Orthopedic Board Review MCQs: Mock Exam Set #1027 (100 Questions)

Key Takeaway
This page offers Mock Exam Set #1027, featuring 100 randomized high-yield orthopedic surgery MCQs. Designed for ABOS, OITE, and FRCS board exams, it helps surgeons test their knowledge, identify areas for improvement, and master critical concepts for surgical success.
Unlock Surgical Success: Lumbar Spines Applie...
00:00
Start Quiz
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?
Explanation
Explanation
19b 19c 19d 19e The injury pattern is that of a burst fracture at L1 contiguous with a compression fracture at T12. There is associated kyphosis and slight spondylolisthesis of T12 on L1. Treatment of this type of burst fracture in neurologically intact patients is somewhat controversial, with at least one study demonstrating equal long-term results comparing nonsurgical treatment to surgical treatment. In this study, however, body casts were used initially in the nonsurgical group. Moreover, because this patient has multiple fractures, spinal fracture stabilization should be considered to facilitate early mobilization. Surgical stabilization and fusion via a posterior approach is the best treatment option in this patient. Anterior decompression is not necessary since the patient is neurologically intact. McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654. Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
- Millis MB, Murphy SB, Poss R : Osteotomies about the hip for the prevention and treatment of osteoarthrosis. Instr Course Lect 1996;45:209-226.
Question 3High Yield
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
Explanation
12b 12c The use of locked nailing for the treatment of established nonunion of the humerus has produced poor results. Since humeral nailing has already failed, exchange humeral nailing without bone grafting has an even less change of success. To increase the likelihood of achieving bony union, the treatment of choice is removal of the humeral nail, dynamic compression plating, and bone grafting. Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
References:
- Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach, an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 4High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 5High Yield
The posterior circumflex artery provides blood supply to what portion of the proximal humerus?
Explanation
Explanation
The posterior circumflex artery provides blood supply only to the posterior portion of the greater tuberosity and a small posteroinferior portion of the humeral head. The humeral head is supplied primarily by the anterolateral ascending branch of the anterior circumflex artery; the terminal branch of this artery is termed the arcuate artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 267-274.
References:
- Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 6High Yield
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of

Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 7High Yield
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
Explanation
Explanation
Survivorship is similar in the two groups. In a recent study, mobile-bearing TKAs showed a slightly higher maximum flexion than the total condylar fixed-bearing-type designs (112 degrees versus 108 degrees with no difference in recovery rate). Using a fixed-bearing or a mobile-bearing design did not seem to influence the recovery rate in early results after knee arthroplasty. Mobile-bearing arthroplasties are suggested, in theory, to offer a reduction in polyethylene wear; however, clinical studies have not yet proven this. Recovery rates have yet to be statistically seen as improved with either method. Differences in strength have not been shown. Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153. Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.
References:
- Dennis DA, Komistek RD: Kinematics of mobile-bearing total knee arthroplasty. Instr Course Lect 2005;54:207-220.
Question 8High Yield
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
Explanation
The radiograph shows enlargement of the bone, coarse trabeculation, a blastic appearance, and thickening of the cortex, revealing the classic appearance of Paget's disease in the sclerotic phase, the most common presentation. While lymphoma may present as a blastic lesion, it will not have the same enlargement, coarse trabeculation of bone, and the significant sclerosis seen here. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
References:
- Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 9High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 10High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 11High Yield
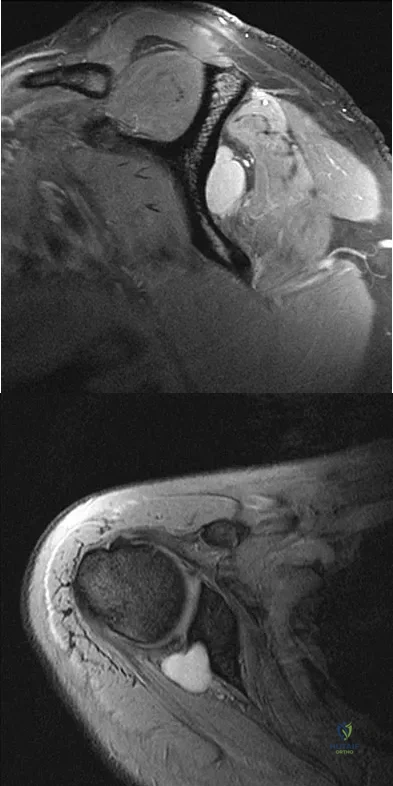
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 12High Yield
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient's program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study. Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Question 13High Yield
The risk of local recurrence after surgical resection of a soft-tissue sarcoma is most closely related to
Explanation
Explanation
A positive margin is most closely related to subsequent local recurrence. The other factors cited, including the size and site of the tumor, may be related to local recurrence; however, they are more commonly prognostic because of the difficulty in obtaining wide surgical margins about large or proximal tumors. Radiation therapy has been noted to decrease the incidence of recurrence but is not felt to be as important as the surgical margin. The grade of the tumor has more influence on the prevalence of metastatic disease than the incidence of local recurrence. Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF: Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol 1997;15:646-652.
References:
- Meterissian SH, Reilly JA Jr, Murphy A, Romsdahl MM, Pollock RE: Soft-tissue sarcomas of the shoulder girdle: Factors influencing local recurrence. Distant metastases and survival. Ann Surg Oncol 1995;2:530-536.
Question 14High Yield
In Gustilo type III open tibial diaphyseal fractures, which of the following factors is associated with an increased risk of a poor functional outcome?
Explanation
Explanation
According to the published outcomes analyses from the Lower Extremity Assessment Project (LEAP) study group of patients prospectively followed for 2 to 7 years, definitive fixation with an intramedullary nail has shown improved outcomes when compared to definitive external fixation. The findings showed that the timing of wound debridement (within 6 hours from injury as compared to within 6 to 24 hours), the timing of soft-tissue coverage (3 days or less from injury as compared to more than 3 days), and the timing of bone grafting after injury (within or after 3 months) did not impact the infection or union rates and had no effect on functional outcome. The LEAP study has shown at 7-year follow-up that patients who are definitively treated with external fixation have a significantly longer time to union, poorer functional outcomes, longer time to achieve full weight bearing, and more time in the hospital.
Question 15High Yield
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?
Explanation
Explanation
Teres minor originates from the middle third of the dorsal surface of the lateral border of the scapula. It is supplied by the axillary nerve (C5). Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 68-72.
Question 16High Yield
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Explanation
Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months. Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36. Artico M, Salvati M, D'Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700. Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
References:
- Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 17High Yield
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 18High Yield
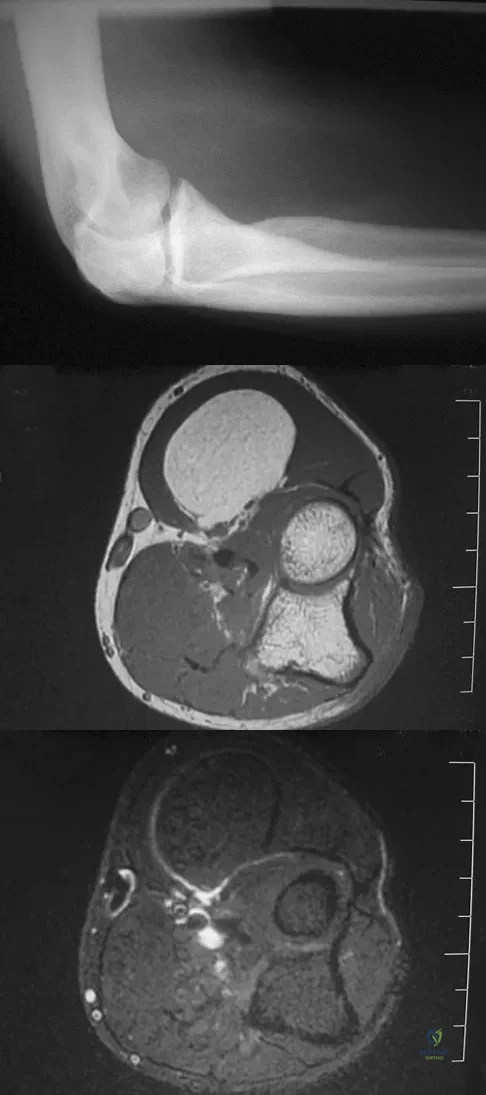
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 19High Yield
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
The patient has a nondisplaced stress fracture of the tarsal navicular. Weight bearing is associated with a high rate of nonunion; therefore, management should consist of immobilization and no weight bearing for 8 weeks. Delayed union or nonunion is treated by excision of sclerotic fracture margins and bone grafting, with or without internal fixation. Generally, CT should be repeated to document healing before permitting a return to sports. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 20High Yield
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of
Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 21High Yield
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a

Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 22High Yield
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with

Explanation
The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival. Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587. Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Question 23High Yield
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
Explanation
35b 35c The patient has an open fracture of the physis of the distal phalanx with a portion of the nail bed interposed in the physis. Seymour initially described this injury in the distal phalanges of fingers. Optimal treatment consists of removing the interposed tissue, irrigating the fracture, and a short course of antibiotics. The nail should be preserved to provide stability. Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34. Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
References:
- Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 24High Yield
A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
Explanation
Explanation
With an incomplete injury, the best chance for recovery occurs when the canal is cleared and the neural structures are decompressed. Anterior decompression, vertebral body reconstruction, and anterior stabilization have been shown to be highly effective in the treatment of burst-type injuries. Laminectomy alone is contraindicated because it increases the instability. Short segment posterior fixation has a high rate of failure in this type of injury at this level. Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
References:
- McGuire R Jr: The role of anterior surgery in the treatment of thoracolumbar fractures. Orthopedics 1997;20:959-962.
Question 25High Yield
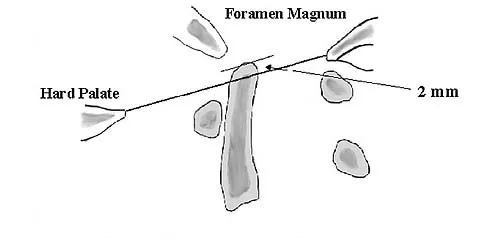
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 26High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 27High Yield
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of

Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 28High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
References:
- Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 29High Yield
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb "feels" different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?

Explanation
The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations. Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695. Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Question 30High Yield
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of
Explanation
Explanation
The patient has a chondroblastoma of the proximal humerus; therefore, the treatment of choice is curettage and bone grafting. Surgical resection of the proximal humerus is not indicated in the initial treatment of an intraosseous chondroblastoma. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
References:
- Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 31High Yield
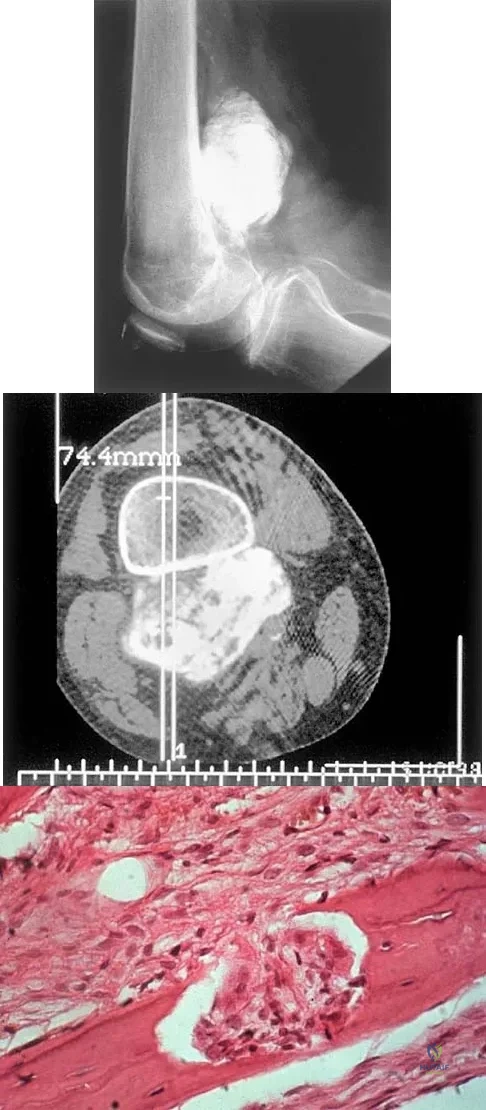
An otherwise healthy 75-year-old man has a painful mass in the popliteal fossa of his right knee. A lateral radiograph of the knee, a CT scan of the distal femur, and a histopathologic specimen are shown in Figures 13a through 13c. Management should consist of
Explanation
The patient has a parosteal osteosarcoma of the distal femur. The findings of mild knee pain, radiographic evidence of a radiodense mass involving the parosseous space or surface of the distal femur, and histologic findings of a spindle cell lesion forming immature osteoid with little to no necrosis most likely suggest a parosteal osteosarcoma. The treatment of choice is surgical resection. Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma: A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Scientific References
- :
Question 32High Yield
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?

Explanation
The presence of synchronous bone disease in young patients carries a dismal prognosis, one that is even worse than the presence of resectable pulmonary metastasis. Many osteosarcomas cross the physis; therefore, this has not been shown to be of prognostic importance. Similarly, the presence of the soft-tissue mass has less prognostic significance.
Question 33High Yield
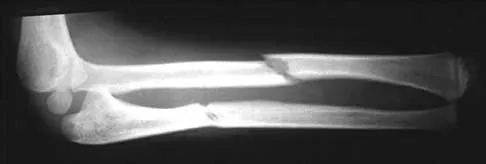
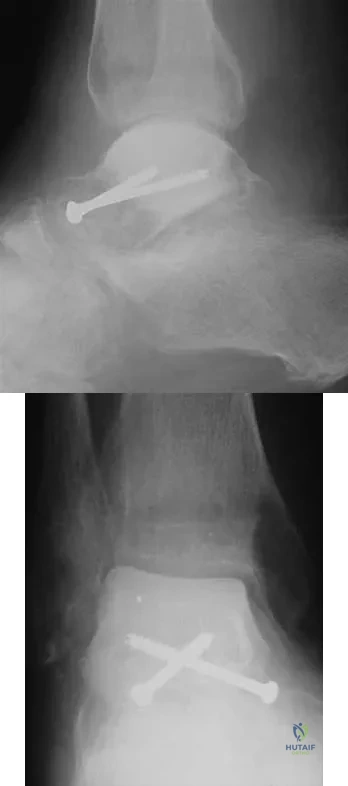
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
Explanation
Explanation
5b The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle. Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 1973-2016.
References:
- Marsh JL, Saltzman CL: Ankle fractures, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green's Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2147-2247.
Question 34High Yield
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
Explanation
The posterior cord of the brachial plexus terminates into the radial and axillary nerves. The lateral cord terminates in branches to the musculocutaneous and the lateral root of the median nerve. The medial cord terminates in branches to the ulnar and medial roots of the median nerve.
References:
- Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Question 35High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 36High Yield
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?

Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 37High Yield
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
Explanation
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
References:
- Pollack R, Brennan M, Lawrence W, Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 38High Yield
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?
Explanation
Explanation
Based on findings of a sudden increase in pain with associated swelling, the most likely diagnosis is a stress fracture. The initial radiographic findings usually will be negative. Morton's neuroma and transfer metatarsalgia are not associated with swelling. Metatarsophalangeal synovitis usually involves the second metatarsophalangeal joint. Freiberg's infraction is seen clearly on a radiograph.
References:
- Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 39High Yield
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
Explanation
Patients with peripheral neuropathy will often initially see an orthopaedic surgeon and report symptoms of burning, numb, dead, or wooden feet. A simple diagnostic evaluation with a tuning fork (to test vibratory sensibility) or use of the Semmes-Weinstein monofilaments will help make the diagnosis. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
References:
- Gorson KC, Ropper AH: Idiopathic distal small fiber neuropathy. Acta Neurol Scand 1995;92:376-382.
Question 40High Yield
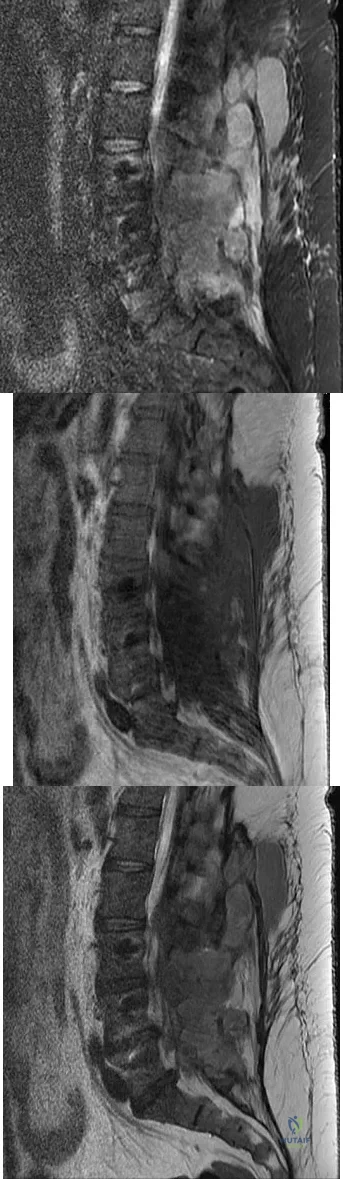
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of

Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 41High Yield
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 42High Yield
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
References:
- Ross PD, Davis JW, Epstein RS, Wasnich RD: Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114:919-923.
Question 43High Yield
A 43-year-old man reports a 3-year history of progressively worsening pain in the first metatarsophalangeal joint that is aggravated by activity. Larger shoes, intra-articular corticosteroid injections, and a Morton's extension pedorthic have failed to provide relief. Motion is limited to 10 degrees of dorsiflexion, and the "grind test" is positive. An AP radiograph is shown in Figure 39. What is the most appropriate surgical treatment?

Explanation
Stage III hallux rigidus comprises end-stage degenerative arthritis with loss of cartilage from the phalanx and metatarsal. Therefore, cheilectomy, osteotomy, and resection arthroplasty are inadequate. Resection arthroplasty results in diminished propulsion and transfer metatarsalgia. Resurfacing implant hemiarthroplasty remains unproven for earlier stages of hallux rigidus, but is not appropriate when there is cartilage loss from the base of the proximal phalanx. First metatarsophalangeal arthrodesis has proven to be a very reliable and functional treatment of end-stage hallux rigidus. Gibson JN, Thomson CE: Arthrodesis or total replacement arthroplasty for hallux rigidus: A randomized controlled trial. Foot Ankle Int 2005;26:680-690.
Question 44High Yield
Figures 12a through 12c show the radiographs of a 28-year-old professional baseball player who has ulnar-sided wrist pain and numbness and tingling in the fourth and fifth digits for the past 6 weeks. Management should consist of
Explanation
Explanation
12b 12c Hook of the hamate fractures typically occur as a result of direct force from swinging a bat, golf club, or racket. Pain is localized to the hypothenar eminence. The injury is best seen on a carpal tunnel view. CT will confirm the diagnosis. Chronic cases can be associated with neuropathy of the ulnar nerve. Excision of the hook through the fracture site usually yields satisfactory results, allowing the athlete to return to competition. Parker RD, Berkowitz MS, Brahms MA, et al: Hook of the hamate fractures in athletes. Am J Sports Med 1986;14:517-523.
References:
- Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 113-128.
Question 45High Yield
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
Explanation
41b 41c The radiographic appearance shows a slightly expansile lesion in the proximal phalanx of the fifth digit typical of an enchondroma. There is a stippled appearance within the bone and no evidence of cortical destruction. The biopsy reveals a cartilage lesion with basophilic cytoplasm. There are some hypercellular areas but no evidence of pleomorphism. Enchondromas in the tubular bones of the hand are usually more cellular than their counterparts in the femur and humerus and should not be considered malignant. No other lesions are noted in the radiograph, so a diagnosis of Ollier's disease cannot be made. An osteochondroma is a benign surface cartilage tumor. Brown tumor and osteomyelitis can be differentiated from enchondroma based on the histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 46High Yield
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
Explanation
In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture. Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 144-148.
References:
- Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 47High Yield
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
Explanation
Explanation
52b 52c 52d The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate approaches although useful for this fracture, have a higher rate of complications. Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.
Question 48High Yield
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 49High Yield
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
Explanation
The patient has transient osteoporosis of the hip. Transient osteoporosis is usually a self-limited condition that is most frequently seen in women in the third trimester of pregnancy and in men in the sixth decade of life. Transient osteoporosis is best treated with protected weight bearing.
References:
- Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 50High Yield
The iliopectineal fascia runs between which of the following structures?
Explanation
Explanation
The sheath of the psoas muscle or the iliopectineal fascia separates the more lateral iliopsoas muscle and the femoral nerve from the more medially located iliac vessels. This fascia has to be taken down to enter the true pelvis. Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 51High Yield
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?

Explanation
The radiograph reveals a metaphyseal lesion with some stippled mineralization suggesting a chondroid tumor. The bone scan shows increased uptake, beyond what is expected for a simple enchondroma, and beyond the limits of the lesion. The MRI sequences shows a lobular lesion on the T1- and T2-weighted (bright on the T2 sequence) images with inhomogeneous uptake of gadolinium; both findings are typical for a chondroid lesion. The history of pain, the positive bone scan, the age of the patient, the size of the lesion, and the central location (enostotic) of the lesion all suggest a malignant cartilage tumor. The images are not consistent with the other diagnoses. In particular, plasmacytoma is more uniformly bright on T2-weighted images and often has a negative bone scan. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-194.
Question 52High Yield
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
Explanation
Explanation
35b The images show a large, almost circumferential, mass surrounding the diaphysis of the femur. The intramedullary signal is normal with minimal cortical destruction, both findings that should be abnormal in conventional osteosarcoma and Ewing's sarcoma. There are very low-signal striations representing osteoid formation that would have a sunburst radiographic pattern. This indicates an osteogenic lesion. Myositis ossificans is not indicated because studies would reveal zonal ossification starting in the periphery rather than the more central pattern seen in this patient. This appearance is typical for periosteal osteosarcoma.
References:
- El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 176.
Question 53High Yield
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?

Explanation
The avulsed fragment represents the origin of the rectus femoris from the anterior inferior iliac spine and the brim of the acetabulum. Avulsion of the anterior inferior iliac spine is much less common than avulsion of the anterior superior iliac spine with its origin of the sartorius. The origin of the gluteus minimus is from the outer cortex of the iliac wing and has not been reported as a source of bony avulsion. The hip capsule is composed of the ischiofemoral and pubofemoral ligaments, in addition to the iliofemoral ligament. The pelvic attachment of the ischiofemoral ligament is from the ischial part of the acetabulum posteriorly, while the pubofemoral ligament attaches to the pubic portion inferiorly. Technically, ligaments do not have origins and insertions as muscle tendon groups do, but have attachment sites. Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 54High Yield
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 55High Yield
A 62-year-old man with diabetes mellitus has had a persistent 2-cm ulcer under the third metatarsal head for the past 4 months. He reports that he has had similar ulcers twice before, and both healed with nonsurgical management. He has used multiple types of commercial walking braces, shoes, and commercial dressings without resolution. He is insensate to the Semmes-Weinstein 5.07 monofilament. When the wound is probed with culture swab, there is no communication with the metatarsal head. Radiographs, bone scans, and laboratory studies reveal no evidence of osteomyelitis. What is the most predictable method of accomplishing wound healing without recurrence?
Explanation
The patient has a persistent diabetic foot ulcer without evidence of osteomyelitis. He has evidence of a sensory peripheral neuropathy and a concomitant motor neuropathy, leading to a dynamic motor imbalance. Use of a total contact cast would offer a high probability of healing the resistant ulcer but with a high potential for recurrence. Combining the total contact cast with Achilles tendon lengthening allows wound healing without a high risk for recurrence. Excision of the noninfected metatarsal head would make the patient vulnerable to the development of a transfer lesion under one of the remaining metatarsal heads. Robertson DD, Mueller MJ, Smith KE, et al: Structural changes in the forefoot of individuals with diabetes and a prior plantar ulcer. J Bone Joint Surg Am 2002;84:1395-1404.
Question 56High Yield
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?
Explanation
An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 57High Yield
A 51-year-old plumber has a failed peroneus brevis tendon repair. He reports continued pain and swelling in the distal retrofibular area. MRI shows longitudinal tears of the peroneus longus and peroneus brevis. What is the surgical treatment of choice at this time?
Explanation
Explanation
A flexor digitorum longus transfer, while not as strong as the peroneals, improves the tendon balance and maintains hindfoot mobility. Subtalar fusion is a salvage procedure. Posterior tibial tendon transfer compromises inversion strength and arch height. Functional absence of the peroneals results in an imbalance that could lead to forefoot varus. Redfern D, Myerson M: The management of concomitant tears of the peroneus longus and brevis tendons. Foot Ankle Int 2004;25:695-707.
References:
- Borton DC, Lucas P, Jomha NM, et al: Operative reconstruction after transverse rupture of the tendons of both peroneus longus and brevis: Surgical reconstruction by transfer of the flexor digitorum longus tendon. J Bone Joint Surg Br 1998;80:781-784.
Question 58High Yield
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Explanation
Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized. Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Question 59High Yield
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
Explanation
A volar lunate fragment of a distal radial fracture is considered a critical component to overall joint stability and function. Obtaining a reduction is difficult through a standard volar approach to the radius between the flexor carpi radialis and radial artery. Visualization and reduction of the ulnar volar facet is not possible from this approach. An extended carpal tunnel incision provides access to the entire articular surface, except for the distal radial styloid component. Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
References:
- Trumble TE, Culp RW, Hanel DP, et al: Intra-articular fractures of the distal aspect of the radius. Instr Course Lect 1999;48:465-480.
Question 60High Yield
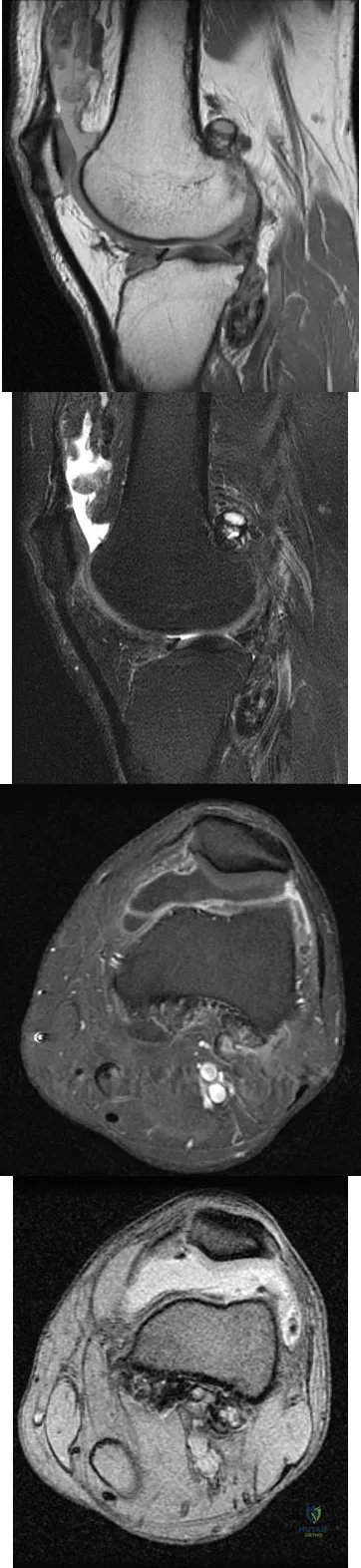
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 61High Yield
What is the second most common primary bone malignancy in children?
Explanation
Explanation
Ewing's sarcoma is the second most common bone tumor in children with an incidence of three per one million Caucasian children younger than 21 years of age. Ewing's sarcoma is rare in African Americans. Osteosarcoma is the most common bone tumor in children. Rhabdomyosarcoma is the most common soft-tissue sarcoma in children. Fibrosarcoma is a rare primary bone tumor most commonly seen in adults. Adamantinoma is a rare primary bone malignancy also most commonly seen in adults in the tibia. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
References:
- Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 62High Yield
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
Explanation
The factors that are independently prognostic of patient survival are tumor size, tumor grade, and tumor depth (ie, subfascial versus superficial). These factors are the basis for the American Joint Committee on Cancer staging criteria. Patient age and neurovascular invasion are not prognostic. Surgical margin is prognostic for local recurrence but not conclusively for patient survival or metastasis. Metastatic disease is also predictive of survival. Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
References:
- Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 63High Yield
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves

Explanation
TFCC tears are common in athletes. As the athlete braces for a fall, the wrist is most commonly in an extended position and the forearm is pronated. Cohen MS: Ligamentous injuries of the wrist in the athlete. Clin Sports Med 1998;17:533-552.
Question 64High Yield
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of
Explanation
Explanation
22b 22c Enchondromas are the most common benign skeletal lesions identified in the bones of the hand. Most are incidentally found or initially become clinically evident after a pathologic fracture. If the patient has a fracture, the hand is immobilized until union. If the lesion is large and further pathologic fractures are expected, then an intralesional curettage and grafting procedure may be warranted. In this patient, the lesion has not significantly altered the size, shape, or morphology of the involved metacarpal head and recurrent fracture is unlikely. Observation with follow-up radiographs is considered appropriate management. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 213-228.
References:
- Marco RA, Gitelis S, Brebach GT, et al: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 65High Yield
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination. Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16. Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27. Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546. Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Question 66High Yield
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
A muscle that lengthens as it is activated is an eccentric contraction. Isometric contraction involves no change in length. Concentric contraction occurs while the muscle is shortening. In isotonic contraction, the force remains constant through the contraction range. Isokinetic muscle contraction occurs at a constant rate of angular change of the involved joint. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 12-13.
Question 67High Yield
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 68High Yield
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
Explanation
The paravertebral musculature, the intervertebral disks, and the normal lordotic curvature of the cervical spine can absorb much of the imparted energy of collision. However, when the neck is flexed approximately 30 degrees, the normal lordotic curvature is flattened and the forces applied to the vertex of the head are directed at a straight segmented column. In this situation, the cervical spine is less able to absorb the applied force. With mounting axial load, compressive deformation occurs within the intervertebral disks, causing angular deformation and buckling. The spine will fail in flexion, with resultant fracture, subluxation, or dislocation. A rotatory component added to axial compression can cause concomitant extension, rotation, and shear injury patterns. The National Football Head and Neck Injury Registry has made two recommendations to the NCAA Football Rules Committee to minimize the risk of such injuries: (1) No player should intentionally strike an opponent with the crown or top of the helmet; and (2) No player should deliberately use his helmet to butt or ram an opponent. Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
References:
- Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978.
- JAMA 1979;241:1477-1479.
Question 69High Yield
Human menisci are made up predominantly of what collagen type?
Explanation
Explanation
Type I collagen accounts for more than 90% of the total collagen content. Other minor collagens present include types II, III, V, and VI. Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, p 41.
References:
- Kawamura S, Rodeo SA: Form and function of the meniscus, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 70High Yield
A 64-year-old man has had increasing pain in the left hip for the past 6 months. A radiograph and MRI scan are shown in Figures 25a and 25b. Biopsy specimens are shown in Figures 25c and 25d. What is the recommended treatment?
Explanation
Explanation
25b 25c 25d The radiograph shows a lytic lesion in the left periacetabular area consistent with chondrosarcoma. A large soft-tissue mass is present along with extension through the supra-acetabular region and pubic ramus. The histology shows a hypercellular lesion infiltrating through the bony trabeculae with a basophilic cytoplasm. This is classified as a grade 2 chondrosarcoma. The treatment of a pelvic chondrosarcoma is wide resection via either an internal hemipelvectomy or amputation. Chondrosarcoma requires surgical resection for control and does not traditionally respond to chemotherapy or external beam irradiation therapy. Pring M, Weber, KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg 2001;83:1630-1642.
References:
- Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 255.
Question 71High Yield
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?

Explanation
Progressive weakness is a common sign with a large differential diagnosis. Nerve, muscle, and joint problems should be excluded when a patient has diffuse weakness and atrophy. Fascioscapulohumeral dystrophy is a rare disease characterized by facial muscle weakness and proximal shoulder muscle weakness. The weakness is usually bilateral, and scapular winging is common. If the scapular winging becomes pronounced, elevation of the shoulder can be affected. In severe cases, scapulothoracic fusion or pectoralis muscle transfer to the scapula may be indicated. Duchenne muscular dystrophy is typically severe and progressive. The other diagnoses are not compatible with the history or the physical findings. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Question 72High Yield
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
Explanation
Chronic lateral instability is commonly associated with a longitudinal split tear of the peroneus brevis tendon. The interrelationship of lateral ankle instability with superior retinacular laxity and resultant peroneus brevis split can account for persistent lateral ankle pain in this patient. Surgical treatment must identify and correct the underlying tendon pathology and should attempt to repair or debride the peroneus brevis tendon, reconstruct the superior peroneal retinaculum, flatten the posterior edge of the fibula by removing the sharp bony prominence, or deepening the fibular groove, along with addressing lateral ankle ligamentous instability. The laboratory values are not consistent with infection. A negative anterior drawer test confirms stability of the repair. Ankle arthritis is not seen on radiographs and usually takes longer than 3 months to develop. Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Question 73High Yield
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?

Explanation
The incidence of injury associated with horseback rising is estimated to be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately 15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled at 6 months after injury as recreational riders. Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Question 74High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 75High Yield
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent clinical result with complete resolution of leg pain. Three months later she now reports increasing back pain and weakness in her legs. Examination reveals weakness in the quadriceps and tibialis anterior. Radiographs show no interval changes in the position of the hardware. MRI scans are shown in Figures 2a through 2c. What is the next most appropriate step in management?
Explanation
The MRI scans reveal a postoperative infection. Observation and antibiotics are not appropriate choices. There is a large fluid collection and this requires decompression because the patient has neurologic changes. There is considerable debate regarding the removal of hardware. Many contend that biofilm on the implants can harbor the infection. However, these complications usually can be treated with serial irrigations, debridements, and IV antibiotics. The incidence of infection has been widely studied with varying rates in fusions with instrumentation. Rates appear to be increased with instrumentation, yet these infections usually can be managed without hardware removal. Glassman SD, Dimar JR, Puno RM, et al: Salvage of instrumental lumbar fusions complicated by surgical wound infection. Spine 1996;21:2163-2169.
Question 76High Yield
If heel varus corrects with a Coleman block test, then the hindfoot deformity is flexible. This test proves that the varus is due to a
Explanation
Explanation
The Coleman block test is used to evaluate the effect of the forefoot on the rearfoot varus. If the deformity corrects with the block, then the hindfoot deformity is flexible and the varus position is secondary to the plantar flexed first ray or valgus position of the forefoot. A rearfoot orthotic will not correct the forefoot cause of the deformity. The patient still may need a lateralizing calcaneal osteotomy to realign the hindfoot. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.
References:
- Alexander IJ, Johnson KA: Assessment and management of pes cavus in Charcot-Marie-Tooth disease. Clin Orthop Relat Res 1989;246:273-281.
Question 77High Yield
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time?
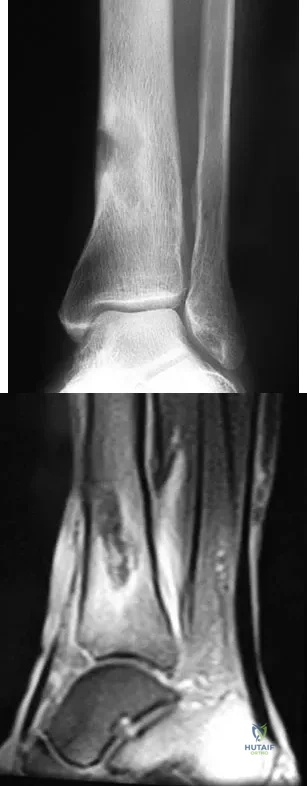
Explanation
The patient has chronic tibial osteomyelitis that is due to low virulent bacteria. The history and studies do not suggest the need for an amputation or a free-flap procedure. This is a localized tibial infection that is in a healed bone; there is no need to resect the entire area of the tibia bone around the infection. The most appropriate treatment is curettage, debridement of nonviable bone, and placement of absorbable antibiotic beads, followed by a course of IV antibiotics from 1 to 4 weeks and a 6-week course of oral antibiotics. Studies have shown that in cases of localized osteomyelitis that are of low virulence, as little as 1 week of IV antibiotics followed by 6 weeks of oral antibiotics is successful. Patzakis MJ, Zalavras CG: Chronic posttraumatic osteomyelitis and infected nonunion of the tibia: Current management concepts. J Am Acad Orthop Surg 2005;13:417-427.
Question 78High Yield
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?

Explanation
It is critical for graft isometry and knee stability that the femoral tunnel be placed as far posterior as possible on the lateral femoral condyle. Superiorly, the graft should be at the one o'clock position on the left knee. Resident's ridge is a false posterior shelf that often seems like the extreme posterior cortex. Abnormal tunnel placement results in a variety of complications, including an unstable knee, early graft failure, and joint stiffness. Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Question 79High Yield
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?

Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 80High Yield
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?

Explanation
C-reactive protein declines rapidly as the clinical picture improves. Failure of the C-reactive protein to decline after 48 to 72 hours of treatment should indicate that treatment may need to be altered. Blood culture is positive only 50% of the time and will be negative soon after antibiotics are administered, even if treatment is not progressing satisfactorily. WBC count is highly variable and poorly correlated with treatment. The ESR rises rapidly but declines too slowly to guide treatment. Radiographic findings may not change but can take up to 2 weeks to show changes.
Question 81High Yield
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by

Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Question 82High Yield
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate?
Explanation
Explanation
Pectoralis major ruptures typically occur in avid weightlifters (often on supplements) and typically while bench-pressing. Clinically there is significant discoloration/bruising over the pectoralis and into the axilla. MRI helps confirm the diagnosis and may help determine if the tear is in the muscle belly or at the bone-tendon junction. Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
References:
- Aarimaa V, Rantanen J, Heikkila J, et al: Ruptures of the pectoralis major muscle. Am J Sports Med 2004;32:1256-1262.
Question 83High Yield
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of
Explanation
Explanation
38b Osteonecrosis of the femoral head is a known complication from the use of rigid intramedullary nails for femoral fractures in adolescents. When the nails are placed through the piriformis fossa, the lateral ascending vessels of the femoral neck may be injured, resulting in osteonecrosis of the femoral head in 1% to 2% of patients. Rigid reamed nails placed into the piriformis fossa are contraindicated in children with open growth plates because the physis is a barrier to blood supply and the ligamentum teres does not provide sufficient vascularity. Alternative fixation methods for femoral fractures in adolescents include external fixation and open reduction and internal fixation. Nailing through the tip of the trochanter may decrease the incidence of this serious complication. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
References:
- Beaty JH, Austin SM, Warner WC, et al: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop 1994;14:178-183.
Question 84High Yield
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal
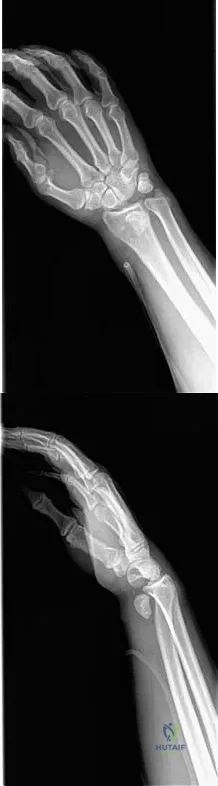
Explanation
The patient has a perilunate dislocation. A volar dislocation of the lunate is often associated with median nerve dysfunction. This injury to the wrist is often overlooked because of its benign clinical appearance and the presence of other injuries, as it is caused by high-energy mechanisms. Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Question 85High Yield
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
Explanation
Pediatric bony Chance fractures occur following severe flexion injuries as seen after motor vehicle accidents with lap belt restraints. There is a high rate of associated intra-abdominal injuries. In the absence of associated injuries, these fractures are best treated with immobilization. Bed rest is not necessary. Surgical fixation usually is not needed. Surgical stabilization and two-level fusion may be indicated in select individuals with progressive kyphosis of more than 25 degrees or other conditions that preclude cast or brace immobilization. Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751. Glassman SD, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
References:
- Raney EM, Bennett JT: Pediatric Chance fracture. Spine 1992;17:1522-1524.
Question 86High Yield
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
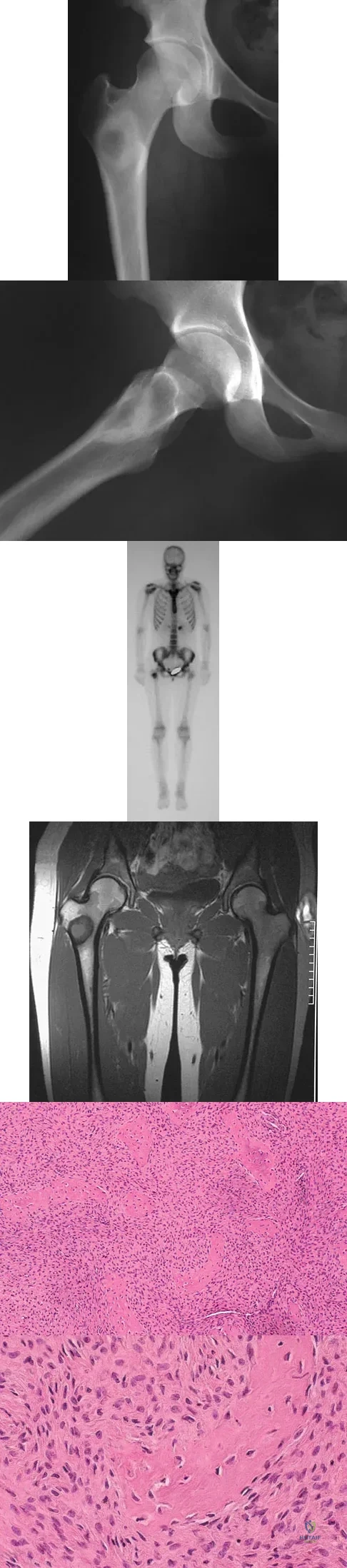
Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 87High Yield
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?

Explanation
A DEXA scan is most appropriately used to establish a baseline score. Even if the bone mineral density is not within the osteoporotic range (T-score less than -2.5), a prior fragility fracture is a strong risk factor for a second fracture as a result of factors other than bone density, such as worsening vision or balance, confusion, or other predispositions to falls. The guidelines of the National Osteoporosis Foundation indicate that, following a fragility hip fracture, active anti-osteoporotic medication should be initiated, whether or not a DEXA scan is performed. A recent study showed that antiresorptive therapy following a hip fracture reduces not only the risk of a second fracture but also overall mortality.
Question 88High Yield
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
Explanation
In a multivariate analysis, the strongest factor for the development of compartment syndrome is fracture of the proximal third of the forearm. However, compartment syndrome can still occur without a fracture. Therefore, these patients should be followed with a high level of suspicion for the development of compartment syndrome. Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
References:
- Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 89High Yield
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?

Explanation
The axillary nerve lies within millimeters of the anterior inferior capsule. The inferior capsule is of varying thickness, and thermal energy used in shortening the ligament can cause damage to the sensory fibers of the axillary nerve. Clinically, this is manifested as a burnt skin sensation in the axillary nerve distribution area. The motor branch of the axillary nerve is usually spared. The suprascapular nerve and the radial nerve are far from the shrinkage zone. The musculocutaneous nerve, frequently at risk with open procedures, lies well anterior. Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
Question 90High Yield
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?
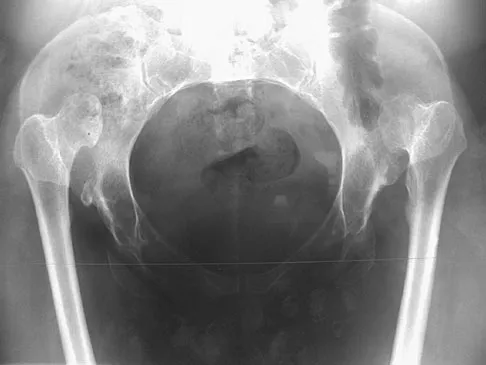
Explanation
The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve. Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Question 91High Yield
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
Explanation
Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen. Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86. McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 92High Yield
Which of the following agents have been shown to reduce the incidence of skeletal events in patients with multiple myeloma?
Explanation
Bisphosphonates are a class of drugs that act to inhibit osteoclast resorption of bone. It has been shown that patients with multiple myeloma who are treated with bisphosphonates have fewer pathologic fractures than patients who are not treated with bisphosphonates. Vitamin D and calcium are considered appropriate for patients who are at risk for the development of osteoporosis, as is estrogen in selected women. Chelating agents and progesterones have no use in the treatment of patients with multiple myeloma or osteoporosis. Berenson JR: Bisphosphonates in multiple myeloma. Cancer 1997;15:1661-1667.
Question 93High Yield
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?
Explanation
Explanation
In a series reported by Blaine and associates, 12 patients were converted from interposition to total elbow arthroplasty. This procedure was successful in 10 out of 12 patients. Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
References:
- Cheng SL, Morrey FB: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 94High Yield
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
Explanation
In secondary amenorrhea, women do not receive the estrogen needed to maintain adequate bone mineralization. This hypoestrogenic state affects bone density, and there is evidence that stress fractures are more frequent in amenorrheic than eumenorrheic athletes. The other conditions are not seen with increased frequency in amenorrheic athletes. Warren MP: Health issues for women athletes: Exercise-induced amenorrhea. J Clin Endocrinol Metab 1999;84:1892-1896.
References:
- Rencken ML, Chesnut CH III, Drinkwater BL: Bone density at multiple skeletal sites in amenorrheic athletes. JAMA 1996;276:238-240.
Question 95High Yield
The thickest bone in the occiput is located
Explanation
Explanation
Anatomic studies have shown that the thickest bone of the occiput is at the level of the external occipital protuberance. It ranges from 11.5 mm to 15.1 mm in men and from 9.7 mm to 12 mm in women. In general, the bone thins as it extends distally from the external occipital protuberance and it also moves laterally from the midline. The structures at risk during screw placement include the venous sinuses. Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
References:
- Ebraheim N, Lu J, Biyani A, et al: An anatomic study of the thickness of the occipital bone: Implications for occipitocervical instrumentation. Spine 1996;21:1725-1729.
Question 96High Yield
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction. Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220. Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
References:
- Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 97High Yield
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?

Explanation
Ample evidence supports an increased rate of degenerative arthritis in the ACL-deficient knee. Several variables play a role in the development of the arthritis, but the integrity of the meniscus has been shown to be the single most important factor. O'Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118. Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
Question 98High Yield
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Explanation
Explanation
6b 6c 6d 6e Although the imaging studies are consistent with a unicameral bone cyst, aneurysmal bone cyst, or giant cell tumor, the histology shows small round blue cells that are typical of Ewing's sarcoma. Although Ewing's sarcoma frequently occurs in the diaphysis, it can occur in the metaphysis.
References:
- Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 99High Yield
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 100High Yield
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
Explanation
Treatment of patients with unplanned excision of soft-tissue sarcomas is challenging. If the margins are positive or unclear, the patient is best managed with repeat excision of the tumor bed, and radiation therapy if the repeat excision does not yield wide margins. In patients with no detectable tumor on physical examination or imaging after unplanned excision, some studies have shown that up to 35% of patients will have residual disease and a poorer local recurrence rate (22% versus 7%). Therefore, whenever feasible, a reexcision of the tumor bed is recommended.
References:
- Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
