High-Yield Orthopedic Surgery MCQs: ABOS, OITE, FRCS Practice Exam Set #225 (100 Questions)

Key Takeaway
This page provides 100 high-yield Orthopedic Surgery MCQs for ABOS, OITE, and FRCS board exam preparation. Surgeons can use this practice test (Set 225) to reinforce knowledge, identify study areas, and master key concepts essential for board certification success.
Medial Hip Approach & Obturator Division: Ana...
00:00
Start Quiz
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
- Rencken ML, Chesnut CH III, Drinkwater BL: Bone density at multiple skeletal sites in amenorrheic athletes. JAMA 1996;276:238-240.
Question 3High Yield
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
The rhomboideus major and minor muscles are innervated by the dorsal scapular nerve, which is supplied entirely by the C5 nerve root. The dorsal scapular nerve arises just distal to the dorsal root ganglion of the C5 nerve root. A functioning rhomboid muscle indicates that an injury involving C5 nerve root fibers must be postganglionic or distal to the C5 dorsal root ganglion. Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Question 4High Yield
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Question 5High Yield
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?
Explanation
The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid. Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 6High Yield
Dislocation following primary total hip arthroplasty is more likely to occur in which of the following situations?
Explanation
Explanation
Dislocation following total hip arthroplasty is twice as common in women than in men. It is more likely to occur in older patients. There is no clear association between dislocation and the method of fixation or the type of bearing, so long as the bearing diameter is the same.
References:
- Berry DJ: Dislocation, in Steinberg ME (ed): Revision Total Hip Arthroplasty. Philadelphia, PA, 1999, pp 463-482.
Question 7High Yield
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 8High Yield
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
Explanation
Explanation
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction. Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.
Question 9High Yield
A 14-year-old boy undergoes application of a circular frame with tibial and fibular osteotomy for gradual limb lengthening. He initiates lengthening 7 days after surgery. During the first week of lengthening, he reports that turning of the distraction devices is becoming increasingly difficult. On the 9th day of lengthening, he is seen in the emergency department after feeling a pop in his leg and noting the acute onset of severe pain. What complication has most likely occurred?

Explanation
Incomplete corticotomy may result from osteotomy with limited soft-tissue stripping and exposure. When the patient begins distraction, tension develops at all wire/half-pin and bone interfaces, leading to increasing difficulty in distraction and limb pain. Sudden spontaneous completion of the osteotomy with continued tension applied by the fixator results in acute distraction of the osteotomy with severe pain. Premature consolidation is unlikely this early following the initial surgery. Birch JG, Samchukov ML: Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J Am Acad Orthop Surg 2004;12:144-154.
Question 10High Yield
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 11High Yield
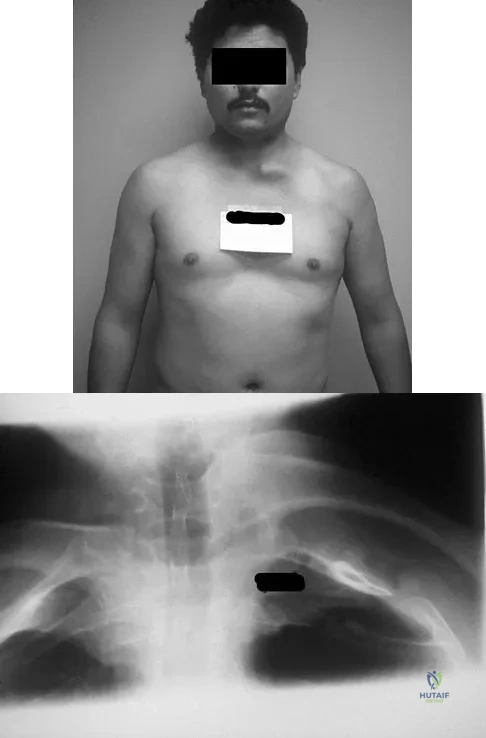
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
The patient sustained an injury to the long thoracic nerve, which supplies the serratus anterior. Branches of C5 and C6 enter the scalenus medius, unite in the muscle, and emerge as a single trunk and pass down the axilla. On the surface of the serratus anterior, the long thoracic nerve is joined by the branch from C7 and descends in front of the serratus anterior, providing segmental innervation to the serratus anterior.
Question 12High Yield
In patients with neurofibromatosis, what is the most important sign of impending rapid progression of a spinal deformity?
Explanation
Neurofibromatosis can progress very rapidly. Rib penciling is the only singular prognostic factor. Significant progression has been observed in 87% of the curves with three or more penciled ribs. The other factors are often present but do not have a high correlation with rapid, severe progression. Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Question 13High Yield
Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?

Explanation
Although all of these factors may influence the decision to perform surgery, the most important is the position of the talus in the mortise. The goal of treatment of ankle fractures is to maintain the talus centered in the mortise. If it is in this position, the other factors do not enter into the decision to intervene surgically. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Question 14High Yield
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
Explanation
The union rate for minimally displaced midthird scaphoid fractures is quite high with cast immobilization while allowing a return to sports. Inadequate immobilization results in a much higher nonunion rate. Early fixation and rehabilitation have been proposed for sports or positions that are not amenable to cast immobilization. While immobilization of a nondisplaced fracture results in an acceptably high union rate, there is no advantage to fixation in conjunction with immobilization in the course of healing. With adequate immobilization and protection, play restrictions until healing has occurred are unnecessary. Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186. Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
References:
- Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 15High Yield
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
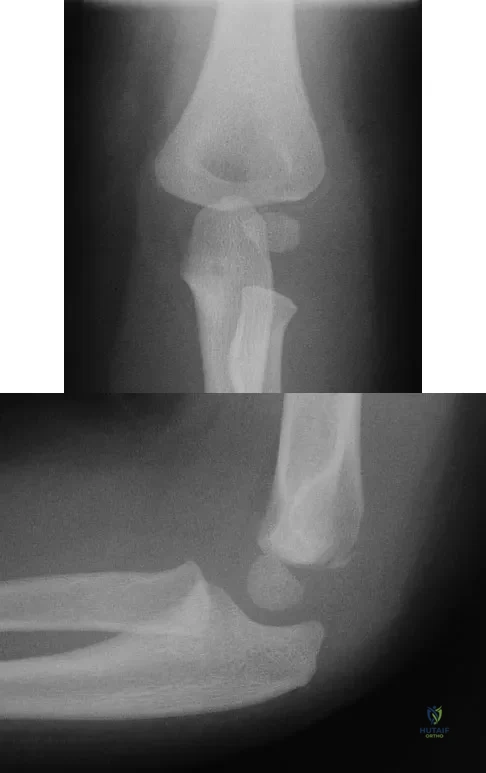
Explanation
The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically. Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Question 16High Yield
Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the exception of an erythrocyte sedimentation rate (ESR) of 90 mm/h. What is the next most appropriate step in management?
Explanation
Explanation
The patient's history, including the timing and type of symptoms, is typical for postoperative diskitis. The elevated ESR, 5 weeks after surgery, is also consistent with infection; a normal WBC count is not unusual. Management should consist of MRI with gadolinium; if positive, this should be followed by percutaneous biopsy to confirm the organism. Open biopsy may be considered if the percutaneous biopsy is unsuccessful. Anterior debridement and interbody fusion is reserved for the occasional patient that fails to respond to intravenous antibiotics, bed rest, and immobilization. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
References:
- Beatty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 17High Yield
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea. Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
References:
- Drinkwater BL: Exercise and bones: Lessons learned from female athletes. Am J Sports Med 1996;24:S33-S35.
Question 18High Yield
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?

Explanation
The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Question 19High Yield
A 14-year-old girl with a right thoracic curve from T4 through L2 measuring 78 degrees is scheduled to undergo posterior spinal fusion for scoliosis. The surgical plan is to fuse from T3 through L2, using pedicle screws at L2 and about the apex at T8. What neural monitoring modality is most likely to identify a reversible neurologic deficit during surgery?
Explanation
Explanation
Neural monitoring during scoliosis surgery was initially developed to avoid the devastating effects of spinal cord injury, particularly paraplegia. Monitoring in some form has become standard for this type of surgery. Somatosensory-evoked potentials in the lower extremities will detect many but not all neurologic difficulties with the spinal cord. Anterior spinal cord vascular disruption also can be detected by monitoring motor potentials. Electromyography following stimulation of lumbar pedicle screws can prevent nerve root injury that is the result of misplacement of the screws. This is best documented in the lumbar spine and has not been routinely used in the thoracic spine. The most common neural deficits following spinal surgery, however, are in the upper extremities because of the positioning of the patient in the prone position for long periods. In Schwartz and associates series of 500 patients, impending upper extremity neural injury was detected by somatosensory-evoked potentials in 18 (3.6%) patients. In contrast, lower extremity deficits were detected by combined motor- and sensory-evoked potentials in only 2 (0.4%) out of 500 patients in Padberg and associates series. Neural compression in the upper extremity can be easily detected by somatosensory-evoked potentials, and injury can be prevented by repositioning the patient. Padberg AM, Wilson-Holden TJ, Lenke LG, Bridwell KH: Somatosensory- and motor-evoked potential monitoring without wake-up test during idiopathic scoliosis surgery: An accepted standard of care. Spine 1998;23:1392-1400.
References:
- Schwartz DM, Drummond DS, Hahn M, Ecker MI, Dormans JP: Prevention of positional brachial plexopathy during surgical correction of scoliosis. J Spinal Disord 2000;13:178-182.
Question 20High Yield
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
Explanation
44b The patient has a displaced comminuted clavicle middle one third fracture from a high-energy mechanism. Recent literature on high-energy clavicular fractures suggests a higher rate of nonunion than previously reported. A nonunion rate of 30% has been reported by Hill and associates when the fracture fragments are displaced more than 1.5 cm. In addition, several patients had neurologic symptoms related to the injury. Robinson and associates reported an increased risk of nonunion in women, elderly patients, comminuted fractures, and injuries with a lack of cortical contact. Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539. Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
References:
- Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 2004;86:1359-1365.
Question 21High Yield
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
Explanation
Traumatic dislocation of the hip in sports injuries is uncommon, and 85% to 92% occur in a posterior direction. In dislocations without fractures, osteonecrosis is the most common complication occurring in 10% to 20% of patients. MRI should be performed at 3 months postreduction to rule out osteonecrosis. Nerve injuries are rare in this setting, and recurrent dislocations are unusual without acetabular fractures. Chondrolysis has been reported as a rare occurrence. Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
References:
- Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 22High Yield
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
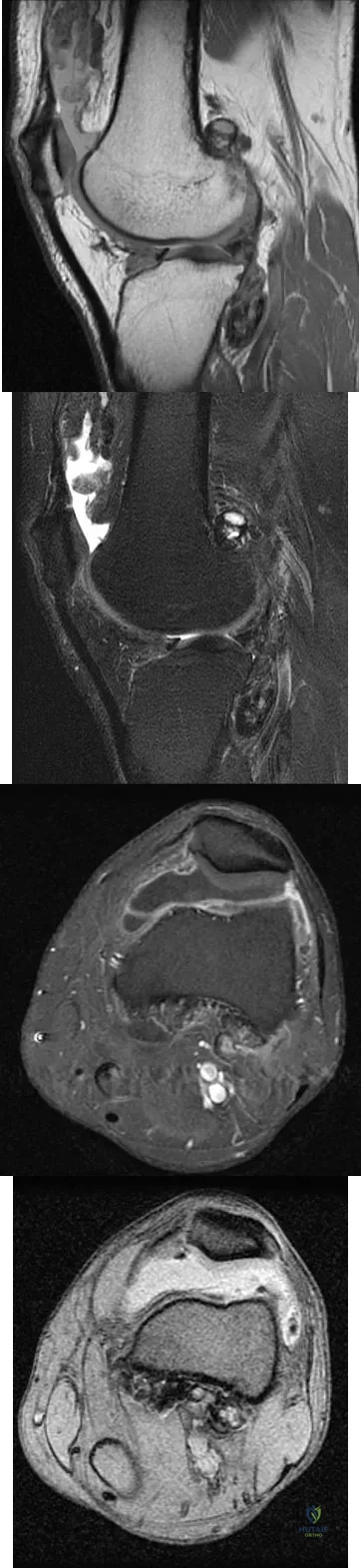
Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 23High Yield
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
References:
- Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 24High Yield
A homebound 75-year-old woman with diabetes mellitus has had progressive left knee pain and swelling for the past 6 weeks. She is febrile with a temperature of 103 degrees F (39.5 degrees C). History reveals that she underwent arthroplasty 5 years ago. Examination shows passive range of motion of 0 to 100 degrees with no active extension. Knee aspiration reveals purulent fluid with a Gram stain showing gram-negative rods. A radiograph is shown in Figure 27. In addition to IV antibiotics, which of the following management options offers the best chance of a successful outcome?
Explanation
Explanation
The patient has an infected total knee arthroplasty and an interrupted extensor mechanism. A late infection of a total knee arthroplasty in a patient with diabetes mellitus and a virulent organism requires removal of the components, debridement, antibiotic spacers, and surveillance to ensure eradication of the infection. Reconstruction of an incompetent extensor mechanism in an infected knee is extremely unlikely to be successful. Arthrodesis is the procedure of choice if a revision total knee arthroplasty is not likely to succeed. Resection arthroplasty is recommended only as a long-term solution if the patient is medically unable to undergo further surgery. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 513-536.
References:
- Hanssen AD, Rand JA: Evaluation and treatment of infection at the site of a total hip or knee arthroplasty. Instr Course Lect 1999;48:111-122.
Question 25High Yield
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity. Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
References:
- Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 26High Yield
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
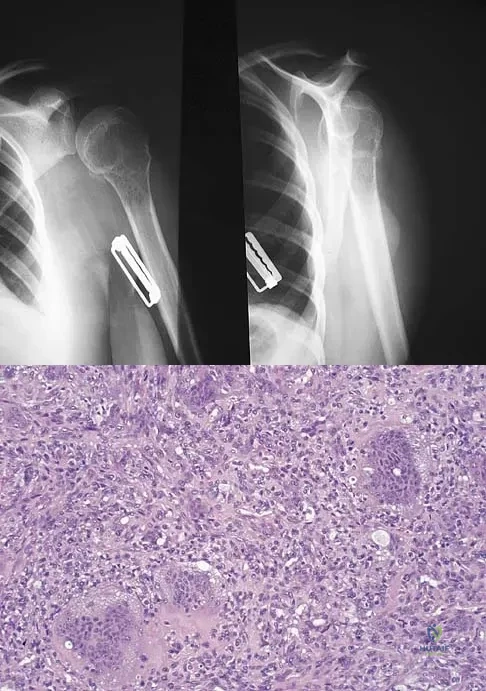
Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 27High Yield
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?

Explanation
Without stabilization, progressive kyphosis will develop between the spine and pelvis. The kyphosis progresses to the point that the child must use his or her hands to support the trunk, and therefore is unable to use his or her hands for other activities. Neck extension contracture does not usually develop. Neurologic deficit, including sexual dysfunction, is generally present at birth and static. Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Question 28High Yield
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
Explanation
45b Because the radiographs reveal poor regenerate bone, especially anteriorly and laterally, the first step in management is to slow the distraction rate. If this does not solve the problem, temporary reversal of the distraction, or "accordionization," can be used to induce a greater healing response. Maintaining the same distraction rate will further impair regenerate formation and delay healing. Bone grafting should be reserved as an option if decreasing the distraction rate or alternating a week of compression with a week of distraction fails to improve the callus formation. Repeat corticotomy is performed in patients with premature consolidation. Raney EM: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
References:
- Ilizarov GA: Pseudarthroses and defects of long tubular bones, in Transosseous Osteosynthesis: Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. Berlin, Springer-Verlag, 1992, p 453.
Question 29High Yield
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause

Explanation
If the Buford complex is mistakenly reattached to the neck of the glenoid, severe painful restriction of external rotation will occur. Williams MM, Snyder SJ, Buford D Jr: The Buford complex - the "cord-like" middle glenohumeral ligament and absent anterosuperior labrum complex: A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 30High Yield
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
Question 31High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 32High Yield
A 13-year-old boy has had pain and swelling in his ankle for the past several months. Based on the radiograph, MRI scan, and biopsy specimen shown in Figures 77a through 77c, what is the best course of action?
Explanation
Explanation
77b 77c Chondroblastomas are benign cartilage lesions frequently seen in adolescents or young adults. They are found in the epiphyseal or apophyseal regions of bones. The radiograph shows a radiolucent lesion with mineralization and a well-marginated rim of reactive bone. The lesion is composed of sheets of immature chondroblasts (polygonal cells with a clear, bluish cytoplasm and a small round central nucleus). In some regions, classic "chicken-wire" matrix calcifications and a "cobblestone" pattern of cell arrangement may be seen. Treatment consists of curettage and bone grafting. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 247-264.
References:
- Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 33High Yield
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?
Explanation
Explanation
27b The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
References:
- Morrissy RT, Wilkins KE: Deformities following distal humeral fracture in childhood. J Bone Joint Surg Am 1984;66:557-562.
Question 34High Yield
The Lisfranc ligament connects the base of the
Explanation
Explanation
The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
References:
- Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 35High Yield
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
Explanation
Growth factors are proteins secreted by cells that can act on target cells to produce certain biologic actions. These actions can be described as autocrine, paracrine, and endocrine. Autocrine actions are those in which the growth factor influences an adjacent cell of its origin or identical phenotype. Paracrine actions are those in which the protein influences an adjacent cell that is different in its origin or phenotype. Endocrine actions are those in which the factor influences a cell located at a distant anatomic site. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
References:
- Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 36High Yield
Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?
Explanation
Explanation
Implant-related fractures following hip fracture surgery were reported by Robinson and associates and showed that the risk of an ipsilateral femoral fracture is significantly increased with the use of short cephalomedullary nails as compared to a compression hip screw. The use of short cephalomedullary nails has not been shown to increase the risk of deep venous thrombosis or nonunion. Cephalomedullary nails overall have decreased surgical blood loss when compared to use of sliding-compression hip-screw devices. Robinson CM, Adams CI, Craid M, et al: Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am 2002;84:1116-1122.
Question 37High Yield
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
Question 38High Yield
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
Explanation
35b The approach to the calcaneus has evolved from several different patterns, driven by a high wound complication rate of 10%. The current extensile lateral approach was described by Zwipp and associates in 1988. The surgical exposure uses an L-shaped incision, with the vertical component positioned one half a finger's breath anterior to the Achilles tendon and extending distally to the junction of the lateral skin and the plantar skin. Borrelli and Lashgari mapped the angiosome of the lateral calcaneal flap and found that the major arterial blood supply to this flap consisted of three arteries: the lateral calcaneal artery, the lateral malleolar artery, and the lateral tarsal artery. The lateral calcaneal artery appeared to be responsible for most of the blood supply to the corner of the flap. This was found 1.5 cm anterior to the Achilles tendon. Division of this artery with inaccurate placement of the vertical limb of the incision can cause ischemia of the lateral skin flap. Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77. Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
References:
- Zwipp H, Tscherne H, Wulker N: Osteosynthesis of dislocated intra-articular calcaneus fractures. Unfallchirurg 1988;91:507-515.
Question 39High Yield
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
Explanation
Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 40High Yield
What is the typical axial plane transverse angulation of the thoracic pedicles?
Explanation
Explanation
Thoracic pedicles typically are angled 25 degrees medially at T1 so the starting point is more lateral. T2 angles about 15 degrees, and then the pedicles average about 5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal. Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.
Question 41High Yield
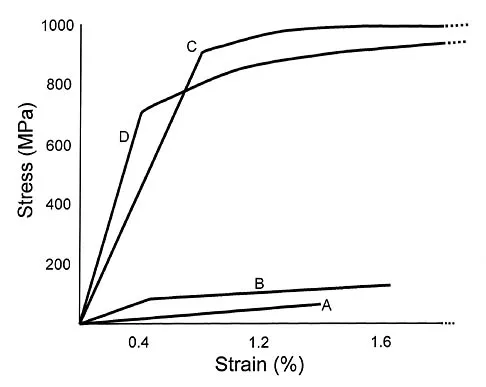
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Explanation
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism. Tencer AF, Johnson KD: Biomechanics in Orthopaedic Trauma: Bone Fracture and Fixation. Philadelphia, PA, JB Lippincott, 1994. Gonza ER: Biomechanical long bone injuries, in Gonza ER, Harrington IJ (eds): Biomechanics of Musculoskeletal Injury. Baltimore, MD, Williams & Wilkins, 1982, pp 1-30.
Question 42High Yield
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?
Explanation
Explanation
The history and physical examination are consistent with a monoarticular joint condition but not typical of joint sepsis. The arthroscopic appearance of brownish proliferative synovium is typical of PVNS. PVNS is a monoarticular synovial disease of unknown etiology and is treated with total synovectomy. The proliferative synovitis is not consistent with chondromalacia. Synovial cell sarcoma is an extracapsular disease. Rheumatoid arthritis typically is polyarticular, and the synovial appearance is not associated with hemosiderin deposition. Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
References:
- Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW: Arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 1999;15:613-617.
Question 43High Yield
A 16-year-old female dancer has persistent posterior ankle pain, particularly after a vigorous dancing schedule. Examination reveals tenderness both posteromedially and posterolaterally. MRI scans are seen in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
Explanation
44b Posterior ankle impingement or os trigonum syndrome is well described in dancers, and it is often associated with flexor hallucis longus tendinitis. High-quality MRI imaging will reveal the inflammation about the os trigonum and flexor hallucis longus tendinitis. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont IL, American Academy of Orthopaedic Surgeons, 1998, pp 315-332.
References:
- Hamilton WG, Hamilton LH: Foot and ankle injuries in dancers, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1225-1256.
Question 44High Yield
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
Explanation
Axial pain can be difficult to manage. Pain management is not always successful, and surgical approaches may provide disappointing results unless there is discrete pathology. Whereas planning of a surgical approach should consider prior approaches and preexisting laryngeal dysfunction, no compelling case for surgical intervention can be made for this patient. Therefore, management should consist of patient education, exercise, and nonnarcotic medication. Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692. Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
References:
- Rao R: Neck pain, cervical radiculopathy, and cervical myelopathy: Pathophysiology, natural history, and clinical evaluation. Instr Course Lect 2003;52:479-488.
Question 45High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted. Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
References:
- Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 46High Yield
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Explanation
Explanation
Rib penciling is the only singular factor; 87% of the curves progressed significantly in patients with three or more penciled ribs. Modulation in neurofibromatosis scoliosis implies the change from an idiopathic type to a dysplastic type of curve with rapid progression and the need for aggressive stabilization by fusion. Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
References:
- Durrani AA, Crawford AH, Chouhdry SN, et al: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 47High Yield
Which of the following methods is considered effective in decreasing the dislocation rate following a total hip arthroplasty using a posterior approach to the hip?
Explanation
A total hip arthroplasty using the posterior approach has resulted in hip dislocation under certain circumstances. Reconstruction of the external rotator/capsular complex is recognized as a stability-enhancing mechanism for the posterior approach. During the procedure, the acetabular component should be placed in 15 to 20 degrees of anteversion and approximately 45 degrees of abduction. Relative retroversion is a risk factor for posterior dislocation. High abduction angles result in edge loading of the polyethylene and possible early failure, as well as an increased risk of dislocation. Smaller diameter heads and skirted neck extensions used together decrease the range of motion that is allowed before impingement occurs, and this can result in dislocation. Shorter neck lengths generally result in soft-tissue envelope laxity. If laxity occurs, increased offset, neck length, or both can improve stability. Pellicci PM, Bostrom M, Poss R: Posterior approach to total hip replacement using enhanced posterior soft tissue repair. Clin Orthop 1998;355:224-228.
Question 48High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 49High Yield
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
Explanation
The radiograph reveals posterolateral rotatory subluxation of the radiohumeral and ulnohumeral joints. The space between the ulna and trochlea is enlarged, particularly posteriorly at the olecranon. These findings are diagnostic of posterolateral rotatory instability, which causes recurrent subluxation and reduction as the elbow is flexed from an extended and supinated position with valgus load. The posterolateral rotatory instability apprehension test was performed on this patient and the result was positive. The lateral pivot-shift test causes a clunk as the elbow reduces but is more difficult to perform, even under general anesthesia. The patient does not have isolated subluxation of the radial head, although these findings can be mistakenly diagnosed as such. The radial head is normally shaped and does not represent a congenital dislocation. There are no findings here to suggest osteochondritis dissecans or loose bodies. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446. Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 50High Yield
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
Explanation
While there are athletes who can function at a full level with an ACL tear, they are in the minority. As yet, there is no reliable way to predict the patients who will be able to compensate for the loss of the ACL. Studies have confirmed the risk of recurrent instability and meniscal injury in athletes with an ACL-deficient knee who participate in cutting sports. One study showed that only 12 of 43 patients who attempted rehabilitation and bracing were able to return successfully for the season. Another study showed that 17 of 31 athletes who were able to return to their sport sustained 23 meniscal tears because of recurrent instability. Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
References:
- Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 51High Yield
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
References:
- Davis AM, O'Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 52High Yield
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
Explanation
The lower extremity symptoms are consistent with a sympathectomy that is the result of an injury to the sympathetic chain, ipsilateral to the approach along the anterior border of the lumbar spine. This results in a warm, red foot, which creates the appearance that the normal cooler foot may have compromised circulation. The latter generally attracts greater attention because of the risks associated with limb ischemia. The condition usually is self-limited and does not require any specific treatment. Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
References:
- Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 53High Yield
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 54High Yield
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
Explanation
The child has an injury involving both the growth plate and the articular surface of the ankle. Because of the significant displacement, open reduction and internal fixation is indicated to realign the physis and joint surface. The best method of fixation to avoid growth arrest is one that does not cross the physis. This is usually achieved by a transverse epiphyseal screw parallel to the physis. If the metaphyseal fragment was large enough, a transverse metaphyseal screw could be used instead. The incidence of growth arrest following physeal ankle injuries is as high as 50%, and long-term follow-up is indicated. Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
References:
- Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 55High Yield
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of

Explanation
A favorable prognosis can be expected in up to 70% of children with Legg-Calve-Perthes disease who are younger than age 6 years. Containment treatment has not been shown to alter the outcome in this age group. The goals of treatment in this patient are to reduce pain (synovitis), restore motion, and improve function. Symptomatic treatment modalities include bed rest, traction, crutches, activity modification, and nonsteroidal anti-inflammatory drugs. Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Question 56High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include

Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 57High Yield
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 58High Yield
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
The median survival of patients after discovery of bone metastasis from primary lung carcinoma is shorter compared with other primary sites.
Question 59High Yield
A 42-year-old woman has persistent thumb pain that she notes is worse with opening jars and turning her car key. Opponens splinting provides some relief, but she is poorly tolerant of the splint. Finkelstein's test is negative, and a carpometacarpal grind test is positive. The radiographs shown in Figures 48a and 48b reveal minimal degenerative changes at the first carpometacarpal joint. What is the best course of action?
Explanation
Explanation
48b The woman has early basilar thumb arthritis. An extension osteotomy will redirect the force to the dorsal, more uninvolved portion of the first carpometacarpal joint and has been reported to alleviate pain in these patients. Arthrodesis is usually reserved for young, typically male laborers. Thermal shrinkage and denervation are considered experimental at this time. Interposition arthroplasty is typically used for more advanced stages of arthritis. Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106. Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
References:
- Tomaino MM, Pellegrini VD, Burton RI: Arthroplasty of the basal joint of the thumb: Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77:346-355.
Question 60High Yield
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 61High Yield
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
References:
- Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.
Question 62High Yield
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
Explanation
The most common complication of dorsal plating is extensor tenosynovitis, which often causes pain and is a frequent reason for hardware removal. Other less frequent complications include loss of reduction and extensor tendon ruptures, with flexor tendon ruptures occuring to an even lesser degree. Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
References:
- Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
Question 63High Yield
Osteoporotic vertebral compression fractures are associated with

Explanation
Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months. Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11. Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Question 64High Yield
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T2-weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
Explanation
10b 10c 10d The radiographs show a lytic lesion in the right proximal tibia that has a high fluid content based on the MRI findings. The radiographic appearance is consistent with either telangiectatic osteosarcoma or aneurysmal bone cyst. Low-magnification histology shows a lesion resembling an aneurysmal bone cyst, with blood lakes separated by cellular septa. However, high-magnification shows severe cytologic atypia, indicative of a telangiectatic osterosarcoma. The appropriate treatment is neoadjuvant chemotherapy followed by wide resection and reconstruction of the lesion. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 65High Yield
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
Explanation
64b 64c 64d 64e The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Question 66High Yield
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
Question 67High Yield
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 68High Yield
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of

Explanation
The radiograph shows the development of a rocker-bottom foot deformity. A rocker-bottom foot occurs in the treatment of clubfoot when casting is continued in the presence of a very tight gastrocnemius-soleus complex and an uncorrected hindfoot. While there are some preliminary reports on using Botox injection and continued casting for the equinus deformity, most authors recommend posterior or posterior medial release. Percutaneous tenotomy has been recently recommended with the resurgence of the Ponsetti technique. Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 135-136. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 927-935.
Question 69High Yield
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c The laboratory studies and histology are both consistent with myeloma. Infection should show white blood cells other than plasma cells on histology. Lymphoma would show lymphocytes, not plasma cells. The lack of bone formation on the imaging studies and the lack of osteoid on histology rule out osteosarcoma. The cells have too much cytoplasm and nuclear chromatin to be Ewing's sarcoma cells.
References:
- Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 70High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 71High Yield
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 72High Yield
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
Repetitive subfailure strains have been shown to affect the mechanical behavior of the inferior glenohumeral ligament, producing dramatic declines in the peak load response and length increases that are largely unrecoverable. In another study, anteroinferior subluxation was found to result in nonrecoverable strain in the anteroinferior capsule, varying from 3% to 7% through a range of joint subluxation. Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Question 73High Yield
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 74High Yield
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
Explanation
Treatment of patients with unplanned excision of soft-tissue sarcomas is challenging. If the margins are positive or unclear, the patient is best managed with repeat excision of the tumor bed, and radiation therapy if the repeat excision does not yield wide margins. In patients with no detectable tumor on physical examination or imaging after unplanned excision, some studies have shown that up to 35% of patients will have residual disease and a poorer local recurrence rate (22% versus 7%). Therefore, whenever feasible, a reexcision of the tumor bed is recommended.
References:
- Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 75High Yield
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
Explanation
Explanation
60b 60c 60d The patient has a large deep anterior thigh mass that has imaging characteristics of mature fat. Intramuscular lipomas are effectively treated with marginal resections with very low recurrence rates. Large lipomas often have small amounts of intralesional signal changes frequently representing trapped muscle fibers and do not necessitate more extensive margins. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
References:
- Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 76High Yield
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
Explanation
35b The radiographs show a minimally displaced fracture of the tibial eminence, which is classified as a McKeever type II injury. In a number of studies, it has been found that most of these fractures will reduce with extension of the knee. This is often made easier with evacuation of the hemarthrosis. The position of knee immobilization is controversial, with some authors preferring full extension and others preferring 20 degrees of flexion. Flexion to 90 degrees will further displace the fragment. If the fragment does not reduce or if the patient has a McKeever type III or IV injury, reduction and internal fixation are required. This can be done with either an open or an arthroscopic procedure. Excision of the fragment is not indicated. Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684. Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60 Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
References:
- Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 77High Yield
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
Explanation
A herniated cervical disk at C5-6 causes a C6 radiculopathy. There are eight cervical nerve roots and seven cervical vertebrae, and C8 exits between the C7 and T1 vertebrae. The C6 nerve root typically innervates the biceps and wrist extensor. The deltoid is predominantly innervated by C5. The wrist flexor and triceps are predominantly innervated by C7. Grip strength is predominantly a function of C8.
References:
- Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 78High Yield
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?
Explanation
Explanation
29b The radiograph and MRI scan show a pedunculated lesion arising from the medial aspect of the distal femoral metaphysis. The cortex of the lesion is contiguous with the cortex of the underlying normal bone. Similarly, the medullary canal of the lesion is contiguous with that of the normal bone. These findings are diagnostic of osteochondroma. Rarely a secondary chondrosarcoma can arise in a preexisting osteochondroma. This diagnosis is suggested by identifying a cartilage cap that is greater than 1.5-cm thick in a skeletally mature patient. MRI is the best study to rule out a secondary chondrosarcoma. CT also may be used for this purpose but is not indicated in this patient because an MRI has already been obtained. A bone scan is not useful to identify a secondary chondrosarcoma. Similarly, there is no role for biopsy in this patient. No further tests are needed. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Murphey MD, Choi JJ, Kransdorf, MJ, et al: Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
Question 79High Yield
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Explanation
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure. Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607. Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 80High Yield
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of

Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 81High Yield
What is the mechanism of action of bisphosphonates?
Explanation
Bisphosphonates are stable analogues of pyrophosphate that have a strong affinity for bone hydroxyapatite; these agents inhibit bone resorption by reducing the recruitment and activity of osteoclasts and increasing apoptosis. Bone formed while patients are receiving bisphosphonate treatment is histologically normal. Bisphosphonates have been shown to be effective in decreasing pathologic fractures, bone pain, and the need for radiation therapy in patients with multiple myeloma and metastatic carcinoma to bone. The most effective method of administration is via monthly intravenous infusion. Osteonecrosis of the mandible is sometimes a complication of this treatment. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 82High Yield
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
Explanation
The groin flap is based on the superficial circumflex iliac artery, an axial flap that has been a mainstay of providing soft-tissue coverage of the upper extremity. Flaps as large as 35 cm in length and 15 cm in width have been reported. An advantage of the flap is that when used as a pedicle flap, the donor site can be closed directly. A disadvantage of the flap is that it can be quite bulky and can have a thick layer of subcutaneous fat. The superficial circumflex iliac artery travels lateral and superficial to the fascia and below and parallel to the inguinal ligament. It is helpful to elevate the fascia at the medial border of the sartorius muscle to include the deep and superficial branches of the artery for improved flap survival. McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
References:
- Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 83High Yield
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
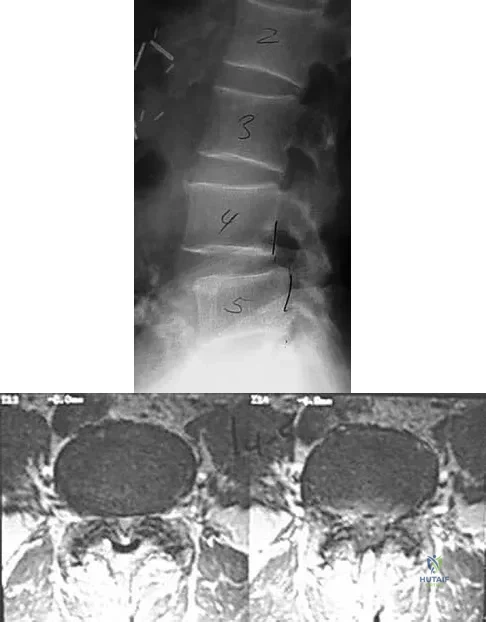
Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 84High Yield
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
Explanation
The lesion is typical of a subungual exostosis, which is most often found on the medial aspect of the great toe in children and young adults. The diagnosis is confirmed on radiographs and usually requires excision for relief. Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79. Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
References:
- Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 85High Yield
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
Explanation
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
References:
- Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 86High Yield
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
Explanation
4b The history and radiographs indicate a Lisfranc fracture-dislocation of the foot. The radiographs show the classic "fleck sign," which is an avulsion of the Lisfranc ligament from the base of the second metatarsal. Most authors recommend open reduction and internal fixation of this injury. Closed reduction can be attempted, but anatomic reduction is unlikely because of the interposed bone fragments and soft tissues. Standard radiographs are not reliable in identifying 1 to 2 mm of subluxation of the tarsometatarsal joint. The tarsometatarsal joint has a poor tolerance to even mild subluxation, and the resulting decrease in joint contact area increases the likelihood of posttraumatic arthritis. Open reduction with the joint visible allows more anatomic reduction and internal fixation of larger osteochondral fragments or excision of smaller interposed fragments. Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
References:
- Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 87High Yield
Figures 21a and 21b show the radiographs of a 22-year-old man who has had progressive pain and swelling about the knee for the past 6 weeks. Examination reveals limited range of motion and fullness about the knee. What is the most likely diagnosis?
Explanation
Explanation
21b The radiographs reveal a destructive lesion in the metaphysis of the distal femur with periosteal changes and an associated soft-tissue mass with subtle mineralization. This suggests an aggressive malignant process. In this age group, the most likely diagnosis is osteosarcoma. Giant cell tumor, which usually is in a more subchondral location, is not typically so aggressive. Aneurysmal bone cyst is usually more geographic, with a well-marginated reactive rim. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
References:
- Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3800-3833.
Question 88High Yield
Anterior subluxation in a throwing athlete is most commonly the result of
Explanation
Explanation
Subtle anterior subluxation in the throwing athlete most frequently results from excessive capsular laxity because of repetitive microtrauma. Avulsion of the inferior glenohumeral ligament from the glenoid, or more rarely from the humerus, occurs with macrotrauma. A large Hill-Sachs lesion and a glenoid rim fracture also may result from a traumatic anterior dislocation. Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
References:
- Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1999, pp 961-990.
Question 89High Yield
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient's program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study. Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Question 90High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
Explanation
25b The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
References:
- Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 91High Yield
Which of the following is considered the most appropriate indication for conversion of a hip fusion to total hip arthroplasty?
Explanation
Explanation
Hip fusion provides successful long-term results (20 to 30 years). The usual mode of failure is symptomatic arthrosis of the lower back, contralateral hip, or the ipsilateral knee. Disabling low back pain is the best indication for conversion and responds well to the procedure. Degenerative changes in the other joints do not respond as well and frequently require replacement arthroplasty. Restoration of limb length is not predictable after conversion to hip replacement. Santore RF: Hip reconstruction: Nonarthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 109-115.
References:
- Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 92High Yield
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Question 93High Yield
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
Explanation
Excessive internal tibial torsion is a common cause of intoeing in toddlers. In most children, this resolves spontaneously by 3 to 4 years of age. Intoeing in elementary age children is usually the result of excessive femoral anteversion. Studies have shown that active intervention (casting, splinting, and shoe modifications) has no demonstrable effect on the natural history or resolution of tibial torsion. Surgery is rarely indicated in adolescents with severe internal tibial torsion that has not resolved and is resulting in cosmetic and functional problems. Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Question 94High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 95High Yield
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
Explanation
The degree of acetabular dysplasia and the age of the child are important considerations when choosing what type of osteotomy to perform. The ability to obtain concentric reduction is a prerequisite of all osteotomies that redirect the acetabulum. Procedures that cut all three pelvic bones allow more displacement and, therefore, correction of acetabular dysplasia. The closer the osteotomy is to the acetabulum, the greater the coverage of the femoral head. Compared with the other acetabular osteotomies, the Ganz periacetabular osteotomy provides the greatest potential for correcting acetabular deficiency because there are no bone or ligamentous restraints to limit correction, but it has the disadvantage of being a technically demanding procedure. The amount of coverage provided by the Salter osteotomy is limited. Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
References:
- Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 96High Yield
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of
Explanation
Explanation
5b Plasmacytoma is very sensitive to radiation therapy and given the complexity of the resection and complications of surgery in the given location, radiation therapy is preferred. However, the patient has clear loss of bony structural integrity, and resultant instability would persist even with tumor irradiation; therefore, posterior stabilization is warranted. Chemotherapy and bone marrow transplant are reserved for systemic disease with multiple myeloma. Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
References:
- Durr HR, Wegener B, Krodel A, et al: Multiple myeloma: Surgery of the spine. Retrospective analysis of 27 patients. Spine 2002;27:320-324.
Question 97High Yield
What fibers of the anterior cruciate ligament tighten with extension of the knee?
Explanation
The anterior cruciate ligament consists of two functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Traditionally, anterior cruciate ligament reconstruction primarily recreates the anteromedial bundle. Recently, techniques for double bundle reconstruction have been described to recreate the normal anatomic relationship of the two bundles. Girgis FG, Marshall JL, Monajem AS: The cruciate ligaments of the knee joint: Anatomical, functional and experimental analysis. Clin Orthop Relat Res 1975;106:216-231. Cha PS, Brucker PU, West RV, et al: Arthroscopic double-bundle anterior cruciate ligament reconstruction: An anatomic approach. Arthroscopy 2005;21:1275.
Question 98High Yield
A 68-year-old woman stepped on a needle while walking barefoot 10 days ago. She is not certain but thinks it is imbedded in her foot, and she notes local tenderness at the puncture site and drainage. Her primary care physician has been treating her with oral antibiotics. A plain radiograph is shown in Figure 38. What is the best course of action?

Explanation
Based on the radiographic findings, the patient has a metallic foreign body in her foot that is consistent with a needle. She has local infection secondary to the continued presence of the foreign body. CT is not necessary to localize the foreign body as it is adequately visualized on the plain radiographs. The infection cannot be adequately treated until the foreign body is removed. Attempted removal of foreign bodies without proper anesthesia and fluoroscopy frequently results in frustration because of the inability to localize the foreign body. Removal in a surgical suite with proper anesthesia and fluoroscopy is the preferred option. Once the foreign body is removed, the local infection will resolve rapidly. Combs AH, Kernek CB, Heck DA: Orthopedic grand rounds: Retained wooden foreign body in the foot detected by computed tomography. Orthopedics 1986;9:1434-1435.
Question 99High Yield
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
Explanation
12b 12c Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome. Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
References:
- Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.
Question 100High Yield
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
Co-planing the distal clavicle may lead to painful acromioclavicular joints in up to 35% of patients; this is felt to be related to destabilizing the distal clavicle. Intra-articular diagnosis of synovitis, degenerative joint disease, and superior labrum anterior and posterior lesions would have been identified at initial arthroscopy (not necessarily seen in open surgery). Ganglions are seen on MRI. Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248. Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
