Orthopedic Board Review: 100 High-Yield MCQs (Set 591)

Key Takeaway
This page offers 100 high-yield Orthopedic Surgery MCQs in Mock Exam Set #591. Ideal for ABOS, OITE, and FRCS board exam preparation, it helps surgeons and residents test their knowledge, identify weaknesses, and master crucial concepts for certification success.
Mastering the Posterior Lateral Thorax Approa...
00:00
Start Quiz
After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?
Explanation
Explanation
It is imperative to recognize the need for a position screw (syndesmosis screw) to hold the syndesmosis in proper alignment when surgically stabilizing an ankle fracture. Although many different fracture patterns are suspicious for a disrupted syndesmosis, the only sure way to assess the syndesmosis is to stress it with abduction and external rotation of the talus and attempt to displace the fibula from the incisura fibularis. Under fluoroscopy, the talus will move laterally and displace the fibula, show a valgus talar tilt, or show an increase in the medial clear space. If any or all of these signs occur, a syndesmosis screw is inserted after making sure that the fibula is reduced into the incisura fibularis. This screw may traverse three or four cortices but must not act as a lag screw. It usually is inserted with the ankle in maximal dorsiflexion, although this is probably not necessary because it is almost impossible to overcompress the syndesmosis. The diameter of the screw does not make any difference. It may or may not be removed but not before 3 months. Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
References:
- Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 3High Yield
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient's pain?
Explanation
Explanation
21b The difference in the clinical results combined with the laboratory findings points to infection. While there is a significant risk of false-positive findings with aspiration, the fact that two successive aspirations grew the same organism strongly suggests infection. The radiograph shows that there is more radiolucency around the left acetabular component than the right component. White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 1377-1385.
References:
- Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 4High Yield
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
Explanation
64b 64c 64d 64e The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Question 5High Yield
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?

Explanation
Because of the previously transferred bone block of coracoid and short arm flexors, the musculocutaneous nerve often scars along the anteroinferior glenohumeral capsule. Mobilization of this tissue places the nerve at greatest risk. The axillary nerve is also potentially at risk, but this is nonspecific to prior surgery, particularly the Bristow procedure. Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 98-116.
Question 6High Yield
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?

Explanation
Tooth avulsions can occur in contact or collision sports. An avulsed tooth is a medical emergency. The likelihood of survival of the tooth depends on the length of time that the tooth is out of the socket and the degree to which the periodontal ligament is damaged. The tooth should be handled only by the crown end and not the root end. It can be rinsed of debris with water or normal saline solution. The tooth should not be brushed or cleaned otherwise. During transport, the tooth must be kept moist. An avulsed tooth can be transported in whole milk, saliva, sterile saline solution, or commercially available kits with physiologic buffer solutions. The tooth and the athlete should be transported to the dentist for reinsertion as soon as possible and preferably within an hour. Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135. Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Question 7High Yield
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Explanation
Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene's molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first 5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of 3 to 5 years has a direct effect on wear of polyethylene. Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122. Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
References:
- Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 8High Yield
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?

Explanation
There is no evidence that early weight bearing enhances ultimate rehabilitation. At the other extreme, weight bearing should not be delayed for a prolonged period of time. In a young, healthy individual, the rigid plaster dressing appears to be the safest method of protecting the wound during the early postoperative period. If the wound appears to be secure, early partial weight bearing can be safely initiated. Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Question 9High Yield
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 10High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 11High Yield
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of

Explanation
The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence. Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Question 12High Yield
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 13High Yield
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?

Explanation
Postoperative migration of lumbar interbody fusion cages is a rare complication. It is most commonly seen after placement of the cages through a posterior approach, with instability of the final construct. It is not associated with the design of the cage, the type of graft used, or a resultant pseudarthrosis. McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
Question 14High Yield
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?

Explanation
The MRI scan shows increased signal intensity along the deep fibers of the supraspinatus near its insertion. This is typical of tendinosis and a probable partial-thickness rotator cuff tear. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 15High Yield
The Lisfranc ligament connects the base of the
Explanation
Explanation
The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
References:
- Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 16High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?

Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 17High Yield
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of

Explanation
In patients with myelomeningocele, the presence of bilateral hip dislocation does not affect ambulation, bracing requirements, sitting ability, degree of scoliosis, or level of comfort. There is little evidence to support active treatment of bilateral hip dislocations in patients with myelomeningocele proximal to L4. Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Question 18High Yield
Figure 53 shows the pedigree of a family with an unusual type of muscular dystrophy. This pedigree is most consistent with what type of inheritance pattern?

Explanation
The pedigree documents involvement of male offspring only, and it also shows transmission through an uninvolved female carrier. This inheritance pattern is most consistent with a x-linked recessive inheritance. It would be inconsistent with a dominant inheritance pattern unless there was incomplete penetrance. Autosomal-recessive inheritance would be possible only if the family member labeled II.F was also a carrier of the same gene; however, this is unlikely. Mitochondrial inheritance is possible, but as with autosomal patterns, mitochondrial inheritance normally affects both male and female offspring. It is transmitted only through the maternal line.
Question 19High Yield
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?
Explanation
Explanation
Motion segments that demonstrate more than 4 mm of translation or 10 degrees of angulation compared with adjacent motion segments on flexion-extension radiographs have excessive motion and instability. Anterior marginal osteophytes form at the insertion of the annulus from increased forces but do not indicate increased motion. A spondylolisthesis or lateral listhesis is often static without increased motion. More than 3.5 mm of translation or 11 degrees of angulation is considered instability criteria for the cervical spine. Internal disk disruption does not denote instability. Boden SD, Wiesel SW: Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1990;15:571-576.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 20High Yield
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Explanation
Explanation
16b 16c This is a classic appearance for an osteosarcoma. The radiographs reveal a mixed osteolytic and osteoblastic lesion in a skeletally immature patient in the distal right femoral metaphysis. The pain pattern with progressive symptoms leading to the presence of night pain is also typical for this condition. The biopsy specimen reveals pleomorphic cells and the presence of osteoid. The current standard of care in the treatment of osteosarcoma is neoadjuvant chemotherapy followed by surgical resection or amputation followed by additional postoperative chemotherapy. Osteosarcoma is not radiosensitive. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
References:
- McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 21High Yield
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
Explanation
The flexor digitorium longus is the commonly accepted tendon transfer for posterior tibial tendon insufficiency. The flexor hallucis longus has to be carefully rerouted to avoid crossing the neurovascular bundle and has not been shown clinically to provide superior results to flexor digitorum longus transfer. Use of the peroneus longus results in loss of plantar flexion strength of the first metatarsal, contributing to the flatfoot deformity. The anterior tibial tendon is in the anterior compartment and fires out of phase with the posterior tibial tendon. Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
References:
- Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 22High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 23High Yield
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
Explanation
Metastatic lesions to bone are usually located in the axial and proximal appendicular skeleton. Metastases below the elbow and knee are rare, but when they do occur they are most commonly from lung carcinoma. Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 24High Yield
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?

Explanation
This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 25High Yield
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a

Explanation
Complications of thermal capsule shrinkage or accelerated rehabilitation include capsule ablation. Since the original surgery did not include labral reattachment, findings of a Bankart lesion or a glenoid fracture from a nontraumatic injury are unlikely. Subscapularis detachment or biceps subluxation is a postoperative complication of open repairs. Failure of early postoperative instability treatment should not produce loose bodies. Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Question 26High Yield
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of

Explanation
The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 27High Yield
A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
Explanation
Explanation
The patient has a both-bone fracture with a comminuted radial shaft. Open reduction and internal fixation of both bones is the treatment of choice. In the past, Chapman and associates recommended bone grafting radial shaft fractures with more than 30% comminution of the circumference. This has remained the recommendation in most textbooks. More recent studies, where modern biologic plating techniques were used, found that the addition of bone graft to comminuted fractures was not necessary because the union rate did not differ from that of nongrafted comminuted fractures. Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297. Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169. Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
References:
- Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
Question 28High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion. Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Question 29High Yield
When performing the exposure for an anterior approach to the cervical spine, the surgical dissection should not enter the plane between the trachea and the esophagus and excessive retraction should be avoided to prevent injury to the
Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal and superior laryngeal nerves are both at risk during the exposure but are not located between the trachea and the esophagus. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 30High Yield
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
Explanation
Pediatric intracapsular hip fractures are challenging because of the high rates of complications, including osteonecrosis and varus malunion. These patients should be treated as emergencies. Principles of treatment include anatomic reduction with internal fixation. Screw fixation short of the physis is preferred and may need to be supplemented with spica cast immobilization. Fixation may be achieved with smooth pins across the physis when little metaphyseal bone is available. Fixation across the physis with threaded screws is acceptable only when the patient is close to skeletal maturity. Pediatric hip screws are appropriate if immediately available. Emergent open reduction, capsulotomy, or joint aspiration may decrease the rate of osteonecrosis. Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343. Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420. Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
References:
- Morsy HA: Complications of fracture of the neck of the femur in children: A long-term follow-up study. Injury 2001;32:45-51.
Question 31High Yield
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
Explanation
A rib stress fracture, the most common injury to the thorax in rowing athletes, generally occurs during periods of intense training with a low stroke rate and heavy loads. It is characterized by the sudden onset of sharp, localized chest pain while rowing. The fifth through the ninth rib is generally affected, and the diagnosis is best established with a bone scan. An intercostal muscle strain generally has an insidious onset and may be poorly localized. Costochondritis affects the anterior costochondral junction. A pneumothorax and an empyema can cause nonlocalized chest pain but are associated with respiratory distress and systemic physical findings. Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
References:
- Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
Question 32High Yield
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
Explanation
29b The studies show marginal syndesmophyte formation characteristic of ankylosing spondylitis. These patients typically have diffuse ossification of the disk space without large osteophyte formation. DISH typically presents with large osteophytes, referred to as nonmarginal syndesmophytes. In this patient, the zygoapophyseal joints are fused rather than degenerative as would be seen in rheumatoid arthritis, and the costovertebral joints are also fused. Osteopetrosis does not normally ankylose the disk space. McCullough JA, Transfeldt EE: Macnab's Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
References:
- Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 33High Yield
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
Explanation
Approximately 75% of people have the artery on the left side between T9 and T11. Its relevance to iatrogenic spinal cord problems is still uncertain. Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
References:
- Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 34High Yield
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
Explanation
Recurrent dislocation following total hip arthroplasty is a difficult problem to correct. Studies conducted by the Mayo Clinic show a failure rate of close to 40% with surgical treatment. A variety of methods have been successful, but no specific approach has been reported to be the most predictably successful. To select and institute the proper treatment option, the cause of the dislocation must be identified. Surgical options fall into several broad categories that include increasing soft-tissue tension (trochanteric advancement or longer neck lengths) or more stable articulation (larger diameter head component, bipolar prosthesis, or a constrained component). In a series of total hip arthroplasties done with a constrained cup, the loosening rates of the cup and the stem were reported to be 6% each, comparable to a reported series of complex revision total hip arthroplasties at a similar follow-up interval. Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
References:
- Goetz DD, Capello WN, Callaghan JJ, Brown TD, Johnston RC: Salvage of a recurrently dislocating total hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.
Question 35High Yield
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
Explanation
The MRI scan reveals a transection of the biceps muscle. The underlying brachialis is intact. This injury can occur as a result of a cord wrapped around the upper arm. Care should be taken to ensure that there is no concurrent vascular injury. A posterior subcutaneous lipoma appears as a well-encapsulated mass on T2-weighted images. Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
References:
- Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 36High Yield
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
References:
- Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 37High Yield
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
Explanation
Microvascular studies have shown that the majority of the blood supply to the cruciate ligaments comes from the middle geniculate artery, although there is collateral flow through the other geniculates and from bone. Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
References:
- Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 38High Yield
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
Explanation
23b Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening. Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496. Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
References:
- Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 39High Yield
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
Explanation
49b The fracture of the proximal phalanx is clearly displaced. There is slight comminution at the area of the fracture. Closed reduction is likely to fail due to the forces of the extensor, flexor, and intrinsic mechanisms. Percutaneous fixation, unlike open fixation techniques, avoids likely problems with stiffness. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 40High Yield
Figures 34a through 34c show the radiographs of a 51-year-old woman who injured her elbow in a fall from standing height. Examination reveals that elbow range of motion is limited by pain only. Management should consist of
Explanation
Explanation
34b 34c The radiographs show a small minimally displaced radial head fracture that is amenable to nonsurgical management. Early range-of-motion exercises will best restore function and minimize stiffness. A long arm cast for any length of time will result in severe elbow stiffness. Morrey BF: Radial head fracture, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 341-364.
References:
- Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 41High Yield
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Explanation
Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.
Question 42High Yield
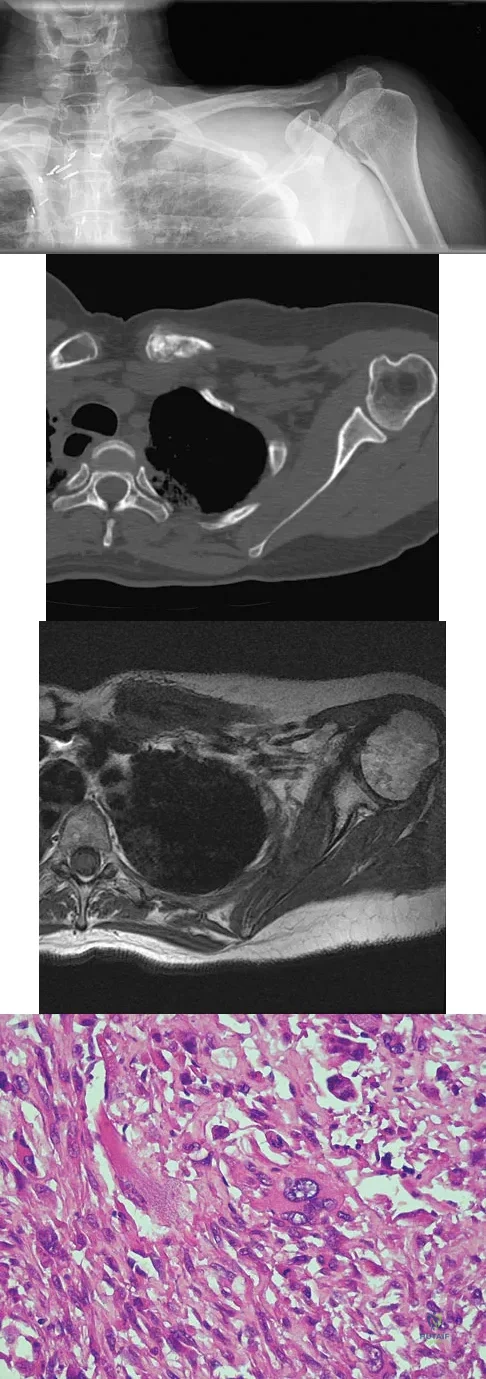
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin's lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?
Explanation
Radiation-associated sarcomas typically occur at least 5 years following radiation therapy, in the radiation therapy field, and with different histology than the original disease. The radiograph shows a lytic destructive lesion of the medial clavicle. The radiographic differential could include any of the above etiologies. The CT and MRI scans show this same reaction with extension into the adjacent soft tissue and periosteal reaction. These findings eliminate a degenerative process or radiation-induced osteonecrosis but do not distinguish between a neoplastic and infectious process. A PET scan showed marked uptake in the distal clavicle, which is more consistent with a malignant neoplastic process than a reactive process, like that of an infection. These findings, combined with the cellular atypia and bone formation on the biopsy specimen, confirm the diagnosis of radiation-associated sarcoma. In this older patient, radiation-associated sarcoma appears in an unusual location secondary to her previous radiation treatment in that region, which can occur 3 to 50 years after previous radiation therapy. Shaheen M, Deheshi BM, Riad S, et al: Prognosis of radiation-induced bone sarcoma is similar to primary osteosarcoma. Clin Orthop Relat Res 2006;450:76-81.
Question 43High Yield
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?

Explanation
Synovectomy of the knee prior to loss of articular cartilage has been shown to consistently relieve pain in patients with rheumatoid arthritis. Partial knee replacement will not arrest the process of joint destruction. Osteotomy of the hip has not been found to be a successful procedure in patients with rheumatoid arthritis. Hip arthrodesis should not be considered because of the multiarticular involvement in patients with rheumatoid arthritis. Core decompression of the hip has not been shown to save the femoral head because the necrosis appears to occur simultaneously with the inflammatory joint process. Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Question 44High Yield
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 45High Yield
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to

Explanation
The radiograph shows a fracture distal to the prosthesis in a stable, apparently well-fixed prosthetic stem. The well-fixed prosthesis-bone composite is stiff, creating a modulus mismatch between the proximal and distal femur. Therefore, the risk of fracture, particularly in osteoporotic bone, is increased at this level. Revision of the stem to a longer construct is unnecessary, and standard plate and screw fixation has been shown to yield union rates of greater than 90%. Nonsurgical treatment of fractures distal to the tip of the prosthesis results in high nonunion rates, reported to be from 25% to 42%. Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 46High Yield
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm3. The aspirate should also yield which of the following findings?
Explanation
Explanation
5b The radiographs reveal chondrocalcinosis of the menisci. This is caused by calcium pyrophosphate crystals, which are weakly positive birefringent rhomboid-shaped crystals. Frequently, this condition is asymptomatic; however, routine abdominal surgery may cause precipitation of these crystals and pain. Gout, which is caused by strongly negative birefringent needle-shaped sodium urate crystals, is not associated with chondrocalcinosis and is rare in younger women. Gross blood is uncommon without trauma. Infection is not likely in a healthy patient who underwent uncomplicated surgery. Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
References:
- Hough AJ Jr, Webber RJ: Pathology of the meniscus. Clin Orthop 1990;252:32-40.
Question 47High Yield
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Explanation
Explanation
Kayanja and associates, in a number of biomechanical studies, showed that in a kyphotic spine the strain is located at the apex of the deformity, the force is transmitted to the superior adjacent vertebrae, and that realignment and cement augmentation effectively normalize the load transfer. Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87. Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63. Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
Question 48High Yield
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the

Explanation
The sciatic nerve is formed by the roots of the lumbosacral plexus. It exits the pelvis through the greater sciatic notch and appears in the buttock anterior to the piriformus. From that point, the sciatic nerve passes posteriorly over the superior gemellus, obturator internus, inferior gemellus, and quadratus femoris before it passes deep to the biceps femoris. The tendon of the obturator internus passes through the lesser sciatic notch. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347. Anderson JE: Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Question 49High Yield
What is the treatment of choice for the injury shown in Figures 20a through 20c?
Explanation
Explanation
20b 20c The radiographs show multiple carpometacarpal dislocations. Reduction is often obtainable but difficult to maintain. Internal fixation is required to maintain the reduction, preferably with Kirschner wires. Closed reduction and percutaneous pinning is preferred by some surgeons. Others recommend open reduction to remove irreconstructable osteochondral fragments from the individual joints and to ensure correct reduction of the carpometacarpal joints. Kirschner wires are removed at 6 to 8 weeks. Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
References:
- Lawlis JF III, Gunther SF: Carpometacarpal dislocations: Long-term follow-up. J Bone Joint Surg Am 1991;73:52-59.
Question 50High Yield
The photomicrograph seen in Figure 41 shows which of the following conditions?
Explanation
Explanation
The photomicrograph shows a synovial cell sarcoma with a characteristic histology of a biphasic pattern of pleomorphic spindle cells and well-differentiated cuboidal to columnar cells forming gland-like spaces. The glandular zones contain mucous-like material that stains positively with periodic acid Schiff. Microscopic calcifications are usually found. Synovial cell sarcoma has a high rate of local recurrence as well as metastases. It is the most common malignancy found in the foot. Krall RA, Kostianovsky M, Patchefsky AS: Synovial sarcoma: A clinical, pathological and ultrastructural study of 26 cases supporting the recognition of a monophasic variant. Am J Surg Pathol 1981;5:137-151.
References:
- Wright PH, Sim FH, Soule EH, Taylor WF: Synovial sarcoma. J Bone Joint Surg Am 1982;64:112-122.
Question 51High Yield
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?

Explanation
The patient has a scaphoid fracture involving the proximal pole. Surgical treatment is recommended for such fractures because of the prolonged period of cast immobilization necessary and the increased risk of delayed union, nonunion, and/or osteonecrosis with nonsurgical management. A cannulated compression screw, inserted in the central scaphoid via a dorsal approach, is biomechanically advantageous and provides greater stability for fracture healing than Kirschner wires. Recently, good outcomes have been reported with arthroscopic-assisted percutaneous fixation of nondisplaced or minimally displaced scaphoid fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210. Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79. Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
Question 52High Yield
Which of the following is most predictive of a medial side ankle injury in the presence of a fibula fracture above the level of the joint?
Explanation
Explanation
Isolated Lauge-Hansen supination-external rotation-type ankle fractures comprise 20% to 40% of ankle fractures and nonsurgical management is effective for managing SER-2 ankle fractures. Tornetta and associates recently showed that medial ankle tenderness, ecchymosis, and swelling are not reliable findings when trying to determine deltoid competence. Stress radiographs showing a medial clear space of greater than 4 mm or one that is also 1 mm greater than the superior joint space, or any lateral talar subluxation are indicative of deltoid incompetence and indicative of a SER-4 ankle fracture. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004:86;2171-2178. Kristensen KD, Hansen T: Closed treatment of ankle fractures: Stage II supination-eversion fractures followed for 20 years. Acta Orthop Scand 1985;56:107-109.
Question 53High Yield
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
References:
- Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 54High Yield
A 12-year-old girl has scoliosis at T5-T10 that measures 62 degrees. A clinical photograph of the axilla is shown in Figure 56. Management should consist of

Explanation
Neurofibromatosis type 1 (NF-1) is an autosomal-dominant disorder affecting about 1 in 4,000 people. NF-1 causes tumors to grow along various types of nerves and affects the development of non-nervous tissues, such as bone and skin. The gene for NF-1 is located on the long arm of chromosome 17 and codes the protein neurofibromin. Research indicates that NF-1 acts as a tumor-suppressor gene and, as such, plays an important role in the control of cell growth and differentiation. Axillary and inguinal freckling is considered a good diagnostic marker for NF-1. The hyperpigmented spots that measure from 2 mm to 4 mm may be congenital, but these typically appear and increase later in life. Scoliosis is the most common musculoskeletal disorder of NF-1. The curves are frequently dystrophic, kyphotic, and have a high risk of pseudarthrosis following spinal fusion. Anterior and posterior spinal fusion with rigid posterior segmental instrumentation is the treatment of choice. Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Question 55High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?

Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 56High Yield
What is the relative amount of type II collagen synthesis in disease-free adult articular cartilage compared to developing teenagers?
Explanation
Explanation
Adult articular cartilage has less than 5% of the synthesis rate of type II collagen than that seen in developing teenagers. Both synthesis and degradation of type II collagen in normal adult articular cartilage is very low compared to children. In osteoarthrosis, both synthesis and degradation are increased, but the collagen does not properly incorporate into the matrix. Lippiello L, Hall D, Mankin HJ: Collagen synthesis in normal and osteoarthritic human cartilage. J Clin Invest 1977;59:593-600.
References:
- Nelson F, Dahlberg L, Laverty S, et al: Evidence for altered synthesis of type II collagen in patients with osteoarthritis. J Clin Invest 1998;102:2115-2125.
Question 57High Yield
A 17-year-old boy has had a mass in his right thigh for the past 6 months. He denies any history of trauma. Examination reveals that the mass is painless and firm. A radiograph and axial MRI scan are shown in Figures 49a and 49b. What is the most likely diagnosis?

Explanation
Osteochondroma typically occurs as a bony projection or a sessile growth on the bone, and there can be flaring of the metaphysis. The radiograph shows continuity from the adjacent cancellous bone into the lesion itself. There is no soft-tissue mass or bone destruction to suggest osteosarcoma or Ewing's sarcoma. Periosteal chondroma has a scalloped out radiographic appearance. Chondroblastoma typically is an epiphyseal-based lesion.
Question 58High Yield
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
Explanation
17b Melanoma comprises 25% of lower extremity lesions and is the most common malignant tumor of the foot. The preferred treatment is wide resection. Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
References:
- Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 59High Yield
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
Explanation
32b 32c 32d 32e Fibromatosis is a benign but aggressive fibrous lesion that principally arises from the connective tissue of muscle and the overlying fascia. The peak incidence is between the ages of 25 and 35 years. Most patients have a deep-seated, firm, poorly circumscribed mass that has grown insidiously and causes little or no pain. MRI is helpful in diagnosing the lesion and in assessing the extent of disease prior to surgical intervention. Histologically, the lesion is poorly circumscribed and infiltrates the surrounding tissue. The lesion appears bland with uniform spindle cells separated by abundant collagen, with little or no cell-to-cell contact. Despite its bland microscopic appearance, the tumor frequently behaves in an aggressive manner. These lesions do not metastasize but have a high incidence of recurrence. Treatment options consist of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
References:
- Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 60High Yield
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?

Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 61High Yield
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
Shufflebarger and others have reported that the placement of anterior interbody structural support at the lumbosacral junction increases the overall construct stiffness and reduces the strain on posterior instrumentation, thereby reducing the risk of screw pull-out or fracture. The stiffness of the posterior instrumentation actually increases, whereas the actual strength of the instrumentation remains the same. Actual strain measured at an adjacent intervertebral disk to a fusion construct is expected to increase. Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393. Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Question 62High Yield
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
Explanation
When retropulsion of the posterior vertebral wall is present, nothing prohibits the cement from following the path of least resistance into the canal or from pushing a bone fragment further into the canal; most clinicians consider it a contraindication to these techniques. Patient age itself is not a contraindication as long as there are no medical contraindications to surgery. An acute fracture in a patient who remains immobile and hospitalized because of pain may be a good indication for such a technique. Prior compression fracture and older compression fractures are not contraindications, but pain relief may be less predictable. Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567. Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
References:
- Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 63High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 64High Yield
A 69-year-old woman is seen in the emergency department with a bilateral C5-6 facet dislocation and complete quadriplegia after falling down a flight of stairs. After initial evaluation and treatment by the trauma service, she is moved to the intensive care unit. Examination reveals a blood pressure of 90/50 mm/Hg, a pulse rate of 50/min, a respiration rate of 12/min, and urine output of 1 mL/kg/h. Her hemodynamic status should be addressed by
Explanation
Explanation
The patient's heart rate is not responding to hypotension with tachycardia, as would be expected in the event of hypovolemic shock. Additionally, the adequate urine output suggests proper fluid resuscitation. Instead, she is bradycardic, possibly indicating neurogenic shock and loss of sympathetic tone to the heart. A Swan-Ganz catheter should be used to help differentiate these problems and guide appropriate fluid resuscitation and use of vasopressor agents. Hadley MN: Management of acute spinal cord injuries in an intensive care unit or other monitored setting. Neurosurgery 2002;50:S51-S57.
References:
- Vaccaro AR, An HS, Betz RR, et al: The management of acute spinal trauma: Prehospital and in-hospital emergency care. Instr Course Lect 1997;46:113-125.
Question 65High Yield
During primary total knee arthroplasty with trial implants in place, the surgeon notes technically satisfactory patellar resurfacing and restoration of a physiologic mechanical axis but excessively lateral patellar tracking. Treatment should now include
Explanation
Explanation
The most common causes of patellar instability after total knee arthroplasty are valgus malalignment, internal rotation of the femoral or tibial component, medialization of the femoral component, errors in patellar preparation and resurfacing, and failure to perform a lateral release. These factors should be addressed before considering capsular closure. Distal extensor mechanism realignment should be avoided because of the complication rate. The proximal extensor mechanism would not adequately compensate for implant malrotation. Barnes CL, Scott RD: Patellofemoral complications of total knee replacement, in Heckman JD (ed): Instructional Course Lectures 42. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 309-314.
References:
- Hungerford DS: Alignment in total knee replacement, in Jackson DW (ed): Instructional Course Lectures 44. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 455-468.
Question 66High Yield
What procedure can eliminate a sulcus sign?
Explanation
A sulcus sign represents inferior subluxation of the shoulder. The elimination of this sign and correction of the inferior subluxation is best achieved through either an open or arthroscopic rotator interval closure. A SLAP repair stabilizes the biceps anchor but does not affect the sulcus sign. A Bankart repair, which corrects anterior-inferior laxity, is not sufficient to eliminate a sulcus sign. Subacromial decompression and supraspinatus repairs have no effect on inferior subluxation. Field LD, Warren RF, O'Brien SJ, et al: Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 1995;23:557-563.
Question 67High Yield
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 68High Yield
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 69High Yield
Which of the following antibiotics is contraindicated in children?
Explanation
The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.
Question 70High Yield
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
Explanation
Explanation
As long as the patient is alert and cooperative, an attempt can be made to reduce the dislocation. This should not be attempted in a patient who is obtunded, comatose, or uncooperative. If any neurologic changes are noted during the reduction maneuver, the attempt should be stopped, appropriate radiographic studies obtained, and open reduction and stabilization planned in the operating room.
References:
- Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
Question 71High Yield
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 72High Yield
What is the most common MRI appearance of a malignant soft-tissue sarcoma?
Explanation
Explanation
The classic MRI appearance of a soft-tissue sarcoma is a well-defined heterogeneous mass deep to the fascia. MRI has greatly enhanced our ability to identify and characterize soft-tissue masses. In many patients, MRI is diagnostic and may obviate the need for biopsy. In other patients, it may indicate with high probability that the mass is malignant and consideration for referral can be made. A common misconception is that sarcomas are infiltrative; therefore, physicians mistakenly exclude the diagnosis of a sarcoma based on a well-defined mass seen on MRI. However, sarcomas grow centrifugally with balloon-like expansion compressing surrounding normal tissue; as such, they appear well defined. Many benign soft-tissue masses such as lipomas are similarly well defined. However, MRI is especially useful in identifying fat. Lipomas appear to be homogeneous masses with fat signal characteristics on all sequences. Ill-defined soft-tissue masses include infection, trauma, and desmoid tumors. Heterogeneity is not unique to malignant tumors but is a characteristic of soft-tissue sarcomas. Bancroft LW, Peterson JJ, Kransdorf MJ, Nomikos GC, Murphey MD: Soft tissue tumors of the lower extremities. Radiol Clin North Am 2002;40:991-1011. Berquist TH, Ehman RL, King BF, et al: Value of MR imaging in differentiating benign from malignant soft-tissue masses: Study of 95 lesions. Am J Roentgenol 1990;155:1251-1255.
References:
- Crim JR, Seegar LL, Yao L, et al: Diagnosis of soft tissue masses with MR imaging: Can benign masses be differentiated from malignant ones? Radiology 1992;185:581-586.
Question 73High Yield
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
Explanation
24b 24c 24d 24e The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
References:
- Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 74High Yield
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb "feels" different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?

Explanation
The patient initially has a distal third femoral fracture and a pulseless limb. The first step is to reduce the fracture and reassess the vascular status. Although the pulse returns, it feels different than the quality of the pulse in the contralateral uninjured extremity. There is a risk of a vascular injury with this fracture pattern due to tethering of the femoral vessels at the adductor hiatus; therefore, the vascular status needs further assessment since the pulses are not symmetrical. A physical examination is not very accurate in assessing whether a vascular injury is present; therefore, serial examinations are not appropriate. Angiography is very sensitive and specific but is time consuming and can cause complications secondary to the dye and the arterial puncture required to perform it. Duplex ultrasound is effective but is very operator-dependent and may not be available 24 hours a day. The ABI is easily performed and has been shown to be sensitive and specific. If the value is greater than 0.9, the negative predictive value is 99% and when the value is less than 0.9, it is 95% sensitive and 97% specific for a major arterial injury. It has been shown to be useful for blunt lower extremity injuries as well as knee dislocations. Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695. Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Question 75High Yield
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
Explanation
According to a recent study, cemented pegged glenoid components had fewer radiolucent lines initially and at 2-year follow-up when compared to a cemented keeled design. Curve-backed designs have also shown fewer radiolucent lines when compared to flat-backed designs. Oversizing the glenoid can lead to impaired rotator cuff function and decreased range of motion. An off-centered glenoid can lead to early loosening. Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257. Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
References:
- Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.
Question 76High Yield
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?

Explanation
The radiograph shows three zones: an outer regenerated cortical layer, an interface zone consisting of viable trabecular bone and occasional particles of bone cement, and an inner layer of necrotic bone embedded in cement. No fibrous membrane is noted, and there is no direct contact of cement with native bone. Based on these findings, it is believed that the middle layer is the result of incorporation of the allograft with further remodeling. Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Question 77High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 78High Yield
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include
Explanation
Explanation
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures. Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780. Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362. Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
References:
- Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
Question 79High Yield
The spring ligament of the foot connects what two bones?
Explanation
Explanation
The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot. Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Question 80High Yield
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of
Explanation
Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
References:
- Baker CL, Morales RW: Arthroscopic treatment of tranchondral talar dome fractures: A long-term follow-up study. Arthroscopy 1999;15:197-202.
Question 81High Yield
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
Explanation
The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
References:
- Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 82High Yield
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?

Explanation
Assessment of the acutely injured patient follows the Advanced Trauma Life Support protocol. Cervical cord injury is often associated with a disruption in sympathetic outflow. Absent sympathetic input to the lower extremities leads to vasodilatation, decreased venous return to the heart, and subsequent hypotension. With hypotension, the physiologic response of tachycardia is not possible because of the unopposed vagal tone. This results in bradycardia. Patient positioning, fluid support, pressor agents, and atropine are used to treat neurogenic shock.
Question 83High Yield
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of

Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 84High Yield
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
A high level of suspicion must be given for a fracture in any patient with ankylosing spondylitis who reports neck pain, even with minimal or no trauma. The neck should be immobilized in its normal position, which is often kyphotic, and plain radiographs should be obtained. If no obvious fracture is seen, CT with reconstruction should be obtained. The placement of in-line traction can have catastrophic effects because it may malalign the spine. Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 724-727.
Question 85High Yield
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?

Explanation
PVNS is a rare inflammatory granulomatous condition of unknown etiology, and causes proliferation of the synovium of joints, tendon sheaths, or bursa. The disorder occurs most commonly in the third and fourth decades but can occur at any age. MRI provides excellent delineation of the synovial disease. Characteristic features of PVNS on MRI include the presence of intra-articular nodular masses of low signal intensity on T1- and T2-weighted images and proton density-weighted images. Synovial biopsy should be performed if there is any doubt of the diagnosis. Total synovectomy (open or arthroscopic) is required for the diffuse form, although recurrence is common. Rheumatoid arthritis and synovial chondromatosis are not typically associated with hemorrhagic effusions. De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607. Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Question 86High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 87High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 88High Yield
Osteoclasts originate from which of the following cell types?
Explanation
Osteoclasts originate from the monocyte/macrophage lineage. Fibroblasts and osteoprogenitor cells originate from mesenchymal stem cells and do not form osteoclasts. Plasma cells reside in the bone marrow and are derivatives of the hematopoietic system. Megakaryocytes are also in the bone marrow and synthesize platelets. Zaidi M, Blair HC, Moonga BS, et al: Osteoclastogenesis, bone resorption, and osteoclast-based therapeutics. J Bone Miner Res 2003;18:599-609. Brinker MR: Bone (Section 1), in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 1-35.
Question 89High Yield
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
There is a spectrum of heat-related conditions. Heat cramps are the mildest form of heat illness. In heat exhaustion, cramps are associated with headache and weakness, and the skin is pale and moist. Treatment of heat cramps or heat exhaustion consists of removing and loosening excess clothing, applying ice to the axilla and groin, ingestion of cool water, and cool water sprays. This patient demonstrates symptoms of heat stroke which is a medical emergency. The core body temperature may be as high as 106 to 110 degrees F (41.1 to 43.3 degrees C). In heat stroke, the patient may no longer be sweating, and the skin may be hot and red. The athlete is usually confused, weak, nauseated, and may have seizure activity. Central nervous system depression has been called the most important marker of heat stroke, and progresses from confusion and bizarre behavior to collapse, delirium, and coma. Bizarre behavior is often the first sign of heat stroke. The patient needs to be treated and moved to a medical facility rapidly. During transfer, IV fluids and cooling of the athlete should be initiated. The best treatment of heat-related illness appears to be prevention with adequate hydration and monitoring of conditions (temperature and humidity), with cancellation of competition when conditions do not comply with guidelines. Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902. Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Question 90High Yield
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
Explanation
Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures. Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Question 91High Yield
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
Explanation
While the patellar tendon ligament is considered by many to be the tissue of choice for ACL reconstruction, more recent studies have shown that the quadruple semitendinosus and gracilis tendon graft has the greatest stiffness and offers the highest maximum load to failure. Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557. Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823. Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
References:
- Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 92High Yield
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?

Explanation
Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a 5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority. Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Question 93High Yield
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
Explanation
Tornetta and associates and Yang and associates found that nearly half of all femoral neck fractures associated with femoral shaft fractures were being missed at their institution. On the basis of the delayed diagnosis of these injuries, a best-practice protocol was developed by the attending trauma surgeons for the evaluation of the femoral neck in patients with a femoral shaft fracture. This protocol includes a preoperative AP internal rotation radiograph of the hip, a fine-cut (2-mm) CT scan through the femoral neck (as a part of the initial trauma scan), and an intraoperative fluoroscopic lateral evaluation of the hip just prior to fixation of the femoral shaft. In addition, postoperative AP and lateral radiographs of the hip are made in the operating room to specifically evaluate the femoral neck before the patient is awakened. They found that fine-cut CT (2 mm was the best screening tool in this group of patients) identified 12 of the 13 fractures, whereas 8 of the 13 fractures were visible on the dedicated preoperative AP internal rotation hip radiographs. Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Question 94High Yield
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
Explanation
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site. Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
References:
- Lynch G, Meyers JF, Whipple TL, et al: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 95High Yield
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
Explanation
For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
References:
- Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 96High Yield
One advantage of using onlay strut allograft in femoral revision surgery is that it can

Explanation
Onlay grafts can provide more structural support than morcellized grafts. They are more easily incorporated into the host femur than bulk segmental total femur allografts; however, the incorporation is never complete. The use of onlay grafts is principally directed at addressing segmental defects of the femur; their use can be applied with either cementless or cement fixation of the femoral stem. Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44. Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Question 97High Yield
A 45-year-old woman has had right wrist pain for the past 2 months. A radiograph, bone scan, and MRI scan are shown in Figures 66a through 66c, and a photomicrograph is shown in Figure 66d. What is the most likely diagnosis?
Explanation
Explanation
66b 66c 66d The radiograph shows a purely radiolucent lesion without matrix mineralization in the epiphysis of the distal radius. The lesion is "hot" on bone scan, and the MRI scan reveals cortical destruction with a soft-tissue mass. These findings are most consistent with giant cell tumor. The distal radius is a common location for giant cell tumors. The other options would be very uncommon in this location in a 45-year-old patient. The photomicrograph demonstrates multinucleated giant cells in a sea of mononuclear cells. The nuclei of the giant cells and the nuclei of the mononuclear stromal cells are identical. This feature helps distinguish giant cell tumor from other lesions that might contain giant cells. Cheng CY, Shih HN, Hsu KY, et al: Treatment of giant cell tumor of the distal radius. Clin Orthop Relat Res 2001;383:221-228.
References:
- Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 263-284.
Question 98High Yield
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)?

Explanation
The rotator cuff interval is located between the supraspinatus and subscapularis and the biceps tendon is deep to the interval. It is a triangular area where the base is the coracoid process and the apex is the transverse humeral ligament at the biceps sulcus. Closure or tightening of this area is often helpful in patients with shoulder instability. Conversely, this area is often contracted in patients with adhesive capsulitis and may need to be released. Selecky MT, Tibone JE, Yang BY, et al: Glenohumeral joint translation after arthroscopic thermal capsuloplasty of the rotator interval. J Shoulder Elbow Surg 2003;12:139-143.
Question 99High Yield
Which of the following tumors have characteristic chromosomal translocations?
Explanation
Explanation
Ewing's sarcoma has an 11;22 translocation that creates the EWS/FLI1 fusion gene, and synovial sarcoma has an X;18 translocation that creates the STT/SSX fusion gene. The other tumors do not have consistent translocations. Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 100High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?

Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
