Orthopedic Surgery Board Exam Prep: 100 High-Yield MCQs (Set 594)

Key Takeaway
This page offers 100 high-yield orthopedic board review questions for ABOS, OITE, and FRCS board exams. Surgeons can practice these multiple-choice questions from Mock Exam Set 594 to master critical concepts and enhance their preparation. Achieve exam success with focused practice.
Master the Shoulder Joint Anterior: Surgical ...
00:00
Start Quiz
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
A positive jaw jerk reflex suggests that the problem is above the level of the pons. All of the other physical signs are exhibited in patients with cervical myelopathy. Although these signs also may be present in conditions affecting the brain, they do not help differentiate between a brain etiology and a cervical spine etiology. A jaw jerk reflex, however, is not present in patients with cervical myelopathy alone. Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493. Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
Question 3High Yield
Collagen orientation is parallel to the joint surface in what articular cartilage zone?
Explanation
Explanation
The collagen orientation changes from parallel in the superficial zone to a more random pattern in the middle zone and finally to perpendicular in the calcified zone. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 498-499.
References:
- Mankin HJ, Mow VC, Buckwalter JA: Articular cartilage structure, composition, and function, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 4High Yield
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?

Explanation
Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient's findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis. Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
Question 5High Yield
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 6High Yield
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
While guidelines for predicting fracture risk are at best imprecise, the scoring system by Mirels (pain, anatomic location, and pattern of bony destruction) has been shown to be most predictive of fracture risk. Functional pain, peritrochanteric location, and lytic bone destruction are the greatest risk factors for pathologic fracture. The factors of patient weight, age, soft-tissue mass, and location within bone are all of lesser importance. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 7High Yield
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of

Explanation
The coracoid process is an essential component of the superior shoulder suspensory complex and must be maintained. Open reduction and internal fixation is recommended if the fragment is large and displaced more than 1 cm. Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Question 8High Yield
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 9High Yield
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with
Explanation
Explanation
Reverse total shoulder arthroplasty is relatively contraindicated in patients with acromial stress fractures and rheumatoid arthritis. A patient with active forward elevation to 130 degrees is better treated with a hemiarthroplasty because the motion already exceeds the average forward elevation attained in most studies using the reverse prosthesis. A centered case of rotator cuff tear arthropathy is also better treated with a hemiarthroplasty, especially in patients with a large external rotation lag sign because the reverse prosthesis has been shown to decrease active external rotation. However, hemiarthroplasties have not performed well in patients with anterior superior escape and in this group of patients, the reverse prosthesis is best. Rittmeister M, Kerschbaumer M: Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J Shoulder Elbow Surg 2001;10:17-22. Visotosky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
References:
- Werner CM, Steinmann PA, Gilbart M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 10High Yield
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
Explanation
Resection of a previously excised soft-tissue sarcoma is recommended. Reoperation is recommended after removal of malignant tumors previously believed to be benign, as approximately one half of the patients will have residual tumor in the re-excised specimen. Observation is not indicated in most patients because local recurrence is likely. Radiation therapy alone may result in long-term local control but is felt to be less effective than reoperation. Chemotherapy and radiation therapy alone are not recommended. Wide excision is the most important factor for local disease control. Radiation therapy after surgical re-excision may also decrease the risk of local recurrence. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348. Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
References:
- Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 11High Yield
What is the most common anatomic location for chondrosarcoma?
Explanation
Explanation
The most common anatomic location of chondrosarcoma is the pelvis (30%), followed by the proximal femur (20%). Chondrosarcomas appear in the shoulder girdle in 15% of patients but rarely affect the spine or hands. Marcove RC, Mike V, Hutter RV, et al: Chondrosarcoma of the pelvis and upper end of the femur: An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am 1972;54:561-572.
References:
- Simon MA, Springfield DS, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 12High Yield
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?

Explanation
Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis. Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765. Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Question 13High Yield
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?
Explanation
Explanation
The radiograph shows a bony avulsion of the ACL attachment site on the tibial spine in this skeletally immature patient. In this age group, injury often results in failure of the bony attachment site rather than the substance of the ligament. Avulsion of the patellar tendon insertion site can occur, but this structure is located at the apophysis of the tibial tubercle. The attachment site of the PCL is much more posterior. In adults, bony avulsion is more commonly associated with PCL injuries than with ACL injuries. When a small bony avulsion of the lateral capsule from the lateral tibial plateau is seen on the AP view, this finding is considered pathognomonic of an ACL injury (Segond sign) in adults. The area of the pes anserinus is anterior and distal; avulsion would be unusual. Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
References:
- DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 406-432.
Question 14High Yield
The parents of a 13-year-old boy with Down syndrome report that he has an increasing limp and decreased endurance with activities. Lateral flexion-extension radiographs of the cervical spine show no evidence of instability. Examination reveals a right Trendelenburg limp and an obvious limb-length discrepancy. Hip motion is symmetric except for some decreased abduction on the right side. A standing AP radiograph is shown in Figure 20. Management should consist of

Explanation
Ligamentous laxity and muscle hypotonia seen in Down syndrome contribute to the incidence of hip subluxation and dislocation. These factors can be progressive and lead to degenerative arthritis in adults with Down syndrome. Because this patient has a progressive limp and decreased endurance, observation and a shoe lift are not options. Bracing may be an option in the younger child before significant bony changes occur. Surgical intervention is the treatment of choice in this patient; however, all components of the deformity need to be addressed. Because of the increased capsular laxity, there is a high likelihood of recurrence if capsulorrhaphy is not included with the pelvic and femoral osteotomies. Surgery in these patients is associated with a high rate of complications. Shaw ED, Beals RK: The hip joint in Down's syndrome: A study of its structure and associated disease. Clin Orthop 1992;278:101-107. Aprin H, Zinc WP, Hall JE: Management of dislocation of the hip in Down's syndrome. J Pediatr Orthop 1985;5:428-431.
Question 15High Yield
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?

Explanation
Based on the MR arthrogram in which gadolinium (bright on T1-weighted images) was injected into the joint space prior to imaging, the study shows a tear of the anterior band of the ulnar collateral ligament (UCL). The disruption in the distal end of the UCL is outlined by contrast. A small collection of contrast extravasation into the flexor musculature further confirms the presence of a tear. The UCL has a broad-based attachment on the medial epicondyle and has a pointed or tapered attachment distally on the ulna. Most UCL tears occur distally at the ulnar (coronoid) attachment. MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 16High Yield
Which of the following patients is considered the most appropriate candidate for an isolated split posterior tendon transfer?

Explanation
Isolated split posterior tendon transfer alone is best performed in a patient with cerebral palsy who is between the ages of 4 and 7 years and has a flexible equinovarus foot. Rigid deformities often must be managed with a combination of soft-tissue and bony procedures. Patients with out-of-phase activity may be best managed with a transfer of the posterior tibialis to the dorsum of the foot, while those with continuous activity are better candidates for an isolated split posterior tendon transfer. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 291-294. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Question 17High Yield
A 72-year-old woman with rheumatoid arthritis who underwent primary total knee arthroplasty 2 years ago has had diffuse knee pain that developed shortly after the surgery. The patient has difficulty with stair descent and arising from chairs. Evaluation for infection is negative. AP and lateral radiographs are shown in Figure 26. Management should now consist of
Explanation
Explanation
The radiographs show posterior flexion instability that is the result of flexion-extension gap imbalance and/or posterior cruciate ligament incompetence after a posterior cruciate-retaining total knee arthroplasty. The radiographs also show anterior femoral displacement on the tibia. Pagnano and associates reported on a series of patients with painful total knee arthroplasties who had been previously diagnosed as having pain of unknown etiology, showing that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
References:
- Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 18High Yield
What is the most appropriate orthosis for hallux rigidus?

Explanation
A Morton's extension limits excursion of the first metatarsophalangeal joint. It also functions as a ground reaction stabilizer during the toe-off phase of gait and thus reduces torque and joint reaction force at the first metatarsophalangeal joint. The metatarsal arch pad and full-length semi-rigid longitudinal arch support may help by dorsiflexing the first metatarsal relative to the phalanx and thus decompress the first metatarsophalangeal joint. However, they are not as biomechanically effective as the Morton's extension. Both medial hindfoot and lateral forefoot posting are contraindicated because they increase ground reaction at the first metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Question 19High Yield
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
Explanation
The coronal MRI scan of the wrist shows the scaphoid. There is a subtle fracture line with a step-off at the radial surface consistent with a nonunion. The signal intensity is markedly different between the two fragments of the scaphoid. This strongly suggests osteonecrosis. Preiser's disease is osteonecrosis typically involving most or all of the scaphoid. Kienbock's disease involves the lunate. Intraosseous ganglia are easily diagnosed on MRI but typically have a fluid-filled area surrounded by denser bone in the periphery. Scapholunate dissociation can be seen on MRI as an injury to the scapholunate ligament and widening of the scapholunate interval, neither of which is seen on this image.
References:
- Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 20High Yield
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?

Explanation
To mobilize the common iliac vessels across the midline, the iliolumbar vein must be ligated. It has a short trunk and can be torn if mobilization is attempted without ligation. It is the only branch off the common iliacs (there are no arterial branches) prior to the terminal branches, the internal (hypogastric) and external iliacs. The middle sacral vessels run distally from the axilla of the bifurcation and are a factor when accessing the L5-S1 disk. Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
Question 21High Yield
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
Explanation
23b The flexor hallucis longus tendon is at risk during a Chevron-Akin osteotomy because of its close relationship to the base of the proximal phalanx. The radiograph reveals a reduced ability to flex the interphalangeal joint secondary to the flexor hallucis longus laceration. The other complications are not supported by the radiograph. Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
References:
- Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 22High Yield
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?

Explanation
In this patient, the radial nerve is most likely injured at the level of the radial neck. The radial nerve emerges from the posterior cord of the brachial plexus and travels along the spiral groove of the humerus. At the level of the lateral humeral condyle, the radial nerve branches into the posterior interosseous nerve after giving off two cutaneous branches, the superficial radial and the posterior cutaneous. The posterior interosseous nerve travels through the supinator muscle and winds around the radial neck. At this level, the posterior interosseous nerve is vulnerable to injury, particularly following fracture or penetrating trauma. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Question 23High Yield
During excision of a Baker cyst, the base or stalk is usually found between the
Explanation
Explanation
Although there are several bursae in the posterior portion of the knee, the most prevalent one with a connection to the knee joint is the one in the interval between the semimembranosus and the medial head of the gastrocnemius muscle. The popliteus muscle and posterior cruciate ligament, the posterior cruciate ligament and lateral gastrocnemius muscle, and the medial gastrocnemius muscle and posterior cruciate ligament are all too lateral and uncommon. The semitendinosus and medial head of the gastrocnemius muscles do not come in contact in the posterior aspect of the knee. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 379.
References:
- Justis EJ Jr: Nontraumatic disorders, in Crenshaw AH (ed): Campbell's Operative Orthopaedics, ed 7. Philadelphia, PA, Lippincott, 1987, vol 3, p 2257.
Question 24High Yield
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
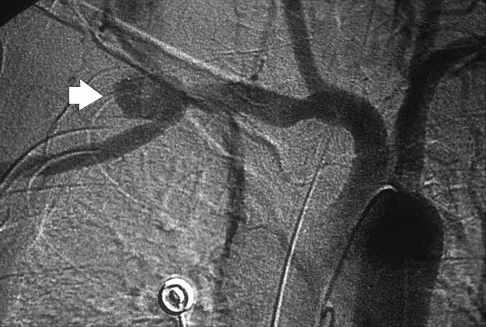
Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
Question 25High Yield
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Explanation
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism. Tencer AF, Johnson KD: Biomechanics in Orthopaedic Trauma: Bone Fracture and Fixation. Philadelphia, PA, JB Lippincott, 1994. Gonza ER: Biomechanical long bone injuries, in Gonza ER, Harrington IJ (eds): Biomechanics of Musculoskeletal Injury. Baltimore, MD, Williams & Wilkins, 1982, pp 1-30.
Question 26High Yield
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
Explanation
The radiograph reveals posterolateral rotatory subluxation of the radiohumeral and ulnohumeral joints. The space between the ulna and trochlea is enlarged, particularly posteriorly at the olecranon. These findings are diagnostic of posterolateral rotatory instability, which causes recurrent subluxation and reduction as the elbow is flexed from an extended and supinated position with valgus load. The posterolateral rotatory instability apprehension test was performed on this patient and the result was positive. The lateral pivot-shift test causes a clunk as the elbow reduces but is more difficult to perform, even under general anesthesia. The patient does not have isolated subluxation of the radial head, although these findings can be mistakenly diagnosed as such. The radial head is normally shaped and does not represent a congenital dislocation. There are no findings here to suggest osteochondritis dissecans or loose bodies. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446. Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
References:
- Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 27High Yield
Figures 13a and 13b show the preoperative radiographs of a 60-year-old woman who is scheduled to undergo total knee arthroplasty under epidural anesthesia. Postoperatively she reports a burning sensation on the dorsum of her foot despite the administration of IV analgesics through a patient-controlled analgesia (PCA) pump. Management should now include
Explanation
Explanation
13b The patient has a significant flexion contracture and valgus deformity; therefore, the risk of peroneal nerve injury is increased. Idusuyi and Morrey noted that epidural anesthesia also increases the risk of peroneal nerve injury. The initial symptom can be a burning sensation on the foot, followed by pain and then motor weakness. Initial management should consist of release of the dressings and knee flexion. Idusuyi OB, Morrey BF: Peroneal nerve palsy after total knee arthroplasty: Assessment of predisposing and prognostic factors. J Bone Joint Surg Am 1996;78:177-184.
References:
- Rose HA, Hood RW, Otis JC, Ranawat CS, Insall JN: Peroneal nerve palsy following total knee arthroplasty: A review of The Hospital for Special Surgery experience. J Bone Joint Surg Am 1982;64:347-351.
Question 28High Yield
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 29High Yield
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
Explanation
Explanation
This is an example of tethering of the flexor hallucis longus/flexor digitorum longus (FHL/FDL) to the fracture site. Additional time and/or physical therapy and bracing would not be expected to be of benefit. Release of the FHL and FDL from the fracture site or retromalleolar lengthening will address the posttraumatic claw toe deformity and Achilles tendon lengthening will address the mild equinus. Posterior tibial tendon transfer is not appropriate as the patient demonstrates a normal heel rise. Midfoot releases and hallux fusion are also not indicated. Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.
References:
- Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.
Question 30High Yield
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?

Explanation
Solitary bone lesions require biopsy, for there is the possibility that the lesion may represent a primary bone sarcoma, which will necessitate a different treatment plan. This is especially true in patients with remote histories of cancer. The most likely cause of a lytic bone lesion in a patient older than age 40 years is a metastatic lesion. Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 31High Yield
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
Explanation
48b Angular deformities of the ankle can occur following physeal injury. While an orthosis may be beneficial, the deformity is at the level of the ankle rather than the hindfoot. An epiphysiodesis or physeal bar resection would not be indicated as the growth plates are closed. Correction of the angular deformity should level the ankle joint and normalize the weight-bearing stresses on the ankle. This is most easily achieved with a closing wedge distal tibial osteotomy with or without concomitant osteotomy of the fibula. Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442. Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
References:
- Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 32High Yield
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20 degrees of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked "A," the resulting ligament reconstruction will excessively

Explanation
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90 degrees. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20 degrees to 0 degrees of flexion. If the graft is tensioned in significant flexion (greater than 60 degrees), it will be excessively loose as the knee fully extends. Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Question 33High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 34High Yield
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
The average location of the anterior portal is 6.3 cm distal to the anterior superior iliac spine. The lateral femoral cutaneous nerve typically has divided into three or more branches at the level of the anterior portal. The portal usually passes within several millimeters of the most medial branch. Injury to the nerve can lead to meralgia paresthetica. The femoral nerve lies an average minimum distance of 3.2 cm from the anterior portal. The ascending branch of the lateral circumflex artery lies approximately 3.7 cm inferior to the anterior portal. Neither the ascending branch of the medial circumflex artery nor the superior gluteal nerve are at risk. Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Question 35High Yield
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient's symptoms?
Explanation
Explanation
8b The patient has a solid ankle fusion radiographically. With a tibiotalar arthrodesis, the adjacent joints (subtalar and transverse tarsal) take additional stress. Over time, progressive degenerative arthritis will occur in these adjacent joints, often necessitating further surgery. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
References:
- Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 36High Yield
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced

Explanation
The literature supports similar clinical outcomes after surgical and nonsurgical methods. The chief difference lies in the complications between the groups. Surgical patients experience more wound problems but a significantly lower rerupture rate. Although suturing the tendon allows earlier mobility, the tendon healing time is unchanged. Nonsurgical methods are less expensive to provide. Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Question 37High Yield
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of

Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 38High Yield
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be

Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 39High Yield
The Lisfranc ligament connects the base of the
Explanation
Explanation
The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
References:
- Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 40High Yield
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Explanation
Explanation
55b 55c The histology shows extraskeletal myxoid chondrosarcoma, characterized by abundant blue myxoid matrix with cords and nests of small tumor cells. Treatment consists of wide resection. Despite the name, hyaline cartilage is not a common component of these tumors. Adult rhabdomyosarcoma and malignant fibrous histiocytoma are highly pleomorphic sarcomas often containing multinucleated giant cells. Myxoid liposarcoma contains a prominent capillary network and lipoblasts. Myxoma is less cellular than extraskeletal myxoid chondrosarcoma and does not have a cord-like arrangement of tumor cells.
References:
- Kawaguchi S, Wada T, Nagoya S, Ikeda T, Isu K, Yamashiro K, et al: Extraskeletal myxoid chondrosarcoma. Cancer 2003;97:1285-1292.
Question 41High Yield
One advantage of using onlay strut allograft in femoral revision surgery is that it can

Explanation
Onlay grafts can provide more structural support than morcellized grafts. They are more easily incorporated into the host femur than bulk segmental total femur allografts; however, the incorporation is never complete. The use of onlay grafts is principally directed at addressing segmental defects of the femur; their use can be applied with either cementless or cement fixation of the femoral stem. Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44. Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Question 42High Yield
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
Explanation
The incidence of osteolysis, particularly around fixation screws in the tibia, can be as high as 30%. Stable femoral component fixation is generally maintained. Infection, subluxation of the patella, and stiffness can occur with either cemented or cementless fixation. Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
References:
- Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 43High Yield
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Explanation
Explanation
If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson's fracture. Patients with this type of injury usually require fusion. Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
References:
- Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 44High Yield
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?
Explanation
Explanation
Based on findings of a sudden increase in pain with associated swelling, the most likely diagnosis is a stress fracture. The initial radiographic findings usually will be negative. Morton's neuroma and transfer metatarsalgia are not associated with swelling. Metatarsophalangeal synovitis usually involves the second metatarsophalangeal joint. Freiberg's infraction is seen clearly on a radiograph.
References:
- Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 45High Yield
Chemotherapy is routinely included in the treatment of which of the following soft-tissue sarcomas?

Explanation
Most soft-tissue sarcomas are treated with a combination of radiation therapy and wide resection. Rhabdomyosarcomas are an exception, where chemotherapy is included in all treatment plans. Chemotherapy for other soft-tissue sarcomas is controversial. Enzinger FM, Weiss SW: Rhabdomyosarcoma, in Soft Tissue Tumors, ed 3. St Louis, MO, CV Mosby, 1995, p 539.
Question 46High Yield
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb's point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
Explanation
Explanation
The change noted is focal and confined to the cortex, sparing the opposite side, both lower extremities, and the subcortical waveforms, making all the choices unlikely with the exception of carotid compression with focal cortical ischemia. This may be associated with poor collateral flow from the opposite hemisphere due to an incomplete circle of Willis. Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Question 47High Yield
A 29-year-old woman reports dysesthesias and burning after undergoing bunion surgery that consisted of a proximal crescentic first metatarsal osteotomy 6 months ago. Examination reveals a positive Tinel's sign at the proximal aspect of the healed incision. What injured nerve is responsible for her continued symptoms?
Explanation
Painful incisional neuromas after bunion surgery frequently involve the dorsomedial cutaneous branch of the superficial peroneal nerve. This is the medial branch of the superficial peroneal nerve that terminates as the dorsomedial cutaneous nerve to the hallux. Branches of the deep peroneal nerve to this area are rare, and no branches to this area exist from the sural nerve. The saphenous nerve branches are generally more proximal, and the medial plantar nerve lies plantarly. Kenzora JE: Sensory nerve neuromas: Leading to failed foot surgery. Foot Ankle 1986;7:110-117.
Question 48High Yield
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?

Explanation
The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
Question 49High Yield
A 47-year-old woman has had left medial clavicle pain for the past 6 months. History is remarkable for mediastinal non-Hodgkin's lymphoma, treated with mantel radiation 22 years ago. A radiograph, CT scan, MRI scan, and a biopsy specimen are shown in Figures 68a through 68d. What is the most likely diagnosis?
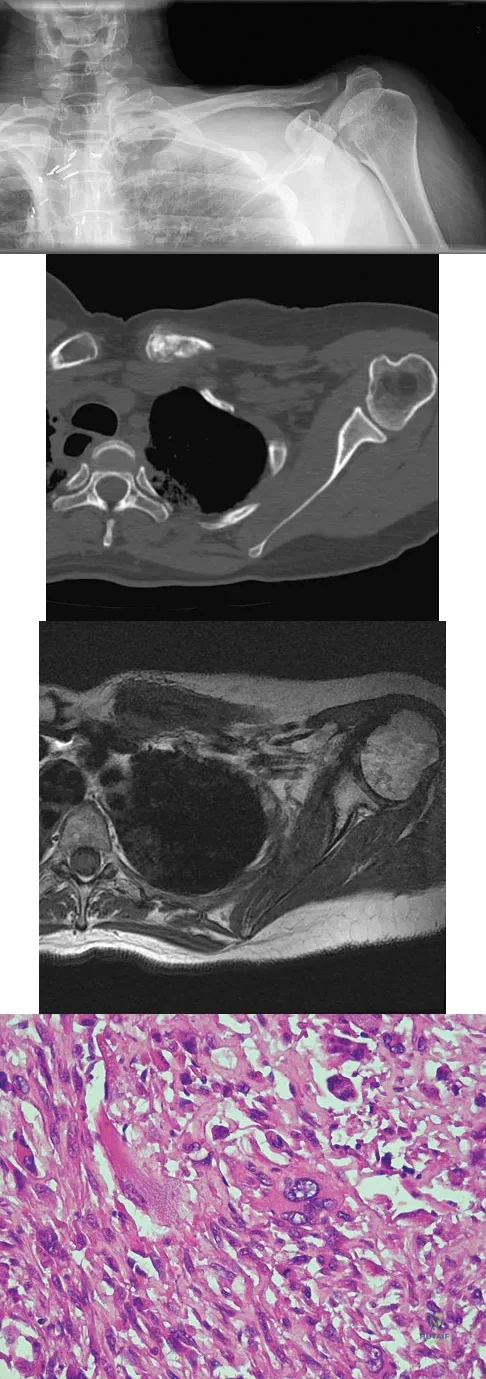
Explanation
Radiation-associated sarcomas typically occur at least 5 years following radiation therapy, in the radiation therapy field, and with different histology than the original disease. The radiograph shows a lytic destructive lesion of the medial clavicle. The radiographic differential could include any of the above etiologies. The CT and MRI scans show this same reaction with extension into the adjacent soft tissue and periosteal reaction. These findings eliminate a degenerative process or radiation-induced osteonecrosis but do not distinguish between a neoplastic and infectious process. A PET scan showed marked uptake in the distal clavicle, which is more consistent with a malignant neoplastic process than a reactive process, like that of an infection. These findings, combined with the cellular atypia and bone formation on the biopsy specimen, confirm the diagnosis of radiation-associated sarcoma. In this older patient, radiation-associated sarcoma appears in an unusual location secondary to her previous radiation treatment in that region, which can occur 3 to 50 years after previous radiation therapy. Shaheen M, Deheshi BM, Riad S, et al: Prognosis of radiation-induced bone sarcoma is similar to primary osteosarcoma. Clin Orthop Relat Res 2006;450:76-81.
Question 50High Yield
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?

Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 51High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?

Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 52High Yield
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
The mainstay of early treatment of open fractures includes irrigation and debridement. Prior to the development of antibiotics, this was traditionally accomplished with some form of detergent irrigation. Antibiotic irrigation has been in favor more recently but has mixed scientific results related to its use. Results of at least one major study show the use of a nonsterile liquid soap additive (castile soap) is at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, and shows a significant decrease in problems with soft-tissue healing.
Question 53High Yield
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
The etiology of hip fractures in the elderly is multifactorial, and intervention and prevention can occur at multiple points. Events leading to hip fracture from a fall include fall initiation (during which the individual's neuromuscular status, cognitive status, and vision come into play along with environmental hazards); fall descent (fall direction toward the side being the most influential, energy content of the fall, and fall height, along with muscle activity of the muscles of the thigh); impact (impact location, soft-tissue attenuation such as from trochanteric padding or from overlying fat, impact surface, and muscle activity); and the structural capacity of the femur (bone mineral density, bone geometry, and bone architecture). Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
Question 54High Yield
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
Explanation
The factors that are independently prognostic of patient survival are tumor size, tumor grade, and tumor depth (ie, subfascial versus superficial). These factors are the basis for the American Joint Committee on Cancer staging criteria. Patient age and neurovascular invasion are not prognostic. Surgical margin is prognostic for local recurrence but not conclusively for patient survival or metastasis. Metastatic disease is also predictive of survival. Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
References:
- Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 55High Yield
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?

Explanation
Because of the previously transferred bone block of coracoid and short arm flexors, the musculocutaneous nerve often scars along the anteroinferior glenohumeral capsule. Mobilization of this tissue places the nerve at greatest risk. The axillary nerve is also potentially at risk, but this is nonspecific to prior surgery, particularly the Bristow procedure. Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 98-116.
Question 56High Yield
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
Explanation
The recent JBJS article by Kocher and associates defines the different psychometric properties that are used in outcome measures. Reliability is a measure of how reproducible a test is. This can be interobserver reliability (ie, reliability between people), or intraobserver reliability (ie, reliability for the same person doing the outcome measure at different occasions).
References:
- Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 57High Yield
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 58High Yield
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
Explanation
Without more distal immobilization such as a thigh extension, the lower two lumbar segments generally show the same or even increased mobility with a TLSO. White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
References:
- Norton PL, Brown T: The immobilizing efficiency of back braces. J Bone Joint Surg Am 1957;39:111-139.
Question 59High Yield
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
Explanation
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
References:
- Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 60High Yield
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
Explanation
Erb's palsy is the most common form of obstetrical plexus palsy resulting in C5, C6, or upper trunk deficits. This causes loss of shoulder abduction and elbow flexion. The biceps muscle and the brachialis muscles are predominately responsible for flexion of the elbow. Each of these muscles is innervated by individual branches of the musculocutaneous nerve which are supplied predominately by axons from the C6 nerve root and the upper trunk of the brachial plexus. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 28-29. Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, pp 1255-1272.
References:
- Zancolli E: Reconstructive surgery in brachial plexus sequelae, in Gupta A, Kay S, Scheker L (eds): The Growing Hand. London, England, Mosby, 1999, p 807.
Question 61High Yield
What is the most common pediatric soft-tissue sarcoma?

Explanation
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
Question 62High Yield
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Explanation
4b Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
References:
- Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 194-202.
Question 63High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303. Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
References:
- Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 64High Yield
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
Explanation
Chronic lateral instability is commonly associated with a longitudinal split tear of the peroneus brevis tendon. The interrelationship of lateral ankle instability with superior retinacular laxity and resultant peroneus brevis split can account for persistent lateral ankle pain in this patient. Surgical treatment must identify and correct the underlying tendon pathology and should attempt to repair or debride the peroneus brevis tendon, reconstruct the superior peroneal retinaculum, flatten the posterior edge of the fibula by removing the sharp bony prominence, or deepening the fibular groove, along with addressing lateral ankle ligamentous instability. The laboratory values are not consistent with infection. A negative anterior drawer test confirms stability of the repair. Ankle arthritis is not seen on radiographs and usually takes longer than 3 months to develop. Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Question 65High Yield
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
Explanation
The surgeon perforated the anterior longitudinal ligament and injured the common iliac artery. Bingol and associates described injuries to the vascular structures during lumbar disk surgery. The common iliac artery was most commonly affected and constituted 76.9% of injuries.
Question 66High Yield
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
Explanation
In the absence of a cauda equina syndrome or progressive weakness, the best indication for surgical management is refractory radicular pain. Surgical decision-making should not be based on the size of the herniation. Large extruded herniations tend to resolve more predictably than smaller herniations. Stable motor weakness and numbness resolve similarly in both surgical and nonsurgical management, although surgery hastens the process. When intractable radicular pain is the strict indication for surgery, surgical intervention provides substantial and more rapid pain relief than nonsurgical care. Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 67High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for

Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 68High Yield
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Explanation
Explanation
Recurrent dislocations may follow an earlier dislocation. One study found that in patients who had a patellar dislocation between the ages of 11 to 14 years, 60% had a recurrent dislocation. The incidence of recurrent dislocation dropped to 33% in patients who had a patellar dislocation between the ages of 15 to 18 years. The authors also found that the incidence of recurrence was greater in patients who demonstrated a predisposition to dislocation as determined by evaluation of the unaffected knee. Predisposing signs included passive lateral hypermobility of the patella, a dysplastic distal third of the vastus medialis obliquis muscle, and a high and/or lateral position of the patella. A second study found that the risk of redislocation was considerably higher in patients who were in their teens at the first episode of dislocation compared to older patients. There are no studies linking either a patella baja or a bipartite patella to an increased risk of redislocation. Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
References:
- Larsen E, Lauridsen F: Conservative treatment of patellar dislocations: Influence of evident factors on the tendency to redislocation and the theraputic result. Clin Orthop 1982;171:131-136.
Question 69High Yield
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of

Explanation
The patient has extensor tendon ruptures at the level of the wrist that are the result of synovitis at the distal radioulnar joint (Vaughn-Jackson syndrome). Extensor indius proprius transfer appropriately matches strength and excursion of the ruptured extensor digiti quinti and extensor digitorum communis tendons. An extensor tenosynovectomy with distal radioulnar joint resection decreases the synovitis, which if left untreated may cause additional tendon ruptures. Radial head resection is used for posterior interosseous nerve compression secondary to radial head synovitis, and in this patient only two fingers are involved, which rules out this diagnosis. Dynamic splinting is not indicated for ruptured tendons. Metacarpophalangeal arthroplasties and imbrication of the sagittal bands are used for metacarpophalangeal arthritis and extensor tendon subluxation. If this was the problem, the patient should be able to maintain the fingers in extension after they are passively extended. Total wrist arthrodesis prevents the tenodesis effect, thus limiting effective tendon excursion and making the proposed transfer less effective. Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1669-1684. Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Question 70High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 71High Yield
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of

Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 72High Yield
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient's program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study. Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Question 73High Yield
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely

Explanation
The patient has a cervical myelopathy with more than 10 mm of space available for the cord; therefore, she has a reasonable chance of improved neurologic function following surgery. If not treated with surgery, however, her neurologic condition likely will worsen and she will die earlier than if she had surgery. Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Question 74High Yield
Figure 29 shows the radiograph of a 10-year-old boy who injured his knee playing football. What is the most appropriate initial treatment?
Explanation
Explanation
Salter type I fractures of the distal femur are quite unstable; therefore, closed reduction and cast immobilization can be expected to result in high rates of redisplacement. Optimal treatment consists of open or closed reduction and smooth pin fixation, and supplemental casting is required to ensure fracture stability. Screw fixation may increase rates of growth plate injury. Blade plate or flexible nail fixation will be challenging to apply and is not necessary. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Thomson JD, Stricker SJ, Williams MM: Fractures of the distal femoral epiphyseal plate. J Pediatr Orthop 1995;15:474-478.
Question 75High Yield
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
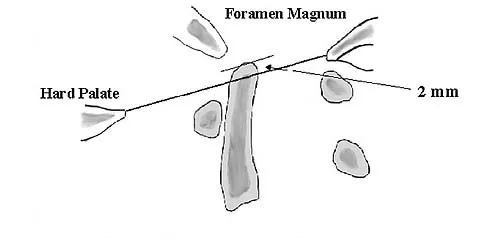
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 76High Yield
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of

Explanation
Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified. Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine 1992;17:1137-1143. Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Question 77High Yield
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
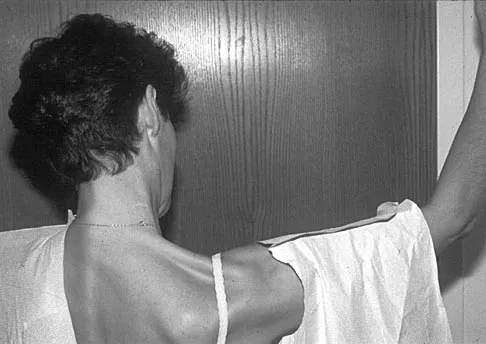
Explanation
The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 78High Yield
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
If the flexion gap is tight and the extension gap is correct, it is preferable to change only the flexion gap and leave the extension gap unchanged; therefore, the treatment of choice is to decrease the size of the femoral component. The smaller component will be smaller in both medial-lateral as well as anterior-posterior dimensions. A smaller anterior-posterior size will allow more space for the flexion gap without significantly affecting the extension gap. Decreasing the size of the tibial polyethylene insert thickness or cutting more proximal tibia will affect both the flexion and extension gaps. Cutting more distal femur will increase the extension gap and not change the flexion gap, making the described situation worse. Cutting both the proximal tibia and distal femur will increase both the flexion and extension gaps.
Question 79High Yield
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 80High Yield
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
Explanation
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure. Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607. Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
References:
- Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 81High Yield
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
Advocates of resurfacing hip arthroplasty cite preservation of the proximal femoral bone stock as the main advantage of this procedure over total hip arthroplasty. Fracture of the retained femoral neck has been reported following resurfacing arthroplasty. The exact etiology of the latter is unknown. Technical errors, such as notching of the femoral neck or possibly disruption of the blood supply to the femoral head during extensive soft-tissue exposure, may result in femoral neck fracture. Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Question 82High Yield
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
In children, the main route of infection in skeletal TB is through hematogenous spread from a primary source. The mycobacterium is deposited in the end arterials in the vertebral body adjacent to the anterior aspect of the vertebral end plate. Thus, the anterior portion of the vertebral body is most commonly involved. The lower thoracic region is the most common segment; next in decreasing order of frequency are the lumbar, upper thoracic, cervical, and sacral regions. Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Question 83High Yield
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
Explanation
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Question 84High Yield
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 85High Yield
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?

Explanation
The resultant spasticity and weakness (paresis) following a cerebrovascular accident leads to muscle imbalance that commonly results in contracture of the shoulder in adduction, internal rotation, and varying degrees of forward flexion. In addition, the elbow is usually flexed and the forearm pronated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 86High Yield
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
The patient has snapping hip syndrome of the internal type, which is more common in ballet dancers. It is caused by the iliopsoas tendon gliding over the iliopectineal line or the femoral head. The diagnosis usually can be made by the history and physical examination. Snapping is reproduced by hip flexion and extension or flexion with external rotation and abduction. Conventional and dynamic ultrasonography will confirm the snapping structure. Radiographs occasionally show calcifications near the lesser trochanter. MRI can be used to rule out other diagnoses that can simulate snapping hip. Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Question 87High Yield
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
Surgical curettage or en bloc resection is the treatment of choice for osteoid osteoma. Night pain and relief of symptoms with nonsteroidal anti-inflammatory drugs are classic findings for osteoid osteoma. Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598. Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Question 88High Yield
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
Explanation
The sympathetic trunk runs longitudinally along the medial border of the psoas. The ilioinguinal nerve emerges along the upper lateral border of the psoas and travels to the quadratus lumborium, and the genitofemoral nerve lies more laterally on the psoas. The ureter is adherent to the posterior peritoneum and falls away from the psoas and the spine in the dissection, as does the aorta. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
References:
- Johnson R, Murphy M, Sourthwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 89High Yield
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Explanation
Explanation
20b 20c The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
References:
- Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 90High Yield
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?

Explanation
Stress fractures of the navicular are often seen in running and jumping sports. Whereas most individuals heal with nonsurgical management consisting of 6 weeks of casting, this gymnast has had pain for 1 year and nonsurgical management has failed. Open reduction with bone grafting is the preferred treatment. Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Question 91High Yield
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Explanation
Measurements of compartment pressures in patients with tibial fractures and compartment syndrome reveal that the highest tissue pressures are recorded at the level of the fracture or within 5 cm of the fracture. Tissue pressures show a statistically significant decrease when they are recorded at increasing distances proximal and distal to the site of the highest pressure recorded. To reliably determine the location of the highest tissue pressure in patients with tibial fractures, measurements should be obtained, at a minimum, in both the anterior and deep posterior compartments at the level of the fracture, as well as at locations proximal and distal. The highest tissue pressure recorded should serve as a basis for determining the need for fasciotomy. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
References:
- Whitesides TE Jr, Heckman MM: Acute compartment syndrome: Update on diagnosis and treatment. J Am Acad Orthop Surg 1996;4:209-218.
Question 92High Yield
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be

Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 93High Yield
An axial T1-weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
Explanation
The obturator internus muscle originates from the internal pelvic wall and passes laterally through the lesser sciatic foramen, banking around the ischium below the sacrospinous ligament before inserting on the medial aspect of the greater trochanter. Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
References:
- Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 94High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 95High Yield
Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
Explanation
Explanation
At the ankle level, the anterior tibial artery lies medial to the EHL tendon. The artery becomes the dorsalis pedis after crossing onto the dorsum of the foot. At this point, the artery lies lateral to the tendon. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Question 96High Yield
What structure provides the major blood supply to the humeral head?
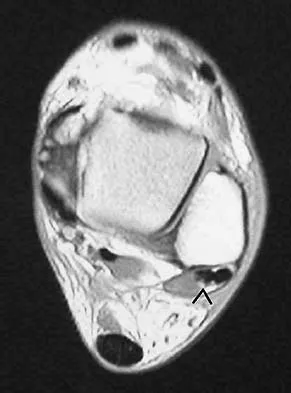
Explanation
The ascending branch of the anterior circumflex humeral artery provides the major blood supply to the humeral head. The posterior circumflex humeral artery supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 97High Yield
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
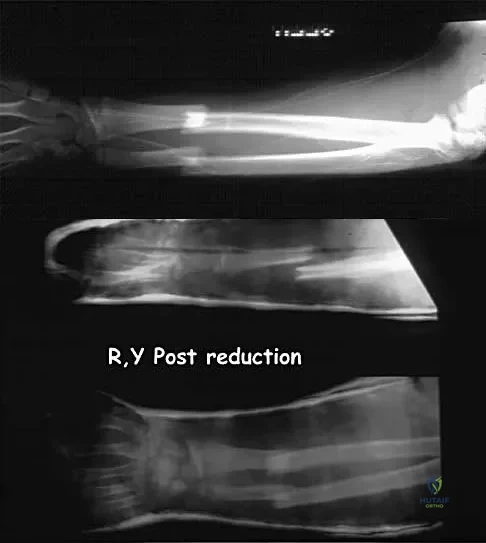
Explanation
Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity. Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Question 98High Yield
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
References:
- Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 31-37.
Question 99High Yield
What structure is most often injured in a volar proximal interphalangeal joint dislocation?

Explanation
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Question 100High Yield
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
Explanation
Positioning of the femoral and tibial components is a common cause of early failure of total knee arthroplasty. Two modes of possible position are raising or lowering the joint line from its anatomic level. Raising or lowering the joint line beyond an established threshold can cause limited range of motion, poor patellar function, and possible instability. It has been determined that a threshold of approximately 8 mm provides consistently good results after knee arthroplasty.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
