Orthopedic Board Review: 100 High-Yield MCQs | Mock Exam Set #395
Key Takeaway
This page provides 100 high-yield orthopedic surgery multiple-choice questions (MCQs) for ABOS, OITE, and FRCS board exam preparation. Surgeons can use this comprehensive mock exam, Set 395, to test their knowledge and master critical concepts for successful certification.
Minimally Invasive Surgery for Precise Retrog...
00:00
Start Quiz
What is the structure indicated by the letter "A" in Figure 21?

Explanation
The ligaments shown are the components of the lateral collateral ligament complex, and the structure indicated by the letter "A" is the radial collateral ligament. The lateral ulnar collateral ligament is the structure indicated by the letter "C" and the annular ligament is indicated by the letter "B." The transverse ligament is a component of the medial collateral ligament complex. Morrey BF: Anatomy of the elbow joint, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 30.
- Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 3High Yield
What nerve is most likely to be injured during the anterior exposure of C2-3?
Explanation
Explanation
The hypoglossal nerve exits from the ansa cervicalis at approximately the C2-3 level and can be injured during retraction up to the C2 level. The superior laryngeal nerve lies at about C4-5. The facial nerve is much higher. The vagus nerve runs with the internal jugular and carotid much more laterally. The phrenic nerve exits posteriorly. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.
Question 4High Yield
Which of the following is considered a major characteristic of hyaluronate?
Explanation
Hyaluronate is a naturally occurring compound that is the backbone of the central core of the proteoglycan aggregate. Cartilage is made of two principal tissue structures. The connective tissue component includes collagen, which forms the framework for structural strength and elasticity. The proteoglycan aggregate provides a unique property of water incorporation and friction reduction capabilities. Hyaluronate forms the base or central core of the aggregate on which a link protein binds a protein core. Chondroitin sulfate and keratin sulfate are then bound to this protein core, forming the terminal extension of the aggregate. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78. Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Question 5High Yield
Which of the following statements about injury of the anterior vascular structures during lumbar disk surgery is true?
Explanation
Explanation
Vascular injury most commonly occurs at L4-L5, followed by L5-S1 and are associated with use of the pituitary rongeur. Hohf reported that 17 of 58 patients died as a result. Early recognition and treatment of this complication is vital; unfortunately, intraoperative bleeding from the disk space may occur in up to 50% of these patients. Some may be first recognized in the recovery room. Common clinical findings include hypotension, tachycardia, and a rigid abdomen. Formation of an arteriovenous fistula is the most common vascular injury resulting from lumbar disk surgery but is usually not recognized until months after surgery. Cardiomegaly and high output cardiac failure are common presenting symptoms. Hohf RP: Arterial injuries occurring during orthopaedic operations. Clin Orthop 1963;28:21-37. Montorsi W, Ghiringhelli C: Genesis, diagnosis and treatment of vascular complications after intervertebral disk surgery. Int Surg 1973;58:233-235.
References:
- Stambough JL, Simeone FA: Vascular complications in spine surgery, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 6High Yield
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O'Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
Explanation
Throwing athletes with symptomatic internal rotation deficits often benefit from an intensive posterior capsular stretching program. Patients that fail to respond to nonsurgical management may benefit from an arthroscopic posterior capsular release. Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
References:
- Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 7High Yield
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Recent evidence has shown that the position of immobilization of the shoulder after a dislocation influences the reduction of the Bankart lesion. In an MRI study in patients who sustained an anterior dislocation, the Bankart lesion was reduced to the glenoid anatomically with the arm in 30 degrees of external rotation. Subsequently, a clinical follow-up study has shown a reduction in recurrence rates when the arm is immobilized in external rotation compared to internal rotation. Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Question 8High Yield
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 9High Yield
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Although management of shoulder pain in the throwing athlete is controversial, there are some general principles. Initial management generally includes rest from throwing, restoring normal joint function, specifically motion and strength as well as eliminating pain. In this patient, examination reveals excessive external rotation and decreased internal rotation. This pattern is common in pitchers; however, the total arc of motion should remain close to 180 degrees in abduction. In this patient, the total arc is 140 degrees. Treatment should first focus on restoring a 180-degree arc with posterior scapular stretching, as well as pain control and muscle rehabilitation. Injections and surgery are generally reserved for patients who fail to respond to rest and rehabilitation.
Question 10High Yield
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
The history and presentation are consistent with type I Charcot-Marie-Tooth (CMT), the most common form of hereditary peripheral motor sensory neuropathy. Type I CMT is the most common, occurring in 50% of patients with CMT, and is characterized by marked slowing of motor neuron velocities, and inconsistent slowing of sensory neuron velocities. Peroneus longus to brevis transfer is indicated to release the overpull of the peroneus longus, and restore the eversion and dorsiflexion function of the peroneus brevis. A lateralizing calcaneal osteotomy with proximal translation is indicated to correct heel varus given that the Coleman block only allows for partial correction of heel varus. Proximal translation of the posterior tuber corrects for the increased calcaneal dorsiflexion, improving the lever arm for the triceps surae. A medial column closing wedge osteotomy is often required to correct a rigid, or semirigid plantar flexed first ray to allow for a balanced, plantigrade foot. Triple arthrodesis is indicated for rigid, arthritic hindfoot deformities. Transfer of the posterior tibial tendon to the tibialis anterior is not indicated since it is an out-of-phase transfer. Transfer of the posterior tibial tendon, when performed, should be to the lateral aspect of the foot. A medializing calcaneal osteotomy would accentuate the heel varus. There is no indication for Botox in CMT; Botox injection of the calf would further weaken push-off during gait. Bracing of a progressive semirigid or rigid deformity is not recommended. Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315. Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Question 11High Yield
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?
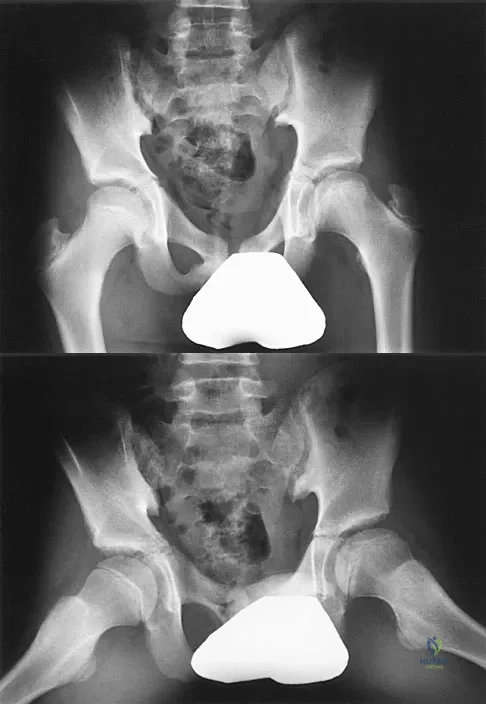
Explanation
The radiographs show a child with Legg-Calve-Perthes disease (LCPD) that has healed. Deformity (asphericity) of the femoral head is evident, but the femoral head and acetabulum are congruous. Stulberg and associates found that hips with aspherical congruity at skeletal maturity functioned well until the fifth or sixth decade of life. Similarly, another study found that degenerative arthritis caused deteriorating hip function after age 40 years in patients with this degree of residual deformity. Repeated episodes of ischemic necrosis are unlikely. Although some studies suggested coagulation abnormalities such as protein C and S deficiencies in children with LCPD, other studies failed to show any evidence of inherited thrombophila in most children with this disorder. There are no studies to suggest growth acceleration occurs following LCPD. Stulberg SD, Cooperman DR, Wallenstein R: The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:479-489.
Question 12High Yield
What gene is expressed the earliest during the differentiation of a chondrocyte during endochondral ossification?
Explanation
Transcription factors regulate the activation or repression of cartilage-specific genes. Sox-9, considered a major regulator of chondrogenesis, regulates several cartilage-specific genes during endochondral ossification, including collagen types II, IV, and XI and aggrecan. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 13High Yield
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?

Explanation
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Question 14High Yield
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
Explanation
Explanation
16b The MRI scans show a rupture of the sternocostal portion of the pectoralis major tendon. This is the most common site of rupture and bench pressing is the most common etiology. Surgical repair yields better functional outcomes and patient satisfaction for tears not only at the tendon/bone interface but also at the myotendinous junction. Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.
References:
- Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 15High Yield
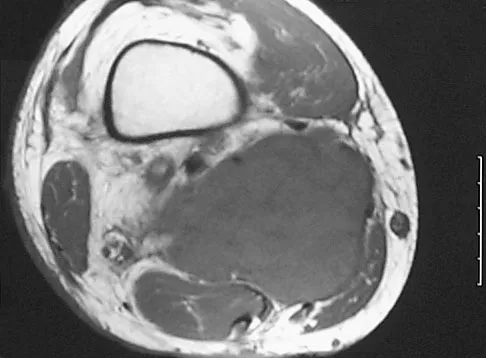
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan shows near complete involvement of the femoral head with bone marrow changes and some collapse of the necrotic segment. This is most suggestive of osteonecrosis.
References:
- Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997.
Question 16High Yield
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of
Explanation
Explanation
8b The MRI scans reveal a severe avulsion injury of the adductor muscle from the pubic ramus with muscle edema and hemorrhage. Injury to the adductor muscle group, a "pulled groin," is caused by forceful external rotation of an abducted leg. Pain is immediate and severe in the groin region. Tenderness is at the site of injury along the subcutaneous border of the pubic ramus. Treatment is dictated by the severity of the symptoms but generally consists of rest, ice, and protected weight bearing, followed by a rehabilitation program that begins with gentle stretching and progresses to resistance exercise with a gradual return to sports. Immobilization should be avoided because this promotes muscle tightness and scarring. No data exist to suggest that open repair yields a better outcome than nonsurgical management. Tenotomy has been performed in high-level athletes with chronic groin pain following injury. Gilmore J: Groin pain in the soccer athlete: Fact, fiction, and treatment. Clin Sports Med 1998;17:787-793.
References:
- Irshad K, Feldman LS, Lavoie C, et al: Operative management of "hockey groin syndrome": 12 years of experience in National Hockey League players. Surgery 2001;130:759-766.
Question 17High Yield
A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?
Explanation
Explanation
This is a classic C6 nerve injury, and it is most likely the result of a herniated nucleus pulposus at C5-6. The C5 nerve root controls the elbow flexors, shoulder abductors, and external rotators. The C7 nerve root controls the elbow extensors, wrist pronators, and the triceps reflex. Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.
Question 18High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303. Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
References:
- Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 19High Yield
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?

Explanation
Chronic anterior inferior tibiofibular ligament sprains can lead to thickening and synovitis that catches or impinges dorsiflexion; patients often note painful clicking with dorsiflexion eversion. The other structures are not affected by this injury. Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH: Syndesmosis sprains of the ankle. Foot Ankle 1990;10:325-330. Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50. Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Question 20High Yield
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
Radiographic fusion success rates are best described as slightly rather than substantially improved. Hospital stay and time to fusion also are not substantially decreased. Use of BMP does eliminate the need for autograft harvest for anterior lumbar interbody fusion/cage. The need for postoperative bracing is not altered based on graft choice. Early studies of posterolateral fusion applications appear to show a greater potential benefit of rhBMP-2 over autograft. Not all BMP formulations perform the same with regard to safety and effectiveness. Other osteoinductive proteins in clinical trials (BMP-7, GDF-5) will require individual analysis of these properties.
Question 21High Yield
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?
Explanation
Explanation
The MRI scan shows disruption of the subscapularis muscle. Subscapularis rupture is associated with weakness in internal rotation as shown with a positive lift-off test as described by Gerber and Krushell. The belly press test also has been shown to be a useful clinical test for this problem. Weakness in external rotation and abduction is more consistent with supraspinatus and infraspinatus tears. Deltoid atrophy is associated with an axillary nerve injury. Loss of biceps contour is associated with rupture of the long head of the biceps. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Greis PE, Kuhn JE, Schultheis J, et al: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 22High Yield
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
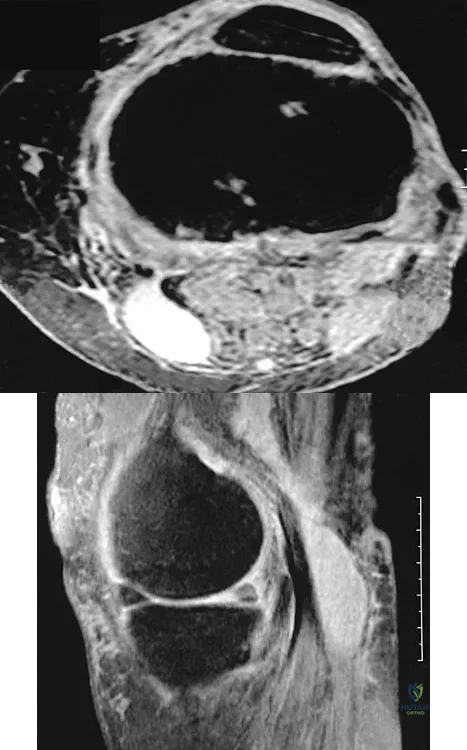
Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 23High Yield
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
Explanation
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL. Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
References:
- McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 24High Yield
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
Explanation
Success of a meniscal allograft transplantation is strongly dependent on accurate graft sizing, typically within 5% of the native meniscus. Previous studies have established that donor cell viability is not mandatory for the survival of these grafts since they are replaced by the recipient's cells (at least peripherally) within several weeks. Thus, cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated. Wirth CA, Kohn D: Meniscal transplantation and replacement, in Fu FH, Harner CD, Vince JG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, vol 1, pp 631-641. Brautigan BE, Johnson DL, Caborn DM, et al: Allograft tissues, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 205-213.
References:
- Shaffer B, Kennedy S, Klimkiewicz J, et al: Preoperative sizing of meniscal allografts in meniscus transplantation. Am J Sports Med 2000;28:524-533.
Question 25High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by

Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 26High Yield
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 27High Yield
A previously healthy 14-year-old boy now reports fatigue, and has a bilateral Trendelenburg gait, right hip pain, and bilateral knee and foot pain. Biopsy of a right sacral mass reveals intermediate grade osteosarcoma. There are no metastases. Laboratory studies reveal a serum calcium level of 7.7 mg/dL (normal 8.5 to 10.5), a phosphate level of 2.0 mg/dL (normal 2.7 to 4.5), a 1,25-dihydroxyvitamin D level of less than 10 pg/mL (normal 18 to 62), a parathyroid hormone level of 19 pg/mL (normal 10 to 60), and an alkaline phosphatase level of 428 U/L (normal 15 to 351). What is the most likely cause of the patient's symptoms?
Explanation
The laboratory findings are typical for rickets. Oncogenic rickets is a paraneoplastic syndrome that results from a substance secreted by the tumor that interferes with renal tubule reabsorption of phosphate. This substance previously had been called phosphatonin but recently has been identified as fibroblast growth factor 23. Nutritional rickets is rare in developed countries. Delayed onset familial hypophosphatemic rickets is possible, but the likelihood of having two rare diseases is unlikely. Osteosarcoma does not sequester calcium. Alkaline phosphatase levels can be elevated in osteosarcoma but does not cause muscle weakness. Tumor cachexia would occur only with advanced metastatic disease. A unilateral sacral mass would not cause a bilateral L5 neuropathy or the abnormal laboratory findings. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 29-2001. A 14-year-old with abnormal bones and a sacral mass. N Engl J Med 2001;345:903-908.
Question 28High Yield
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
Explanation
With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Question 29High Yield
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
References:
- Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 30High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 31High Yield
Which of the following best describes the course of the median nerve at the elbow?

Explanation
The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 32High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted. Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
References:
- Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 33High Yield
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?

Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 34High Yield
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
Explanation
Anteversion of the humeral component may result in anterior instability of the component. Posterior instability after total shoulder arthroplasty is usually the result of some combination of the following factors: untreated anterior soft-tissue contractures, excessive posterior capsular laxity, and excessive retroversion of the humeral and/or glenoid components. Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
References:
- Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 35High Yield
The anticoagulant effect of the low-molecular-weight heparins (LMWH) is mediated by the binding affinity of antithrombin III to which of the following coagulation factors?

Explanation
Standard heparin mediates its anticoagulant effect largely through its interaction with antithrombin III. A conformational change in antithrombin III occurs that markedly accelerates its ability to inactivate the coagulation enzymes thrombin factor (II), factor Xa, and factor IXa. In contrast, LMWHs do not contain the necessary saccharide units to bind thrombin and antithrombin III simultaneously. The anticoagulant effect of LMWHs involves binding of antithrombin III to factor Xa.
Question 36High Yield
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm3. Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of
Explanation
Explanation
This clinical situation requires careful analysis because some data suggest infection and some a noninfectious inflammatory process. Bilateral hip involvement, the absence of significant fluid collection or fever, the streptozyme level, and the history of upper respiratory infection all suggest poststreptococcal toxic synovitis as the most likely cause for the clinical presentation. In the first 24 hours, this type of presentation might warrant incision and drainage given uncertainty of the diagnosis and the risks associated with missing an infection. However, 5 days after onset, surgery is not warranted, especially given that the patient remains afebrile and her symptoms are improving. Cardiology consultation would be appropriate. There is no evidence to suggest slipped capital femoral epiphysis. Treatment with antibiotics is not advised because there is no bacteriologic data on which to base treatment. De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
References:
- Haueisen DC, Weiner DS, Weiner SD: The characterization of "transient synovitis of the hip" in children. J Pediatr Orthop 1986;6:11-17.
Question 37High Yield
A 55-year-old woman fell and sustained an elbow dislocation with a coronoid fracture and a radial head fracture. The elbow is reduced and splinted. What is the most common early complication?

Explanation
The patient has a dislocation of the elbow with displaced coronoid process and radial head fractures. The elbow is extremely unstable after this injury, and recurrent dislocation in a splint is the most common early complication. Skeletal stabilization of the fractures is required to restore stability of the joint. Characteristics of the fractures will determine the techniques required to restore stability. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 38High Yield
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10 degrees of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
Explanation
17b The radiograph and MRI scan show osteochondritis dissecans of the capitellum, and the patient's history suggests a loose body. The treatment of choice is arthroscopic removal of the loose body and microfracture of the crater. Excision of the radial head, a cortisone injection, or tennis elbow release does not treat the pathology in the capitellum. Nonsurgical treatment would not relieve the mechanical symptoms of the loose body or promote healing in the crater. Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-530. Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast's elbow. Arthroscopy 1989;5:129-136.
References:
- Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow. Arthroscopy 1998;14:797-803.
Question 39High Yield
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
References:
- Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 40High Yield
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically. Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 41High Yield
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel's sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
Explanation
The patient has entrapment of the superficial peroneal nerve against its fascial opening in the distal leg. It is typically exacerbated by passive or active plantar flexion and inversion of the foot, which leads to traction of the nerve as it exits this opening. Treatment involves release of the fascial opening to reduce this traction phenomenon. Closure of the defect will only aggravate the condition and potentially result in an exertional compartment syndrome. A four-compartment fasciotomy is only indicated for an established compartment syndrome of the leg. Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169. Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
References:
- Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression. J Bone Joint Surg Br 1989;71:131-135.
Question 42High Yield
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?

Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 43High Yield
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
Explanation
35b In an adult with an anterior cortical tibial lesion, this is the classic histologic appearance and anatomic location for an adamantinoma. The histology reveals areas of epithelial cells (in a glandular pattern) within a fibrous stroma. The epithelial cells are shown in nests. They would stain positively for keratin. Adamantinoma is a rare malignant bone tumor with a propensity for late metastasis. It has a high incidence of local recurrence unless resected with a wide margin. Chemotherapy and radiation therapy are not helpful in the treatment of this disease. Amputation generally is not necessary because a diaphyseal resection is usually possible. McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
References:
- Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 44High Yield
A 19-year-old woman has a painful right knee. A radiograph, MRI scan, CT scan, and histopathologic specimen are shown in Figures 24a through 24d. What is the most likely oncologic stage of the lesion?
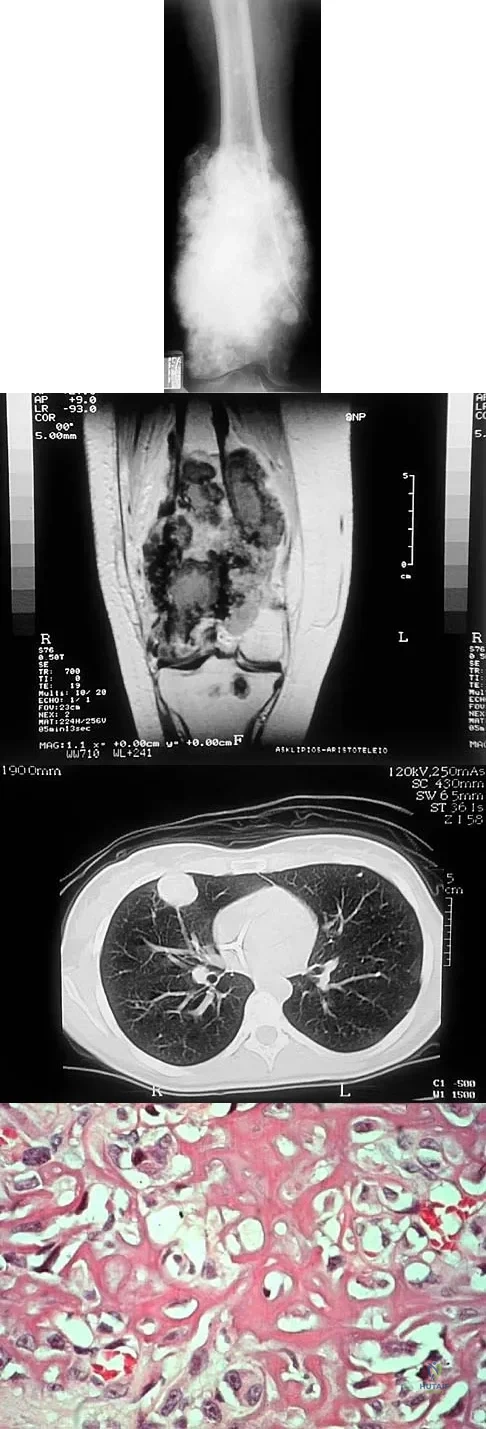
Explanation
The patient has a high-grade osteosarcoma of the distal femur with a skip lesion, and pulmonary metastasis is seen on the CT scan. This corresponds to a stage III lesion according to the Musculoskeletal Tumor Society System as adopted from Enneking.
Question 45High Yield
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Explanation
Explanation
39b 39c 39d 39e The lesion is a chondroblastoma. The plain radiographs show a well-defined radiolucent lesion in the distal femoral epiphysis of a skeletally immature patient. The margins are well defined, suggesting a benign growth. The epiphysis is an unusual location for bone tumors, except for chondroblastomas. Of all chondroblastomas, 95% are located within the epiphysis. The MRI scans show a punctate appearance that is commonly seen in cartilage lesions. The biopsy specimen shows a chondroid lesion with polygonal chondrocytes. These findings are consistent with a chondroblastoma. The natural history of chondroblastomas is for continued growth and bone destruction if left untreated. Treatment should consist of curettage, with or without the use of physical or chemical adjuvants, and bone grafting.
References:
- Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 46High Yield
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Explanation
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
References:
- Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 47High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with

Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 48High Yield
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?

Explanation
Type I fractures are trochanteric fractures usually secondary to osteolysis. Type II fractures are located around the stem. Type III fractures are distal to the stem. If the fracture and prosthesis are stable, the fracture can be treated nonsurgically. If the fracture is unstable, the stability of the prosthesis should be assessed. If the prosthesis is unstable (type IIB), treatment should consist of revision to a long stem prosthesis that bypasses the fracture by two cortical diameters. If, as in this patient, the prosthesis is not loose (type IIA), open reduction and internal fixation is the appropriate option. Proximal femoral allograft is appropriate for type IIIC fractures in which the proximal bone is significantly compromised and the femoral component is loose. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 49High Yield
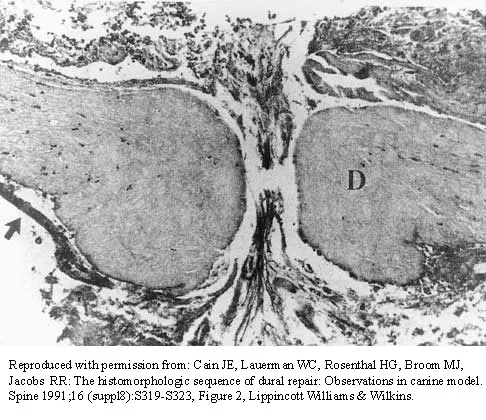
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of
Explanation
During the initial healing phases of a dural tear, pia and arachnoid from adjacent nerve roots migrate, fill the dural defect, and create a pia-arachnoid plug. It is this initial plugging of the defect that is believed to prevent further egress of cerebrospinal fluid through the defect. The plug has been shown to develop by the second postoperative day. Fibroblastic proliferation occurs within the dura itself and accounts for the bulbous ends of the dura seen in the photomicrograph. The appearance of the material within the dural edges is inconsistent with the appearance of neural elements, and scar tissue formation occurs later in the healing process. Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 50High Yield
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
Explanation
The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
References:
- Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 51High Yield
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
Explanation
In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture. Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 144-148.
References:
- Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 52High Yield
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
Explanation
Explanation
This is a very large near circumferential defect with posterior as well as anterior skin and muscle injury. Bone is exposed. The posterior muscles cannot be rotated since they are part of the zone of injury. The bone and other poorly vascularized areas of this wound would not accept a skin graft. The best chance for limb salvage will be to obtain soft-tissue coverage with a free tissue transfer using the latissimus dorsi. Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
References:
- Bos GD, Buehler MJ: Lower-extremity local flaps. J Am Acad Orthop Surg 1994;2:342-351.
Question 53High Yield
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
Explanation
The size of the rotator cuff tear in both anteroposterior and mediolateral dimensions has been found to correlate best with outcome. Older patient age and rupture of the long head of the biceps tend to be associated with larger tears and, therefore, may be associated indirectly with a poorer outcome. Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 54High Yield
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing's sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
Explanation
The current treatment regimen for Ewing's sarcoma typically involves induction chemotherapy followed by local control and further chemotherapy. Local control consists of surgery only, radiation therapy only, or a combination of the two. In bones that are easily resectable (expendable) with wide margins, surgery is usually recommended. For areas that cannot be resected (ie, large bulky pelvic tumors), radiation therapy alone is sometimes the preferred method of local control. If surgery is chosen and the margins are close, radiation therapy can be used as an adjuvant treatment. Amputation is rarely required for an isolated fibular lesion. Observation without adequate local control results in local recurrence. Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing's sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
References:
- Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 296.
Question 55High Yield
A healthy 52-year-old woman is seeking professional advice about management of osteoporosis. She has no risk factors for osteoporosis. What is the best recommendation for bone health for this patient?
Explanation
Women older than age 50 years should receive daily supplementation with calcium and vitamin D to help preserve bone density. Bone mineral density testing is recommended for women age 65 years or older and postmenopausal women with at least one risk factor for osteoporotic fractures: prior fragility fracture, low estrogen levels, premature menopause, long-term secondary amenorrhea, glucocorticoid therapy, maternal history of hip fracture, or low body mass index. Hormone therapy is not approved for the treatment of osteoporosis. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 56High Yield
A 6-year-old girl has never been able to crawl or walk and can sit only when propped. History reveals no complications during pregnancy or delivery. Examination reveals a 30-degree scoliosis from T4 to L3. Deep tendon reflexes are absent, but fasciculations are present. The most likely genetic defect is the result of an abnormality in
Explanation
Explanation
The patient's findings are consistent with an intermediate form of spinal muscular atrophy. Children with this condition appear normal at birth but are not able to walk. The disorder affects anterior horn cells. Fasciculations may be present, but deep tendon reflexes are typically absent. The development of scoliosis is almost universal with this type of spinal muscular atrophy. More than 90% of patients with spinal muscular atrophy have deletions in the telomeric survival motor neuron gene. Peripheral myelin protein 22 is abnormal in Charcot-Marie-Tooth type IA. Connexin 32 is abnormal in the X-linked type of Charcot-Marie-Tooth disease. Neurofibromin is affected in neurofibromatosis type 1. Friedreich's ataxia is secondary to a disorder of frataxin. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
References:
- Thompson GH, Berenson FR: Other neuromuscular disorders, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 633-676.
Question 57High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?

Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 58High Yield
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?

Explanation
A chordoma is a malignant neoplasm originating from remnants of the notochord. It is usually localized to the midline with 50% at the sacrococcygeal area, 35% at the skull base, and 15% at the mobile portion of the spine. Large vacuolated cells (physaliferous cells) are a characteristic of the tumor. Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Question 59High Yield
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?
Explanation
Explanation
2b In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise. Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608. Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208. Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.
References:
- Baumgaertner MR, Tornetta P III (eds): Orthopaedic Knowledge Update: Trauma 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 65-74.
Question 60High Yield
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of

Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 61High Yield
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?

Explanation
Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH ("athlete's heart") from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm). Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete's heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436. Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Question 62High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 63High Yield
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 64High Yield
Femoral osteotomy for dysplasia of the hip will most likely result in
Explanation
Explanation
Patients should expect pain relief after femoral osteotomy for hip dysplasia. Patients should not expect improved motion or abduction strength and should be counseled about a postoperative limp and unequal limb lengths. Pellicci PM, Hu S, Garvin KL, Salvati EA, Wilson PD Jr: Varus rotational femoral osteotomies in adults with hip dysplasia. Clin Orthop 1991;272:162-166.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 65High Yield
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?
Explanation
Explanation
19b Following a calcaneal fracture, the patient has severe subtalar arthritis with loss of talar declination and shortening of the heel; therefore, the treatment of choice is subtalar distraction arthrodesis. Orthotics will not provide significant relief as bracing has failed. Ankle arthrodesis will not be beneficial because the arthritis is in the subtalar joint. Subtalar arthroscopy would only be helpful for a small area of arthrosis, and calcaneal osteotomy would not be beneficial given the extent of the arthritis of the subtalar joint.
References:
- Robinson TF, Murphy GA: Arthrodesis as salvage for calcaneal avulsions. Foot Ankle Clin 2002;7:107-120.
Question 66High Yield
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?

Explanation
An isolated tear of the subscapularis tendon has been noted as early as 1835 by Smith. In Gerber and associates' 1991 report of 16 men with an average age of 51 years, isolated subscapularis tendon rupture was often caused by a violent hyperextension injury. All patients reported pain anteriorly along with night pain. They also noted pain and weakness of the arm. The lift-off test is performed by having the patient lift the palm of the hand away from the small of the back. The patient must have sufficient internal rotation to allow this test to be performed. A subscapularis rupture is likely if the patient cannot perform the lift-off test. Hertel R, Ballmer FT, Lombert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394. Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 67High Yield
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of

Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Question 68High Yield
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
Advances in development of new tumor markers and techniques of antigen retrieval have enhanced the sensitivity and reliability of identifying the primary source of metastasis. New markers such as CK7, CK20, CA125, and thyroid transcription factor-1 (TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene). Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Question 69High Yield
The strongest biomechanical construct for open reduction and internal fixation of a talar neck fracture uses what interval and entry point?
Explanation
The strongest biomechanical construct is posterior to anterior fixation with the entry point being at the level of the posterolateral tubercle of the talus. This uses the interval between the peroneus brevis and the flexor hallucis longus. The interval between the flexor digitorum longus and the flexor hallucis longus with entry at the posteromedial tubercle of the talus is not an accepted approach for fixation of talar neck fractures. All of the other options use screw placements from anterior to posterior. Swanson TV, Bray TJ, Homes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Question 70High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
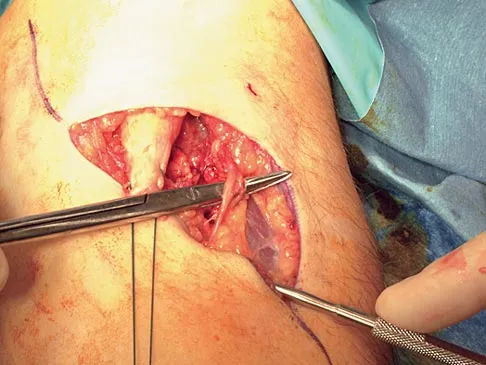
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Question 71High Yield
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
Explanation
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
References:
- Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 72High Yield
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of
Explanation
Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
References:
- Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 73High Yield
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
Explanation
16b 16c 16d 16e The imaging studies are consistent with a chondrosarcoma. The radiograph shows a radiolucent lesion in the pelvis, and there are stippled calcifications on the CT scan. The histology shows a low-grade cellular hyaline cartilage neoplasm with stellate, occasionally binucleated chondrocytes. Enchondroma has a more benign histologic appearance.
References:
- Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 74High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 75High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?

Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 76High Yield
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
Explanation
Alendronate is a second-generation bisphosphonate, and it can cause epigastric distress in up to 30% of patients. This side effect can be minimized by gradually building up to therapeutic doses over a period of 4 to 8 weeks. Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
References:
- Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 77High Yield
A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the most likely diagnosis?
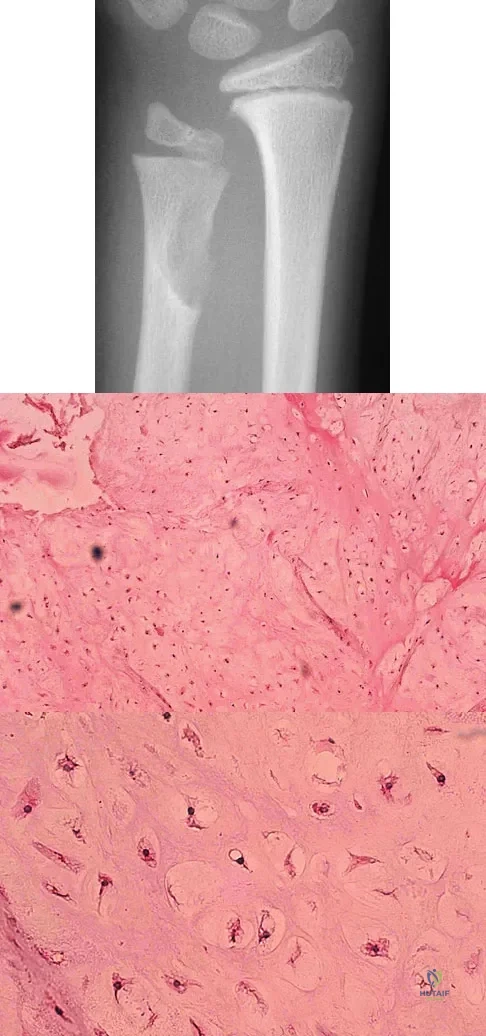
Explanation
The radiograph shows a benign-appearing cortically based lesion eroding the underlying cortex, producing a saucer-shaped defect typical of a periosteal chondroma. The histology shows benign-appearing neoplastic cartilage. Although enchondroma would have the same histologic appearance, radiographs generally show a lesion with a central medullary epicenter. The benign-appearing histology does not support chondrosarcoma. Chondromyxoid fibroma will generally show histologic elements of its fibrous and myxoid components. Chondroblastoma typically demonstrates histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification. Schajowicz F: Tumors and Tumorlike Lesions of Bone: Pathology, Radiology, and Treatment, ed 2. Berlin, Springer-Verlag, 1994, pp 147-151.
Question 78High Yield
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
Explanation
Cervical laminectomy is an accepted treatment for multilevel cervical spondylotic myelopathy. When the compression is posterior, laminectomy addresses it directly; when the compression is anterior, it is addressed indirectly (the spinal cord floats posteriorly away from the anterior compression). Preexisting kyphosis is a contraindication to laminectomy because the cord is unable to float posteriorly away from the anterior compression, and the risk for increasing kyphosis is significant. Kyphosis after laminectomy is more likely to develop in younger patients who have fewer degenerative changes to stabilize the spine. Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 79High Yield
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?
Explanation
Explanation
59b 59c 59d This classic case of osteosarcoma illustrates the typical radiographic and histologic characteristics of this disease. The radiographs show an aggressive-appearing lesion of the distal femur. The lesion has both lytic and blastic areas. Periosteal reaction is present in the form of a Codman's triangle. The radiographs are highly suggestive of osteosarcoma. The photomicrographs show malignant spindle cells that produce osteoid, thus confirming the diagnosis of osteosarcoma. Treatment of osteosarcoma is multimodal including multi-agent chemotherapy and surgery (wide resection or amputation). Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
References:
- Mankin HJ, Hornicek FJ, Rosenberg AE, et al: Survival data for 648 patients with osteosarcoma treated at one institution. Clin Orthop Relat Res 2004;429:286-291.
Question 80High Yield
What is the most common pediatric soft-tissue sarcoma?

Explanation
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
Question 81High Yield
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option. Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Question 82High Yield
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 83High Yield
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of
Explanation
Explanation
28b The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture. Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
References:
- Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 84High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 85High Yield
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?

Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 86High Yield
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component. Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348. Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491. Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Question 87High Yield
A Canale view best visualizes which of the following structures?

Explanation
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 88High Yield
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
Explanation
The string passes under the ligamentum flavum as it runs from the posterior aspect of the vertebra above to the inferior aspect of the vertebra below in the sagittal midline. This is an important structure in diskectomy and in posterior approaches to the thoracolumbar spine and neural elements. It is rarely visualized in its entirety because typical exposures provide only a limited view.
References:
- Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, p 1465.
Question 89High Yield
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?

Explanation
Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann's angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs. Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45. Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Question 90High Yield
When performing an arthroscopic subacromial decompression, bleeding can be encountered when dividing the coracoacromial ligament because of injury to what artery?
Explanation
The acromial branch of the thoracoacromial trunk courses along the coracoacromial ligament. This artery enters the ligament approximately 5 mm below the acromial edge. Division of the ligament at its insertion on the acromion minimizes the risk of bleeding. Esch JC, Baker CL: Arthroscopic anatomy and normal variations, in Whipple TL (ed): Surgical Arthroscopy: The Shoulder and Elbow. Philadelphia, PA, JB Lippincott, 1993, pp 63-76.
Question 91High Yield
A 72-year-old woman who underwent right total hip arthroplasty 7 years ago now reports right hip pain and limb shortening. Studies for infection are negative. AP and lateral radiographs are shown in Figures 13a and 13b. What is the most appropriate management?
Explanation
Explanation
13b Current literature supports the use of reinforcement cages for the reconstruction of failed, loosened acetabular components associated with major bone loss as seen in this patient. Although results of revision using the so-called jumbo cup with screws generally have been good, the amount of bone loss and medial wall penetration shown here and the likelihood of pelvic discontinuity precludes the use of that technique. With either technique, bone grafting of remaining defects is recommended. Sporer SM, O'Rourke M, Paprosky WG: The treatment of pelvic discontinuity during acetablular revision. J Arthroplasty 2005;20:79-84.
References:
- Paprosky WG, O'Rourke M, Sporer SM: The treatment of acetabular bone defects with an associated pelvic discontinuity. Clin Orthop 2005;441:216-220.
Question 92High Yield
In Figure 49, line AB connects the anterior arch of C1 to the posterior margin of the foramen magnum. Line CD connects the anterior margin of the foramen magnum to the posterior arch of C1. What is the normal ratio of displacement from CD to AB (Power's ratio)?
Explanation
Explanation
The ratio of displacement from CD to AB normally equals 1.0. If the ratio is greater than 1.0, an anterior atlanto-occipital dislocation may exist. Ratios slightly less than 1.0 are normal except in posterior dislocations, fractures of the odontoid process or ring of the atlas, or congenital abnormalities of the foramen magnum. In these conditions, the ratio may approach 0.7. Powers B, Miller MD, Kramer RS, et al: Traumatic anterior atlanto-occipital dislocation. Neurosurgery 1979;4:12-17.
References:
- Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 93High Yield
Figure 29 shows the radiograph of a 10-year-old boy who injured his knee playing football. What is the most appropriate initial treatment?
Explanation
Explanation
Salter type I fractures of the distal femur are quite unstable; therefore, closed reduction and cast immobilization can be expected to result in high rates of redisplacement. Optimal treatment consists of open or closed reduction and smooth pin fixation, and supplemental casting is required to ensure fracture stability. Screw fixation may increase rates of growth plate injury. Blade plate or flexible nail fixation will be challenging to apply and is not necessary. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Thomson JD, Stricker SJ, Williams MM: Fractures of the distal femoral epiphyseal plate. J Pediatr Orthop 1995;15:474-478.
Question 94High Yield
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
Explanation
CT of the abdomen and pelvis is not part of the staging of osteosarcoma. Staging studies should consist of CT of the chest, radiographs of the chest and primary tumor, MRI of the primary tumor, and a bone scan. The MRI should be obtained prior to the biopsy.
References:
- O'Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 95High Yield
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
References:
- Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 96High Yield
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
Explanation
Explanation
Emboli are created during TKA. Usually there is an increased incidence with the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury. Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232. Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
References:
- McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.
Question 97High Yield
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
Explanation
In a multivariate analysis, the strongest factor for the development of compartment syndrome is fracture of the proximal third of the forearm. However, compartment syndrome can still occur without a fracture. Therefore, these patients should be followed with a high level of suspicion for the development of compartment syndrome. Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
References:
- Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 98High Yield
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?

Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 99High Yield
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
Continuous fluoroscopy and cine radiography expose the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Question 100High Yield
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?

Explanation
Congenital vertical talus is a fixed dorsal dislocation of the talonavicular joint with equinus of the ankle joint. The AP radiograph shows valgus of the midfoot and an increased talocalcaneal angle; the lateral radiograph shows a vertically positioned talus and equinus of the ankle joint, and the plantar flexion lateral view shows that the talonavicular joint does not reduce. A line drawn through the long axis of the talus passes below the long axis of the first metatarsal. Initial management should consist of serial casting to stretch the dorsal soft-tissue structures; surgery eventually will be required to reduce the talonavicular joint. The differential diagnosis of congenital vertical talus includes pes calcaneovalgus, flexible pes planus, and peroneal spastic flatfoot. Pes calcaneovalgus, flexible pes planus, congenital short Achilles tendon, and peroneal spastic flatfoot would not show resistent dorsal dislocation of the navicular on the plantar flexion view. Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
