Orthopedic Surgery Mock Exam Set 447: 100 High-Yield MCQs for Complex Cases

Key Takeaway
This page offers 100 high-yield Orthopedic Board Review MCQs, curated as Mock Exam Set #447, to help surgeons prepare and excel in ABOS, OITE, and FRCS board exams. Practice with challenging, randomized questions designed to reinforce knowledge and build confidence for complex orthopedic scenarios.
Complex Management of Chronic Infected Femora...
00:00
Start Quiz
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
- Allen GL, Ferguson RL, Lehmann TR, O'Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 3High Yield
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?

Explanation
Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient's findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis. Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
Question 4High Yield
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
References:
- Ross PD, Davis JW, Epstein RS, Wasnich RD: Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114:919-923.
Question 5High Yield
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of

Explanation
The patient has the findings of classic subacromial impingement. Initial management should consist of stretching exercises directed at the posterior capsule and a program of rotator cuff and deltoid strengthening exercises performed below the horizontal in a "safe" plane. The judicious use of subacromial cortisone injections (one or two) may be helpful. Anterior acromioplasty is reserved for patients who have failed to respond to nonsurgical management. Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737. Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Question 6High Yield
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Explanation
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure. Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607. Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 7High Yield
A 39-year-old man reports low back pain, lower extremity numbness, and urinary retention after being injured in a motor vehicle accident 1 day ago. He is able to walk but is in pain. A straight leg raise results in increased back pain, and examination reveals that perianal sensation is decreased. Placement of a urinary catheter results in 500 mL of urine. What is the next most appropriate step in management?
Explanation
Explanation
Acute cauda equina syndrome, including saddle hypesthesia and bowel/bladder incontinence, is a red flag that demands emergent evaluation with MRI and urgent surgery if compression is confirmed. Results appear to be improved if surgery is performed within 48 hours. The other treatment approaches listed are not indicated if a cauda equina syndrome is present. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522. Shapiro S: Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine 2000;25:348-351.
References:
- Kostuik JP, Harrington I, Alexander D, et al: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Question 8High Yield
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
Explanation
Many congenital limb deficiencies and bowing deformities result in growth retardation. If unilateral, a gradually progressive limb-length discrepancy will result; however, the proportional lengths of the lower extremities will remain at a relatively constant ratio. For example, if the right foot is at the level of the left knee at birth, this will still be true at maturity. This concept can be useful for early prediction of limb-length discrepancy by using a "multiplier method," as described by Paley and associates. This method can facilitate early treatment decisions, such as the need for amputation, without having to wait for serial scanography measurements. Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
References:
- Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 9High Yield
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
Explanation
The os peroneum is an accessory ossicle located within the peroneus longus tendon. It is typically located at the level of the cuboid groove in the lateral hindfoot and midfoot region. Proximal migration of the os peroneum indicates disruption of the peroneus longus tendon and is an important clue to diagnosis. This unusual condition can cause chronic lateral ankle pain, and surgical repair may be indicated. Active eversion indicates that the peroneus brevis is clinically intact. Disruption of the extensor digitorum brevis, plantar fascia, or syndesmosis would have no effect on the position of the os peroneum. Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
References:
- Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 10High Yield
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
Explanation
The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).
References:
- Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 11High Yield
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
The contracted Achilles tendon leads to increased forefoot pressure, thus increasing the risk for ulceration in neuropathic patients. Several studies have shown the benefit of Achilles tendon lengthening to heal and prevent forefoot ulceration in these patients. The flexor hallucis longus transfer is used for chronically torn/deficient Achilles tendons, not a contracted Achilles tendon. The Jones procedure works well for the first ray but does not help to alleviate pressure under the second ray. Peripheral bypass surgery is unnecessary because the ulcer healed during the initial treatment, indicating that the patient has adequate circulation. The posterior tibial tendon transfer is used for foot drop or other neuromuscular conditions to correct deformity and increase function. It is not used for forefoot ulcers in patients with diabetes mellitus. Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 12High Yield
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
Explanation
18b 18c The MRI scans reveal an enlarged posterior tibial tendon, with degenerative signal within the tendon and an excessive amount of fluid in its sheath. This is a type II tear, as noted by Conti and associates, which is the most commonly seen tear. Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
References:
- Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 13High Yield
An Asian 45-year-old man has bilateral upper extremity dysfunction. Figure 35a shows a T2-weighted sagittal MRI scan of the cervical spine, and Figure 35b shows a T2-weighted axial MRI scan at the level of the C3 vertebral body. What is the most likely pathologic process?
Explanation
Explanation
35b Although relatively common in people of Asian origin, OPLL has been reported in other races as well. The radiographic appearance can be variable as there are different types described, but some of the discerning characteristics are seen in these images. On the sagittal view, the bone posterior to the vertebral body extends along the entire length of C2 and C3. This is characteristic of OPLL, whereas cervical spondylosis and DISH more commonly are not confluent. Ankylosing spondylitis more commonly extends significantly into the spinal canal, and neurofibromatosis generally does not cause any bony growth. The axial view shows a large, oval bony projection into the spinal canal, a typical finding of OPLL. McAfee PC, Regan JJ, Bohlman HH: Cervical cord compression from ossification of the posterior longitudinal ligament in non-orientals. J Bone Joint Surg Br 1987;69:569-575.
References:
- Kricun R, Kricun ME: MRI and CT of the Spine. New York, NY, Raven Press, 1994, pp 126-130.
Question 14High Yield
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 15High Yield
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
Explanation
The goal of fluid replenishment should be to replace the sweat that has been lost. Sweat is mostly water, with a small concentration of salts and other electrolytes. Absorption is enhanced by solutions of low osmolality. Scientific research has also shown that adding carbohydrates to the drink improves athletic performance. Carbohydrates such as glucose and maltodextrins (glucose polymers) stimulate fluid absorption by the intestines. Fructose slows intestinal absorption of fluids. Drinks that are high in fructose, such as orange juice, can lead to gastrointestinal distress and osmotic diarrhea. Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
References:
- Gisolfi CV, Duchman SM: Guidelines for optimal replacement beverages for different athletic events. Med Sci Sports Exerc 1992;24:679-687.
Question 16High Yield
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?
Explanation
Explanation
Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3. Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
References:
- Freedman KB, Brookenthal KR, Fitzgerald RH, et al: A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 2000;82:929-938.
Question 17High Yield
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
Explanation
Improved peak-to-load failure data have been demonstrated by reconstruction of the sternoclavicular joint using a semitendinosis graft in a figure-of-eight pattern through the clavicle and manubrium. Resection of the medial clavicle, which compromises the integrity of the costoclavicular ligament, results in medial clavicular instability. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 608-609.
Question 18High Yield
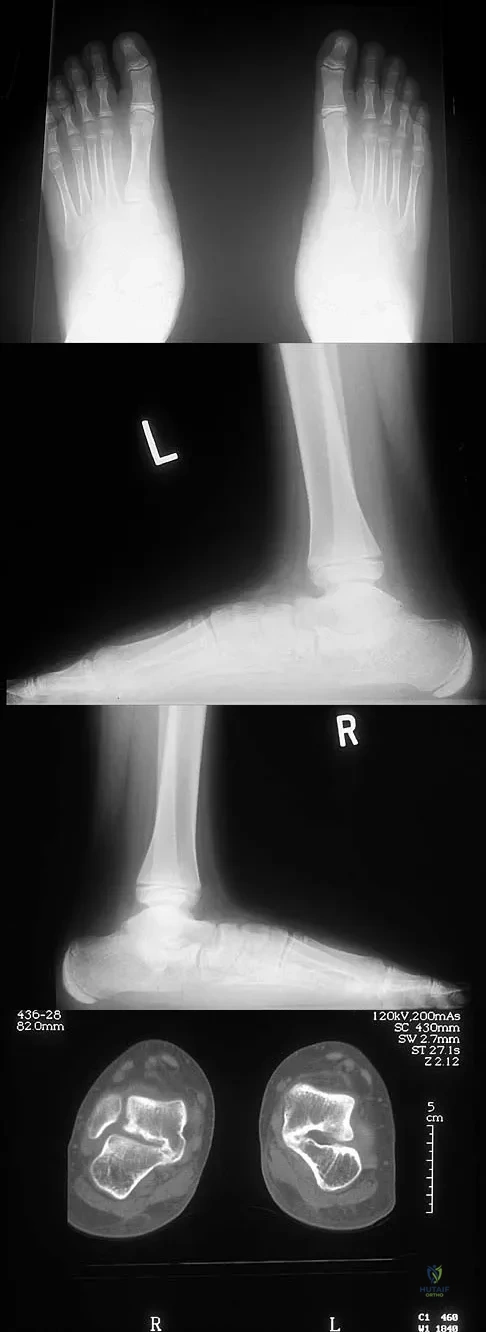
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
The axial views show fusion of the talus and calcaneus at the medial facet (talocalcaneal coalition). Peroneal spastic flatfoot is a descriptive term applying to the symptoms of painful flatfoot associated with apparent peroneal spasm and is sometimes caused by tarsal coalition; however, this is not the most appropriate diagnosis for this patient. Flexible flatfoot with a short Achilles tendon often causes symptoms similar to the ones listed above, but subtalar motion should be normal. A diagnosis of calcaneonavicular coalition can be made based on plain oblique views of the foot but is not seen in these views. Posterior tibial tendon dysfunction in the absence of other pathology is uncommon in children. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 19High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 20High Yield
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
Explanation
29b The studies show marginal syndesmophyte formation characteristic of ankylosing spondylitis. These patients typically have diffuse ossification of the disk space without large osteophyte formation. DISH typically presents with large osteophytes, referred to as nonmarginal syndesmophytes. In this patient, the zygoapophyseal joints are fused rather than degenerative as would be seen in rheumatoid arthritis, and the costovertebral joints are also fused. Osteopetrosis does not normally ankylose the disk space. McCullough JA, Transfeldt EE: Macnab's Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
References:
- Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 21High Yield
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures. Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Question 22High Yield
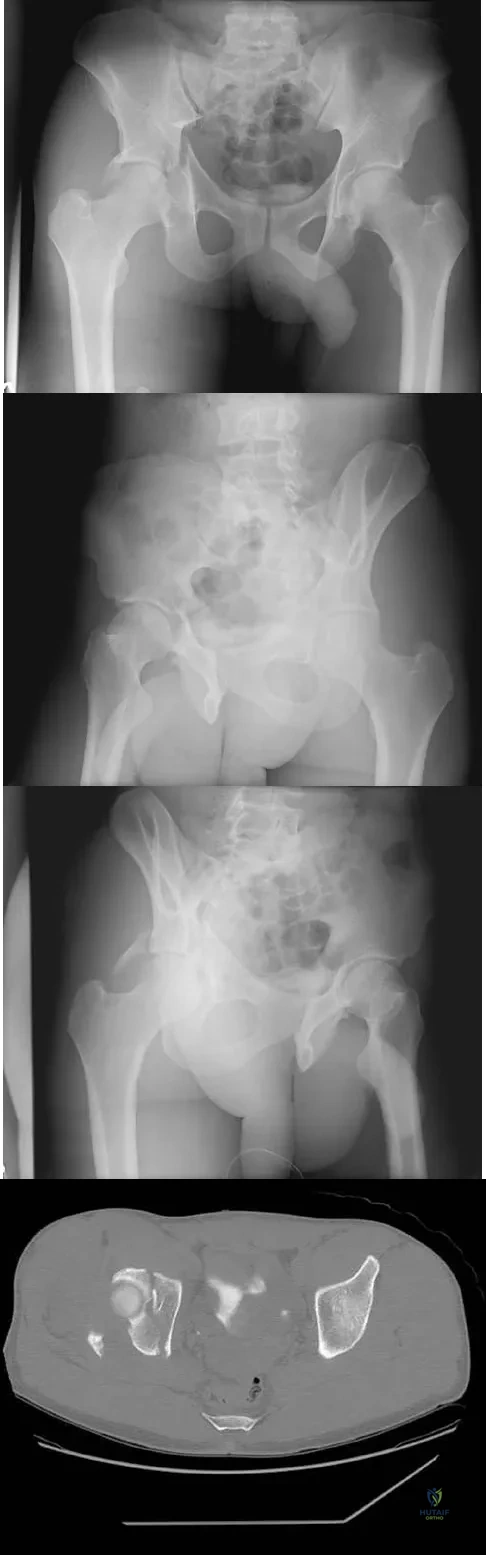
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?
Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 23High Yield
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
References:
- Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 24High Yield
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?

Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 25High Yield
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
Local control of osteosarcoma consists of wide resection and reconstruction. Radiation therapy is not recommended except in unresectable lesions or for palliation. Curettage and bone grafting result in intralesional resection with an unacceptable high rate of local recurrence. Chemotherapy alone is not adequate for local control. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Question 26High Yield
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Scientific References
- :
Question 27High Yield
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include

Explanation
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 28High Yield
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?

Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 29High Yield
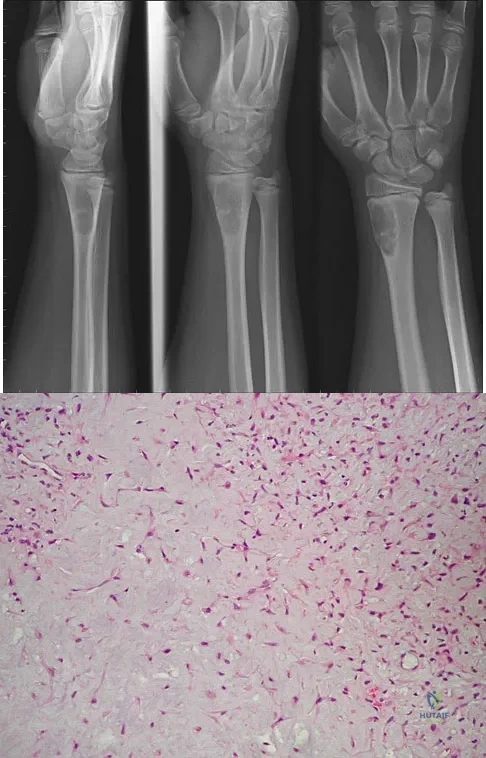
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?
Explanation
The radiographs show a benign-appearing, well-defined lytic lesion with a thin rim of surrounding reactive bone. The photomicrograph shows spindle cells with a myxoid cartilaginous matrix. These findings are diagnostic of chondromyxoid fibroma. This is a rare, benign tumor that usually causes pain and can be locally aggressive. Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Question 30High Yield
A 25-year-old man has ankle instability and a lateral foot callosity. Radiographs are shown in Figures 49a through 49c. Management options are best determined by the

Explanation
The patient has a cavovarus deformity that has resulted in lateral foot overload and stressing of the lateral ligaments. Further treatment depends on the ability to correct the deformity. The Coleman block test indicates whether a deformity is fixed or supple. A supple deformity will respond to orthotic management or soft-tissue procedures, while a fixed deformity requires corrective osteotomy or fusion. Physical therapy, casting, and injection will not address the underlying pathophysiology. There is no indication that this is a neuropathic problem.
Question 31High Yield
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of

Explanation
Initial management of a young patient with a cavovarus deformity of the foot and a family history of Charcot-Marie-Tooth disease should focus on mobilization and strengthening of the weakening muscular units and an accommodative insert. Surgical intervention should be delayed until progression of the deformity begins to cause symptoms and/or weakness of the muscular units, resulting in contractures of the antagonistic muscle units. Pinzur MS: Charcot's foot. Foot Ankle Clin 2000;5:897-912. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 32High Yield
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?

Explanation
Isolated split posterior tendon transfer alone is best performed in a patient with cerebral palsy who is between the ages of 4 and 7 years and has a flexible equinovarus foot. Rigid deformities often must be managed with a combination of soft-tissue and bony procedures. Patients with out-of-phase activity may be best managed with a transfer of the posterior tibialis to the dorsum of the foot, while those with continuous activity are better candidates for an isolated split posterior tendon transfer. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Question 33High Yield
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
Because the patient has significant arthritis, arthrodesis is the treatment of choice. Adding a bone graft will prevent further shortening and add length to her toe, resulting in improved cosmesis. A cheilectomy will not alleviate her arthritis pain. The toe is too short for an effective Moberg phalangeal dorsiflexion osteotomy. A Waterman first metatarsal dorsal osteotomy will not address the degenerative joint disease or shortening. Silastic arthroplasty may help, but there is the risk of additional problems with foreign body reaction and a significant risk of failure known to occur with Silastic materials. Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Question 34High Yield
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
Explanation
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition. Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
References:
- Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 35High Yield
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
Explanation
Dense pods of ingrowth into the porous coating of cementless ingrowth sockets are seen. Channels through the non-ingrown portion allow access to the trabecular bone of the ilium. Polyethylene wear debris can enter these areas through screw holes. Expansile, lytic lesions can result, which can become large without compromising implant fixation. Loosening is late and results from catastrophic loss of bone. A well-fixed acetabular component with a modular design, a well-designed locking mechanism, and a good survivorship history is a candidate for exchange of the liner and grafting of the osteolytic lesion. Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265. Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
References:
- Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 36High Yield
Figure 18a shows the clinical photograph of a 2-year old boy who has a deformity of the right leg. Examination reveals eight cutaneous markings similar to those shown in Figure 18b. Radiographs are shown in Figure 18c. Management should consist of

Explanation
The diagnosis of neurofibromatosis may be based on the presence of at least six cafe-au-lait spots larger than 5 mm in diameter and the osseous lesion shown in Figure 18c. Neurofibromatosis occurs in 50% of patients who have an anterolateral bowing deformity of the tibia, and this bowing may be the first clinical manifestation of this disorder. The patient has anterolateral bowing of the tibia and fibula that warrants concern for a possible fracture and pseudarthrosis; therefore, the limb should be protected in a total contact orthosis to prevent fracture. In contradistinction to posteromedial bowing of the tibia and fibula, spontaneous remodeling of an anterolateral bowing deformity is not expected. Intramedullary nailing or the use of a vascularized fibula is reserved for the treatment of a congenital pseudarthrosis of the tibia. Crawford AH Jr, Bagamery N: Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72-88.
Question 37High Yield
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?

Explanation
The diagnosis is eosinophilic granuloma. The plain radiograph and MRI scan show a lesion in the midshaft of the femur. There is no soft-tissue mass. There is reactive bone about the lesion that suggests a less aggressive tumor. The histology reveals eosinophils in an otherwise bland cellular background with no evidence of mitotic figures or malignant cells to suggest sarcoma. The diagnostic elements are the amphophilic (ie, pale purple) histiocytes with cigar-shaped nuclei, some of which have linear longitudinal grooves. There is no histologic evidence of infection. Lymphoma of bone would be an unusual occurrence in this age group, and the histology is not consistent with that diagnosis.
Question 38High Yield
A characteristic genetic translocation has been noted in which of the following tumors?

Explanation
There have been no characteristic gene translocations or rearrangements noted in osteosarcoma, chondrosarcoma, neurofibrosarcoma, or epithelioid sarcoma. In contrast, Ewing's sarcoma has been noted to have a consistent genetic translocation t(11:22). Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Question 39High Yield
A 12-year-old boy who pitches on two "select" baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of
Explanation
Explanation
19b The imaging study demonstrates characteristics of Little Leaguer's shoulder, including physeal widening. This condition is secondary to overuse (typically throwing) and responds well to rest from the inciting activity. There is no evidence from the patient's history or examination that he has an impingement syndrome, nor is there any indication of labral pathology on the MRI scan. The changes in the proximal humerus are classic for this condition and are not suggestive of a neoplastic process requiring biopsy for definitive diagnosis. Lipscomb AB: Baseball pitching injuries in growing athletes. J Sports Med 1975;3:25-34. Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
References:
- Barnett LS: Little league shoulder syndrome: Proximal humeral epiphysis in adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 40High Yield
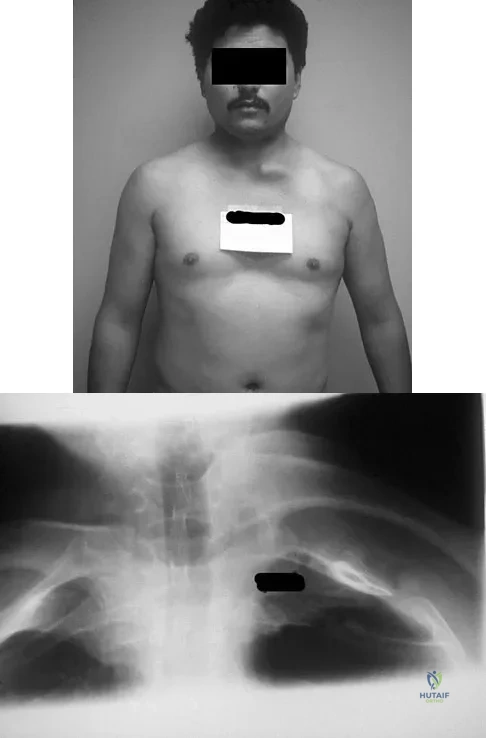
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
Explanation
49b The radiographs show the characteristic features of osteopetrosis. The condition results from defective resorption of immature bone by osteoclasts. There are three distinct clinical forms: (1) infantile-malignant, which is autosomal recessive and fatal in the first few years of life if untreated; (2) intermediate autosomal recessive; and (3) autosomal dominant. These conditions do not follow a malignant course, and patients have normal life expectancy with orthopaedic problems and anemia. In the malignant form, the clinical features include frequent fractures, macrocephaly, progressive deafness and blindness, hepatosplenomegaly, and severe anemia beginning in early infancy or in utero. Deafness and blindness are generally thought to represent effects of pressure on nerves and usually occur later in life. The anemia is caused by encroachment of bone on marrow, resulting in obliteration, and the hepatosplenomegaly is caused by compensatory extramedullary hematopoiesis. Dental caries and abscesses, as well as osteomyelitis of the mandible, are also seen. Most patients have normal intelligence. Treatment of the malignant form includes high dose 1,25 dihydroxy vitamin D with a low-calcium diet to stimulate bone resorption, not because there are vitamin deficiencies. Bone marrow transplant has also been successful. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550. Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
References:
- Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 41High Yield
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Explanation
Explanation
Diabetes mellitus has been associated with resistant cases of adhesive capsulitis. With other causes of onset, adhesive capsulitis frequently responds to nonsurgical management such as stretching exercises or, when this fails, manipulation under anesthesia and/or arthroscopic release. Manipulation is rarely successful for the treatment of adhesive capsulitis associated with diabetes mellitus, and arthroscopic release may be preferred. Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146. Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
References:
- Pollock RG, Duralde XA, Flatow EL, Bigliani LU: The use of arthroscopy in the treatment of resistant frozen shoulder. Clin Orthop 1994;304:30-36.
Question 42High Yield
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?
Explanation
Explanation
1b 1c 1d The patient has had a clear and sudden onset of a profound neurologic deficit. The radiographic studies suggest a lesion in the conus medullaris that appears to be intradural and intramedullary. MRI, with and without contrast, will best evaluate this mass further. The addition of gadolinium allows further evaluation of vascularity and the extent of the lesion. Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
References:
- Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 81-87.
Question 43High Yield
A 23-year-old man has had heel pain and fullness for the past several months. He reports that initially the pain was present only with activity, but more recently the pain has become constant. Figures 53a through 53d show a radiograph, a bone scan, and T2-weighted and gadolinium MRI scans. What is the most likely diagnosis?
Explanation
Explanation
53b 53c 53d The imaging studies reveal an expansile lesion with the classic soap bubble appearance that involves most of the calcaneus. The bone scan reveals a very active lesion with intense uptake, and the MRI scans show the classic, loculated appearance of the lesion with multiple fluid-fluid levels. While it is important to rule out telangiectatic osteosarcoma, the most likely diagnosis is an aneurysmal bone cyst. While giant cell tumor might have a similar appearance, the multiple fluid levels in a expansile lesion strongly favor an aneurysmal bone cyst. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
References:
- Dorfman HD, Czerniak B: Bone Tumors. St Louis, MO, Mosby, 1998, pp 855-879.
Question 44High Yield
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time?

Explanation
Ackland and associates demonstrated that the failure to achieve early spinal clearance in an unconscious blunt trauma patient predisposed the patient to increased morbidity secondary to the prolonged used of cervical immobilization. They demonstrated that the four significant predictors of collar-related ulcers were ICU admission, mechanical ventilation, the necessity for cervical MRI, and the time to cervical spine clearance and collar removal. The risk of pressure-related ulceration increased by 66% for every 1-day increase in Philadelphia collar time and this highlights the need for definitive C-spine clearance. Ackland HM, Cooper DJ, Malham GM, et al: Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine 2007;32:423-428.
Question 45High Yield
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
Explanation
Despite the relatively few problems with porous-coated cementless stems, stress shielding and thigh pain do occur. One design feature of proximally coated stems that has been associated with a higher incidence of distal osteolysis is the presence of noncircumferential proximal porous coating. Tapered, modular with sleeve, and hydroxyapatite proximally porous-coated stems have all performed well. Fully porous-coated straight stems have a high survivorship rate as well. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
References:
- Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 46High Yield
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of

Explanation
The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Question 47High Yield
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction. Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220. Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
References:
- Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
Question 48High Yield
Stiffness relates the amount of load applied to a structure like a long bone or an intramedullary nail to the amount of resulting deformation that occurs in the structure. What is the most important material property affecting the axial and bending stiffness of a structure?
Explanation
The amount of deformation resulting in response to an applied load depends on the stress distribution that the load creates in the structure and the stress versus strain behavior of the material that makes up the structure. Axial and bending loads create stress distributions that involve normal stresses and normal strains. Although all five responses are indeed material properties, only one, elastic modulus, relates normal stresses to normal strains. In fact, axial and bending stiffness are directly proportional to modulus, so that a nail made from stainless steel will have nearly twice the stiffness of a nail made from titanium alloy (because their respective elastic moduli differ by about a factor of two). Hayes WC, Bouxsein ML: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 74-82. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 159-165.
Question 49High Yield
A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that
Explanation
Explanation
Stiffness following primary total knee arthroplasty remains a vexing problem. Treatment options have included extensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic arthrolysis, open arthrolysis with polyethylene exchange, and ultimately revision arthroplasty. Results are not as gratifying as would be expected. Babis and associates performed an open arthrolysis and polyethylene exchange on seven patients who were followed for a mean of 4.2 months. The results were poor. The mean improvement in arc of motion was only 20 degrees. Nicholls and Dorr treated 13 patients for stiffness. Only 40% of those patients obtained good to excellent results. Four patients (30%) required manipulation because of recurrent stiffness postoperatively. They noted they could not predictably improve the arc of motion with a revision operation. Haidukewych and associates reported on 15 patients who underwent revision of well-fixed components after total knee arthroplasty for stiffness. Of the 15 patients, 10 (66%) were satisfied with the outcome revision. Interestingly, they noted that in patients for whom the total arc of motion did not improve but who regained near full extension, there was a greater amount of satisfaction with the procedure than for those who did not regain full extension. Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536. Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.
References:
- Haidukewych GJ, Jacofsky DJ, Pagnano MW, et al: Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. J Arthroplasty 2005;20:133-138.
Question 50High Yield
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?
Explanation
Explanation
14b 14c 14d 14e From an imaging point of view, all of the diagnoses are possible. Biopsy results and cultures are necessary to make the diagnosis. The biopsy specimen shows inflammatory cells and necrotic bone, consistent with osteomyelitis. Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
References:
- Hanna SL, Fletcher BD, Kaste SC, Fairclough DL, Parham DM: Increased confidence of diagnosis of Ewing sarcoma using T2-weighted MR images. Magn Reson Imaging 1994;12:559-568.
Question 51High Yield
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
Explanation
When a study yields a negative result between treatment groups, the next step is to perform a power analysis. The power, by definition, is the probability of rejecting the null hypothesis: in this example the null hypothesis would be that children treated with bisphosphonates would have fewer fractures than the untreated control population. The power analysis helps answer the question as to whether the null hypothesis should be rejected and the finding is real, or whether the sample size was too small or the effect of treatment too subtle to demonstrate a difference between the treatment and control groups. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
References:
- Kocher MS, Zurakowski D: Clinical epidemiology and biostatistics: A primer for orthopaedic surgeons. J Bone Joint Surg Am 2004;86:607-620.
Question 52High Yield
A 35-year-old male laborer with isolated posttraumatic degenerative arthritis of the right hip undergoes the procedure shown in Figure 8. What is the most appropriate position of the right lower extremity?

Explanation
The primary indication for hip arthrodesis is isolated unilateral hip disease in a young, active patient. Avoiding abductor damage and preserving proximal femoral anatomy are imperative to allow conversion to a future total hip arthroplasty. Optimal positioning is 30 degrees of flexion to allow swing-through. Neutral abduction and adduction and slight external rotation allow the most efficient gait while allowing sufficient support in stance. A small degree of adduction is acceptable for a successful hip arthrodesis. Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 53High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
References:
- Krause JO, Brodsky JW: Peroneus brevis tendon tears: Pathophysiology, surgical reconstruction, and clinical results. Foot Ankle Int 1998;19:271-279.
Question 54High Yield
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was
Explanation
Explanation
25b 25c The radiographs show L5 spondylolysis without spondylolisthesis (slip). The bone scan is normal, indicating that the pars interarticularis fractures are not acute. The incidence of spondylolysis is approximately 5% in the general population. The lesion generally develops in children age 5 to 6 years, and there is a second peak in the adolescent population. There is a familial predisposition, with reported rates of 27% to 69% in close relatives. A recent long-term follow-up study found that 90% of the spondylolisthesis had occurred before the patient's first visit to the physician. Spondylolisthesis tends to progress during the initial growth spurt and is similar in some respects to idiopathic scoliosis. Progression of a lytic spondylolysis to spondylolisthesis in adulthood has been reported; however, this is exceedingly rare. Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208. Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
References:
- Fredrickson BE, Baker D, McHolik WJ, Yuan HA, Lubicky JP: The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 1984;66:699-707.
Question 55High Yield
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
Explanation
In a recent analysis of 200 patients with tibial fractures, Bhandari and associates attempted to identify variables that were predictive of reoperation. The variables in the study were type of injury (fracture pattern), degree of open injury, mechanism of injury, cortical bone contact, postoperative complications, polytrauma, anti-inflammatory drug use, nail insertion technique (reamed versus nonreamed), smoking history, alcohol use, diabetes mellitus, peripheral vascular disease, age, disability status pre-injury, gender, surgeon, time to surgery, steroid use, phenytoin use, antibiotic use, anticoagulant use, and type of fixation used. Three variables were statistically significant predictors of reoperation to achieve bone union in the first postinjury year: transverse fracture pattern, open fracture, and cortical contact of 50% or less. Using these three variables, four reoperation risk groups were identified based on the number of these three variables present: 0, 1, 2, or 3. The risk for reoperation was 0%, 18%, 47%, and 94%, respectively. The authors concluded that these statistics can provide prognostic information to patients and help identify those high-risk patients where early intervention to achieve union is indicated. In addition, the data highlights the significance of achieving cortical contact at the time of initial fixation.
References:
- Bhandari M, Tornetta P III, Sprague S, et al: Predictors of reoperation following operative management of fractures of the tibial shaft. J Orthop Trauma 2003;17:353-361.
Question 56High Yield
A 50-year-old laborer sustained an isolated closed injury to his heel after falling 11 feet off a wall. A radiograph and a CT scan are shown in Figures 4a and 4b. To minimize the patient's temporary disability and allow him to return to work most rapidly, management should consist of

Explanation
With a severe articular injury to the calcaneus, the ability to achieve satisfactory results with open reduction and internal fixation diminishes. An arthrodesis is often needed to allow a person who works as a laborer to return to work. Recent literature suggests that this can be successfully performed primarily, improving the odds of an earlier return to the labor force at 1 year. Huefner T, Thermann H, Geerling J, Pape HC, Pohlemann T: Primary subtalar arthrodesis of calcaneal fractures. Foot Ankle Int 2001;22:9-14. Coughlin MJ: Calcaneal fractures in the industrial patient. Foot Ankle Int 2000;21:896-905.
Question 57High Yield
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
References:
- Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 58High Yield
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?

Explanation
The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid. Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 59High Yield
What ligament is the primary restraint to applied valgus loading of the knee?
Explanation
Explanation
The superficial portion of the MCL contributes 57% and 78% of medial stability at 5 degrees and 25 degrees of knee flexion, respectively. The deep MCL and posteromedial capsule act as secondary restraints at full knee extension. The anterior cruciate ligament and PCL also provide secondary resistance to valgus loads.
References:
- Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 60High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 61High Yield
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of

Explanation
Patients require prophylaxis for heterotopic bone after resection to prevent recurrence. The optimal management has been found to be a dose of 700 cGy in one dose delivered either pre- or postoperatively. A dose of 2,000 to 3,000 cGy is considered excessive. Radiation therapy consisting of 1,000 cGy in five doses is an acceptable prophylaxis; however, it will require an extended hospital stay of 3 to 4 days and is more problematic for the patient who must be transported for radiation therapy for 5 days. A dose of 400 cGy is not as effective in prophylaxis for heterotopic bone formation. Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595. Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Question 62High Yield
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?

Explanation
The history, examination, and radiographs are pathognomonic for Little League shoulder, a stress syndrome of the proximal humeral physis caused by overuse. Complete fracture rarely occurs, and recovery usually occurs with rest. Night pain is always a serious concern and further work-up is needed if the patient does not respond to activity modification. Occult instability is not a real concern in this patient, although it should be included in the differential diagnosis. Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Question 63High Yield
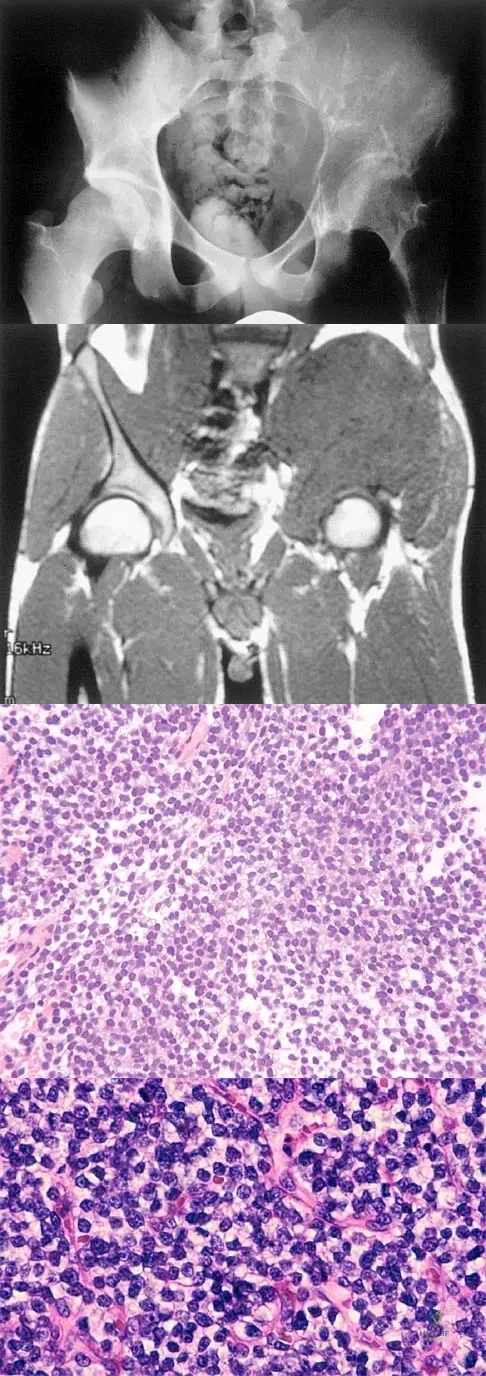
A 25-year-old man has had an insidious onset of left hip pain over the past 11 months. A radiograph, coronal MRI scan, and histopathologic specimens are seen in Figures 2a through 2d. What is the most likely diagnosis?
Explanation
Ewing's sarcoma is the second most common primary sarcoma of bone in children and young adults. It is a malignant round cell tumor with uncertain histogenesis. Sheets of uniform small round blue cells with a high nuclear-to-cytoplasm ratio and the absence of osteoid formation differentiate this histologic diagnosis from the other conditions. Immunohistochemical staining and molecular diagnostic studies are useful to verify the diagnosis.
Question 64High Yield
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 65High Yield
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?

Explanation
Scapulothoracic dissociation is a rare, violent traumatic injury in which the scapula is torn away from the chest wall but the skin remains intact. Massive swelling and ecchymosis are common. Neurovascular injury is the rule with possible subclavian or axillary artery disruption and severe partial or complete brachial plexus paralysis. The diagnosis is made on a nonrotated chest radiograph that shows significant lateral displacement of the medial scapular border from the sternal notch. A right midshaft clavicular fracture is present but is not considered the most significant finding. Ebraheim NA, An HS, Jackson WT, et al: Scapulothoracic dissociation. J Bone Joint Surg Am 1988;70:428-432. Ebraheim NA, Pearlstein SR, Savolaine ER, et al: Scapulothoracic dissociation. J Orthop Trauma 1987;1:18-23. Sampson LN, Britton JC, Eldrup-Jorgensen J, et al: The neurovascular outcome of scapulothoracic dissociation. J Vasc Surg 1993;17:1083-1088.
Question 66High Yield
What is the most common surgical cause of the foot deformity shown in Figure 9?

Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 67High Yield
Figures 17a through 17c show the radiographs of a 38-year-old man following a motorcycle accident. The posterior portion of the talus extruded through a posterolateral wound. The extruded talar body is visible in the wound along with some road debris. Management should now consist of surgical irrigation, debridement, and
Explanation
Explanation
17b 17c The extruded talus should be placed in sterile bacitracin solution, irrigated thoroughly, gently debrided, and immediately replanted in the OR. Open reduction and internal fixation of the talar fracture may be attempted immediately depending on the soft-tissue envelope, or delayed after soft-tissue stabilization with an external fixator. A retrospective study of 19 patients with an extruded talus reported that 12 patients had no subsequent surgery after definitive fixation, 7 had subsequent procedures, and 2 patients developed infections that were treated successfully at an average of 42-month follow-up. Successful outcome in this series was attributed to multiple debridements, soft-tissue stabilization, and primary wound closure. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424. Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
References:
- Marsh JL, Saltzman CL, Iverson M, et al: Major open injuries of the talus. J Orthop Trauma 1995;9:371-376.
Question 68High Yield
A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?

Explanation
This deformity is early in the disease process. The foot is still flexible, as evidenced by correction with the Coleman block test. A simple dorsiflexion osteotomy of the first metatarsal should provide a plantigrade foot. More complex osteotomies are required later in the disease process when the foot is not flexible and the deformity does not correct with the Coleman block test. The patient may also require a tibialis anterior transfer later in the disease process but not at the present time. Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.
Question 69High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 70High Yield
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 71High Yield
A 59-year-old woman underwent open reduction and internal fixation (ORIF) of her ankle 6 months ago, with subsequent hardware removal 3 months later. She now reports persistent, diffuse ankle pain, swelling, and limited range of motion. Figure 48 shows an oblique radiograph of the ankle. What is the next most appropriate step in management?
Explanation
Explanation
The radiographs demonstrate persistent widening of the medial clear space with an ossicle. This represents soft-tissue interposition-scar tissue, the deltoid ligament, or the posterior tibialis tendon. Physical therapy will not improve the symptomatic malalignment. Hardware removal would be indicated for pain localized to the lateral fibula. Repeat syndesmotic screw fixation alone will not reduce the malalignment. Deltoid ligament repair may be necessary but will need to be combined with debridement of the medial ankle and syndesmosis, as well as repeat placement of one or more syndesmotic screws to maintain the reduction. Weening B, Bhandari M: Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma 2005;19:102-108.
Question 72High Yield
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
Explanation
Numerous clinical and basic science investigations have evaluated meniscal tear characteristics to identify factors that either promote or mitigate against meniscal healing. Complex tears have been noted to heal poorly, while longitudinal tears heal more predictably. Tear length, time from injury to repair, medial versus lateral meniscal tears, and the use of a fibrin clot have not been shown to consistently affect meniscal healing. However, rim width, the distance of the tear site from the peripheral meniscocapsular junction (vascular supply), has been shown to have a significant role in the ability of a meniscus repair to heal. DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
References:
- Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 73High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
References:
- Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 74High Yield
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of
Explanation
Explanation
The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months. Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
References:
- Stern PJ, Fassler PR: Anterior interosseous nerve compression syndrome, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, 1991, vol 2, pp 983-1002.
Question 75High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 76High Yield
During impaction of a cementless acetabular component, the posterior column was fractured and found to be displaced. Which of the following is considered the most appropriate surgical option?
Explanation
Explanation
Acetabular bone loss presents a challenge during reconstruction. A cementless hemispherical cup can be used in most patients provided that the acetabular rim, particularly the posterior column, is intact. When the posterior column is disrupted, fixation with a reconstruction plate and/or the use of an antiprotrusio cage is recommended. The latter is particularly important when the posterior column is fractured and displaced, such as in this patient. Under these circumstances, reduction of the fracture and application of an antiprotrusio cage is recommended. In this particular type of case, some surgeons may elect to retain the hemispherical cup and apply an antiprotrusio cage over the cup ("cage over cup" technique). Berry DJ: Antiprotrusio cages for acetabular revision. Clin Orthop 2004;420:106-112.
References:
- Peterson CA, Lewallen DG: Periprosthetic fracture of the acetabulum after total hip arthroplasty. J Bone Joint Surg Am 1996;78:1206-1213.
Question 77High Yield
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?
Explanation
Explanation
59b 59c 59d This classic case of osteosarcoma illustrates the typical radiographic and histologic characteristics of this disease. The radiographs show an aggressive-appearing lesion of the distal femur. The lesion has both lytic and blastic areas. Periosteal reaction is present in the form of a Codman's triangle. The radiographs are highly suggestive of osteosarcoma. The photomicrographs show malignant spindle cells that produce osteoid, thus confirming the diagnosis of osteosarcoma. Treatment of osteosarcoma is multimodal including multi-agent chemotherapy and surgery (wide resection or amputation). Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
References:
- Mankin HJ, Hornicek FJ, Rosenberg AE, et al: Survival data for 648 patients with osteosarcoma treated at one institution. Clin Orthop Relat Res 2004;429:286-291.
Question 78High Yield
The superior glenohumeral ligament primarily restrains
Explanation
Explanation
Several cutting studies have evaluated the primary static restraints and the role of the glenohumeral ligaments in providing static stability. With the arm at the side in adduction, the superior glenohumeral ligament and coracohumeral ligament are the primary restraints to inferior translation. The middle glenohumeral ligament functions with the arm in 45 degrees of abduction and resists anterior translation. The inferior glenohumeral ligament is the primary restraint to anterior translation at 90 degrees of abduction. Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
References:
- Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 79High Yield
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
Improvement in the appearance of the hip joint on functional radiographic evaluation (abduction/adduction views) has been shown to be predictive of outcome following joint preserving surgery. CT and MRI findings have not been shown to be predictive of outcome.
Question 80High Yield
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of

Explanation
The findings are classic for a pectoralis major tendon avulsion. Deformity of the anterior axillary fold is a classic finding, and ecchymosis down the arm suggests that the injury is at the humeral attachment rather than at the musculotendinous junction. Good external rotation strength indicates that function in the supraspinatus and infraspinatus has been preserved. The treatment of choice for a tendon avulsion in a young individual is early surgical repair. Conversely, if the injury is within the muscle or at the musculotendinous junction, initial nonsurgical management is recommended. If the location of the injury cannot be determined by physical examination, then MRI of the pectoralis major can be helpful. Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 81High Yield
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
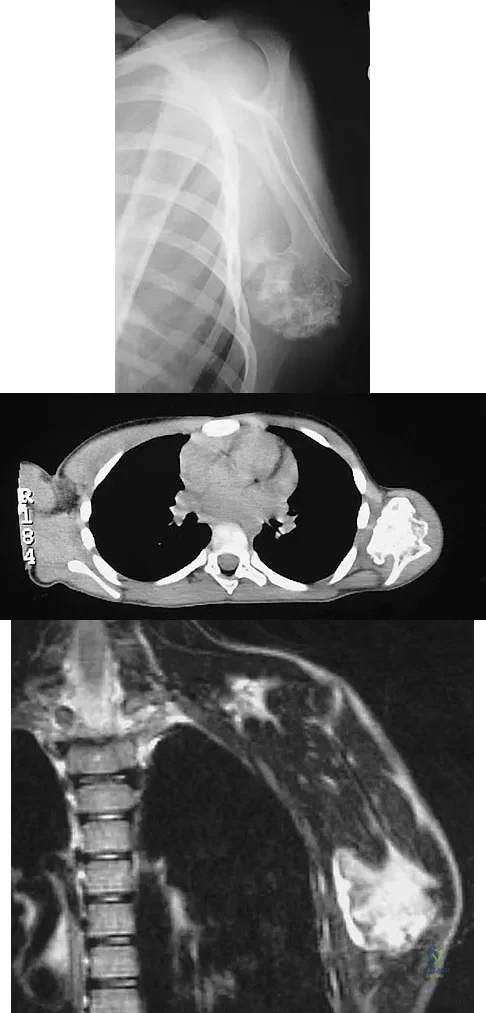
Explanation
The findings are typical for an osteochondroma. It is found as an outgrowth of bone and cartilage from those bones that arise from enchondral ossification. It may be flat, verrucous, or with a long stalk and cauliflower-like cap. Osteochondromas can become symptomatic secondary to irritation of the adjacent musculature. They cease to proliferate when epiphyseal growth ceases.
Question 82High Yield
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess
Explanation
Explanation
The radiograph shows a faux profil view of the hip. The primary purpose of this view is to evaluate anterior coverage of the femoral head. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
References:
- Lequesne M, deSez S: Le faux profil du bassin: Nouvelle incidence radiographique pour l'etude de la hance. Son utilite dans les dysplasies et les differentes coxopathies. Rev Rhum Mal Osteoartic 1961;28:643.
Question 83High Yield
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?

Explanation
Osteonecrosis of the femoral head is the most devastating complication of SCFE. There is a 47% incidence of ischemic necrosis associated with an unstable SCFE. By definition, the patient with an unstable SCFE is unable to bear weight even with crutches. Osteonecrosis is most likely associated with the initial femoral head displacement rather than the result of either tamponade from hemarthrosis or from gentle repositioning prior to stabilization. Age, sex, and obesity are not risk factors for osteonecrosis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 84High Yield
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?

Explanation
The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg's syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers. Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Question 85High Yield
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of
Explanation
Explanation
The patient has symptomatic grade IV Brooker heterotopic ossification. Once the bone has matured, it can be excised. Surgical excision should be combined with postoperative irradiation to avoid recurrence. Pharmacologic and irradiation intervention are not successful beyond the perioperative period unless they are combined with surgical excision of mature heterotopic ossification. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
References:
- Iorio R, Healy WL: Heterotopic ossification after total hip and total knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Question 86High Yield
A 69-year-old woman reports a painful clicking in her right shoulder. A soft-tissue mass is palpated at the lower portion of the scapula. Based on the MRI scan and biopsy specimens shown in Figures 72a through 72c, what is the most likely diagnosis?
Explanation
Explanation
72b 72c Elastofibroma is a rare, benign soft-tissue pseudotumor characteristically located in the subscapular region. Most patients are between 50 and 70 years of age and have pain, decreased shoulder range of motion, or a mass. The lesion usually is best visualized with the arm elevated forward and adducted to displace the scapula laterally and allow the mass to protrude from the chest wall. They are frequently bilateral. Grossly, the mass is ill-defined, oblong or spherical, firm, and ranges in size from 5 cm to 10 cm. These masses appear infiltrative and frequently are mistaken for a sarcomatous lesion. Histologically, the mass is composed of a mixture of intertwining eosinophilic collagen and elastic fibers, and scattered fibroblasts, mucoid material, and fat. Vastamaki M: Elastofibroma scapulae. Clin Orthop Relat Res 2001;392:404-408. Nielsen T, Sneppen O, Mykre-Jensen O, et al: Subscapular elastofribroma: A reactive pseudotumor. J Shoulder Elbow Surg 1996;5:209-213.
References:
- Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 286-289.
Question 87High Yield
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
Explanation
45b 45c 45d Giant cell tumors typically occur in a juxta-articular location involving the epiphysis and metaphysis of long bones, usually eccentric in the bone. The radiographs show a destructive process within the distal tibia and an associated soft-tissue mass. The histology shows multinucleated giant cells in a bland matrix with a few scattered mitoses. Osteosarcoma can have a similar destructive appearance but a very different histologic pattern with osteoid production. Ewing's sarcoma also can have a diffuse destructive process in the bone. The histologic pattern of Ewing's sarcoma is diffuse round blue cells. Aneurysmal bone cysts typically are seen as a fluid-filled lesion on imaging studies and have only a scant amount of giant cells histologically. Metastatic adenocarcinoma does not demonstrate the pattern shown in the patient's histology specimen. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
References:
- Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 88High Yield
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?

Explanation
The patient has sustained a Vancouver B2 periprosthetic femoral fracture (a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthoplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 89High Yield
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
Explanation
Closed-chain exercise requires the distal portion of the extremity to be fixed. It is more commonly used in lower extremity exercise, and movement is produced by co-contraction of muscles. Joint compression is increased, and multiple joints are involved with closed-chain exercise. In open-chain exercise, the distal portion of the extremity is free. Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
References:
- Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 90High Yield
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?

Explanation
The radiograph and MRI scan show elongation and fragmentation of the os peroneum. Although casting, orthoses, and steroid injection may relieve symptoms, excision of the os peroneum and primary repair when necessary, with or without tenodesis of the peroneus longus to the peroneus brevis, have been shown to produce excellent results. Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 812-817.
Question 91High Yield
Which of the following positions of immobilization has been shown to best approximate the anterior labrum against the glenoid rim following anterior dislocation of the shoulder?
Explanation
Explanation
Following anterior dislocation of the shoulder, the affected arm is typically placed in a sling with the shoulder in adduction and internal rotation. A recent study has shown that placement in this position actually results in laxity of the anterior supporting structures of the shoulder, allowing the postinjury hemarthrosis to push the labrum and capsular ligaments away from the anterior glenoid rim. Thus, immobilization in this position may actually impede healing of these structures. Alternatively, resting the arm in a position of adduction and external rotation allows the anterior supporting structures to abut against the anterior glenoid rim by forcing the hemarthrosis posteriorly. Placing the arm in this position following anterior dislocation is believed to allow for better healing of the anterior labrum and ligaments.
References:
- Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2002;84:873-874.
Question 92High Yield
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of

Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 93High Yield
Which of the following actions best enhances performance when an athlete is participating in a 10K race?
Explanation
Proper hydration prior to an athletic event is the most important determinant of performance. It is virtually impossible to keep pace with fluid loss during an athletic competition. When a net loss of fluid occurs and the athlete is properly prehydrated, this fluid loss will not adversely affect performance. It is not necessary to load up on carbohydrates prior to a 10K race, or to replace calories burned during the race. Hyponatremia can develop in ultra-endurance athletes, especially marathoners, if they hydrate without replacing electrolytes lost through sweating; however, this is highly unlikely for a 10K race. Newmark SR, Toppo FR, Adams G: Fluid and electrolyte replacement in the ultramarathon runner. Am J Sports Med 1991;19:389-391.
Question 94High Yield
The parents of a 15-month-old child report that he is not yet walking. Further evaluation, rather than reassurance and observation, should be conducted if the child is not performing what other activity?
Explanation
Explanation
A child not ambulating at age 15 months is still within normal limits. The child should be able to sit by age 9 months. The remaining milestones listed are reached later in development.
References:
- Behrman RE, Kliegman RM, Jenson HB: The first year, in Fletcher J, Thorp D, Davis RE (eds): Nelson Textbook of Pediatrics, ed 17. Philadelphia, PA, WB Saunders, 2004, p 33.
Question 95High Yield
In patient selection for meniscal allograft transplantation, which of the following variables has the greatest influence on outcome?

Explanation
Many clinical studies to date show that the extent of arthritis is the most common variable that has the greatest influence on outcome. The success rate of allograft transplantation is significantly diminished in patients who have grade IV chondromalacia of the knee or notable flattening and general joint incongruity. Carter TR: Meniscal allograft transplantation. Sports Med Arthroscopy Rev 1999;7:51-63. Garrett JC: Meniscal transplantation: A review of 43 cases with two- to seven-year follow-up. Sports Med Arthroscopy Rev 1993;2:164-167.
Question 96High Yield
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
EIP transfer results in no functional deficit. If the tendon is cut proximal to the sagittal band, there will be no extensor deficit. Browne EX, Teague MA, Snyder CC: Prevention of extensor lag after indicis proprius transfer. J Hand Surg Am 1979;4:168-172.
Question 97High Yield
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?

Explanation
The radiographs demonstrate a rapid erosion of the bipolar component into the acetabulum. Although acetabular erosion is more common with unipolar hip arthroplasties, it can occur with bipolar components. Haidukewych and associates noted a very low erosion rate but none in the first 2 years. The second finding on the radiographs is the linear radiolucency progressing from the joint toward the end of the stem at the cement-bone interface suggesting chronic infection or diffuse loosening. The persistent pain since implantation also suggests chronic infection. High activity levels and osteoporosis do not lead to acetabular erosion in the first 2 years after hemiarthroplasty. While the cement technique is suboptimal, loosening and erosion should not be expected from this alone. An oversized bipolar head would extrude and not erode. Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126. Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Question 98High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 99High Yield
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?

Explanation
The lesion has the typical "blown out" lytic radiographic appearance that is most commonly found in thyroid or renal cell metastases. Given the history of hematuria and histology findings, the most likely diagnosis is metastatic renal cell carcinoma. This tumor is relatively resistant to chemotherapy. Radiation therapy is used as a postoperative adjuvant treatment with varying response rates. Surgery should be performed after preoperative embolization to decrease the risk of intraoperative bleeding, as no tourniquet can be used in this location. Patients with metastatic renal cell carcinomas may survive for years, resulting in a higher likelihood of local tumor progression with ineffective adjuvant therapy. Intramedullary fixation combined with curettage and cementation will provide the best chance of local control while maintaining the patient's native shoulder and elbow joints. A total humeral resection is an extensive surgery with considerable morbidity and is not indicated for this patient because less extensive surgery is likely to be effective. Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054. Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 100High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
References:
- Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
