Orthopedic Board Review: 100 High-Yield MCQs | Mock Exam Set #640

Key Takeaway
This page provides 100 high-yield orthopedic board review questions (MCQs) to help surgeons master ABOS, OITE, and FRCS exams. This comprehensive practice set (No. 640) tests your knowledge, identifies weaknesses, and reinforces critical concepts for successful board certification.
Minimally Invasive Anterolateral Proximal Hum...
00:00
Start Quiz
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?

Explanation
The images show an epiphyseal lesion. The MRI scan shows extensive bone edema surrounding the lesion, consistent with chondroblastoma. Histology shows polygonal chondroblasts in a cobblestone-like pattern and areas of calcification consistent with chondroblastoma. Although some giant cells are seen, the age of the patient and the polygonal chondroblasts differentiate this lesion from giant cell tumor. Clear cell chondrosarcoma is an epiphyseal lesion that occurs in an older population, and the cells have clear cytoplasm. This lesion is not producing bone on imaging or histologic specimen, eliminating osteosarcoma. Tuberculous septic arthritis can be an epiphyseal lesion, but granulomas would be seen on histology. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 3High Yield
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
Explanation
Because the patient is essentially asymptomatic, the most appropriate course of action is observation. Prophylactic hallux valgus surgery is not medically indicated. Steroid injection would only risk infection, as well as joint and capsule damage. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Special shoe wear or an extra-depth shoe is not necessary and is unlikely to be accepted by the patient. Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
References:
- Teitz CC, Hu SS, Arendt EA: The female athlete: Evaluation and treatment of sports-related problems. J Am Acad Orthop Surg 1997;5:87-96.
Question 4High Yield
What is the second most common primary bone malignancy in children?
Explanation
Explanation
Ewing's sarcoma is the second most common bone tumor in children with an incidence of three per one million Caucasian children younger than 21 years of age. Ewing's sarcoma is rare in African Americans. Osteosarcoma is the most common bone tumor in children. Rhabdomyosarcoma is the most common soft-tissue sarcoma in children. Fibrosarcoma is a rare primary bone tumor most commonly seen in adults. Adamantinoma is a rare primary bone malignancy also most commonly seen in adults in the tibia. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
References:
- Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 5High Yield
A 30-year-old woman has pain in her right hand. The radiograph, CT scan, and biopsy specimen are seen in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c An enchondroma is the most common primary tumor of the long bones of the hand. The lesion is usually asymptomatic and often is detected when there is a pathologic fracture. Shimizu K, Kotoura Y, Nishijima N, Nakamura T: Enchondroma of the distal phalanx of the hand. J Bone Joint Surg Am 1997;79:898-900.
References:
- Takigawa K: Chondroma of the bones of the hand: A review of 110 cases. J Bone Joint Surg Am 1971;53:1591-1600.
Question 6High Yield
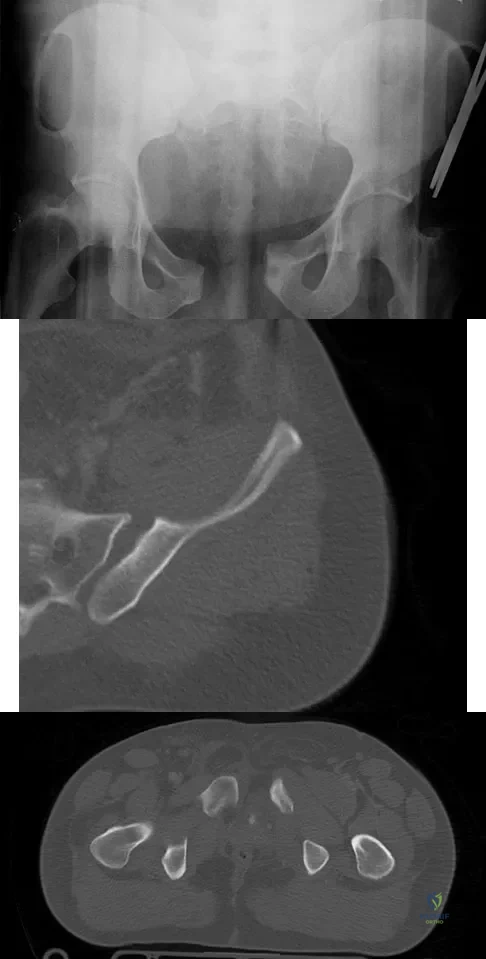
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 7High Yield
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
Explanation
All of the answers are possible complications of meniscal repair. There are large volumes of literature evaluating the results of meniscal repair, both for the all-inside technique, as well as the inside-out technique. Failure rates are similar. Intra-articular synovitis occurs with absorbable sutures and absorbable implants. Peroneal nerve injuries are more common with the lateral-sided repairs. Saphenous nerve injuries are more common with medial-sided tears. Because of the incision required and the technique of tying over soft tissue, the risk of a saphenous nerve injury is greater with an inside-out technique than with an all-inside technique. Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
References:
- Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 8High Yield
During stabilization of a slipped capital femoral epiphysis, the screw penetrates into the joint. The screw is repositioned so that it is within the femoral head. This transient penetration of the hip joint will most likely lead to
Explanation
Explanation
Chondrolysis may be associated with unrecognized permanent penetration of the joint space by a pin or screw. However, transient penetration by the guide wire or screw is not associated with this problem. One study described 11 hips in which there was transient intraoperative penetration of the joint space by a guide wire or screw. These patients were followed for at least 2 years, with none showing any clinical or radiographic evidence of chondrolysis. Another retrospective study of 55 slipped epiphyses described 11 hips with transient intraoperative pin penetration, with none showing development of chondrolysis. There are no studies to suggest that transient pin penetration leads to osteonecrosis, stiffness, or premature physeal closure. Zionts LE, Simonian PT, Harvey JP Jr: Transient penetration of the hip joint during in situ cannulated-screw fixation of slipped capital femoral epiphysis. J Bone Joint Surg Am 1991;73:1054-1060.
References:
- Vrettos BC, Hoffman EB: Chondrolysis in slipped upper femoral epiphysis: Long-term study of the etiology and natural history. J Bone Joint Surg Br 1993;75:956-961.
Question 9High Yield
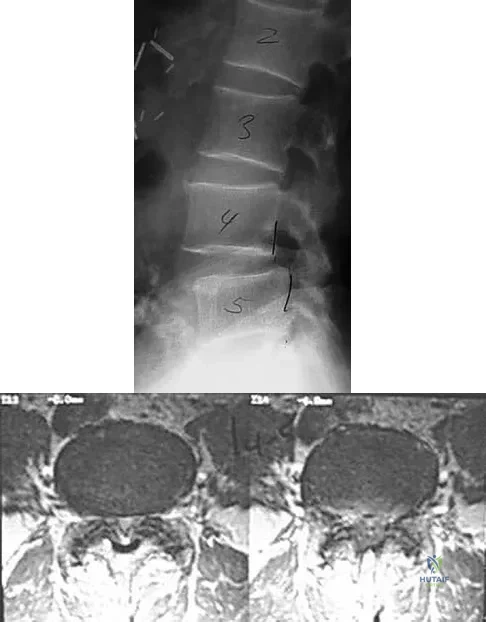
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
Explanation
Nonsurgical modalities remain the mainstay for treatment of herniated disks. Spontaneous resorption of herniated disks frequently is detected by MRI. Marked infiltration by macrophages and neovascularization are observed on histologic examination of herniated disks, and the resorption is believed to be related to this process. Many cytokines such as vascular endothelial growth factor, tumor necrosis factor-alpha, and metalloproteinases have been implicated in this process, but none has been found to be singularly responsible. Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
References:
- Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine 2001;26:1522-1527.
Question 10High Yield
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
A positive jaw jerk reflex suggests that the problem is above the level of the pons. All of the other physical signs are exhibited in patients with cervical myelopathy. Although these signs also may be present in conditions affecting the brain, they do not help differentiate between a brain etiology and a cervical spine etiology. A jaw jerk reflex, however, is not present in patients with cervical myelopathy alone. Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493. Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
Question 11High Yield
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 12High Yield
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows

Explanation
The radiograph shows a well-osseointegrated tapered stem with a metaphyseal porous coating, spot welds in the porous region, and calcar rounding. Trochanteric stress shielding and distal cortical hypertrophy are also signs of ingrown stems but are seen more frequently in association with extensively porous-coated stems exhibiting diaphyseal ingrowth. There is no evidence of lucent lines or a pedestal, signs that suggest instability. Femoral stem subsidence can be determined only by a review of sequential radiographs. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Question 13High Yield
A 50-year-old laborer sustained an isolated closed injury to his heel after falling 11 feet off a wall. A radiograph and a CT scan are shown in Figures 4a and 4b. To minimize the patient's temporary disability and allow him to return to work most rapidly, management should consist of

Explanation
With a severe articular injury to the calcaneus, the ability to achieve satisfactory results with open reduction and internal fixation diminishes. An arthrodesis is often needed to allow a person who works as a laborer to return to work. Recent literature suggests that this can be successfully performed primarily, improving the odds of an earlier return to the labor force at 1 year. Huefner T, Thermann H, Geerling J, Pape HC, Pohlemann T: Primary subtalar arthrodesis of calcaneal fractures. Foot Ankle Int 2001;22:9-14. Coughlin MJ: Calcaneal fractures in the industrial patient. Foot Ankle Int 2000;21:896-905.
Question 14High Yield
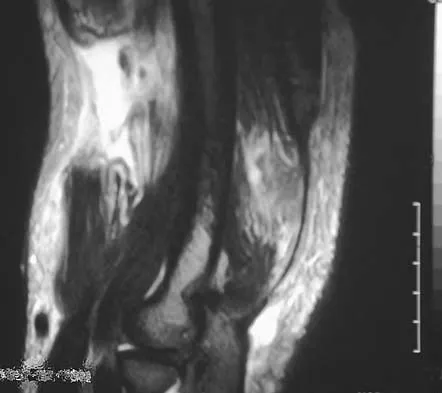
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel's sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of

Explanation
Neurilemoma is a benign tumor of nerve sheath origin, and peak incidence is in the third through sixth decades. The tumor is well encapsulated on the surface of a peripheral nerve. MRI findings may be significant for a "string sign." A positive Tinel's sign in the distribution of the nerve affected may be present. Grossly, the lesion is well encapsulated in a nerve sheath. Microscopically, there are structures referred to as Antoni A (a pattern of spindle cells arranged in intersecting bundles) and Antoni B (areas with less cellularity with loosely arranged cells). These lesions are benign, and treatment should consist of marginal excision. Nerve function may be preserved by careful dissection, excising the lesion parallel to the nerve fascicles so the lesion may be extruded. Recurrence is rare. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Question 15High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Question 16High Yield
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?

Explanation
Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 17High Yield
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient's symptoms?

Explanation
The patient has a symptomatic os trigonum caused by impingement that occurs with maximal plantar flexion of the ankle in the demi-pointe or full-pointe position. Patients frequently report posterolateral pain localized behind the lateral malleolus that may be misinterpreted as a disorder of the peroneal tendon. Pain with passive plantar flexion (the plantar flexion sign) indicates posterior impingement, not a problem with the peroneal tendon. The symptoms are not characteristic of a stress fracture, nor do the radiographs show a stress fracture or an osteochondritis dissecans lesion. The os trigonum is modest in its dimensions. The incidence or magnitude of symptoms does not correlate with the size of the fragment. Large fragments may be asymptomatic, while small lesions may create significant symptoms. Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 18High Yield
A 52-year-old man has a stage IIB malignant fibrous histiocytoma of the distal femur. Local treatment should consist of
Explanation
Explanation
Local control of malignant fibrous histiocytoma of bone typically consists of wide excision. Curettage and bone grafting is a procedure with an intralesional surgical margin, with an unacceptable rate of local recurrence. Prophylactic fixation is considered for patients with metastatic disease. Radiation therapy alone is not adequate for local control of this tumor. Neoadjuvant chemotherapy is often used primarily for systemic tumor control.
References:
- Bacci G, Picci P, Mercuri M, Bertoni F, Ferrari S: Neoadjuvant chemotherapy for high grade malignant fibrous histiocytoma of bone. Clin Orthop 1998;346:178-189.
Question 19High Yield
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
Explanation
The use of multiagent chemotherapy has been shown to be associated with a survival benefit in patients with osteosarcoma. The use of chemotherapy in adults with soft-tissue sarcoma remains somewhat controversial. It has not been associated with improved survival rates in patients with renal carcinoma, dedifferentiated chondrosarcoma, or melanoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
References:
- Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 20High Yield
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
Joshi and associates reported a 96% incidence of pain relief in 181 total hip arthroplasties in patients with ankylosing spondylitis. Only 65% of patients had good to excellent functional results, primarily the result of associated systemic diseases and spinal deformity. The incidence of infection was slightly higher, and the incidence of heterotopic ossification was higher in this group of patients.
Question 21High Yield
The fracture shown in Figure 32 is strongly indicative of what diagnosis?

Explanation
Fractures that occur through the primary spongiosa at the subphyseal region of the metaphysis are highly specific for child abuse. On radiographic studies, the metaphyseal lucency in these injuries may appear as either the so-called "bucket-handle" or "metaphyseal corner" fracture. These fractures are not typical features of osteogenesis imperfecta or vitamin D-resistant rickets. The ingestion of lead may lead to thick, transverse bands of increased density at the distal metaphysis. Fractures in the subphyseal region of the metaphysis are not typically seen in children who have osteomyelitis. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Question 22High Yield
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
The mainstay of early treatment of open fractures includes irrigation and debridement. Prior to the development of antibiotics, this was traditionally accomplished with some form of detergent irrigation. Antibiotic irrigation has been in favor more recently but has mixed scientific results related to its use. Results of at least one major study show the use of a nonsterile liquid soap additive (castile soap) is at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, and shows a significant decrease in problems with soft-tissue healing.
Question 23High Yield
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes' disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?

Explanation
Several authors have reported good success in relieving pain with shelf acetabuloplasty. This patient's Perthes' disease is in the healed phase; therefore, proximal femoral varus and Salter innominate osteotomies aimed at improving containment are not indicated. The medial one half of the patient's femoral head is markedly deformed, and rotating it into a weight-bearing position with proximal femoral valgus osteotomy is unlikely to relieve pain. Hip arthrodesis can always be performed as a salvage procedure if the shelf acetabuloplasty fails. Daly K, Bruce C, Catterall A: Lateral shelf acetabuloplasty in Perthes' disease: A review of the end of growth. J Bone Joint Surg Br 1999;81:380-384.
Question 24High Yield
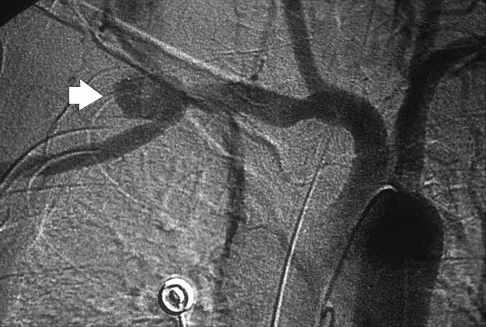
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
Question 25High Yield
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 26High Yield
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Explanation
Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root. Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
References:
- Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 27High Yield
Figure 16 shows the radiograph of an otherwise healthy 62-year-old woman who fell. Management should consist of
Explanation
Explanation
The radiograph reveals that the femoral component is grossly loose as evidenced by disruption of the cement column; therefore, retention of the original components will not yield a successful outcome. A cementless revision is the procedure of choice. A strut graft and/or plate may be added at the surgeon's discretion. A resection arthroplasty would only be considered in a nonambulatory patient. Cemented fixation of the revision component would be problematic given the numerous fracture fragments and the inability to contain the cement. Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.
References:
- Duwelius PJ, Schmidt AH, Kyle RF, et al: A prospective, modernized treatment protocol for periprosthetic femur fractures. Orthop Clin North Am 2004;35:485-492.
Question 28High Yield
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include
Explanation
Explanation
9b In addition to mild hip dysplasia, the radiograph shows an osteoblastic lesion of the right ilium. The patient's symptoms are much more severe than is typical for late hip dysplasia. MRI can determine the extent of the lesion in the bone and soft tissues. Following work-up and biopsy, the patient was diagnosed with Ewing's sarcoma. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
References:
- Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 2030.
Question 29High Yield
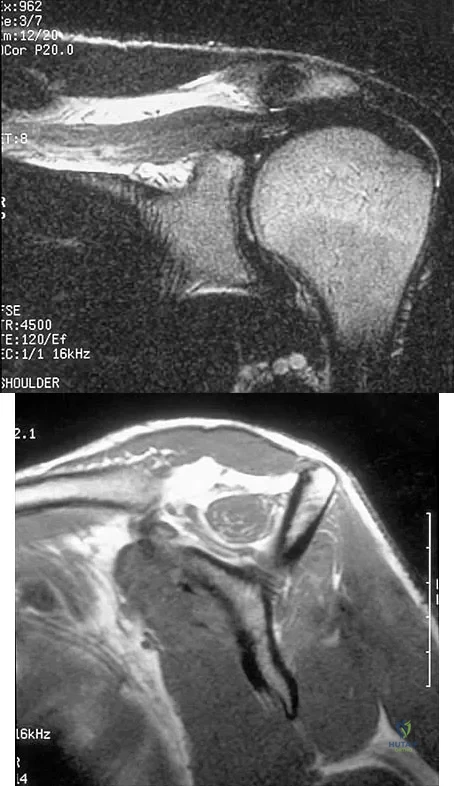
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 30High Yield
What is the most common mechanism of injury that produces turf toe?
Explanation
Explanation
The most common mechanism of injury for turf toe is a hyperextension injury to the MTP joint. The foot is typically in a dorsiflexed position with the heel raised when an external force drives the MTP joint into further dorsiflexion. The joint capsule usually tears at the metatarsal neck because its attachment is weaker there than at the proximal phalanx. Some compression injuries to the dorsal articular surface of the metatarsal head can result from extension or hyperextension. Clanton TO, Ford JJ: Turf toe injury. Clin Sports Med 1994;13:731-741.
References:
- Rodeo SA, O'Brien S, Warren RF, et al: Turf toe: An analysis of metatarsophalangeal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 31High Yield
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T2-weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
Explanation
Explanation
The MRI scan reveals a rudimentary disk at the L5-S1 level, suggesting transitional anatomy. There is a posterior disk bulge at L3-4. At L4-5, there is disk desiccation and loss of disk height, with a posterior disk bulge and a high intensity zone in the posterior annulus, suggesting an annular tear. While these and similar radiographic findings have been associated with the severity of a patient's pain, they are also commonly found in cross-sectional studies of asymptomatic subjects. Carragee and associates found 59% of symptomatic patients undergoing diskography have high intensity zones as compared to 25% of asymptomatic subjects of a similar patient profile. Diskographic injections provoked pain in disks with high intensity zones approximately 70% of the time whether the individual was previously symptomatic or not. This patient's non-specific pain pattern does not require further work-up as she is not a surgical candidate. Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992. Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain. J Am Acad Orthop Surg 2006;14:46-55. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 32High Yield
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Question 33High Yield
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?

Explanation
The MRI scan shows an ALPSA lesion. This is also known as a medialized Bankart with medial displacement of the torn anterior labrum. During surgical stabilization, the labrum and periosteal sleeve must be mobilized and repaired laterally to reduce recurrent instability. A Perthes lesion is a nondisplaced labral tear. A GLAD lesion represents a nondisplaced anterior labral tear with an associated articular cartilage injury. Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion: A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Question 34High Yield
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
The median survival of patients after discovery of bone metastasis from primary lung carcinoma is shorter compared with other primary sites.
Question 35High Yield
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
Explanation
15b 15c The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
References:
- Hensinger RN, DeVito PD, Ragsdale CG: Changes in the cervical spine in juvenile rheumatoid arthritis. J Bone Joint Surg Am 1986;68:189-198.
Question 36High Yield
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Explanation
Explanation
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 37High Yield
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?

Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 38High Yield
Flexion and extension of the elbow occur about an axis of rotation that
Explanation
Explanation
The elbow mimics a true hinge and flexes and extends around an axis that is centered in the centers of the trochlea and capitellum. The medial epicondyle is not perfectly isometrically placed; rather the axis of rotation passes through a point on the anteroinferior aspect of the medial epicondyle. Application of a hinged external fixator is possible because of the fact that there is a single axis of rotation. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54. London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
References:
- Morrey BF, Chao EY: Passive motion of the elbow joint. J Bone Joint Surg Am 1976;58:501-508.
Question 39High Yield
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?

Explanation
The radiographs show an osteochondritis dissecans (OCD) lesion in the medial femoral condyle of a skeletally immature patient. The lesion is not displaced from its bed. Nonsurgical management of a stable OCD lesion in a patient with open physes consists of a period of activity limitation and occasional immobilization. Unstable lesions, loose bodies, and patients with closed physes require more aggressive treatment. Most of the surgical procedures can be done arthroscopically. Because the radiographic appearance is typical, biopsy is unnecessary. The radiographs do not show an osteocartilaginous loose body, and the patient reports no catching or locking; therefore, removal of the loose body is not indicated. Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776. Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Question 40High Yield
A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
Explanation
Explanation
Severe valgus deformity is frequently accompanied by hypoplasia of the lateral femoral condyle. Posterior referencing instrumentation can substantially internally rotate the femoral component with respect to the transepicondylar axis and Whiteside's line. The femoral component malrotation must be corrected to properly address this problem. Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.
References:
- Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 1995;321:168-172.
Question 41High Yield
A 32-year-old football coach has had a 4-month history of increasing right wrist pain, particularly during blocking exercises, and he reports significant pain with range of motion and gripping activities. He denies any history of trauma. Examination reveals dorsal wrist tenderness and boggy fullness over the dorsum of the wrist. No erythema is noted. Grip strength is 60% compared with the opposite side. Radiographs are shown in Figures 5a and 5b. What is the most likely diagnosis?
Explanation
Explanation
5b The patient has Kienbock's disease (osteonecrosis of the lunate), which presents with boggy synovitis of the wrist, decreased range of motion, and often normal radiographs. The patient's radiographs reveal small fragments from the lunate, with increased density in the lunate body. While a traumatic event may precede the patient's pain, often an insidious increase in pain is found. Repetitive trauma has been suggested as a possible cause. This disease process is classically associated with an ulnar-negative variant. An MRI scan, revealing a low-intensity signal in the lunate, is the best diagnostic tool for early Kienbock's disease. Green DP, Hotchkiss RN, Pederson WC: Green's Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
References:
- Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
Question 42High Yield
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?

Explanation
The patient has no clinical or observed signs of sepsis. The skin just proximal to the gangrenous tissue appears somewhat hyperemic and is clearly viable. These wounds should be managed much like burn wounds. Moist dressings should be used until the tissue clearly demarcates. Much of the insult may simply be superficial and only require late debridement. McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective. Am J Orthop 1999;28:21-26.
Question 43High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 44High Yield
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?

Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 45High Yield
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a supple plantigrade foot that would benefit from a drop foot brace to prevent catching of the toes. Tendon transfer should not be considered until the patient has undergone bracing. Achilles tendon lengthening is not necessary because the foot is plantigrade and flexible. Nerve grafting is not indicated because of the length of time the peroneal nerve palsy has been present. Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
References:
- Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int 1996;17:425-439.
Question 46High Yield
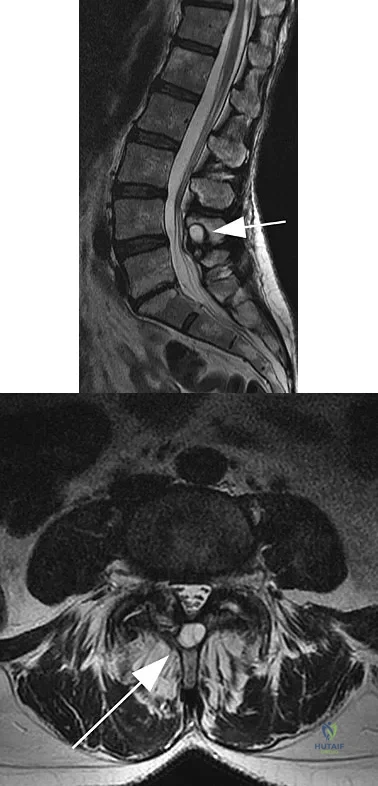
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?
Explanation
The arrow is pointing to a cystic-appearing structure with high signal intensity on T2-weighted image sequencing. It appears to be contiguous with the hypertrophied right facet joint, which appears to also have high signal intensity. The mass significantly narrows the right lateral recess. The high signal intensity suggests that this is a fluid-filled mass. In addition, the facet joints are degenerative and there is a very mild degree of anterolisthesis on the sagittal image. These findings make a lumbar synovial cyst the most likely diagnosis. Most lumbar juxtafacet cysts are observed at the L4-5 level, extradurally and adjacent to the degenerative facet joint. They may contain synovial fluid and/or extruded synovium. Presentation is indistinguishable from that of a herniated disk. The etiology of spinal cysts remains unclear, but there appears to be a strong association between their formation and worsening spinal instability. They occasionally regress spontaneously and may respond to aspiration and injection of corticosteroids, though there is a high recurrence rate with nonsurgical management. Synovial cysts resistant to nonsurgical management should be treated surgically. If the patient's symptoms can be attributable to radicular findings, a microsurgical decompression that limits further destabilization should suffice. However, if there is significant low back pain attributable to spinal instability, decompression and fusion remains an appropriate option. Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972. Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Question 47High Yield
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?

Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 48High Yield
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
Explanation
Explanation
The preferred approach is posterolateral, placing the sural nerve most at risk. The dorsal intermediate cutaneous nerve is anterolateral to the ankle, and the medial and lateral plantar branches are medial and inferior to the surgical site. The saphenous nerve is anteromedial and away from the surgical approach. Swanson TV, Bray TJ, Holmes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
References:
- Lawrence S, Botte M: The sural nerve of the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 49High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
- Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 50High Yield
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
Explanation
Explanation
Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates. Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248. Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289. Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354. Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200. Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372. Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170. Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
References:
- Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.
Question 51High Yield
The injury seen in the CT scan shown in Figure 56 is related to or associated with injury to which of the following structures?
Explanation
Explanation
The right syndesmosis appears disrupted on the CT scan when compared to the normal left side. CT can be helpful in determining injury to the syndesmosis, especially with occult clinical findings. Ebraheim NA, Lu J, Yang H, et al: The fibular incisure of the tibia on CT scan: A cadaver study. Foot Ankle Int 1998;19:318-321. Ebraheim NA, Lu J, Yang H, et al: Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int 1997;18:693-698.
References:
- Harper MC: Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int 2001;22:15-18.
Question 52High Yield
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of
Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 53High Yield
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?
Explanation
Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
References:
- Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 54High Yield
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
Explanation
The major criteria for the diagnosis of fat embolism syndrome include hypoxemia (PaO2 of less than 60 mm Hg), central nervous system depression, and a petechial rash that is most often located in the axillae, conjunctivae, and palate. The rash is often transient. Tachycardia, pyrexia, anemia, thrombocytopenia, and the presence of fat in the urine are all considered minor criteria. To establish the diagnosis of fat embolism syndrome, one major and four minor signs should be present. Pulmonary embolism, which is the major differential diagnosis, usually is not associated with conjunctival petechia or thrombocytopenia.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 55High Yield
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?
Explanation
Explanation
62b 62c 62d 62e The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
References:
- Ghanem I: The management of osteoid osteoma: Updates and controversies. Curr Opin Pediatr 2006;18:36-41.
Question 56High Yield
A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and physical therapy. Following a fall in a game, he noted a recurrence of neck pain without radicular signs or symptoms. Additional nonsurgical management over the past few months has failed to provide relief. A cervical MRI scan shows a right-sided C5-6 herniation without any evidence of disk disease at other cervical levels. The patient desires to continue his career as a professional soccer player. What treatment offers the best long-term option for return to play?
Explanation
Explanation
The patient has chronic neck pain that is affecting his career as a professional soccer player. Although he had signs and symptoms of a right C6 radiculopathy, neck pain is his only current symptom. Therefore, procedures to address the relief of radiculopathy (keyhole foraminotomy and transforaminal epidural steroid injection) are likely to be ineffective. Although Watkins and others have described continuing nonsurgical management for symptomatic herniated disks and return to play only when asymptomatic, the patient has not found relief with these modalities. A single-level cervical fusion (either postoperative or congenital) generally is not considered a contraindication for return to play in collision or contact sports. Therefore, anterior cervical fusion at C5-6 offers the best long-term option for return to play. Watkins RG: Cervical spine injuries in athletes, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 373-386. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
References:
- Garvey T, Transfeldt EE, Malcolm JR, et al: Outcome of anterior cervical discectomy and fusion as perceived by patients treated for dominant axial-mechanical cervical spine pain. Spine 2002;27:1887-1895.
Question 57High Yield
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
Recovery of upper extremity motor function after a cerebrovascular accident follows a predictable pattern. The greatest amount of recovery is seen within the first 6 weeks. Return of function proceeds from proximal to distal. Shoulder flexion occurs first, followed by return of flexion to the elbow, wrist, and fingers. Return of forearm supination follows the return of finger flexion.
Question 58High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 59High Yield
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of
Explanation
Explanation
4b The history and radiographs indicate a Lisfranc fracture-dislocation of the foot. The radiographs show the classic "fleck sign," which is an avulsion of the Lisfranc ligament from the base of the second metatarsal. Most authors recommend open reduction and internal fixation of this injury. Closed reduction can be attempted, but anatomic reduction is unlikely because of the interposed bone fragments and soft tissues. Standard radiographs are not reliable in identifying 1 to 2 mm of subluxation of the tarsometatarsal joint. The tarsometatarsal joint has a poor tolerance to even mild subluxation, and the resulting decrease in joint contact area increases the likelihood of posttraumatic arthritis. Open reduction with the joint visible allows more anatomic reduction and internal fixation of larger osteochondral fragments or excision of smaller interposed fragments. Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
References:
- Murphy GA: Fractures and dislocations of the foot, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, vol 2, pp 1956-1960.
Question 60High Yield
Figures 30a and 30b show the MRI scans of a 51-year-old woman who has had an enlarging soft-tissue mass in her right thigh for the past 18 months. Examination reveals no inguinal adenopathy. Results of a biopsy show a high-grade sarcoma. A bone scan is unremarkable, and a CT scan of the chest shows no evidence of pulmonary metastasis. According to the Musculoskeletal Tumor Society (MSTS) staging system, the tumor should be classified as what stage?
Explanation
Explanation
30b According to the MSTS staging system, soft-tissue sarcomas are staged according to the following factors: grade, site, and metastasis. Roman numerals are used to designate malignant tumors, and Arabic numerals are used for benign tumors. Low-grade malignant tumors are staged as I while intermediate- and high-grade tumors are staged as II. Site is defined as intracompartmental (A) or extracompartmental (B). Any metastasis is staged as III. This patient has a high-grade tumor (II), and the MRI scans show that it is confined to a single compartment; therefore, it is staged as IIA. There is no evidence of metastatic disease. Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF: Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996;14:1679-1689.
References:
- Wunder JS, Healey JH, Davis AM, Brennan MF: A comparison of staging systems for localized extremity soft tissue sarcoma. Cancer 2000;88:2721-2730.
Question 61High Yield
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
Explanation
10b The radiographs show fragmentation of the inferior pole of the patella. This finding, along with the clinical presentation, is most consistent with Sindig-Larsen-Johansson disease. This is an overuse syndrome commonly seen in boys ages 9 to 11 years. The differential diagnosis includes bipartite patella and patellar sleeve fracture. Like most overuse syndromes, Sindig-Larsen-Johansson disease responds to activity modification and nonsteroidal anti-inflammatory drugs. While symptoms usually resolve with short periods of activity restriction, radiographic findings may persist. Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
References:
- Stanitski CL: Anterior knee pain syndromes in the adolescent, in Schafer M (ed): Instructional Course Lectures 43. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1994, pp 211-220.
Question 62High Yield
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon's) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include

Explanation
The examination and MRI scan confirm a subscapularis rupture and dislocation of the long head of the biceps tendon. The greatest return of function will result from repair of the subscapularis and tenodesis of the biceps tendon. Physical therapy alone will result in inadequate healing of the subscapularis and will not address the biceps tendon. While biceps tenotomy is an option, it will not provide the same level of pain relief and return of function as a tenodesis in a young, active man. There is no evidence for a supraspinatus tear. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 63High Yield
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures. Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Question 64High Yield
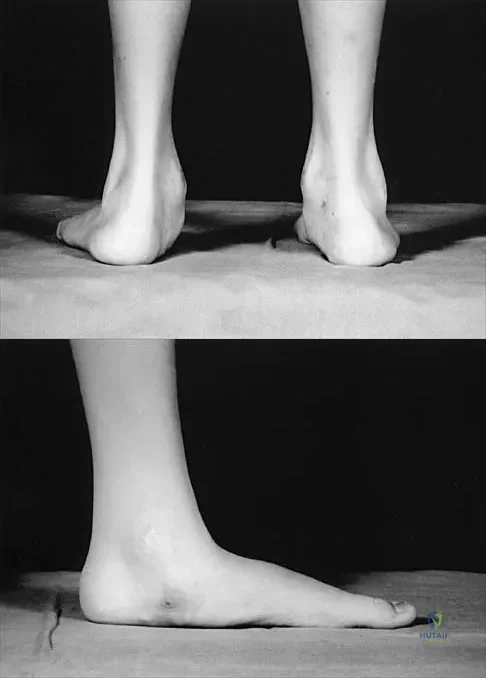
Figures 50a and 50b show the standing clinical photographs of a 12-year-old boy who has had increasing pain in the left foot for the past 9 months. He reports that the pain is activity related, aching in nature, and localized to the medial aspect of the midfoot and hindfoot. History reveals that he sustained a puncture wound located superior and posterior to the medial malleolus from a plate glass window 18 months ago. Examination reveals no restriction of ankle or subtalar motion, normal neurovascular status, no masses, and a well-healed 1.5-cm laceration posterior to the superior aspect of the medial malleolus. Inversion strength of the foot is decreased to grade 3/5. Radiographs of the foot show no bony abnormalities. Treatment should consist of
Explanation
The photographs show a planovalgus posture of the foot. The foot deformity and decreased inversion strength are secondary to laceration of the posterior tibial tendon 18 months ago. If the injury had been recognized acutely, optimal treatment would have consisted of repair of the tendon; however, contracture now precludes that possibility. Therefore, transfer of the flexor digitorum longus or flexor hallucis longus is the preferred treatment. In adults with posterior tibial dysfunction, the entire tendon is typically degenerated and the transfer must be anchored through a drill hole in the navicular. In this patient, the distal end of the posterior tibial tendon is a satisfactory insertion site. Lengthening osteotomy of the calcaneus could be combined with the tendon transfer if the patient had a fixed deformity of the foot. UCBL orthoses and an ankle-foot orthosis are not considered good long-term solutions for a 12-year-old patient. Mosca VS: Flexible flatfoot and skewfoot, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 355-376.
Question 65High Yield
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer's representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture's representative suggests a partnership in a boat costing $200,000. The manufacture's representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
Explanation
Rejecting this proposal is the only appropriate course of action. Accepting it would, in essence, be receiving a huge gift from industry in the form of a sailboat. Physicians frequently assert that they are not influenced by gifts and relationships with industry representatives, but evidence is to the contrary. Such an arrangement constitutes a tremendous incentive to use the manufacturer's products. The fact that the boat partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6-8. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf Opinions on Ethics and Professionalism: The Orthopaedic Surgeon's Relationship with Industry (Document 1204), in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 36-40. www.aaos.org/about/papers/ethics/1204eth.asp AdvaMed Code of Ethics on Interactions with Health Care Professionals, Advanced Medical Technology Association, Washington, DC. www.AdvaMed.org
Question 66High Yield
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63. Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Question 67High Yield
Figure 23 shows failure of the femoral stem in a patient. What is the most likely reason for the failure?
Explanation
Explanation
A two-dimensional stress analysis has been used to study the effects of some of the factors leading to early fatigue failure of the femoral stem in total hip arthroplasty. It has been demonstrated that loss of proximal stem support at the level of the calcar femorale and subsequent stem stress can lead to fatigue failure. In addition, the role of body weight and range of cyclic stress fluctuation play an important role in fatigue life under conditions where the stem has lost proximal support. These results indicate that stem design could be improved by incorporating some means of adequate support at the calcar femorale where maximum tensile stresses are found to occur. Femoral component fracture is a rare but well-documented complication after total hip arthroplasty. Historically, most stem fractures occur at the middle third of the implant where proximal stem loosening and solid distal stem fixation result in cantilever bending and eventual fatigue failure. The component shown is a modular fluted cementless stem that occasionally fractures at the modular junction in patients with poor proximal bone support. Andriacchi TP, Galante JO, Belytschko TB, et al: A stress analysis of the femoral stem in total hip prostheses. J Bone Joint Surg Am 1976;58:618-624.
References:
- Gruen TA, McNeice GM, Amstutz HC: "Modes of failure" of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop 1979;141:17-27.
Question 68High Yield
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?
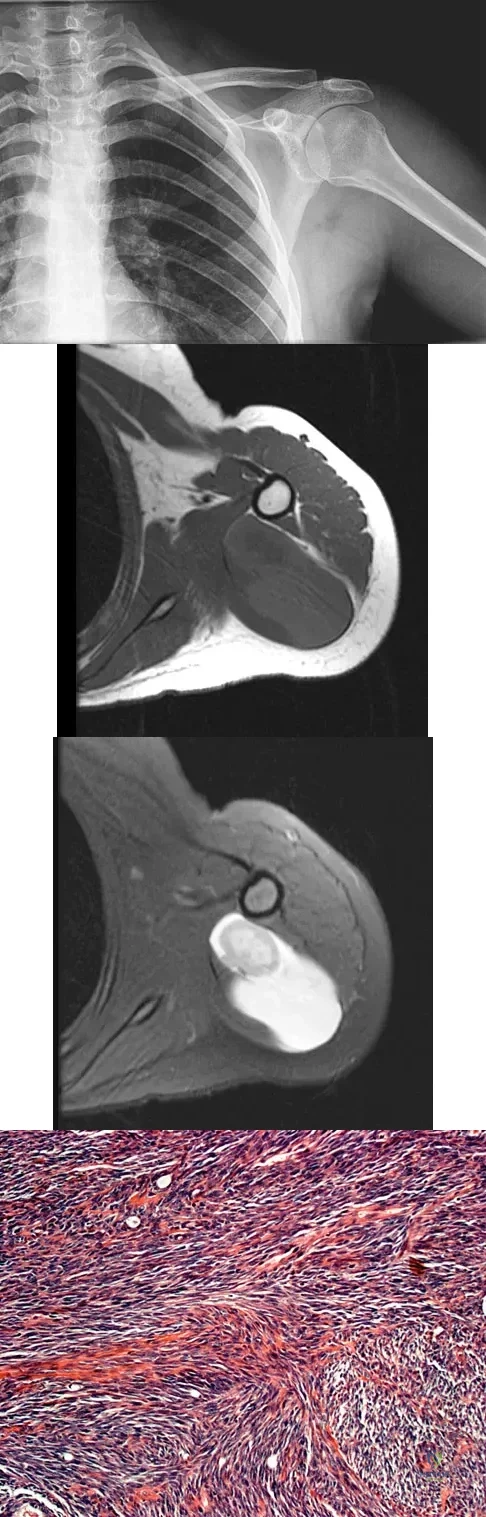
Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 69High Yield
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
Explanation
Metastatic lesions to bone are usually located in the axial and proximal appendicular skeleton. Metastases below the elbow and knee are rare, but when they do occur they are most commonly from lung carcinoma. Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 70High Yield
Which of the following statements describing chordomas is false?
Explanation
Explanation
Casali and associates provided a recent review of the treatment options for chordomas. These tumors are not radiosensitive; however, modern intensity modulated radiosurgery techniques may be of value. The combination of surgery and radiotherapy compared to surgery alone results in the same disease-free survival time. Complete surgical resection of the chondroma with clean margins offers the best survival; however, its location may make total removal impossible. Thus subtotal resection followed by radiotherapy results in better survival despite the tumor's lack of radiosensitivity.
Question 71High Yield
A 72-year-old woman with rheumatoid arthritis who underwent primary total knee arthroplasty 2 years ago has had diffuse knee pain that developed shortly after the surgery. The patient has difficulty with stair descent and arising from chairs. Evaluation for infection is negative. AP and lateral radiographs are shown in Figure 26. Management should now consist of
Explanation
Explanation
The radiographs show posterior flexion instability that is the result of flexion-extension gap imbalance and/or posterior cruciate ligament incompetence after a posterior cruciate-retaining total knee arthroplasty. The radiographs also show anterior femoral displacement on the tibia. Pagnano and associates reported on a series of patients with painful total knee arthroplasties who had been previously diagnosed as having pain of unknown etiology, showing that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
References:
- Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 72High Yield
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
Explanation
Chordomas are very radio- and chemotherapy resistant; therefore, en bloc resection with a negative margin is the preferred treatment. Lesions at or below S3 can be resected without compromising pelvis stability, and continence usually is maintained. The mean survival rate for patients with sacral chordomas is approximately 7 years. Patients with chordoma of the mobile (cervical, thoracic, or lumbar) spine have a mean survival rate of approximately 5 years. This difference is most likely the result of an earlier diagnosis. Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133. Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
References:
- Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 73High Yield
A 21-year-old college student fell from a balcony and landed on his outstretched right hand. He is seen in the emergency department 4 hours later and reports wrist pain and diffuse hand numbness. The volar forearm compartment is soft and there is no pain with passive finger extension. Radiographs are shown in Figures 25a and 25b. Definitive treatment should consist of
Explanation
Explanation
25b A spectrum of perilunate injury patterns exists, with the dorsal trans-scaphoid perilunate fracture-dislocation being the most common. Perilunate injuries are highly unstable complex carpal disruptions that are not amenable to closed treatment. Open reduction and internal fixation is necessary to accurately restore carpal alignment via fracture reduction and fixation and intercarpal ligament repair. Controversy exists regarding the need for dorsal or combined dorsal and volar approaches. Based on the radiographic findings of a volar dislocation of the lunate and the associated median nerve injury, the patient requires open reduction and internal fixation via combined dorsal and volar approaches with a concomitant carpal tunnel release. Herzberg G, Forissier D: Acute dorsal trans-scaphoid perilunate fracture-dislocations: Medium-term results. J Hand Surg Br 2002;27:498-502. Melone CP Jr, Murphy MS, Raskin KB: Perilunate injuries: Repair by dual dorsal and volar approaches. Hand Clin 2000;16:439-448.
Question 74High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 75High Yield
Figure 46 shows the AP radiograph of an active 80-year-old patient with an acetabular fracture. The fracture was initially managed nonsurgically; however, the patient is now scheduled to undergo total hip arthroplasty. What is the treatment of choice for the contained acetabular bone defect?
Explanation
Explanation
Acetabular fractures can result in a relative or actual acetabular bone defect. The medial blow-out fracture of the acetabulum has united well in this patient. It is likely that a medial shell of bone will be present during hip arthroplasty. The femoral head may be used as morcellized or structural bone to augment the medial defect and is preferred to structural allograft. Bipolar hip arthroplasty is notorious for medial migration in patients without a medial bone defect; therefore, it will not be a good choice in this patient. Filling the defect with methylmethacrylate cement, though an option, is not the best option in this active patient with an extensive medial defect. A double-bubble acetabular cup is used for patients with deficiency of the bone in the dome region. Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-141.
References:
- Bellabarba C, Berger RA, Bentley CD, et al: Cementless acetabular reconstruction after acetabular fracture. J Bone Joint Surg Am 2001;83:868-876.
Question 76High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature. Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233. Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526. Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
References:
- Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 77High Yield
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include

Explanation
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 78High Yield
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Explanation
Explanation
Plate and screw fixation of allograft is associated with the highest incidence of union but also the highest prevalence of allograft fracture. Conversely, intramedullary fixation is associated with a higher incidence of nonunion but fewer fractures. Step-cut osteotomies are not associated with a higher incidence of union.
References:
- Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 79High Yield
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
Explanation
Elbow release and triceps transfer to restore motion can be performed in children who are age 4 years and older. The ability to flex the elbow either actively or passively is of great assistance in activities of daily living. Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
References:
- Caroll RE, Hill NA: Triceps transfer to restore elbow flexion: A study of fifteen patients with paralytic lesions and arthrogryposis. J Bone Joint Surg Am 1970;52:239-244.
Question 80High Yield
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 81High Yield
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and

Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 82High Yield
An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
Explanation
Explanation
51b Most radial nerve palsies associated with closed fractures of the humerus resolve spontaneously, including Holstein-Lewis lesions (radial nerve palsy associated with oblique distal third fractures of the humerus). Initial sign of recovery at the brachioradialis may not occur for 4 months. There has been no evidence of deleterious effects occurring during this observation period. There are advocates of early exploration of the nerve. Exploration in the intermediate period between 1 and 4 months is not supported. As overall alignment of the fracture is acceptable, there is no need for hardware exchange until nonunion is clearly identified. Shao YC, Harwood P, Grotz MR, et al: Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-1652.
Question 83High Yield
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 84High Yield
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?
Explanation
Explanation
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
References:
- Sartor O: Radioisotopic treatment of bone pain from metastatic prostate cancer. Curr Oncol Rep 2003;5:258-262.
Question 85High Yield
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
The patient has sustained a low-velocity, low-caliber gunshot wound to the foot. Because the injury occurred within a period of 8 hours, this is classified as a type I wound. Several studies support the use of surface debridement, cleansing, and sterile dressings as the treatment of choice. More aggressive measures are reserved for high-velocity injuries and shotgun injuries. Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31. Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Question 86High Yield
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?
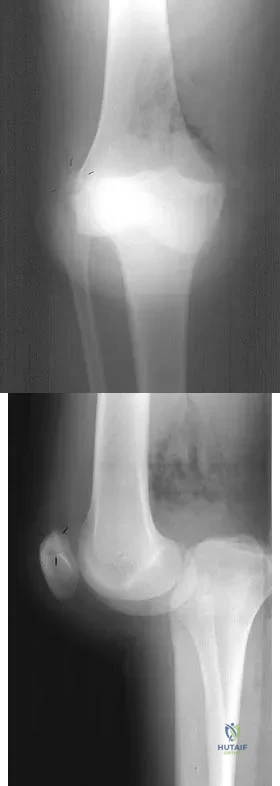
Explanation
The radiographs show a posterior knee dislocation. Knee dislocations almost always involve rupture of both the anterior and posterior cruciate ligaments. Collateral ligament injuries also are common. Arterial, nerve, and tendon injuries each occur in less than half of knee dislocations. Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Question 87High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 88High Yield
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?

Explanation
Excessive flexion gap tightness can be addressed with a variety of techniques; including: (a) recess and release the posterior cruciate ligament; (b) resect a posterior slope in the tibia; (c) avoid an oversized femoral component that moves the posterior condyles more distally; (d) resect more posterior femoral condyle and use a smaller femoral component placed more anteriorly; and (e) release the tight posterior capsule and balance the collateral ligaments.
Question 89High Yield
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?

Explanation
Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment. Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Question 90High Yield
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
Explanation
Arthrodesis of the failed infected total knee arthroplasty may be accomplished by external fixation, intramedullary rod fixation, and dual plates and screws. External fixation runs the risk of pin tract infection, although after its removal, there are no metal surfaces left in place. Intramedullary rods have been used successfully in the treatment of infected total knees, although they also leave metal within the region of the infection. The dual plate technique of knee fusion is useful in patients with rheumatoid arthritis who require fusion in the absence of infection because it provides good initial stability and avoids the use of external pins. However, in the face of infection, the large surface area of the screws and plates may serve as a site for bacteria to hide within a glycocalyx and make eradication of the infection almost impossible.
References:
- Windsor RE: Knee arthrodesis, in Insall JN, Windsor R, Kelly M, et al (eds): Surgery of the Knee. New York, NY, Churchill Livingstone, 1993, pp 1103-1116.
Question 91High Yield
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
Explanation
The effects of cigarette smoking and smoking cessation on spinal fusion have been studied extensively. Although permanent smoking cessation is ideal, significant improvements in fusion rates are seen in patients who avoid smoking for greater than 6 months postoperatively.
Question 92High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?

Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 93High Yield
What are the five major compartments of the foot?
Explanation
Explanation
The five major compartments of the foot are medial, lateral, central, interosseous, and calcaneal. There is no dorsal compartment in the foot. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 262-264.
References:
- Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 94High Yield
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient's left knee. Abnormal findings include

Explanation
The MRI scans show meniscal tissue extending across the entire lateral compartment, revealing a discoid lateral meniscus. The increased signal within the lateral meniscal tissue indicates a tear. Discoid lateral menisci are congenital variants that often present with mechanical symptoms in adolescents. The other structures in the knee are normal. Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Question 95High Yield
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?
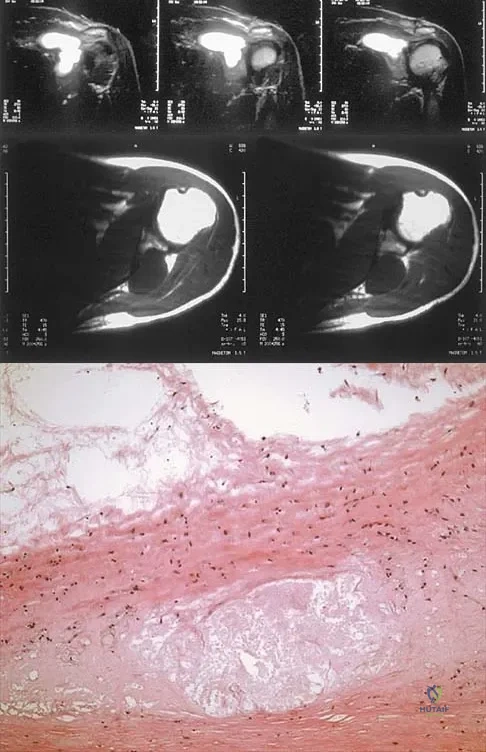
Explanation
A ganglion cyst arising from the posterior labrum of the shoulder is a known cause of suprascapular nerve impingement. The MRI characteristics of low-signal intensity on T1 and high-signal intensity on T2 are seen in lesions with a high fluid content. The histology shows a cavity with a thin fibrous lining. Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Question 96High Yield
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
Explanation
7b 7c The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Question 97High Yield
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Explanation
Lonner and associates conducted a prospective study to determine the reliability of analysis of intraoperative frozen sections for the identification of infection during 175 consecutive revision total joint arthroplasties (142 hips and 33 knees). The mean interval between the primary arthroplasty and the revision arthroplasty was 7.3 years (range, 3 months to 23 years). Of the 175 patients, 23 had at least 5 polymorphonuclear leukocytes per high-powered field on analysis of the frozen sections and were considered to have an infection. Of these 23 patients, five had 5 to 9 polymorphonuclear leukocytes per high-powered field and 18 had at least 10 polymorphonuclear leukocytes per high-powered field. The frozen sections for the remaining 152 patients were considered negative. On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field. The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection. Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813. Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558. Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Question 98High Yield
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
Explanation
Results show that patients who underwent humeral head replacement for fracture almost routinely report pain relief, but functional reports vary. The most commonly reported difficulty is the use of weight in the overhead position with wide variation in active elevation. Factors found to affect active elevation include age, humeral offset, greater tuberosity positioning, and four-part (as compared with three-part) fractures. Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
References:
- Hawkins RJ, Switlyk P: Acute prosthetic replacement for severe fractures of the proximal humerus. Clin Orthop 1993;289:156-160.
Question 99High Yield
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?
Explanation
Explanation
31b The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
References:
- Kier R, McCarthy SM: Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 1990;14:395-396.
Question 100High Yield
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction. Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220. Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
References:
- Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
