Orthopedic Board Review MCQs: Mock Exam Set #849 – 100 High-Yield Questions

Key Takeaway
This page offers 100 randomized, high-yield Orthopedic Surgery Multiple Choice Questions (MCQs) for ABOS, OITE, and FRCS board exam preparation. Surgeons can test their knowledge, reinforce critical concepts, and prepare effectively for certification and in-training assessments across various orthopedic subspecialties.
Is MCP Joint Synovectomy Right for Your Infla...
00:00
Start Quiz
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
- Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Question 3High Yield
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20 degrees of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked "A," the resulting ligament reconstruction will excessively

Explanation
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90 degrees. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20 degrees to 0 degrees of flexion. If the graft is tensioned in significant flexion (greater than 60 degrees), it will be excessively loose as the knee fully extends. Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Question 4High Yield
The inheritance of the deformity shown in Figure 1 is most commonly
Explanation
Explanation
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
References:
- Kay SPJ: Cleft hand, in Green DP (ed): Green's Operative Hand Surgery. Philadelphia, Pa, Churchill Livingston, 1999, pp 402-414.
Question 5High Yield
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon. Haher TR, Felmly WT, O'Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Question 6High Yield
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
Explanation
9b Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 7High Yield
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
Explanation
Polyethylene wear debris can result in significant synovitis and subsequent cloudy appearing synovial fluid. Typically, laboratory studies show a WBC of less than 30,000/mm3 no left shift. Cytologic examination can reveal intra-articular polyethylene particles. Infected total knee arthroplasty is extremely uncommon in a healthy, immune-competent patient who has a normal preoperative erythrocyte sedimentation rate and C-reactive protein level.
References:
- Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 8High Yield
What is the most common short-term complication following femoral impaction grafting for revision total hip arthroplasty?
Explanation
Explanation
Impaction grafting is an alternative for severe femoral bone deficiency; however, stem subsidence is commonly observed during the first few months. Slight subsidence is felt to be integral to the success of the procedure. Predictable bone graft incorporation and stable stem fixation have been reported in the medium-term. The incidence of periprosthetic fractures has been reported as high as 24%. Mikhail MWE, Weidenhielm L, Jazrawi LM, et al: Collarless, polished, tapered stem failure. J Bone Joint Surg Am 2000;82:1513-1514.
References:
- Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Instr Course Lect 2000;49:111-118.
Question 9High Yield
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 10High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 11High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 12High Yield
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
The correct progression of the annular and cruciform pulley in the digits is A1, A2, C1, A3, C2, A4, C3. The two cruciform pulleys are collapsible elements adjacent to the more rigid annular pulleys of the flexor tendon sheath. This arrangement enables unrestricted flexion of the proximal interphalangeal joint. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Question 13High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
References:
- Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 14High Yield
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
After an osteoporotic vertebral compression fracture, the risk of subsequent fractures at adjacent levels increases. This is felt to be the result of a shifting of the sagittal alignment more anteriorly, putting more stress on the osteopenic vertebral bodies and their anterior cortices. Pain generally resolves with rest, but this may take weeks or months. It has been demonstrated experimentally that osteoporotic vertebral bodies are actually less stiff and weaker after a compression fracture; therefore, deformity predisposes to further deformity. The extensor musculature often fatigues over time and usually does not hypertrophy. Frontal plane deformity is a rare development. Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Question 15High Yield
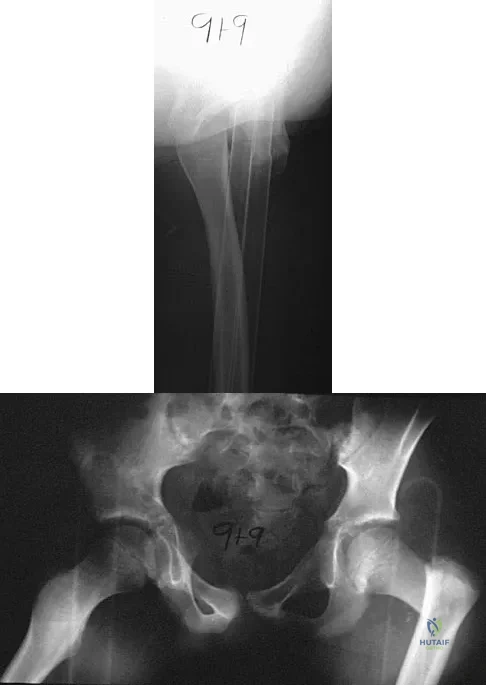
Figure 18a shows the clinical photograph of a 2-year old boy who has a deformity of the right leg. Examination reveals eight cutaneous markings similar to those shown in Figure 18b. Radiographs are shown in Figure 18c. Management should consist of

Explanation
The diagnosis of neurofibromatosis may be based on the presence of at least six cafe-au-lait spots larger than 5 mm in diameter and the osseous lesion shown in Figure 18c. Neurofibromatosis occurs in 50% of patients who have an anterolateral bowing deformity of the tibia, and this bowing may be the first clinical manifestation of this disorder. The patient has anterolateral bowing of the tibia and fibula that warrants concern for a possible fracture and pseudarthrosis; therefore, the limb should be protected in a total contact orthosis to prevent fracture. In contradistinction to posteromedial bowing of the tibia and fibula, spontaneous remodeling of an anterolateral bowing deformity is not expected. Intramedullary nailing or the use of a vascularized fibula is reserved for the treatment of a congenital pseudarthrosis of the tibia. Crawford AH Jr, Bagamery N: Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72-88.
Question 16High Yield
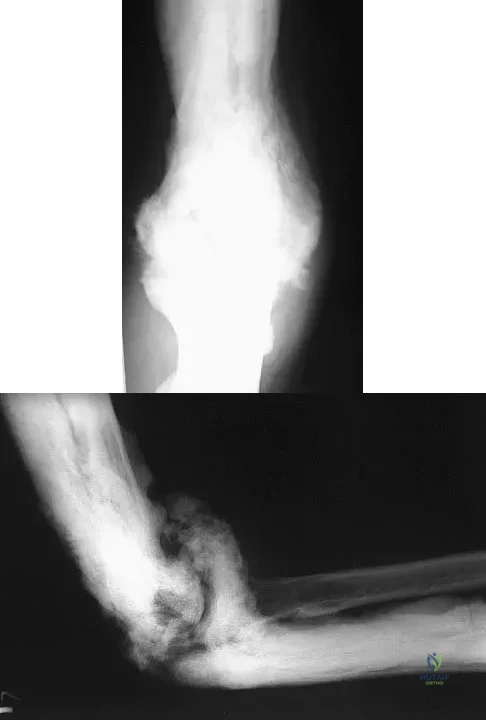
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?
Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 17High Yield
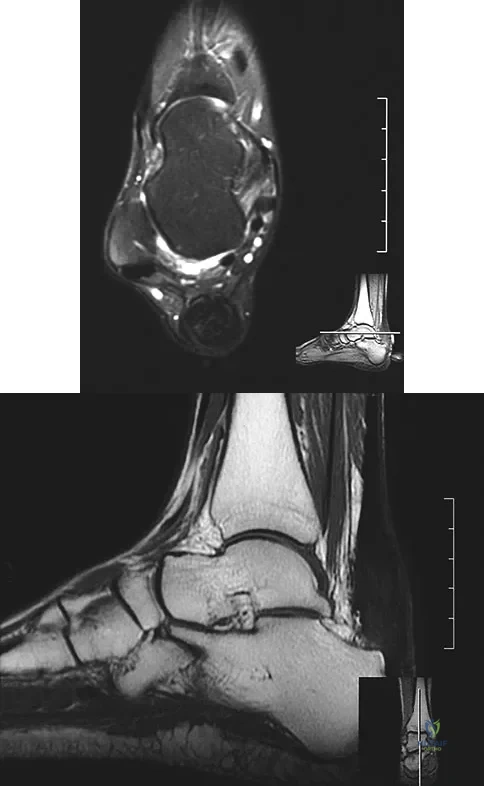
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
Explanation
Explanation
60b 60c 60d The patient has a large deep anterior thigh mass that has imaging characteristics of mature fat. Intramuscular lipomas are effectively treated with marginal resections with very low recurrence rates. Large lipomas often have small amounts of intralesional signal changes frequently representing trapped muscle fibers and do not necessitate more extensive margins. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
References:
- Rozental TD, Khoury LD, Donthineni-Rao R, et al: Atypical lipomatous masses of the extremities: Outcome of surgical treatment. Clin Orthop Relat Res 2002;398:203-211.
Question 18High Yield
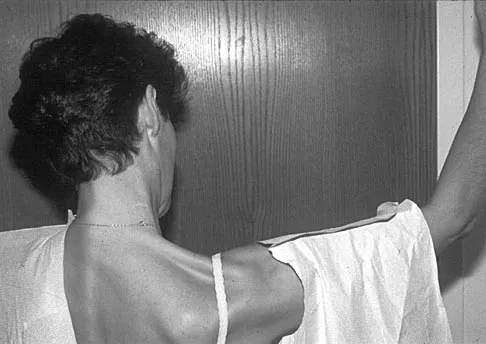
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 19High Yield
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
Explanation
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
References:
- Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 20High Yield
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of
Explanation
Explanation
14b The patient has osteonecrosis of the lateral femoral condyle with collapse of the articular surface. Because there is already collapse of the articular surface, a total knee arthroplasty is the treatment of choice. The results of total knee arthroplasty in these patients are usually excellent. However, knee replacement is only a resurfacing procedure, and some patients with global osteonecrosis of the distal femur may have residual pain after knee replacement. High tibial osteotomy may be indicated in younger patients who have a varus deformity and localized osteonecrosis. Arthroscopic surgery would provide minimal relief for this patient because there is already collapse of the articular surface. A hinged knee brace will not adequately unload the joint. An osteochondral allograft should be considered only for younger patients with localized osteonecrosis. Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
References:
- Lotke PA, Abend JA, Ecker ML: The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop 1982;171:109-116.
Question 21High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 22High Yield
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
References:
- Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 23High Yield
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
Explanation
Although thoracic disk herniations have been reported at all levels of the thoracic spine, more than two thirds are found at T9-T12, which is the more mobile lower third of the thoracic region. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
References:
- Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:70-77.
Question 24High Yield
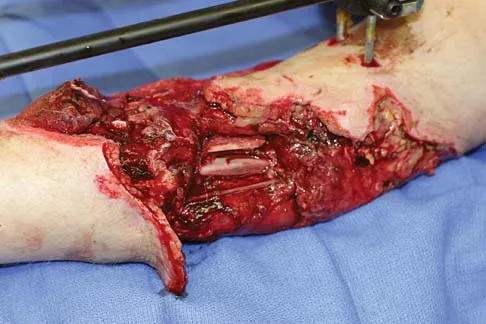
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?

Explanation
The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated. Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
Question 25High Yield
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 26High Yield
Treatment of a cruciate-retaining total knee that is unstable in flexion is best accomplished by
Explanation
Explanation
Pagnano and associates revised 25 painful primary posterior cruciate-retaining total knee arthroplasties for flexion instability. The patients shared typical clinical presentations that included a sense of instability without frank giving way, recurrent knee joint effusion, soft-tissue tenderness involving the pes anserine tendons and the retinacular tissue, posterior instability of 2+ or 3+ with a posterior drawer or a posterior sag sign at 90 degrees of flexion, and above-average motion of the total knee arthroplasty. Twenty-two of the knee replacements were revised to posterior stabilized implants, and three underwent tibial polyethylene liner exchange only. Nineteen of the 22 knee replacements revised to a posterior stabilized implant showed marked improvement after the revision surgery. Only one of the three knee replacements that underwent tibial polyethylene exchange was improved. Flexion instability can be a cause of persistent pain and functional impairment after posterior cruciate-retaining total knee arthroplasty. Revision surgery that focuses on balancing the flexion and extension spaces, in conjunction with a posterior stabilized knee implant, seems to be a reliable treatment for symptomatic flexion instability after posterior cruciate-retaining total knee arthroplasty.
References:
- Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate-retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Question 27High Yield
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
Explanation
The gradient-echo MRI scan highlights the ulnar and radial arteries, as indicated by the arrow. This technique suppresses the signal of the surrounding fat and causes the stationary surrounding tissues to become intermediate in signal intensity. The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient's symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue. Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
References:
- Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
Question 28High Yield
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?

Explanation
The knee is the most common location of spontaneous bleeding in children with hemophilia. Treatment generally requires replacement to 40% to 50% of normal. For surgery, the replacement should be to 100%. The plasma level generally rises 2% for every unit (per kg body weight) of factor VIII administered. Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
Question 29High Yield
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation. Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
References:
- Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 30High Yield
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?

Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 31High Yield
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?
Explanation
Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
References:
- Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 32High Yield
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?
Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 33High Yield
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of

Explanation
The coracoid process is an essential component of the superior shoulder suspensory complex and must be maintained. Open reduction and internal fixation is recommended if the fragment is large and displaced more than 1 cm. Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Question 34High Yield
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Question 35High Yield
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures?
Explanation
Explanation
Synovial folds or plicae are the result of incomplete or partial resorption of the synovial membranes during fetal development of the knee. The arthroscopic view shows a medial patellar plica, which has been noted in 5% to 55% of all individuals but becomes symptomatic in only a small number of patients. Symptoms may include crepitus, pain, snapping, and swelling and often respond to nonsurgical management. Clarke HD, Scott WN, Insall JN: Anatomic aberrations, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 67-85.
References:
- Patel D: Plica as a cause of anterior knee pain. Orthop Clin North Am 1986;17:273-277.
Question 36High Yield
Following a chevron bunionectomy performed through a dorsal approach, a patient has persistent numbness on the dorsal and medial aspect of the hallux. What nerve has most likely been injured?
Explanation
Explanation
The dorsomedial cutaneous nerve of the hallux, which is a distal branch of the superficial peroneal nerve, supplies sensation to the skin on the dorsal and medial half of the hallux and may be injured during a chevron bunionectomy. Injury to the nerve leads to particularly painful neuromas that directly impinge on the shoe. For this reason, direct medial approaches are typically preferred for access to the medial aspect of the metatarsophalangeal joint.
References:
- Miller SD: Dorsomedial cutaneous nerve syndrome: Treatment with nerve transection and burial into bone. Foot Ankle Int 2001;22:198-202.
Question 37High Yield
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?

Explanation
The Weber and Lauge-Hansen fracture classifications suggest that the interosseous membrane (IOM) is torn with certain fracture patterns. In a recent study that evaluated ankle fractures with MRI, Nielson and associates identified 30 patients with IOM tears. Ten of the tears did not correspond with the level of the fibular fracture. The authors concluded that stability of the syndesmosis should not be based on the level of the fibular fracture alone but should also include an intraoperative stress test. Transsyndesmotic fixation should be considered for those fractures where the intraoperative stress test demonstrates instability. A widened medial clear space may occur with a deltoid injury and distal fibular fracture in the absence of a significant tear of the interosseous membrane.
Question 38High Yield
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
Extensor pollicis longus tendon rupture can occur after a fracture of the distal radius, even a minimally displaced one. Poor vascularity of the tendon within the third dorsal compartment is the suspected etiology, not the displaced fracture fragments. Tendon transfer will suitably restore active extension of the thumb interphalangeal joint. Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Question 39High Yield
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
The complications of femoral neck fractures in children include osteonecrosis, malunion, nonunion, and premature physeal closure. It is presumed that the risk of osteonecrosis is directly related to the amount of displacement at the time of injury and is not affected by the type of treatment. The risk of the other complications can be decreased depending on the type of treatment. Anatomic reduction by either closed or open methods can reduce the risk of malunion. The addition of internal fixation allows for maintenance of the reduction. In young children who cannot comply with a partial or non-weight-bearing status, the addition of a spica cast gives added protection. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 40High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 41High Yield
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Explanation
Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root. Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
References:
- Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 42High Yield
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Explanation
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure. Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607. Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 43High Yield
Plots of stress versus strain for four orthopaedic biomaterials are shown in Figure 3. Referring to the figure, what is the correct identification of the curves?

Explanation
Stress-strain plots allow easy comparison of a number of important mechanical properties, including elastic modulus (the slope of the initial straight line portion of the curve) and yield stress (the stress at the break in the curves for bone, steel, and titanium alloy). Important considerations here are much lower modulus and ultimate stress of bone and cement compared to the two metallic alloys, the fact that titanium is lower modulus but higher strength than stainless steel, and the identification of cement as the only brittle material among the four. Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 97-129.
Question 44High Yield
A 14-year-old football player has had thigh pain and weakness following a full-contact scrimmage 24 hours ago. He recalls that he felt a sharp pain in his back after colliding with a much heavier player. Examination reveals that the spine is minimally tender to palpation in the upper lumbar region. Motor testing reveals quadriceps weakness bilaterally, and a reverse straight leg raising test is positive. Plain radiographs of the thoracolumbar spine are normal. A myelogram, a CT scan with contrast, and an MRI scan are shown in Figures 41a through 41c. What is the most likely diagnosis?
Explanation
Explanation
41b 41c Fracture of the vertebral end plate is a relatively uncommon injury that is most often seen in adolescent boys. The injury is characterized by traumatic displacement of the vertebral ring-apophysis into the spinal canal and associated disk herniation. Over one third of these injuries are seen in children with lumbar Scheuermann disease. The injury most frequently involves the midlumbar vertebra, and symptoms are often indistinguishable from those associated with a herniated disk. The injury is usually not visible on plain radiographs. The diagnosis is typically made after obtaining MRI or contrast CT scans. Treatment consists of laminotomy and excision of the osteochondral fragments. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
References:
- Epstein NE, Epstein JA, Mauri T: Treatment of fractures of the vertebral limbus and spinal stenosis in five adolescents and five adults. Neurosurgery 1989;24:595-604.
Question 45High Yield
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 46High Yield
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?
Explanation
The risk of Salmonella osteomyelitis is much greater in patients with sickle cell disease than the general population. The exact reason for this increased risk is still unclear, but it appears to be associated with an increased incidence of gastrointestinal microinfarcts and abscesses. Both Staphylococcus aureus and Salmonella have been mentioned as the most prevalent causative organisms. Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227. Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413. Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Question 47High Yield
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?
Explanation
Explanation
5b The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle. Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 1973-2016.
References:
- Marsh JL, Saltzman CL: Ankle fractures, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green's Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2147-2247.
Question 48High Yield
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
Explanation
Explanation
9b Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
References:
- Vroomen PC, Van Hapert SJ, Van Acker RE, et al: The clinical significance of gadolinium enhancement of lumbar disc herniations and nerve roots on preoperative MRI. Neuroradiology 1998;40:800-806.
Question 49High Yield
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
Explanation
Bilateral flattening of the femoral heads suggests multiple epiphyseal dysplasia; therefore, a skeletal survey is indicated to look for involvement of other epiphyses. Unilateral flattening of the femoral head would suggest Legg-Perthes disease. Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
References:
- Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 50High Yield
Which of the following statements describing chordomas is false?
Explanation
Explanation
Casali and associates provided a recent review of the treatment options for chordomas. These tumors are not radiosensitive; however, modern intensity modulated radiosurgery techniques may be of value. The combination of surgery and radiotherapy compared to surgery alone results in the same disease-free survival time. Complete surgical resection of the chondroma with clean margins offers the best survival; however, its location may make total removal impossible. Thus subtotal resection followed by radiotherapy results in better survival despite the tumor's lack of radiosensitivity.
Question 51High Yield
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
Explanation
A player who has an acute cervical disk herniation should not be allowed to return to play until the acute phase is over. Certain players with large herniations may require surgery before returning to play to eliminate the risk of disk-related stenosis and cord compression. Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
References:
- Vaccaro AR, Watkins B, Albert TJ, Pfaff WL, Klein GR, Silber JS: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-705.
Question 52High Yield
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 53High Yield
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be

Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 54High Yield
The preferred surgical approach to the elbow of a child with an irreducible type III supracondylar distal humerus fracture and pulseless extremity is through which of the following muscle intervals?
Explanation
In a type III supracondylar distal humerus fracture of the elbow, the brachial artery can become incarcerated, yielding a pulseless extremity. In this situation, closed reduction may not be effective; therefore, open management is often necessary. The preferred surgical approach to the brachial artery and to this fracture is the anterior approach to the cubital fossa. The lacertus fibrosis is incised, and the dissection is carried out between the brachialis (musculocutaneous nerve) and the pronator teres (median nerve), mobilizing the brachial artery. Once the brachial artery is mobilized, the anterior elbow joint capsule may be exposed. The interval between the brachialis and the biceps describes the anterolateral approach to the elbow more commonly used for exposure of the proximal aspect of the posterior interosseous nerve. The dissection interval between the brachioradialis and the pronator teres describes the proximal extent of the anterior approach to the radius. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 115.
Question 55High Yield
The lesion seen in Figure 4 is most likely the result of metastases from what solid organ?
Explanation
Explanation
The primary carcinoma most likely to metastasize distal to the elbow and knees is lung carcinoma. Renal cell carcinoma can also metastasize to distal sites. Most metastatic bone disease occurs in the vertebral bodies, pelvis, and proximal long bones. Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
References:
- Leeson MC, Makley JT, Carter JR: Metastatic skeletal disease distal to the elbow and knee. Clin Orthop 1986;206:94-99.
Question 56High Yield
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
Explanation
The latissimus dorsi inserts on the humerus metaphysis between the pectoralis major (posterior) and teres major (anterior). Teres minor inserts on the base of the greater tuberosity. Pectoralis minor does not insert on the humerus. Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 57High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
References:
- Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 58High Yield
A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
Explanation
Explanation
The L5 nerve root lies directly over the superior and anterior alae. If the screw is directed approximately 20 degrees laterally and bicortical purchase is achieved, there is the risk of injuring the L5 nerve root. If the screw is directed medially into the body of S1, there is little risk of injury. The same root is at risk during placement of an iliosacral screw. Ebraheim NA, et al: Lumbosacral nerve and dorsal screw placement. Orthopedics 2000;23:245-247. Ebraheim NA, Mermer M, Xu R, Yeasting RA: Radiological evaluation of S1 dorsal screw placement. J Spinal Disord 1996;9:527-535.
References:
- Routt ML Jr, Nork SE, Mills WJ: Percutaneous fixation of pelvic ring disruptions. Clin Orthop 2000;375:15-29.
Question 59High Yield
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?
Explanation
Explanation
47b 47c 47d The figures show a lesion of the proximal humerus consistent with an enchondroma. The lesion is calcified on the radiographs. There is no cortical destruction, significant endosteal scalloping, or soft-tissue mass. The bone scan shows mild uptake in the area of the proximal humerus, and the T2-weighted MRI scan shows a lesion with high uptake, suggesting a lesion with high water content. A CT scan could also be obtained to rule out bone destruction or periosteal reaction. Pain with overhead activities is likely related to the rotator cuff. A biopsy is unlikely to add information because of inherent difficulties interpreting low-grade cartilaginous lesions. Curettage and grafting and en bloc resection are excessive treatments for a benign lesion that is apparently asymptomatic. Observation with a follow-up radiograph in 3 to 6 months is appropriate. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
References:
- Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 60High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 61High Yield
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Although there is no significant alteration in motion with a corset, studies have shown a decrease in intradiskal pressure. Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Question 62High Yield
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 63High Yield
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
Explanation
The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Question 64High Yield
What type of multiple lesions is associated with Maffucci's syndrome?
Explanation
Explanation
Maffucci's syndrome is a form of enchondromatosis associated with subcutaneous and deep hemangiomas. Similar to Ollier's disease, the risk of malignant transformation of the enchondromas is much higher than that of a solitary enchondroma. Multifocal nonossifying fibromas associated with other clinical findings such as mental retardation and café-au-lait spots is known as Jaffe-Campanacci syndrome. There are two types of multifocal forms of histiocytosis: Letterer-Siwe and Hand-Schüller-Christian disease. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274. Frassica F: Orthopaedic pathology, in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 292-335.
References:
- Yuan J, Fuchs B, Scully SP: Molecular basis of cancer, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 65High Yield
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of

Explanation
The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
Question 66High Yield
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T2-weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
Explanation
10b 10c 10d The radiographs show a lytic lesion in the right proximal tibia that has a high fluid content based on the MRI findings. The radiographic appearance is consistent with either telangiectatic osteosarcoma or aneurysmal bone cyst. Low-magnification histology shows a lesion resembling an aneurysmal bone cyst, with blood lakes separated by cellular septa. However, high-magnification shows severe cytologic atypia, indicative of a telangiectatic osterosarcoma. The appropriate treatment is neoadjuvant chemotherapy followed by wide resection and reconstruction of the lesion. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
References:
- Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 67High Yield
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?
Explanation
Explanation
Full exposure of the volar plate of the proximal interphalangeal joint of the finger is best accomplished by incision of the distal C1, A3, and proximal C2 pulleys; followed by gentle retraction of the flexor digitorum superficialis and profundus tendons. Sacrifice of the A3 pulley, although associated with some biomechanic disadvantage, can be tolerated without causing functionally limiting bowstringing of the flexor tendon. Sacrifice of even a portion of the A2 or A4 pulleys can decrease the biomechanic leverage provided by the flexor tendon sheath, leading to bowstringing of the flexor tendons. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186. Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 1853-1855.
References:
- Lin GT, Amadio PC, An KN, et al: Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 1989;14:949-956.
Question 68High Yield
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Explanation
Explanation
The patient has a pars interarticularis defect of L5 without apparent listhesis. The other diagnoses are not present. Papanicolaou N, Wilkinson RH, Emmans JB, Treves S, Micheli LJ: Bone scintigraphy and radiography in young athletes with low back pain. Am J Roentgenol 1985;145:1039-1044.
References:
- Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 291-302.
Question 69High Yield
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
Explanation
38b The CT scans show large cystic lesions in the talus and calcaneus with complete subluxation of the subtalar joint, allowing the calcaneus to slide laterally until it becomes blocked by the fibula. The cause of this subluxation is severe posterior tibial tendon dysfunction. Although no fibular fracture has yet appeared, it can occur with continued stress from the calcaneus. There is, however, a pathologic fracture in the medial calcaneus through a medial degenerative cyst. The joint space is irregular and not symmetrical as would be seen in an inflammatory arthropathy. Cystic lesions are not present in the tibia. No stress fracture is seen in the talus. Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
References:
- Anderson RB, Davis WH: Management of the adult flatfoot deformity, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1017-1039.
Question 70High Yield
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as

Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 71High Yield
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
Explanation
12b 12c 12d The radiographs show tarsometatarsal joint subluxation without fragmentation. The clinical history and delay in presentation with the radiographic findings suggest a neuropathic or Charcot arthropathy involving the midfoot area. Intact sensory examination to light touch is not diagnostic for an intact peripheral neurologic system; monofilament testing is a more accurate office baseline examination for the presence of sensory peripheral neuropathy. With an acute traumatic Lisfranc fracture-dislocation, a history of a traumatic event is necessary, and radiographic abnormalities are expected, although nonstanding radiographs still may be misleading. Acquired pes planus due to posterior tibial tendon rupture may have negative nonstanding radiographs. Standing radiographs may reveal pes planus. However, intermetatarsal disruption is not expected as seen in a Lisfranc abnormality. Localized osteomyelitis of the foot without a penetrating injury or cutaneous ulceration is extremely unlikely and does not fit with the clinical picture described. An isolated metatarsal stress fracture would show osseous irregularity without the instability pattern pictured. Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
References:
- Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
Question 72High Yield
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of
Explanation
Explanation
1b The patient has a displaced intra-articular tibial tuberosity fracture; therefore, the treatment of choice is open reduction and internal fixation. Periosteum is often interposed between the fracture fragments and prevents satisfactory closed reduction. Fortunately, most patients with this injury are close to skeletal maturity and therefore, growth arrest and recurvatum are unusual. Nondisplaced fractures can be treated with a cast, but displaced fractures are best treated with open reduction and internal fixation. Intra-articular fractures can disrupt the joint surface and are sometimes associated with a meniscal tear; therefore, arthroscopy may be needed at the time of open reduction and internal fixation. McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
References:
- Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
Question 73High Yield
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
Explanation
The patient has arthritis and supracondylar nonunion of the elbow. Total elbow replacement has been shown to give almost immediate return of function as it can be performed while leaving the triceps intact and resecting the distal humerus fragment. Attempts at osteosynthesis are indicated in younger individuals with good joint surface. Resection arthroplasty yields poor function and is reserved as a salvage procedure. Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
References:
- Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 74High Yield
A 7-year-old boy has a limp with pain and tenderness over the distal right femur. Radiographs are shown in Figures 5a and 5b. Based on these findings, what is the best course of action?
Explanation
Explanation
5b The patient has a nonossifying fibroma, and the symptoms suggest that there is significant weakening of the cortex and/or microfracture; therefore, biopsy, curettage, and bone grafting is the treatment of choice. Based on the size of the lesion and the presence of symptoms, observation is likely to result in pathologic fracture. A biopsy will further weaken the bone unless combined with curettage and bone grafting. Radiation therapy is not used in the treatment of nonossifying fibroma and is rarely used in any benign condition affecting skeletally immature individuals. Steroid injection has been used in the treatment of unicameral bone cysts and in Langerhan's cell histiocytosis but not for nonossifying fibroma. Dormans, JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
References:
- Easley ME, Kneisl JS: Pathologic fractures through nonossifying fibromas: Is prophylactic treatment warranted? J Pediatr Orthop 1997;17:808-813.
Question 75High Yield
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
Explanation
53b 53c 53d Heterotopic ossification may occur spontaneously or following trauma. The imaging studies and histology reveal mature fatty bone marrow and trabecular bone. Osteochondromas are cortically based with the medullary canal extending into the lesion. This is not evident in this patient. Also, no obvious cartilage cap is present. Parosteal osteosarcoma commonly occurs in the posterior distal femoral cortex but is ruled out by the lack of the typical fibrous stromal cells forming the low-grade malignant osteoid. The histology and clinical presentation eliminate osteomyelitis and osteoblastoma. Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388. Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
References:
- Mills WJ, Tejwani N: Heterotopic ossification after knee dislocation: The predictive value of the injury severity score. J Orthop Trauma 2003;17:338-345.
Question 76High Yield
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
Explanation
The spleen is the most common organ injured in the abdomen as the result of blunt trauma. It is also the most common cause of death because of an abdominal injury. The liver is the second most commonly injured organ. Injury to the other organs is rare. The diagnosis can be made with CT. Treatment ranges from observation to splenectomy, depending on the severity of injury. Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
References:
- Kibler WB (ed): ACSM's Handbook for Team Physician. Philadelphia, PA, Williams & Wilkins, 1996, p 151.
Question 77High Yield
What is the known manner in which the growth hormone-insulin-like growth factor-I (GH-IGF-I) system functions to stimulate bone growth?
Explanation
Explanation
IGF-I, formerly known as somatomedin-C, possibly acts by both paracrine and endocrine hormone pathways. The products of the GH-IGF-I system induce proliferation without maturation of the growth plate and thus induce linear skeletal growth. The action of the thyroid hormone axis is via an active metabolite that enters target cells and signals a nuclear receptor to stimulate both proliferation and maturation of the growth plate. Increased amounts of the active steroid hormone metabolite promote proliferation and maturation of the growth plate. Calcitonin inhibits bone resorption. Binder G, Grauer ML, Wehner AV, et al: Outcome in tall stature: Final height and psychological aspects in 220 patients with and without treatment. Eur J Pediatr 1997;156:905-910. Wang J, Zhou J, Cheng CM, et al: Evidence supporting dual, IGF-I-independent and IGF-I-dependent, roles for GH in promoting longitudinal bone growth. Endocrinol 2004;180:247-255.
References:
- Gertner JM: Childhood and adolescence, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 45-47.
Question 78High Yield
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a

Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 79High Yield
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 80High Yield
A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?
Explanation
Explanation
All but the Moberg osteotomy are capable of providing pain relief; however, arthrodesis offers the best long-term results and restores weight bearing and propulsion function to the first ray. Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.
References:
- Myerson MS, Schon LC, McGuigan FX, et al: Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Question 81High Yield
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?
Explanation
Explanation
The radiograph shows a bony avulsion of the ACL attachment site on the tibial spine in this skeletally immature patient. In this age group, injury often results in failure of the bony attachment site rather than the substance of the ligament. Avulsion of the patellar tendon insertion site can occur, but this structure is located at the apophysis of the tibial tubercle. The attachment site of the PCL is much more posterior. In adults, bony avulsion is more commonly associated with PCL injuries than with ACL injuries. When a small bony avulsion of the lateral capsule from the lateral tibial plateau is seen on the AP view, this finding is considered pathognomonic of an ACL injury (Segond sign) in adults. The area of the pes anserinus is anterior and distal; avulsion would be unusual. Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
References:
- DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 406-432.
Question 82High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?

Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 83High Yield
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?

Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 84High Yield
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Severe osteoporosis is a contraindication to manipulation under anesthesia in patients with a resistant frozen shoulder because of the higher risk of humeral fracture. Manipulation is considered for frozen shoulder in patients who are symptomatic despite undergoing a reasonable course of appropriate physical therapy. Harryman DT II: Shoulder: Frozen and stiff. Instr Course Lect 1997;42:247-257.
Question 85High Yield
Chronic anterior donor site pain following the harvest of autologous iliac crest bone graft for use during anterior cervical diskectomy and fusion is reported by approximately what percent of patients?
Explanation
Explanation
Four years after surgery, more than 90% of patients are satisfied with the cosmetic appearance of the iliac donor site scar. Approximately 25% still have pain and/or functional difficulty, including 12.7% who still report difficulty with ambulation, 11.9% difficulty with recreational activities, 7.5% with sexual intercourse, and 11.2% require pain medication for iliac donor site symptoms. Silber JS, Anderson DG, Daffner SD, et al: Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine 2003;28:134-139.
References:
- Cockin J: Autologous bone-grafting complications at the donor site. J Bone Joint Surg Br 1971;49:153.
Question 86High Yield
Figures 4a through 4c show the radiographs, CT scans, and T1-weighted MRI scan of a 19-year old man who has had increasing right hip pain and decreasing range of motion for the past several years. He also reports intermittent "locking" of the hip. What is the most likely diagnosis?
Explanation
Explanation
4b 4c The radiographs reveal small ossified masses around the femoral neck. The CT scans also show these masses and suggest that they are separate from the underlying cortex of the femoral neck, although they abut it. The MRI scan does not reveal significant marrow changes in the proximal femur apart from some mild reactive changes immediately adjacent to the nodules. These findings suggest a synovial or joint-based disorder as opposed to a primary bone tumor. The most likely diagnosis is synovial osteochondromatosis, which is consistent with the patient's mechanical symptoms. Crotty JM, Monu JU, Pope TL Jr: Synovial osteochondromatosis. Radiol Clin North Am 1996;34:327-342.
References:
- Frassica F: Orthopaedic pathology, in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 292-335.
Question 87High Yield
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Explanation
Explanation
While other surgical and nonsurgical options exist for management of spasticity, the criteria originally laid out by Peacock and associates describe the most appropriate candidate for rhizotomy as a patient with spastic diplegia who is between the ages of 4 to 8 years and has a stable gait pattern that is limited by lower extremity spasticity. Rhizotomy is not recommended in patients with athetosis because of unpredictable results. In addition, rhizotomy should be avoided in nonambulatory patients with spastic quadriplegia because it is associated with significant spinal deformities. Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
References:
- Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 88High Yield
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
Explanation
The patient has the typical history and presentation of transient synovitis of the hip, a condition that is more common in children age 2 to 5 years but which may affect children up to 12 years. The discomfort typically is noted on awakening, and the child will refuse to walk. Later in the day, the pain commonly improves and the child can walk but will have a limp. Mild to moderate restriction of hip abduction is the most sensitive range-of-motion restriction. The extent of the evaluation for transient synovitis depends on the intensity and duration of symptoms. Because she has been afebrile for the past 24 hours, observation is the management of choice. In the differential diagnosis of suspected transient synovitis, septic arthritis of the hip is the primary disorder to exclude. Osteomyelitis of the proximal femur also should be considered. In most patients, clinical examination will differentiate of these disorders to a reasonable certainty. Plain radiographs are normal in the early stage of an infectious process. Ultrasonography shows increased fluid in the hip joint in both transient synovitis and septic arthritis. MRI can differentiate the two conditions; however, this test would require general anesthesia and is not required in most patients in this age group. If a child with transient synovitis has a concurrent infectious process such as an upper respiratory tract infection or otitis media, the temperature will most likely be elevated. In this situation, a full evaluation for an infectious process and initiation of IV antibiotics should be considered. This would include radiographs, CBC count, erythrocyte sedimentation rate, blood cultures, aspiration of the hip joint, and IV antibiotics. Del Beccaro MA, Champoux AN, Bockers T, Mendelman PM: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Annals Emerg Med 1992;21:1418-1422.
References:
- Kehl DK: Developmental coxa vara, transient synovitis, and idiopathic chondrolysis of the hip, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1035-1058.
Question 89High Yield
A 12-year-old boy who pitches on two "select" baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of
Explanation
Explanation
19b The imaging study demonstrates characteristics of Little Leaguer's shoulder, including physeal widening. This condition is secondary to overuse (typically throwing) and responds well to rest from the inciting activity. There is no evidence from the patient's history or examination that he has an impingement syndrome, nor is there any indication of labral pathology on the MRI scan. The changes in the proximal humerus are classic for this condition and are not suggestive of a neoplastic process requiring biopsy for definitive diagnosis. Lipscomb AB: Baseball pitching injuries in growing athletes. J Sports Med 1975;3:25-34. Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
References:
- Barnett LS: Little league shoulder syndrome: Proximal humeral epiphysis in adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 90High Yield
Which of the following is considered the most important factor in eliminating infection in chronic osteomyelitis?
Explanation
Explanation
The most important factor in eliminating infection in chronic osteomyelitis is a complete debridement of the compromised bone and soft tissue. Antibiotics should be used in conjunction with surgical debridement. However, the foundation of treating infected bone is removal of the diseased tissue. Cierny G III, Cook WG, Mader JT: Ankle arthrodesis in the presence of ongoing sepsis: Indications, methods, and results. Orthop Clin North Am 1989;20:709-721. Cierny G, Zorn EZ: Arthrodesis of the tibiotalar joint for sepsis. Foot Ankle Clin 1996;1:177-197.
References:
- Richter D, Hahn MP, Laun RA, Ekkernkamp A, Muhr G, Osterman PA: Arthrodesis of the infected ankle and subtalar joint: Technique, indications and results of 45 consecutive cases. J Trauma 1999;47:1072-1078.
Question 91High Yield
What type of metastatic tumor most often has a lytic radiographic appearance?

Explanation
Lung carcinoma most often has a lytic radiographic appearance. Bladder and prostate carcinoma are usually blastic. Breast carcinoma can be both blastic and lytic. Thyroid carcinoma may be difficult to visualize radiographically and may be seen only on MRI scans. Metastatic osteosarcomas typically produce bone. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 92High Yield
Figure 1 shows the radiograph of a patient who underwent a total knee revision with a posterior stabilized mobile-bearing prosthesis and now has recurrent knee dislocations. What is the most likely cause?
Explanation
Explanation
The patient has a posterior stabilized total knee revision, and the femoral component has dislocated over the tibial polyethylene cam/post. This usually indicates a loose flexion gap, or "flexion instability." A loose flexion gap can occur due to undersizing of the femoral component, anteriorization of the femoral component, excessive distal augmentation of the distal femur, or collateral ligament insufficiency, especially if combined with posterior capsular insufficiency. Isolated laxity of the extension gap (with a well-balanced flexion gap) causes varus/valgus instability, but it rarely causes the femoral component to "jump" the tibial cam of a posterior stabilized tibial insert. Malrotation of the components may cause patellar instability or a rotational instability of the tibiofemoral joint but should not cause a frank posterior dislocation of the tibia, unless combined with other errors of balancing. Although a mobile-bearing total knee arthroplasty may be more sensitive to errors in balancing than a fixed-bearing total knee arthroplasty, this complication does not reflect a faulty prosthetic design. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 173-186, 227-249.
References:
- Clarke HD, Scuderi GR: Flexion instability in primary total knee replacement. J Knee Surg 2003;16:123-128.
Question 93High Yield
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
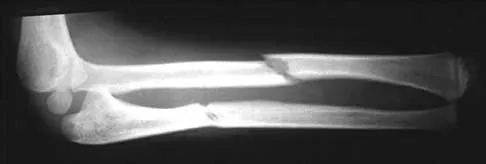
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 94High Yield
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
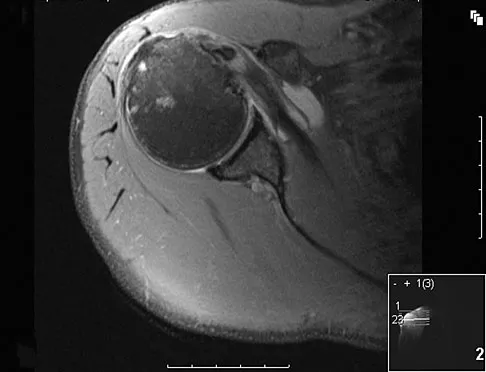
Explanation
The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 95High Yield
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 96High Yield
Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?
Explanation
Explanation
Implant-related fractures following hip fracture surgery were reported by Robinson and associates and showed that the risk of an ipsilateral femoral fracture is significantly increased with the use of short cephalomedullary nails as compared to a compression hip screw. The use of short cephalomedullary nails has not been shown to increase the risk of deep venous thrombosis or nonunion. Cephalomedullary nails overall have decreased surgical blood loss when compared to use of sliding-compression hip-screw devices. Robinson CM, Adams CI, Craid M, et al: Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am 2002;84:1116-1122.
Question 97High Yield
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
Explanation
The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).
References:
- Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 98High Yield
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
Explanation
15b 15c The biopsy specimen shows a wavy collagenous matrix with elongated cells; this is most consistent with neurofibroma. The patient has a mass in the region of the sciatic nerve. Imaging characteristics, homogeneous and very low signal on T1-weighted and very high signal on the T2-weighted sequences, are consistent with a myxoid-type lesion. These include myxoma, myxoid sarcomas, and nerve sheath tumors. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
References:
- Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 99High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?
Explanation
Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
References:
- Vocke AK, Vocke AR: Cartilaginous avulsion fracture of the tibial spine. Orthopedics 2002;25:1293-1294.
Question 100High Yield
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient's pain?
Explanation
Explanation
21b The difference in the clinical results combined with the laboratory findings points to infection. While there is a significant risk of false-positive findings with aspiration, the fact that two successive aspirations grew the same organism strongly suggests infection. The radiograph shows that there is more radiolucency around the left acetabular component than the right component. White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 1377-1385.
References:
- Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
