duchenne muscular dystrophy is an indication for posterior fusion with instrumentation. Because of progressive cardiomyopathy and pulmonary deficiency, waiting until the curve is larger can increase the risk of pulmonary or cardiac complications during or following surgery. There is some disagreement as to whether all such fusions must extend to the pelvis. Bracing or other nonsurgical management is ineffective and is not indicated in this situation. Sussman M: Duchenne muscular dystrophy. J Am Acad Orthop Surg 2002;10:138-151.
References:
Mubarek SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 38:
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Options:
- Improve the conformity of the articular surfaces
- Reduce the maximum compressive stresses on the underlying cancellous bone
- Increase the tensile forces on the other condyle when one is loaded
- Decrease the thickness of the polyethylene tray
- Decrease the compressive forces on the polyethylene tray
Correct Answer: Reduce the maximum compressive stresses on the underlying cancellous bone
Explanation:
In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
References:
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 39:
The main blood supply to the lateral two thirds of the talar body is provided by the
Options:
- peroneal artery.
- anterior tibial artery.
- anterior lateral malleolar artery.
- artery of the tarsal sinus.
- artery of the tarsal canal.
Correct Answer: artery of the tarsal canal.
Explanation:
The main blood supply to the lateral two thirds of the talar body is derived from the artery of the tarsal canal, a branch of the posterior tibial artery. The peroneal artery helps form a vascular plexis over the posterior tubercle and combines with other arteries to form the artery of the sinus tarsi, which is the principal blood supply of the intrasinus structures of the talus. The anterior tibial arteries send branches to the superior surface of the talar head and give rise to the anterolateral malleolar artery, which may anastomose with other vessels to form the artery of the tarsal sinus. Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
References:
Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115-1120.
Question 40:
What is the main mechanism for nutrition of the adult disk?
Options:
- Capillary network from the adjacent segmental arteries
- Capillary network from the arterioles in the vertebral body
- Diffusion through the anulus fibrosus
- Diffusion through pores in the end plates
- Diffusion through nerves in the dorsal root ganglion
Correct Answer: Diffusion through pores in the end plates
Explanation:
Disk nutrition occurs via diffusion through pores in the end plates. The disk has no direct blood supply, and the anulus is not porous to allow diffusion. The dorsal root ganglion does not provide blood supply to the disc. Biyani A, Andersson GB: Low back pain: Pathophysiology and management. J Am Acad Orthop Surg 2004;12:106-115. Urban JG, Holm S, Maroudas A, et al: Nutrition of the intervertebral disc: Effect of fluid flow on solute transport. Clin Orthop 1982;170:296-302.
References:
Park AE, Boden SD: Intervertebral disk: Form and function, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 41:
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Options:
- remain essentially unchanged in size.
- result in neurologic deterioration.
- gradually resorb and widen the spinal canal.
- potentially migrate within the spinal canal.
- increase the risk of further injury to the adjacent dural sac.
Correct Answer: gradually resorb and widen the spinal canal.
Explanation:
Numerous articles have reported that both surgical and nonsurgical management of burst fractures are associated with resolution of impingement at long-term follow-up. If the patient is neurologically intact and appropriately treated at the time of injury, neurologic deterioration is not expected nor is there a risk of injury to the dural sac. The retained fragments can be expected to gradually resorb and widen the spinal canal. Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
References:
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 42:
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?
Options:
- Synovial herniation pits
- Osteoid osteoma
- Fibrous dysplasia
- Metastatic bone disease
- Multiple enchondromas
Correct Answer: Synovial herniation pits
Explanation:
Synovial herniation pits or Pitt's pits are tumor simulators and are incidentally identified on radiographs obtained for either pain or trauma. The main diagnostic pitfall with this lesion is mistakenly identifying it as an osteoid osteoma. Accurate diagnosis is achieved by knowledge of the location and the characteristic imaging appearance. These are common lesions in individuals with femoroacetabular impingement. Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
References:
Daenen B, Preidler KW, Padmanabhan S, et al: Symptomatic herniation pits of the femoral neck: Anatomic and clinical study. Am J Roentgenol 1997;168:149-153.
Question 43:
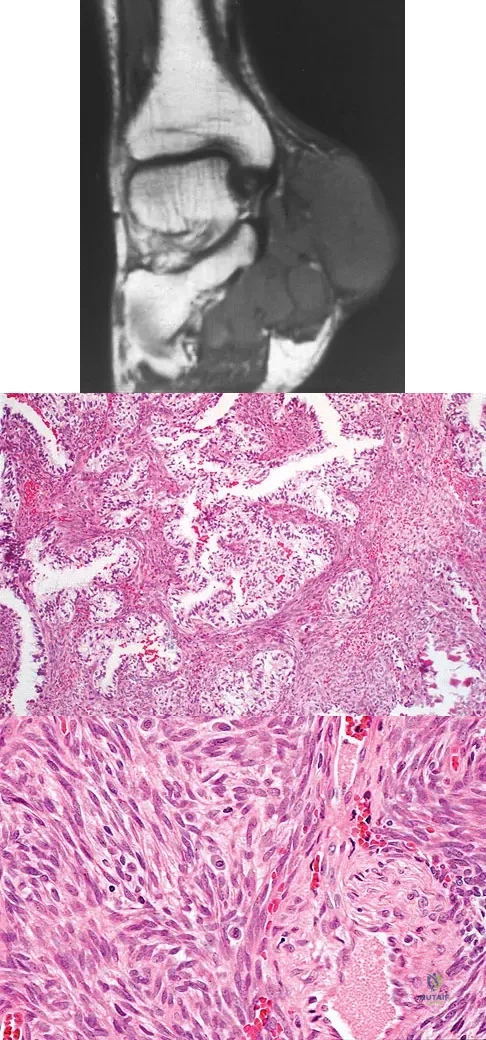
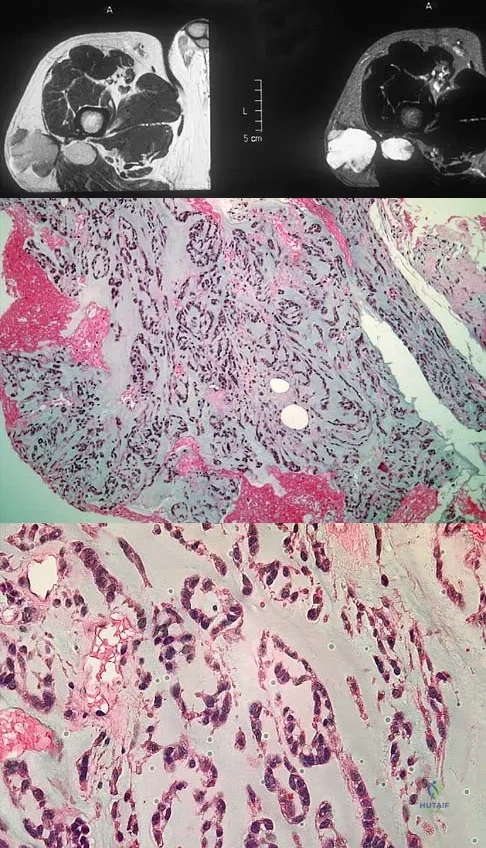
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?
Options:
- Epithelioid sarcoma
- Clear cell sarcoma
- Pigmented villonodular synovitis
- Malignant fibrous histiocytoma
- Synovial sarcoma
Correct Answer: Synovial sarcoma
Explanation:
The biopsy specimen is a low-power view of a soft-tissue sarcoma with a biphasic pattern of epithelial cells and fibrous spindle cells that are typical of a synovial sarcoma. A deep, painless soft-tissue mass greater than 5 cm in size is suspicious for a sarcoma. The imaging in this patient is indeterminate and the patient requires a biopsy for an accurate diagnosis. The biopsy reveals a tumor with a biphasic appearance consistent with a synovial sarcoma. These tumors are slow growing, occur primarily in the lower extremities, and are found in a younger demographic population compared to malignant fibrous histiocytoma and liposarcoma. They can occur in a biphasic pattern with clumps of epithelial cells and fibrous spindle cells or in a monophasic pattern. Synovial sarcomas stain positively for keratin. Keratin is positive in nearly all biphasic types and in many tumors of the monophasic fibrous type. Sixty percent of these tumors are found in the lower extremity. The area around the knee is the most common location, followed by the ankle and foot. Epithelioid and clear cell sarcomas are found associated with tendon sheaths of the hand and feet and are generally smaller in size. Epithelioid sarcoma may resemble granulomatous inflammation histologically; clear cell sarcoma is composed of nests of clear cells with occasional multinucleated giant cells. Pigmented villonodular synovitis is found within the synovium and is characterized by a villous histologic appearance with hemosiderin-laden macrophages. Malignant fibrous histiocytoma has a storiform histologic pattern with an abundance of pleomorphic cells. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 757.
References:
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 227.
Question 44:
Mutations of what gene are associated with the subsequent development of osteosarcoma?
Options:
- RB
- EWS-FLI1
- EGF-R
- IGF-R
- VEGF
Correct Answer: RB
Explanation:
Patients with a mutation of the retinoblastoma gene (RB) have an increased likelihood for the development of osteosarcoma. The EWS-FLI1 gene is the fusion product of a chromosomal translocation of 11:22. EGF-R and IGF-R are growth factor receptors, but mutations in these genes have not been correlated with osteosarcoma. VEGF is a proangiogenic molecule that is involved in tumor formation in multiple sites but not the development of osteosarcoma. Scholz RB, Kabisch H, Delling G, et al: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;7:265-273.
References:
Hansen MF, Koufos A, Gallie BL, et al: Osteosarcoma and retinoblastoma: A shared chromosomal mechanism revealing recessive predisposition. Proc Natl Acad Sci USA 1985;82:6216-6220.
Question 45:
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Options:
- Recurrent valgus overload (medial collateral ligament sprain)
- Posterior lateral rotatory instability
- Biceps tendinitis
- Medial epicondylitis
- Osteochondritis of the capitellum
Correct Answer: Osteochondritis of the capitellum
Explanation:
Osteochondritis of the capitellum is characterized by pain, swelling, and limited motion. Catching, clicking, and giving way also can occur. It commonly affects athletes who participate in competitive sports with high stresses, such as pitching or gymnastics. Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
References:
Schenck RC, Goodnight JM: Osteochondritis dissecans. J Bone Joint Surg Am 1996;3:439-456.
Question 46:
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Options:
- Flexor hallucis longus
- Flexor digitorum longus
- Peroneus longus
- Posterior tibial
- Quadratus planti
Correct Answer: Flexor hallucis longus
Explanation:
The flexor hallucis longus tendon provides the best, most direct route of transfer for filling Achilles tendon gaps. The tendon lies lateral to the neurovascular structures, making it safe for harvest and providing a direct route for transfer into the calcaneus without crossing these important structures. The flexor hallucis longus tendon also has muscle belly that extends distal on the tendon itself, often beyond the actual tibiotalar joint. When the tendon is transferred, this muscle belly brings excellent blood supply to the anterior portion of the reconstruction. Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
References:
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 47:
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Options:
- Determines the patient's ability to balance
- Determines hindfoot flexibility
- Determines forefoot flexibility
- Assesses the patient for Achilles tendon contractures
- Evaluates peroneus longus strength
Correct Answer: Determines hindfoot flexibility
Explanation:
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
References:
Thometz JG, Gould JS: Cavus deformity, in The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 48:
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
Options:
- Nonunion
- Deep infection
- Delayed wound healing
- Peroneal tendinitis
- Posttraumatic arthritis
Correct Answer: Delayed wound healing
Explanation:
Delayed wound healing and wound dehiscence is the most common complication of surgical management of calcaneal fractures through an extensile lateral approach, occurring in up to 25% of patients. Most wounds ultimately heal with local treatment; the deep infection rate is approximately 1% to 4% in closed fractures. Posttraumatic arthritis may develop despite open reduction and internal fixation, but the percentages remain low. Peroneal tendinitis may occur from adhesions within the tendon sheath or from prominent hardware but is relatively uncommon. Nonunion of a calcaneal fracture is rare. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
References:
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green's Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 49:
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Options:
- split-thickness skin graft.
- thenar flap.
- cross-finger flap.
- lateral arm flap.
- Moberg (volar advancement) flap.
Correct Answer: cross-finger flap.
Explanation:
The wound described indicates loss of soft tissue directly to the level of the tendon, precluding use of skin grafts if excursion of the tendon is desired. A cross-finger flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb. Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
References:
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 50:
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?
Options:
- Degenerative cyst with collapse
- Osteonecrosis
- Chondroblastoma
- Metastatic carcinoma
- Clear cell chondrosarcoma
Correct Answer: Osteonecrosis
Explanation:
Alcohol abuse, steroids, Caisson disease, sickle cell disease, and radiation therapy are the leading causes of nontraumatic osteonecrosis of the femoral head. Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
References:
Stulberg BN, Bauer TW, Belhobek GH, Levine M, Davis A: A diagnostic algorithm for osteonecrosis of the femoral head. Clin Orthop 1989;249:176-182.
Question 51:
Figure 23 shows failure of the femoral stem in a patient. What is the most likely reason for the failure?
Options:
- Torsional loading
- Cantilever bending
- Pistoning
- Subsidence
- Torque
Correct Answer: Cantilever bending
Explanation:
A two-dimensional stress analysis has been used to study the effects of some of the factors leading to early fatigue failure of the femoral stem in total hip arthroplasty. It has been demonstrated that loss of proximal stem support at the level of the calcar femorale and subsequent stem stress can lead to fatigue failure. In addition, the role of body weight and range of cyclic stress fluctuation play an important role in fatigue life under conditions where the stem has lost proximal support. These results indicate that stem design could be improved by incorporating some means of adequate support at the calcar femorale where maximum tensile stresses are found to occur. Femoral component fracture is a rare but well-documented complication after total hip arthroplasty. Historically, most stem fractures occur at the middle third of the implant where proximal stem loosening and solid distal stem fixation result in cantilever bending and eventual fatigue failure. The component shown is a modular fluted cementless stem that occasionally fractures at the modular junction in patients with poor proximal bone support. Andriacchi TP, Galante JO, Belytschko TB, et al: A stress analysis of the femoral stem in total hip prostheses. J Bone Joint Surg Am 1976;58:618-624.
References:
Gruen TA, McNeice GM, Amstutz HC: "Modes of failure" of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop 1979;141:17-27.
Question 52:
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Options:
- dural ectasia.
- Lisch nodules.
- juvenile xanthogranuloma.
- malignant peripheral nerve sheath tumor.
- plexiform neurofibroma.
Correct Answer: plexiform neurofibroma.
Explanation:
Plexiform neurofibromas are lesions found in patients with NF1. Clinical reports show the prevalence of plexiform neurofibroma to be 20% to 30% but increases to 40% when imaging studies are routinely obtained. The lesions are characterized by diffuse hypertrophy of the involved nerves but with preservation of the nerves' fascicular organization. The lesions may involve the dermis or may arise in the deeper structures. Palpation of a dermal lesion provokes an image of a "bag of worms." Plexiform neurofibromas may cause disfigurement and hyperpigmentation of the overlying skin. The lesions also can cause diffuse hypertrophy of the soft tissue and bone, with resultant changes ranging from a relatively minor limb-length discrepancy to gigantism of the entire extremity. Dural ectasia is frequently found in patients with NF1. Therefore, MRI should be obtained prior to planning spinal procedures in these patients; however, dural ectasia is not the cause of limb overgrowth. Lisch nodules are benign hamartomas of the iris. The lesions are uncommon during early childhood but are found in all adults with NF1. Juvenile xanthogranuloma has a low occurrence rate in patients with NF1; its presence is associated with juvenile chronic myeloid leukemia. Malignant peripheral nerve sheath tumors, formally called neurofibrosarcoma, result from malignant degeneration of a plexiform neurofibroma. This condition occurs in up to 4% of patients with NF1. Localized pain, an enlarging mass, or progressive neurologic symptoms suggest a malignant peripheral nerve sheath tumor in a patient with NF1. However, progressive neurologic symptoms also may occur with benign growth of a plexiform neurofibroma. Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
References:
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 53:
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?
Options:
- Ankle arthroscopy and lateral ligament reconstruction
- Tendon transfer, lateral column lengthening, and heel cord lengthening
- Ankle arthrodesis with retrograde intramedullary nail fixation
- Calcaneal osteotomy and transverse tarsal osteotomy
- Total ankle arthroplasty and deltoid ligament reefing
Correct Answer: Calcaneal osteotomy and transverse tarsal osteotomy
Explanation:
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
References:
Mäenpää H, Lehto MU, Belt EA: What went wrong in triple arthrodesis? An analysis of failures in 21 patients. Clin Orthop Relat Res 2001;391:218-223.
Question 54:
Figure 40 shows the radiographs of a 2-year-old boy who has a deformed leg. The patient is ambulatory and has no pain. What is the most appropriate management?
Options:
- Observation
- Patellar tendon bearing (PTB) orthosis
- Osteotomy to correct the deformity and fixation with an intramedullary rod
- Vascularized fibular graft from the contralateral leg
- Amputation
Correct Answer: Patellar tendon bearing (PTB) orthosis
Explanation:
The patient has a prefractured stage of congenital pseudarthrosis of the tibia and is at risk for fracture. The PTB orthosis may prevent or delay the fracture. Osteotomy is frequently complicated by nonunion. When established nonunion does not respond to intramedullary nailing and bone grafting, vascularized grafting may succeed. Amputation is a salvage procedure. Murray HH, Lovell WW: Congenital pseudarthrosis of the tibia: A long-term follow-up study. Clin Orthop 1982;166:14-20.
References:
Crossett LS, Beaty JH, Betz RR, et al: Congenital pseudarthrosis of the tibia: Long-term follow-up study. Clin Orthop 1989;245:16-18.
Question 55:
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Options:
- Closed reduction and bracing
- Retrograde femoral intramedullary nailing
- Open reduction and internal fixation of the fracture, leaving the femoral stem in place
- Open reduction and internal fixation of the fracture and insertion of a proximally porous-coated stem
- Open reduction and internal fixation of fracture fragments and insertion of a fully porous-coated femoral stem with diaphyseal fixation distal to the fracture
Correct Answer: Open reduction and internal fixation of the fracture, leaving the femoral stem in place
Explanation:
The patient has a periprosthetic fracture below the femoral stem. The component is porous coated and well fixed. Open reduction and internal fixation, leaving the stem in place, can be performed when bone quality is good. Plating with or without allograft struts and supplemental cerclage fixation generally is acceptable. If the component is loose, revision to a longer device is recommended with appropriate stabilization of the fracture using the aforementioned methods. If bone loss has occurred, allograft supplementation or a tumor prosthesis may be indicated. Fractures located well below the stem tip can be treated without regard for the prosthesis. Closed reduction and bracing is not associated with good results for periprosthetic femoral fractures. Retrograde intramedullary nailing is not appropriate for this fracture. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
References:
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 56:
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?
Options:
- Nonunion
- Malunion
- Infection
- Knee pain
- Compartment syndrome
Correct Answer: Knee pain
Explanation:
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
References:
Keating JF, Orfaly R, O'Brien PJ: Knee pain after tibial nailing. J Orthop Trauma 1997;11:10-13.
Question 57:
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Options:
- Mobile-bearing knee
- Posterior cruciate ligament-sparing knee
- Posterior cruciate ligament-substituting knee
- Semiconstrained-style knee
- Triaxial hinged knee
Correct Answer: Posterior cruciate ligament-substituting knee
Explanation:
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
References:
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 58:
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Options:
- surgical exploration and tendon reinsertion of the flexor digitorum profundis.
- surgical exploration and tendon reinsertion of the flexor digitorum superficialis.
- steroids and physical therapy.
- surgical release of the anterior interosseous nerve.
- surgical release of the median nerve.
Correct Answer: surgical exploration and tendon reinsertion of the flexor digitorum profundis.
Explanation:
The patient has an avulsion of the flexor digitorum profundus. Treatment should include surgical exploration and tendon reinsertion. This is not an avulsion of the flexor digitorum superficialis because the patient's deficiency is the inability to flex the distal interphalangeal joint, not the proximal interphalangeal joint. Surgical release of the anterior interosseous nerve is not indicated because the flexor digitorum profundus of the ring finger is innervated by the ulnar nerve. A median nerve contusion causes wrist pain and/or numbness and tingling in the median nerve distribution. Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 1851-1897.
References:
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 59:
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Options:
- Warfarin with a targeted international normalized ratio (INR) of 2.0 to 3.0 for 10 to 14 days
- Low-molecular-weight heparin used for at least 3 days
- Pneumatic compression sleeves used while the patient is in the hospital
- Fondaparinux used for 5 to 7 days
- Aspirin for 4 weeks
Correct Answer: Warfarin with a targeted international normalized ratio (INR) of 2.0 to 3.0 for 10 to 14 days
Explanation:
In the 2004 ACCP guidelines, there were three prophylactic regimens that received a grade 1A favorable recommendation. These included low-molecular-weight heparin, warfarin, or fondaparinux, as long as they are used for at least 10 days. If warfarin is used, the target INR should be 2.0 to 3.0, according to the guidelines. Pneumatic compression sleeves have gained popularity in the orthopaedic community but have not received a grade 1A rating from the ACCP at this time. Use of aspirin by itself is discouraged by the ACCP.
References:
Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: The seventh ACCP Conference on antithrombotic and thrombolytic therapy. Chest 2004;126:338S-400S.
Question 60:
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm3. The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Options:
- Arthrotomy, debridement, and polyethylene exchange
- One-stage exchange arthroplasty
- Two-stage exchange arthroplasty
- Parenteral antibiotics
- Nonsurgical management without antibiotics
Correct Answer: Nonsurgical management without antibiotics
Explanation:
Synovial fluid analysis is a very sensitive tool for detecting infection in total knee arthroplasties. Several studies have demonstrated that an absolute leukocyte count in the synovial fluid of less than 1,700 to 2,500/mm3 is an accurate predictor of absence of infection. Similarly, a differential cell count of the WBCs demonstrating less than 50% to 60% neutrophils is an accurate predictor of absence of infection. If both parameters are normal, it is unlikely that the patient has an infection. The three surgical options are contraindicated based on the normal examination findings and laboratory parameters. Similarly, antibiotics should be avoided. The work-up should include tests to evaluate noninfectious sources of knee pain and sources of referred knee pain. Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562. Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
References:
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 61:
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Options:
- Median nerve lesion in the arm
- Radial nerve lesion in the arm
- Anterior interosseous nerve syndrome
- Posterior interosseous nerve syndrome
- Median neuropathy at the wrist
Correct Answer: Median nerve lesion in the arm
Explanation:
The clinical presentation is characteristic of a high median nerve palsy. When trying to make a fist, the patient is unable to flex the thumb and index fingers due to paralysis of flexion of the distal interphalangeal joint of the thumb and the distal and proximal interphalangel joints of the index finger. This hand attitude differs from the anterior interosseous nerve lesion in which loss of distal interphalangeal joint flexion is seen in the thumb, index, and middle fingers. Posterior interosseous nerve syndrome presents with dropped fingers at the metacarpophalangeal joints with wrist extension in radial deviation. Wrist and finger drop is the typical posture of patients with radial nerve lesions.
References:
Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 189.
Question 62:
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Options:
- splinting and injections for carpal tunnel syndrome.
- scaphoid excision and four-bone fusion.
- proximal row carpectomy via dorsal and volar incisions.
- MRI of the wrist.
- carpal tunnel release.
Correct Answer: proximal row carpectomy via dorsal and volar incisions.
Explanation:
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
References:
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 63:
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Options:
- closed reduction and cast immobilization.
- closed reduction and percutaneous pinning.
- open reduction and fixation using an absorbable suture.
- open reduction and fixation using two Kirschner wires and a figure-of-8 tension band of absorbable suture.
- open reduction and fixation using an intramedullary screw.
Correct Answer: open reduction and fixation using two Kirschner wires and a figure-of-8 tension band of absorbable suture.
Explanation:
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
References:
Dormans JP, Rang M: Fractures of the olecranon and radial neck in children. Orthop Clin North Am 1990;21:257-268.
Question 64:
What is the main function of collagen found within articular cartilage?
Options:
- Compressive properties
- Tensile properties
- Proteoglycan synthesis
- Cartilage metabolism
- Joint lubrication
Correct Answer: Tensile properties
Explanation:
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
References:
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 65:
A Canale view best visualizes which of the following structures?
Options:
- Posterior facet of the subtalar joint
- Lisfranc joint
- Talar neck
- Sustentaculum tali
- Lateral column of the foot
Correct Answer: Talar neck
Explanation:
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
References:
Bruden B: Roentgen examination of the subtaloid joint in fractures of the calcaneus. Acta Radiol 1949;31:85-91.
Question 66:
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of
Options:
- CT of the chest.
- a bone scan.
- a repeat radiograph in 6 to 8 weeks.
- repeat MRI in 6 to 8 weeks.
- an open biopsy.
Correct Answer: a repeat radiograph in 6 to 8 weeks.
Explanation:
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
References:
Wang SY, Lomasney LM, Demos TC, Hopkinson WJ: Radiologic case study: Traumatic myositis ossificans. Orthopedics 1999;22:991-995, 1000.
Question 67:
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Options:
- Observation
- Medical management
- Needle biopsy
- Incisional biopsy
- Resection
Correct Answer: Observation
Explanation:
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
References:
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 68:
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?
Options:
- Femoral head articular defect
- Acetabular articular defect
- Haversian fat pad hypertrophy
- Labral tear
- Loose body
Correct Answer: Labral tear
Explanation:
The motorized shaver is adjacent to the acetabular labrum, which is torn. The femoral head and acetabulum are normal in appearance. Neither the fat pad nor a loose body is identified.
References:
Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 93-104.
Question 69:
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Options:
- Deep to the arcuate ligament
- Closer to bone in larger legs
- On the muscle belly of the popliteus
- On the bony posterolateral corner of the tibia
- Superficial to the lateral head of the gastrocnemius
Correct Answer: Superficial to the lateral head of the gastrocnemius
Explanation:
At the level of tibial bone resection in total knee arthroplasty, the common peroneal nerve lies superficial to the lateral head of the gastrocnemius and is therefore protected by this structure. In an MRI study of 60 knees, the mean distance from the bony posterolateral corner of the tibia to the nerve was 1.49 cm, with no distance less than 0.9 cm. The distance from the bone to nerve was greater in larger legs. Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the "pie crust" technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
References:
Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-52, 4-53.
Question 70:
In the most common condition causing a winged scapula, which of the following nerves is affected?
Options:
- Long thoracic nerve
- Spinal accessory nerve
- Suprascapular nerve
- Dorsal scapular nerve
- Thoracodorsal nerve
Correct Answer: Long thoracic nerve
Explanation:
A winged scapula is most often associated with Parsonage-Turner syndrome, a condition thought to be due to an inflammatory or immune-mediated mechanism. Certain muscles are predisposed, particularly the serratus anterior muscle innervated by the long thoracic nerve. Other less common nerve lesions (eg, the spinal accessory and dorsal scapular nerves) may also cause winged scapulae. Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995.
References:
van Alfen N, van Engelen BG: The clinical spectrum of neuralgic amyotrophy in 246 cases. Brain 2006;129:438-450.
Question 71:
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Options:
- shoulder exercises, mild analgesics, and activity modification.
- transfer of the latissimus dorsi to the greater tuberosity.
- arthroscopy and debridement of the tendon edges.
- arthroscopy, arthroscopic acromioplasty, coracoacromial ligament release, and mini open repair.
- arthroscopy, arthrotomy, acromioplasty, and primary repair of the rotator cuff.
Correct Answer: shoulder exercises, mild analgesics, and activity modification.
Explanation:
The MRI scan shows a massive tear of the supraspinatus tendon with medial retraction to the level of the glenoid. This is most likely an attritional tear with a high risk of failure of the repair. The preferred treatment is nonsurgical management for pain and stiffness. Acromioplasty and coracoacromial ligament release in this setting are controversial, as they can result in the devastating complication of anterosuperior subluxation of the humerus. Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
References:
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 299-312.
Question 72:
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Options:
- Fibrous tissue
- Bone
- Articular cartilage
- Fibrocartilage
- Type II collagen
Correct Answer: Fibrocartilage
Explanation:
Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
References:
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 73:
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Options:
- Osteolysis because of polyethylene debris
- Spot weld
- Osteosclerotic pedestal
- Cement fragmentation
- Allergic reaction to titanium
Correct Answer: Osteolysis because of polyethylene debris
Explanation:
Osteolysis of an otherwise well-functioning total hip arthroplasty is a recognized complication, and its radiographic appearance is typical, as shown here. Distal osteolysis, such as that shown here, is more prevalent when there is noncircumferential sealing of the proximal femoral canal. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
References:
Engh CA, Massin P, Suthers KF: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Question 74:
An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?
Options:
- Simple bone cyst
- Nonossifying fibroma
- Osteomyelitis
- Aneurysmal bone cyst
- Giant cell tumor
Correct Answer: Aneurysmal bone cyst
Explanation:
The radiograph shows an osteolytic eccentric lesion in the metaphyseal-diaphyseal region of the bone, and the photomicrographs show an aneurysmal bone cyst. The low-power photomicrograph shows large empty spaces with fibrous stroma and multinucleated giant cells. The red area in the center is hemorrhage in the stroma. The large empty spaces are cysts, which would be filled with blood in vivo. The medium-power photomicrograph shows a large cyst-like space and hemorrhage in the surrounding stoma. Giant cell tumors have "sheets" of giant cells. A nonossifying fibroma would have spindle cells, and a unicameral bone cyst may have a few giant cells, but blood is rare. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 540-542.
References:
Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1906-1909.
Question 75:
Thoracic disk herniations are most frequently found in what area of the spine?
Options:
- C7-T2
- T2-T5
- T5-T8
- T9-T12
- T12-L1
Correct Answer: T9-T12
Explanation:
Although thoracic disk herniations have been reported at all levels of the thoracic spine, more than two thirds are found at T9-T12, which is the more mobile lower third of the thoracic region. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
References:
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 76:
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?
Options:
- 0% to 10%
- 20% to 30%
- 40% to 50%
- 60% to 70%
- 80% to 90%
Correct Answer: 40% to 50%
Explanation:
The knee is the most common location of spontaneous bleeding in children with hemophilia. Treatment generally requires replacement to 40% to 50% of normal. For surgery, the replacement should be to 100%. The plasma level generally rises 2% for every unit (per kg body weight) of factor VIII administered. Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
References:
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 235.
Question 77:
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Options:
- closed reduction of the ulna and transcapitellar pinning of the radial head.
- closed reduction of the ulna and radial head dislocation.
- closed reduction of the ulna and annular ligament repair.
- open reduction of the radius and plating of the ulna.
- open reduction of the ulna and immobilization in an extension cast.
Correct Answer: closed reduction of the ulna and radial head dislocation.
Explanation:
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
References:
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 78:
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
Options:
- normal sexual function and normal vaginal childbirth.
- sexual dysfunction (dyspareunia) and normal vaginal childbirth.
- normal sexual function and caesarean section childbirth.
- sexual dysfunction (dyspareunia) and caesarean section childbirth.
- normal sexual function and caesarean section childbirth until hardware removal.
Correct Answer: sexual dysfunction (dyspareunia) and caesarean section childbirth.
Explanation:
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not. Copeland CE, Bosse MJ, McCarthy ML et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
References:
Wright JL, Nathans AB, Rivara FP, et al: Specific fracture configurations predict sexual and excretory dysfunction in men and women 1 year after pelvic fracture. J Urol 2006;176:1540-1545.
Question 79:
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T2-weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Options:
- Chemotherapy and radiation therapy
- Neoadjuvant chemotherapy followed by wide resection and reconstruction
- Curettage and bone grafting
- Curettage and intravenous antibiotics
- Above-knee amputation
Correct Answer: Neoadjuvant chemotherapy followed by wide resection and reconstruction
Explanation:
The radiographs show a lytic lesion in the right proximal tibia that has a high fluid content based on the MRI findings. The radiographic appearance is consistent with either telangiectatic osteosarcoma or aneurysmal bone cyst. Low-magnification histology shows a lesion resembling an aneurysmal bone cyst, with blood lakes separated by cellular septa. However, high-magnification shows severe cytologic atypia, indicative of a telangiectatic osterosarcoma. The appropriate treatment is neoadjuvant chemotherapy followed by wide resection and reconstruction of the lesion. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 80:
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Options:
- application of a Pavlik harness.
- botulinum toxin A injections to the adductor and iliopsoas muscles.
- bilateral release of the adductor and iliopsoas muscles.
- bilateral soft-tissue release and proximal femoral varus rotational osteotomies.
- selective dorsal rhizotomy.
Correct Answer: bilateral release of the adductor and iliopsoas muscles.
Explanation:
Progressive hip subluxation occurs in up to 50% of children with spastic quadriparesis. The subluxation is the result of chronic muscle hypertonicity, especially in the adductor muscle group. In time, the constant muscle tension will lead to dislocation, dysplastic changes in the acetabulum, and erosive changes in the cartilage of the femoral head. Many of these children will experience pain. Two recent studies have shown that early soft-tissue releases can successfully prevent progressive subluxation in children who are younger than age 4 years and who have a Reimers index (migration index) of less than 40%. Botulinum toxin A injections may reduce tone in the adductors for 4 to 6 months, but it is difficult to inject into the iliopsoas. Additionally, there are no long-term studies documenting the efficacy of botulinum toxin A to treat progressive hip subluxation in patients who have spastic quadriparesis. In general, proximal femoral osteotomy, combined with soft-tissue release as necessary, is indicated in older children (older than age 4 years) with progressive subluxation. Although selective dorsal rhizotomy has been used in nonambulatory patients, outcomes are less well documented than in ambulatory patients. There are no studies documenting the effect of selective dorsal rhizotomy on progressive hip subluxation in nonambulatory children. Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
References:
Cornell MS, Hatrick NC, Boyd R, et al: The hip in children with cerebral palsy: Predicting the outcome of soft tissue surgery. Clin Orthop 1997;340:165-171.
Question 81:
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Options:
- Baker's cyst
- Torn medial meniscus
- Patellofemoral pain syndrome
- Lipoma
- Ganglion cyst of the cruciates
Correct Answer: Ganglion cyst of the cruciates
Explanation:
Ganglia involving the cruciate ligaments have been recently reported as a cause of knee pain that interferes with knee flexion and extension. The symptoms are poorly localized in this patient and not along the medial joint line, making the diagnosis of a torn medial meniscus less likely. In addition, the MRI findings do not show a significant medial meniscal lesion. A Baker's cyst is usually posteromedial and extends posterior to the interval between the medial head of the gastrocnemius and semimembranosus. MRI scans show a fluid-filled lesion with an increased signal on T1- and T2-weighted images. A lipoma would be bright on the T1-weighted image only. Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
References:
Brown MF, Dandy DJ: Intra-articular ganglia of the knee. Arthroscopy 1990;6:322-323.
Question 82:
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Options:
- Extraskeletal myxoid chondrosarcoma
- Rhabdomyosarcoma
- Malignant fibrous histiocytoma
- Myxoma
- Liposarcoma
Correct Answer: Extraskeletal myxoid chondrosarcoma
Explanation:
The histology shows extraskeletal myxoid chondrosarcoma, characterized by abundant blue myxoid matrix with cords and nests of small tumor cells. Treatment consists of wide resection. Despite the name, hyaline cartilage is not a common component of these tumors. Adult rhabdomyosarcoma and malignant fibrous histiocytoma are highly pleomorphic sarcomas often containing multinucleated giant cells. Myxoid liposarcoma contains a prominent capillary network and lipoblasts. Myxoma is less cellular than extraskeletal myxoid chondrosarcoma and does not have a cord-like arrangement of tumor cells.
References:
Kawaguchi S, Wada T, Nagoya S, Ikeda T, Isu K, Yamashiro K, et al: Extraskeletal myxoid chondrosarcoma. Cancer 2003;97:1285-1292.
Question 83:
What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
Options:
- Saphenous nerve
- First branch of the lateral plantar nerve
- Superficial peroneal nerve
- Sural nerve
- Deep peroneal nerve
Correct Answer: Sural nerve
Explanation:
The sural nerve and its terminal branches course through the lateral hindfoot and midfoot area and are directly at risk in surgeries involving the peroneal tendon complex and the fifth metatarsal. The first branch of the lateral plantar nerve originates in the tarsal tunnel region and courses across the plantar heel area to innervate the abductor digiti minimi; it is not at direct risk with fifth metatarsal surgery. The saphenous, superficial peroneal, and deep peroneal nerves are not at risk anatomically with a lateral midfoot incision. Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
References:
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 84:
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to
Options:
- a physeal scar.
- a femoral stress fracture.
- a normal growth plate.
- Looser's line.
- an abnormal growth plate.
Correct Answer: a physeal scar.
Explanation:
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
References:
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 85:
A patient with a left-sided C6-7 herniated nucleous pulposis would likely have which of the following constellation of findings?
Options:
- Pain into the thumb, triceps weakness, and loss of triceps reflex
- Middle finger numbness, wrist extensor weakness, diminished brachioradialis reflex
- Thumb numbness, wrist extensor weakness, diminished brachioradialis reflex
- Middle finger numbness, triceps weakness, and loss of biceps reflex
- Middle finger numbness, triceps weakness, and loss of triceps reflex
Correct Answer: Middle finger numbness, triceps weakness, and loss of triceps reflex
Explanation:
A C6-7 herniation affects the C7 root. The C7 root has the middle finger as its predominant sensory distribution. Its motor function is the triceps, wrist extension, and finger metacarpophalangeal extension. The reflex is the triceps. Magee D: Principles and concepts, in Orthopedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
References:
An H: History and physical examination of the spine, in Principles and Techniques of Spine Surgery. Baltimore, MD, Lippincott Williams & Wilkins, 1998, pp 91-101.
Question 86:
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on
Options:
- bone scan results returning to normal.
- a decline in intensity on serial bone scans.
- the serum levels of alkaline phosphatase measured over time.
- the level of serum calcium-phosphorus product.
- the time since injury and evidence of bone maturation on plain radiographs.
Correct Answer: the time since injury and evidence of bone maturation on plain radiographs.
Explanation:
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
References:
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 325-335.
Question 87:
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?
Options:
- Intraosseous pressures
- AP and frog-lateral radiographs
- Technetium Tc 99m bone scan
- MRI scan
- CT scan
Correct Answer: MRI scan
Explanation:
An MRI scan is both highly sensitive and specific for the evaluation of osteonecrosis. The measurement of increased intraosseous pressure can be technically difficult and the results have been variable. Plain radiographs can be normal early in the progression of osteonecrosis of the femoral head. The technetium Tc 99m bone scan is a very sensitive test. However, it is not specific; increased uptake can be noted in patients with arthritis, neoplastic disease, fracture, or sepsis. In addition, because of bilaterality, the frequency of false-negative scans is relatively high. Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
References:
Glickstein MF, Burk DL Jr, Schiebler ML, et al: Avascular necrosis versus other diseases of the hip: Sensitivity of MR imaging. Radiology 1988;169:213-215.
Question 88:
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Options:
- aspiration and steroid injection.
- rest.
- acromioplasty.
- arthroscopic repair and decompression.
- rehabilitation.
Correct Answer: arthroscopic repair and decompression.
Explanation:
The MRI scans reveal a large posterior paralabral cyst associated with a posterior-superior labral tear. The cyst appears as a well-defined, smoothly marginated mass with low signal intensity on T1-weighted MRI scans and with high signal intensity on T2-weighted MRI scans. MRI also reveals changes in the supraspinatus and infraspinatus muscles secondary to denervation, including decreased muscle bulk and fatty infiltration. MRI has the added advantage, compared with other imaging modalities, of detecting intra-articular lesions, such as labral tears, which are frequently associated with ganglion cysts of the shoulder. In this case of a professional baseball player with a space-occupying lesion causing nerve compression with an associated labral tear, the treatment of choice is arthroscopic decompression of the cyst and repair of the tear. Acromioplasty would not address the primary pathology in this patient. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Scientific References
:
Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 89:
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Options:
- decreased risk of heterotopic ossification.
- higher hip pain score.
- lower level of functional return.
- comparable infection rate.
- comparable level of blood loss.
Correct Answer: lower level of functional return.
Explanation:
Joshi and associates reported a 96% incidence of pain relief in 181 total hip arthroplasties in patients with ankylosing spondylitis. Only 65% of patients had good to excellent functional results, primarily the result of associated systemic diseases and spinal deformity. The incidence of infection was slightly higher, and the incidence of heterotopic ossification was higher in this group of patients.
References:
Joshi A, Markovic L, Hardinge K, Murphy J: Total hip arthroplasty in ankylosing spondylitis: An analysis of 181 hips. J Arthroplasty 2002;17:427-433.
Question 90:
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Options:
- Absence of acetabular protrusio
- Presence of posterior column
- Presence of anterior column
- Presence of at least 50% host bone
- Presence of a segmental defect
Correct Answer: Presence of at least 50% host bone
Explanation:
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
References:
Gross AE, Allan DG, Catre M, et al: Bone grafts in hip replacement surgery: The pelvic side. Orthop Clin North Am 1993;24:679-695.
Question 91:
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Options:
- immediate casting with the expectation of a satisfactory correction.
- immediate casting with the expectation that surgical correction will be needed.
- immediate surgery to correct the deformity.
- delayed casting and corrective bracing.
- therapeutic and frequent physical therapy to stretch the soft tissues and observe the skin.
Correct Answer: immediate casting with the expectation that surgical correction will be needed.
Explanation:
In a child with myelomeningocele, the guiding principle of treatment is to achieve a plantigrade foot by the time the child is ready to stand. The standard clubfoot protocol should be followed, but these children will require an aggressive surgical release to obtain a sufficient correction. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
References:
Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 503-514.
Question 92:
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Options:
- Arthroscopy
- MRI scan
- Stress radiographs
- Tomogram
- Arthrogram
Correct Answer: Stress radiographs
Explanation:
In the skeletally mature individual, this mechanism of injury will often result in a sprain of the medial collateral ligament. In skeletally immature patients, the same mechanism can cause a fracture of the distal femoral physis. If the fracture is nondisplaced, the plain radiographs may show only soft-tissue swelling or effusion. While the MRI scan may show edema in the soft tissues on the medial side of the knee and even an abnormality of the physis, stress radiographs provide a quicker and less expensive means of making the diagnosis. Arthroscopy and arthrography would not be helpful in making the diagnosis. Arthroscopy may result in further displacement of the injury. Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
References:
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 93:
Which of the following benign bone lesions can develop lung metastases?
Options:
- Chondroblastoma
- Chondromyxoid fibroma
- Fibrous dysplasia
- Aneurysmal bone cyst
- Desmoplastic fibroma
Correct Answer: Chondroblastoma
Explanation:
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
References:
Bloem JL, Mulder JD: Chondroblastoma: A clinical and radiological study of 104 cases. Skeletal Radiol 1985;14:1-9.
Question 94:
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
Options:
- Sacral fracture through the foramen
- Sacral fracture through the ala
- Sacroiliac joint dislocation
- Reverse fracture-dislocation of the sacroiliac joint through the ilium
- Iliac wing fracture
Correct Answer: Sacroiliac joint dislocation
Explanation:
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
References:
Henderson RC: The long-term results of nonoperatively treated major pelvic disruptions. J Orthop Trauma 1989;3:41-47.
Question 95:
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by
Options:
- weight.
- gender.
- the knee compartment involved.
- open or closed growth plates.
- limb alignment.
Correct Answer: open or closed growth plates.
Explanation:
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
References:
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 96:
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Options:
- Broad-spectrum parenteral antibiotics
- Repeat aspirations
- Irrigation and debridement
- Hyperbaric oxygen
- Resection of the sternoclavicular joint
Correct Answer: Resection of the sternoclavicular joint
Explanation:
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
References:
Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 97:
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?
Options:
- Visualization of the articular surface
- Avoidance of an olecranon osteotomy
- A muscle-sparing approach
- The likelihood a total elbow arthroplasty will be performed
- The likelihood that reconstruction of the anterior elbow joint will be performed
Correct Answer: Visualization of the articular surface
Explanation:
When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures. McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522 McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707. Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop 2000;370:19-33.
References:
Bryan RS, Morrey BF: Extensive posterior exposure of the elbow: A triceps-sparing approach. Clin Orthop 1982;166:188-192.
Question 98:
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Options:
- 0.01 to 0.05 mm/yr
- 0.1 to 0.2 mm/yr
- 0.5 to 1 mm/yr
- 1 to 2 mm/yr
- Greater than 2 mm/yr
Correct Answer: 0.1 to 0.2 mm/yr
Explanation:
Several studies have shown that ultra-high molecular weight polyethylene liners used in total hip arthroplasties wear at a rate of 0.1 to 0.2 mm/yr. The orthopaedic surgeon performing total hip arthroplasties should be aware of the average wear rate so that potential problems can be identified when following patients postoperatively. Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC: Charnley total hip arthroplasty with cement: Minimum twenty-five year follow-up. J Bone Joint Surg Am 2000;82:487-497.
References:
Isaac GH, Wroblewski BM, Atkinson JR, Dowson D: A tribological study of retrieved hip prostheses. Clin Orthop 1992;276:115-125.
Question 99:
The primary function of structure "A" in Figure 29 is to limit
Options:
- posterior tibial displacement at 90 degrees of flexion.
- varus knee laxity at 30 degrees of flexion.
- varus knee laxity at 0 degrees of flexion.
- anterolateral rotation of the tibia on the femur.
- posterolateral rotation of the tibia on the femur.
Correct Answer: posterolateral rotation of the tibia on the femur.
Explanation:
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur. Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
References:
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 100:
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Options:
- anterior diskectomy and fusion at C4-C5.
- immobilization in a Philadelphia collar and voluntary flexion and extension radiographs when awake.
- occipital-cervical fusion with instrumentation.
- halo immobilization for 12 weeks.
- left C6 superior facetectomy and posterior fusion at C6-C7 with instrumentation.
Correct Answer: occipital-cervical fusion with instrumentation.
Explanation:
The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7. Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
References:
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.