Orthopedic Board Exam Prep: 100 High-Yield MCQs | Set 426
14 Apr 2026
100 min read
84 Views
Key Takeaway
This page provides 100 high-yield orthopedic board review questions (MCQs) for ABOS, OITE, and FRCS exam preparation. Surgeons can utilize this randomized mock test (Set 426) to assess their knowledge, identify weak areas, and effectively prepare to master their orthopedic certification exams.
Acute Jones Fractures: Understanding ORIF & S...
00:00
Start Quiz
Question 1High Yield
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
Internal rotators of the shoulder include the subscapularis, pectoralis major, teres major, and latissimus dorsi muscles. The subscapularis has two portions, with the upper portion receiving its innervation from the upper subscapular nerve (C5) and the lower portion from the lower subscapular nerve (C5-6). The two tests commonly performed to isolate the internal rotation to the subscapularis muscle are the lift-off test and the belly press test. Electromyographic findings have shown the lift-off test to be more accurate for the lower portion of the subscapularis and the belly press test to be more sensitive for the upper portion. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Question 2High Yield
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Question 3High Yield
Etanercept is a recombinant genetically engineered fusion protein used to treat rheumatoid arthritis. What is its mode of action?
Explanation
Explanation
Etanercept is a molecule consisting of the Fc portion of IgG fused to the extracellular domain of the p76 human THF-a receptor. It is soluble and binds TNF-a. Infliximab is the monoclonal antibody that binds TNF-a. IL-1 receptor antagonists are still in development. Leflunomide is a drug that inhibits pyrimidine synthesis and is similar to methotrexate as an antimetabolite.
References:
- Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 4High Yield
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by
Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Question 5High Yield
Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?
Explanation
Explanation
The labeled structure is the LCL, and it is avulsed from the lateral humeral epicondyle. This is the most common site of injury for the LCL. The biceps and brachialis tendon insertions are not well visualized in this section. The MCL and flexor/pronator origin are intact. Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.
References:
- King JC, Spencer EE: Lateral ligamentous instability: Techniques of repair and reconstruction. Techniques in Orthopaedics 2000;8:93-104.
Question 6High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
References:
- Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 7High Yield
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?

Explanation
The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 8High Yield
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of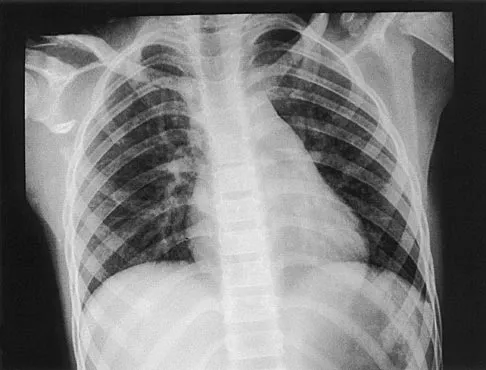


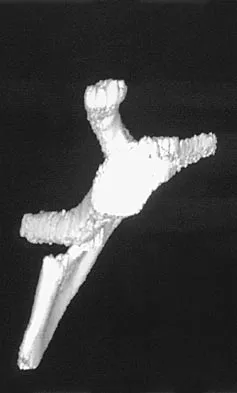
Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 9High Yield
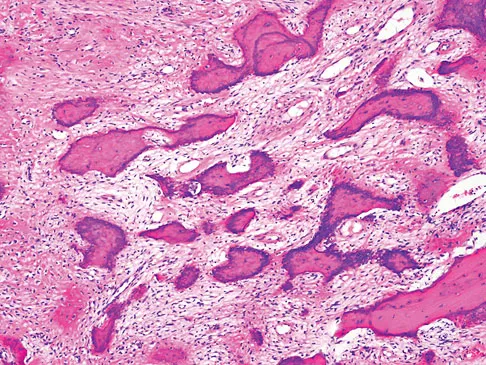
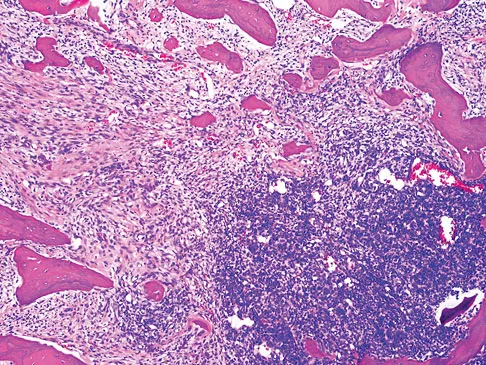
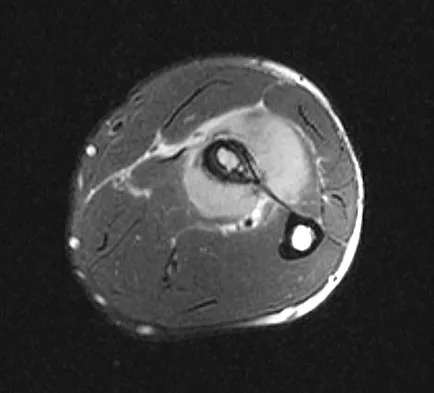
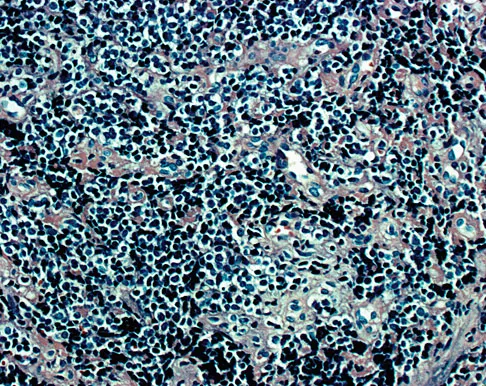
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?
Explanation
Explanation
45b 45c 45d Giant cell tumors typically occur in a juxta-articular location involving the epiphysis and metaphysis of long bones, usually eccentric in the bone. The radiographs show a destructive process within the distal tibia and an associated soft-tissue mass. The histology shows multinucleated giant cells in a bland matrix with a few scattered mitoses. Osteosarcoma can have a similar destructive appearance but a very different histologic pattern with osteoid production. Ewing's sarcoma also can have a diffuse destructive process in the bone. The histologic pattern of Ewing's sarcoma is diffuse round blue cells. Aneurysmal bone cysts typically are seen as a fluid-filled lesion on imaging studies and have only a scant amount of giant cells histologically. Metastatic adenocarcinoma does not demonstrate the pattern shown in the patient's histology specimen. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
References:
- Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 200-202.
Question 10High Yield
A senior resident is scheduled to perform a posterior medial release on a 10-month-old infant who has a congenital clubfoot deformity. Informed consent is obtained for the procedure. The supervising surgeon is obligated to give the parents what information?
Explanation
Explanation
Informed consent is generally considered to be a process of mutual decision making between the physician and patient. The physician is required to provide to the patient all material information that is needed for the patient to make an informed decision. The courts have held that a patient's choice of surgeon is as important to the consent as the procedure itself. Assistance by a surgical trainee with adequate supervision is permissible when there has been adequate disclosure. Adequate supervision may be defined as active participation by the attending during the essential parts of the procedure. Allowing a substitute surgeon to operate on a patient without the patient's knowledge "ghost surgery" may result in charges of battery against the substitute surgeon and malpractice against the surgeon to whom the patient gave consent. Kocher MS: Ghost surgery: The ethical and legal implications of who does the operation. J Bone Joint Surg Am 2002;84:148-150.
References:
- Holmes MK: Ghost surgery. Bull NY Acad Med 1980;56:412-419.
Question 11High Yield
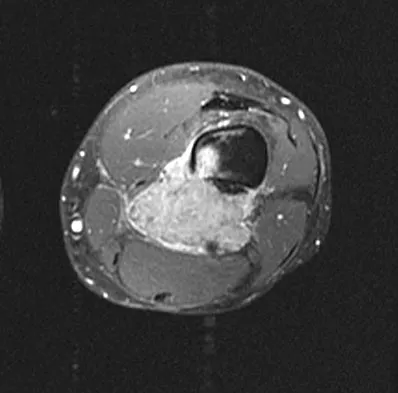
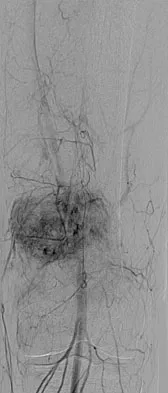
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T1-weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?

Explanation
Dedifferentiated parosteal osteosarcoma designates high-grade transformation of conventional low-grade parosteal osteosarcoma. Unlike conventional parosteal osteosarcoma, where wide surgical excision alone is considered adequate treatment, patients with dedifferentiated osteosarcoma are treated with neoadjuvant chemotherapy and wide local resection. Recognition of dedifferentiated areas with angiography can localize the area that should be biopsied and thus render an accurate diagnosis. Percutaneous biopsy of hypervascular areas should prompt the administration of chemotherapy and wide local excision to optimize patient outcome. Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Question 12High Yield
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?
Explanation
The MRI scan reveals an abnormal signal in the trapezoid, which lies adjacent to the capitate in the distal carpal row. The tumor is a giant cell tumor of bone. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240. bar based on these measurements is shown in Figure 54d. Initial treatment should consist of 1- bony bar resection and distal fibula epiphysiodesis. 2- bony bar resection and corrective osteotomy. 3- bony bar resection and physiodesis of the opposite distal tibial physis. 4- corrective osteotomy and a limb-lengthening procedure. 5- corrective osteotomy and physiodesis of the opposite distal tibial physis. 2 54a 54b 54c 54d Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 13High Yield
In a longitudinal study of children with spastic diplegia, analysis of long-term function will most likely reveal
Explanation
In a longitudinal study of 18 patients with spastic diplegia over a period of 32 months, three-dimensional gait analysis revealed a deterioration of gait stability with increases in double support time and decreases in single support time. Kinematic data also identified a loss of excursion about the knee, ankle, and pelvis. Interestingly, the static examination of the children showed a decrease in the popliteal angle over time. The authors concluded that ambulatory ability tends to worsen over time in children with spastic diplegia.
Question 14High Yield
The sartorius muscle is innervated by which of the following nerves?
Explanation
Explanation
The femoral nerve enters the thigh behind the inguinal ligament, lying on the surface of the iliopsoas muscle lateral to the femoral artery and vein. The nerve divides into numerous muscular and cutaneous branches in the femoral triangle. The first motor branch (sometimes two branches) is to the sartorius. There is a variable branch to the pectineus. Subsequent branches go to the rectus femoris and then the vastus muscles in variable order. The last motor branch is to the articularis genu. The muscular branches can be injured in anterior approaches to the hip, especially the middle window of the ilioinguinal approach. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 139.
Question 15High Yield
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
The superior gluteal artery is most at risk with a posterior iliac crest bone graft harvest. The artery leaves the pelvis through the sciatic notch and can be injured by retractors or other sharp instruments entering the sciatic notch area. The deep circumflex iliac, iliolumbar, and fourth lumbar arteries supply the iliacus and iliopsoas muscles and can be damaged during anterior bone graft harvest. The ascending branch of the lateral femoral circumflex artery is at risk during the anterior approach to the hip. Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Question 16High Yield
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Explanation
Explanation
20b 20c The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
References:
- Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 17High Yield
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of
Explanation
The MRI findings show highly increased signal through the entire femoral head and neck that is diagnostic of transient osteoporosis of the femoral head. This recently described entity is often seen in middle-aged men and should be treated nonsurgically with protected weight bearing and anti-inflammatory drugs. The natural history is that of self-resolution. Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 18High Yield
Which of the following statements best describes the location of the nerve that is at risk in a direct posterior approach to the Achilles tendon?
Explanation
The sural nerve lies lateral to the Achilles tendon at the level of the foot but follows an oblique course proximally to lie directly over the tendon as it heads to the popliteal fossa. It is at risk with any proximal dissection from a direct posterior approach and in particular with procedures done at the musculotendinous junction. The nerve crosses over the lateral border of the Achilles tendon at an average of 9.8 cm above its insertion. Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Question 19High Yield
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
Explanation
The size of the rotator cuff tear in both anteroposterior and mediolateral dimensions has been found to correlate best with outcome. Older patient age and rupture of the long head of the biceps tend to be associated with larger tears and, therefore, may be associated indirectly with a poorer outcome. Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
References:
- Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 20High Yield
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?
Explanation
Explanation
Curettage and bone grafting typically is the preferred method of treatment for chondroblastoma, with local recurrence rates of approximately 10%. Some clinicians advocate the addition of adjuvants such as phenol. Left alone, these lesions can destroy bone and invade the joint. Large intra-articular lesions may require major joint reconstruction. Wide local excision rarely is required to eradicate the tumor. Radiation therapy rarely is indicated and only for unresectable or multiply recurrent lesions. Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
References:
- Simon MA, Springfield DS, et al: Chondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 21High Yield
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of
Explanation
Explanation
Congenital dislocation of the knee is an uncommon deformity that varies in presentation from simple hyperextension to complete anterior dislocation of the tibia on the femur. Treatment varies with the age at presentation and the severity of the deformity. Most authors recommend early nonsurgical management. A recent study of 24 congenital knee dislocations in 17 patients found that satisfactory results were obtained in most instances using closed treatment. Based on their findings, the authors concluded that immediate reduction or serial casting should be performed when the patient is seen early after birth. If the patient is seen late and correction cannot be achieved by serial casting, traction followed by closed or open reduction may be necessary. Early percutaneous quadriceps recession has been described for complex congenital knee dislocations associated with underlying disorders, such as arthrogryposis and Ehlers-Danlos syndrome. Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259. Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
References:
- Roy DR, Crawford AH: Percutaneous quadriceps recession: A technique for management of congenital hyperextension deformities of the knee in the neonate. J Pediatr Orthop 1989;9:717-719.
Question 22High Yield
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in
Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 23High Yield
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of
Explanation
In patients with myelomeningocele, the presence of bilateral hip dislocation does not affect ambulation, bracing requirements, sitting ability, degree of scoliosis, or level of comfort. There is little evidence to support active treatment of bilateral hip dislocations in patients with myelomeningocele proximal to L4. Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Question 24High Yield
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Question 25High Yield
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?
Explanation
The patient has a very wide humeral growth plate, indicating the presence of a proximal humeral stress fracture, an uncommon diagnosis in gymnasts. Gymnasts are prone to stress fractures of the scaphoid, distal radius, elbow, and clavicle. Proximal humeral stress fractures are more commonly seen in those participating in racket or throwing sports. Stress fractures can lead to growth arrest or inhibition, particularly in the distal radius. The radiograph shows normal findings for the acromion, acromioclavicular joint, scapula, and triceps origin. Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449. Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202. Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Question 26High Yield
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?


Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 27High Yield
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Explanation
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
References:
- Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 28High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 29High Yield
Up to what time frame are the risks minimized in anterior revision disk replacement surgery?
Explanation
Revision anterior exposure within 2 weeks of total disk replacement incurs relatively little additional morbidity because adhesion formation is minimal. Surgeons should have a low threshold for revising implants that are clearly dangerously malpositioned or show early migration within this 2-week window. Beyond this time period, a revision strategy must be individualized to the particular clinical situation. A posterior fusion with instrumentation with or without a laminectomy is currently the most effective salvage procedure.
Question 30High Yield
A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of
Explanation
Explanation
The child has the classic findings of Kohler's disease or osteochondrosis of the tarsal navicular. The cause of this condition is not known, but osteonecrosis and mechanical compression have been proposed. Children generally report midfoot pain over the tarsal navicular and limping. Physical findings include tenderness, swelling, and occasionally redness in the region of the tarsal navicular. Radiographs show sclerosis and narrowing of the tarsal navicular. The natural history of the condition is spontaneous resolution and reconstitution of the navicular. Symptomatic treatment with restriction of weight bearing or casting is recommended. Karp M: Kohler's disease of the tarsal scaphoid. J Bone Joint Surg 1937;19:84-96.
References:
- Borges JL, Guille JT, Bowen JR: Kohler's bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 31High Yield
A newborn with bilateral talipes equinovarus undergoes serial manipulation and casting. What is the primary goal of manipulation?
Explanation
Manipulative treatment and casting of talipes equinovarus has become popular because of disappointing surgical results and enthusiasm for the Ponseti method of manipulation. In this technique, the primary goal is to rotate the foot laterally around a talus that is held fixed by the manipulating surgeon's hands. While the navicular may be rotated anterolaterally with this technique, the primary focus is on the calcaneus. The calcaneus is rotated laterally and superiorly, not translated. Some dorsiflexion of the calcaneus can be obtained by manipulation, but the primary focus is on the rotational relationship of the talus and calcaneus, not the degree of calcaneal dorsiflexion. Ponseti IV: Common errors in the treatment of congenital clubfoot. Int Orthop 1997;21:137-141.
Question 32High Yield
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 33High Yield
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
References:
- Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 34High Yield
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of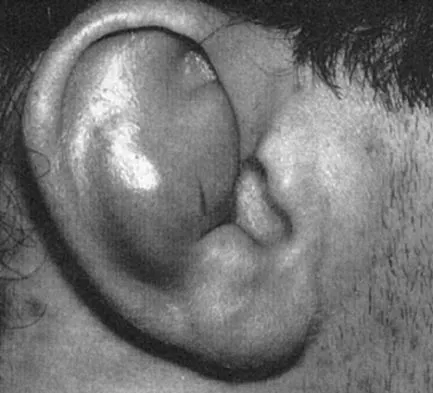
Explanation
Loss of internal rotation is common among overhead throwers and tennis players. Posterior capsular stretching can improve symptoms when accompanied by rest and gradual resumption of throwing. To avoid a false impression of improvement, cortisone injection is not recommended. Pitching through pain can cause further damage to the labrum and capsule. A sling and external rotator strengthening will not improve internal rotation. Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Question 35High Yield
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
Explanation
With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Question 36High Yield
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?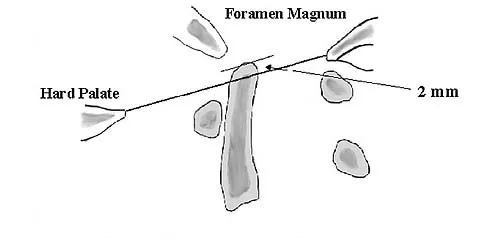
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 37High Yield
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
Explanation
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool. Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
References:
- Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 38High Yield
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T1- and T2-weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?

Explanation
The imaging studies show a permeative lytic destructive lesion in the proximal radius with "hair-on-end" periosteal reaction and a large soft-tissue mass most consistent with Ewing's sarcoma. The pathology reveals monotonous sheets of "round blue" cells. This limits the differential diagnosis to primary lymphoma of bone versus Ewing's sarcoma. These are best differentiated by immunohistochemistry, cytogenetics, and flow cytometry. Lymphoma of bone is typically CD34 positive and CD99 negative; whereas, the reverse is true of Ewing's sarcoma, CD34 negative and CD99 positive. The most common cytogenetic translocation with Ewing's sarcoma is 11; 22; 21; 22 and 7; 22 translocations have also been reported in Ewing's sarcomas. The X; 18 translocation is most commonly associated with synovial cell sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Flow cytometry is used to characterize the cell types of lymphomas. Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21. Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing's sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Question 39High Yield
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
Explanation
Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.
Question 40High Yield
A 65-year-old man has a painful right hip mass that has been growing for several years. A radiograph, CT scan, and photomicrograph are shown in Figures 56a through 56c. What is the most appropriate treatment?


Explanation
This is a conventional chondrosarcoma. The radiograph and the CT scan show a lesion arising from the inferior pubic ramus with a large soft-tissue mass. Abundant punctate, stippled, or "popcorn-like" calcification is present. The photomicrograph demonstrates hypercellular cartilage. Surgical resection is the only effective treatment. Whereas chemotherapy might play a role in the treatment of a dedifferentiated chondrosarcoma, it has no role in the treatment of a conventional chondrosarcoma. Chondrosarcomas are relatively radioresistant. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 41High Yield
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Isometric quadriceps contraction between 15 and 30 degrees of flexion creates significant strain in the ACL and potential damage to the reconstructed graft. Isolated quadriceps contraction with knee flexion of greater than 60 degrees, hamstring contraction at any angle of knee flexion, and active knee motion between 35 and 90 degrees of flexion create substantially less strain in the properly implanted ACL graft. Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Question 42High Yield
A 12-year-old boy with an ankle fracture undergoes closed reduction under sedation in the emergency department. Figure 27 shows a lateral radiograph of the ankle after two attempts at closed reduction. Based on these findings, treatment should now consist of
Explanation
The widening of the physis associated with incomplete reduction of this fracture suggests that periosteum is interposed at the fracture site. Clinical and animal study findings suggest that the interposed periosteum may lead to premature physeal closure. Repeated forceful attempts at reduction may subject the physis to further injury and should be avoided. Growth problems are common in children with Salter-Harris type I fractures of the lower extremities. Nonunions are rare in children with Salter-Harris type I fractures. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibial physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 43High Yield
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
Explanation
Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients. Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
References:
- Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 44High Yield
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?
Explanation
Explanation
28b 28c Excessive hindfoot valgus can lead to abutment between the calcaneus and fibula. This valgus force can lead to a stress fracture of the distal fibula. Surgery may be required if an insufficiency fracture recurs despite orthotic management. Of the choices listed, a subtalar arthrodesis is most likely to achieve rebalancing of the foot at the level of the deformity. Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
References:
- Easley ME, Trnka HJ, Schon LC, Myerson MS: Isolated subtalar arthrodesis. J Bone Joint Surg Am 2000;82:613-624.
Question 45High Yield
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
Explanation
27b 27c The osseous sites most frequently involved by giant cell tumor of bone are the distal femur, proximal tibia, and distal radius with approximately 10% of giant cell tumors involving the distal radius. The goals of treatment are to remove the tumor completely and to preserve maximum function of the extremity.
References:
- Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 46High Yield
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis?
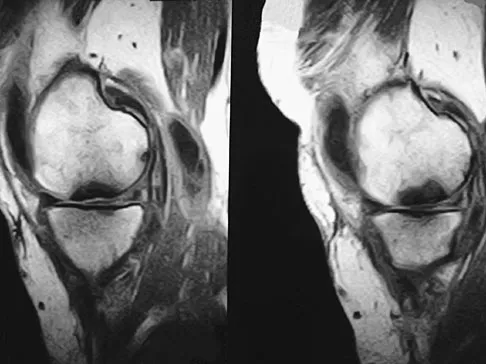
Explanation
Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial. Kidwai AS, Hemphill SD, Griffiths HJ: Spontaneous osteonecrosis of the knee reclassified as insufficiency fracture. Orthopedics 2005;28:236,333-336. Soucacos PN, Xenakis TH, Beris AE, et al: Idiopathic osteonecrosis of the medial femoral condyle: Classification and treatment. Clin Orthop 1997;341:82-89.
Question 47High Yield
Figures 27a through 27c show the radiographs and CT scan of a 27-year-old man who sustained a low-velocity gunshot wound to the neck. He is quadriplegic (ASIA A), hemodynamically stable, and does not have drainage from his wound. After initial resuscitation and stabilization, the cervical spine and spinal cord injuries are best managed by
Explanation
Explanation
27b 27c Although the spinal canal has been penetrated, the lateral masses are intact bilaterally with only partial destruction of the vertebral body and penetration of the lamina on one side, thus the cervical spine is not unstable and surgical stabilization is not indicated. Dural repair is not indicated since there is no external cerebrospinal fluid leakage. Surgical treatment should be based on the need to treat extraspinal pathology only. Bono CM, Heary RF: Gunshot wounds to the spine. Spine J 2004;4:230-240.
Question 48High Yield
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
The superior gluteal nerve is located approximately 7.82 cm above the tip of the greater trochanter as it courses through the gluteus medius. This anatomic consideration is relevant during a Hardinge approach to the hip, where excessive proximal dissection or retraction could result in nerve injury. A split of the gluteus medius of no more than 4 cm above the greater trochanter is considered safe. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Question 49High Yield
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
Explanation
Pediatric intracapsular hip fractures are challenging because of the high rates of complications, including osteonecrosis and varus malunion. These patients should be treated as emergencies. Principles of treatment include anatomic reduction with internal fixation. Screw fixation short of the physis is preferred and may need to be supplemented with spica cast immobilization. Fixation may be achieved with smooth pins across the physis when little metaphyseal bone is available. Fixation across the physis with threaded screws is acceptable only when the patient is close to skeletal maturity. Pediatric hip screws are appropriate if immediately available. Emergent open reduction, capsulotomy, or joint aspiration may decrease the rate of osteonecrosis. Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343. Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420. Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
References:
- Morsy HA: Complications of fracture of the neck of the femur in children: A long-term follow-up study. Injury 2001;32:45-51.
Question 50High Yield
Figure 6 shows a sagittal oblique MRI scan. The arrow is pointing to what structure?
Explanation
The meniscofemoral ligaments connect the posterior horn of the lateral meniscus to the intercondylar wall of the medial femoral condyle. The ligament of Humphrey (arrow) passes anterior to the posterior cruciate ligament, whereas the ligament of Wrisberg passes posterior to the posterior cruciate ligament. One or the other has been identified in 71% to 100% of cadaver knees, with the ligament of Wrisberg being more common. Clarke HD, Scott WN, Insall JN, et al: Anatomy, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 3-66.
Question 51High Yield
A 55-year-old woman fell and sustained an elbow dislocation with a coronoid fracture and a radial head fracture. The elbow is reduced and splinted. What is the most common early complication?
Explanation
The patient has a dislocation of the elbow with displaced coronoid process and radial head fractures. The elbow is extremely unstable after this injury, and recurrent dislocation in a splint is the most common early complication. Skeletal stabilization of the fractures is required to restore stability of the joint. Characteristics of the fractures will determine the techniques required to restore stability. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 52High Yield
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
Explanation
The artery of the tarsal canal is a branch of the posterior tibial artery. Among the branches of the artery of the tarsal canal is the deltoid artery. This arterial complex supplies the medial one third of the talar body. Disruption of this artery may lead to osteonecrosis of the medial body and subsequent collapse into varus. This is most commonly seen with talar body fractures but may be seen in Hawkins type 3 talar neck fractures. The artery of the tarsal sinus arises from the dorsalis pedis, lateral malleolar, and perforating peroneal arteries. The peroneal artery anastomoses with the calcaneal branches of the posterior tibial artery to form a plexus of vessels that supplies the posterior tubercle of the talus. Disruption of this artery would not result in collapse of the medial body, and thus would not lead to a varus deformity. Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
References:
- Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 53High Yield
A 20-year-old woman has had wrist pain for the past 5 months. A radiograph, MRI scans, and biopsy specimen are shown in Figures 46a through 46d. The patient is then treated with intralesional surgery. The patient should be counseled that her risk of developing lung metastasis is approximately what percent?
Explanation
Explanation
46b 46c 46d Giant cell tumor of bone has about a 2% risk of benign pulmonary metastasis in all cases and 6% risk in recurrent cases. The radiograph and MRI scans show a lytic destructive lesion in the distal radius with no matrix mineralization. The lesion extends up to the subchondral bone. In a young woman, the most likely diagnosis is giant cell tumor of bone, which is supported by the pathology results that show monotonous fibrovascular stroma with numerous multinucleated giant cells where the nuclei that make up the giant cells are identical to the nuclei that make up the background stromal cells. Athanasian EA, Wold LE, Amadio PC: Giant cell tumors of the bones in the hand. J Hand Surg Am 1997;22:91-98.
References:
- Siebenrock KA, Unni KK, Rock MC: Giant-cell tumor of bone metastasizing to the lungs: A long-term follow-up. J Bone Joint Surg Br 1998;80:43-47.
Question 54High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 55High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic. Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
References:
- Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 56High Yield
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
Explanation
The patient has iliac apophysitis. The radiographic findings are easily overlooked but usually reveal slight asymmetric widening of the iliac crest apophysis. The apophysis is the most vulnerable structure, as it is three to five times weaker than the tendon. This is not an epiphyseal site, and injury to the muscle or the tendinous insertion to bone (enthesis) is unlikely. Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218. Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293. Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
References:
- Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 57High Yield
Involvement of what single muscle best distinguishes an L5 radiculopathy from a peroneal neuropathy?
Explanation
Explanation
All of the muscles are innervated by the peroneal nerve with the exception of the tibialis posterior which is innervated by the tibial nerve. Tibialis posterior function is best tested with resistance to plantar flexion and inversion.
References:
- Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, pp 291-296.
Question 58High Yield
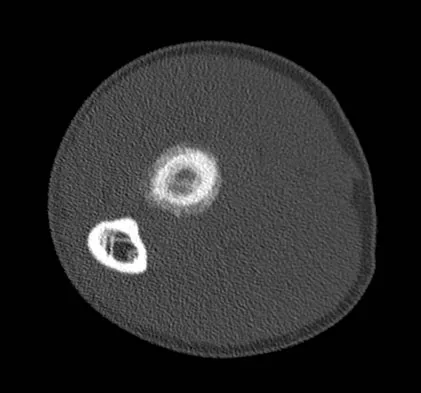
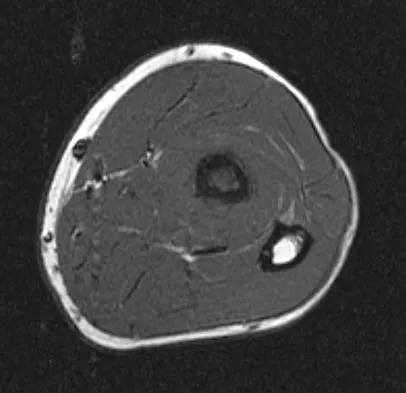
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
Explanation
12b 12c The use of locked nailing for the treatment of established nonunion of the humerus has produced poor results. Since humeral nailing has already failed, exchange humeral nailing without bone grafting has an even less change of success. To increase the likelihood of achieving bony union, the treatment of choice is removal of the humeral nail, dynamic compression plating, and bone grafting. Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
References:
- Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach, an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 59High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?


Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 60High Yield
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
Explanation
Miller and associates reported the results of a cadaveric study of the vascular risk of a posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. The average distance from the screw to the popliteal artery was 21.1 mm (range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon's finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle. Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804. Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
References:
- Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 61High Yield
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
BMPs signal through the activation of a transmembrane serine/threonine kinase receptor that leads to the activation of intracellular signaling molecules called SMADs. There are currently eight known SMADs, and the activation of different SMADs within a cell leads to different cellular responses. The other mediators are not believed to be directly involved with BMP signaling. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 62High Yield
What structure is marked Q in the diagram of the brachial plexus shown in Figure 22?
Explanation
From proximal to distal, the brachial plexus is divided into roots, trunks, divisions, and cords before forming specific peripheral nerve branches. The structure marked Q is called the posterior cord because it lies posterior to the axially artery at the level of the cords. Its terminal branches are the upper subscapular (V), thoracodorsal (W), lower subscapular (X), axillary (F), and radial (G) nerves. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-24.
Question 63High Yield
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of
Explanation
Explanation
The clinical scenario describes infantile tibia vara (Blount's disease). The radiograph shows severe deformity with the characteristic Langenskiold stage 3 changes of the medial proximal tibial metaphysis that distinguish it from physiologic bowing. The preferred treatment is proximal tibiofibular osteotomy with acute correction into slight valgus to unload the damaged area of the physis. This method provides the best results in patients younger than age 4 years. Continued observation would result in progressive deformity. Bracing is most effective in younger children with less severe deformity. Lateral proximal tibial hemiepiphysiodesis relies on growth of the injured medial physis for correction and would result in severe tibial shortening in this young child. Complete epiphysiodesis also produces severe shortening and requires multiple lengthening procedures. Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
References:
- Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount's disease. J Pediatr Orthop 1998;18:374-380.
Question 64High Yield
What is the function of the rotator cuff during throwing?
Explanation
Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
References:
- Abrams JS: Special shoulder problems in the throwing athlete: Pathology, diagnosis, and nonoperative management. Clin Sports Med 1991;10:839-861.
Question 65High Yield
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?

Explanation
Osteolysis in the trochanteric bed can result in weakening of the bone and fracture. Nonsurgical management will provide reasonable clinical and radiographic results in patients with limited fracture displacement. Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Question 66High Yield
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 67High Yield
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?
Explanation
The grading of response to chemotherapy for osteosarcoma was introduced by Huvos and associates. Patients with tumors that show more than 90% necrosis after neoadjuvant chemotherapy are considered to have had a good response and have better survival rates than those with less than 90% necrosis. However, it should be noted that survival rates for patients with a poor response are still better than in patients who do not receive neoadjuvant chemotherapy. More recently, similar results have been reported in patients with Ewing's sarcoma. Chemotherapy is not typically used for giant cell tumor of bone. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Question 68High Yield
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
Explanation
The use of multiagent chemotherapy has been shown to be associated with a survival benefit in patients with osteosarcoma. The use of chemotherapy in adults with soft-tissue sarcoma remains somewhat controversial. It has not been associated with improved survival rates in patients with renal carcinoma, dedifferentiated chondrosarcoma, or melanoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
References:
- Link M, Goorin A, Miser A, et al: The effect of adjuvant chemotherapy and relapse free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 69High Yield
A Trendelenburg gait is most likely to be seen in association with
Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 70High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
Explanation
25b The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
References:
- Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 71High Yield
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Explanation
Explanation
Plate and screw fixation of allograft is associated with the highest incidence of union but also the highest prevalence of allograft fracture. Conversely, intramedullary fixation is associated with a higher incidence of nonunion but fewer fractures. Step-cut osteotomies are not associated with a higher incidence of union.
References:
- Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 72High Yield
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
The major determinant of ALS (Lou Gehrig disease) is progressive loss of motor neurons. The loss usually begins in one area, is asymmetrical, and later becomes evident in other areas. The first signs of ALS may include either upper or lower motor neuron loss. Recognition of upper motor neuron involvement depends on clinical signs, but electromyography and nerve conduction velocity studies can help identify lower motor neuron involvement. Electrodiagnostic abnormalities in three or more areas are required to make a definitive diagnosis. The motor unit potentials (MUPs) changes in ALS include impaired MUPs recruitment, unstable MUPs, and abnormal MUPs size and configuration. A number of abnormal spontaneous discharges can occur with ALS, especially fibrillation potentials and fasciculation potentials. In ALS, the motor nerve conduction study will be abnormal, but a co-existing normal sensory study is definitive for this disease. de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348. Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
References:
- Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 73High Yield
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
Explanation
Retrograde ejaculation is a sequela of injury to the superior hypogastric plexus. The structure needs protection, especially during anterior exposure of the lumbosacral junction. The use of monopolar electrocautery should be avoided in this region. The ideal exposure starts with blunt dissection just to the medial aspect of the left common iliac vein, sweeping the prevertebral tissues toward the patient's right side. Although erectile dysfunction can be seen after spinal surgery, it is not typically related to the surgical exposure because erectile function is regulated by parasympathetic fibers derived from the second, third, and fourth sacral segments that are deep in the pelvis and are not at risk with the anterior approach. The other choices are complications of spinal surgery but are not uniquely associated with an anterior L5-S1 exposure. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
References:
- An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 74High Yield
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
Explanation
Children with cerebral palsy are often difficult to examine. However, this patient clearly has a peroneal nerve deficit, most likely from the acute stretch after the hamstring lengthening. The nerve has the best chance of recovery if it is relaxed by flexing the knee. Once the nerve has recovered, gradual knee extension can be accomplished. Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
References:
- Heydarian K, Akbarnia BA, Jabalameli M, Tabador K: Posterior capsulotomy for the treatment of severe flexion contractures of the knee. J Pediatr Orthop 1984;4:700-704.
Question 75High Yield
Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?
Explanation
Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy. Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.
Question 76High Yield
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?



Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 77High Yield
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
References:
- Wold LA, et al: Ewing's Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 210-211.
Question 78High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 79High Yield
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
Explanation
In patients with radial nerve injuries with closed humeral fractures, it has been reported that 85% to 95% spontaneously recover. Based on this premise, most surgeons favor expectant management of these injuries. Even if there is no evidence of recovery at 6 weeks, repeat electromyography at 12 weeks is advocated. If there is no clinical or electromyographic signs of recovery at 6 months, exploration is recommended. If the nerve is in continuity at the time of exploration, nerve action potentials are useful in helping determine the need for neurolysis, excision, and grafting, or if excision and repair is the best option. Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
References:
- Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 80High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?

Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 81High Yield
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Explanation
Explanation
Because the MRI scan shows a complete rupture of the distal biceps tendon, the preferred treatment is anatomic repair of the tendon to the radial tuberosity either with the use of suture anchors or transosseous sutures through a two-incision technique. Several studies have documented superior results with anatomic repair of the distal biceps tendon when compared with results of nonsurgical management or repair of the tendon by attachment to the brachialis muscle. Patients undergoing anatomic repair of the distal biceps tendon through a two-incision technique typically regain a functional range of motion and nearly normal strength. D'Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119. Boyd JB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon. J Bone Joint Surg Am 1961;43:1041-1043. Morrey BF, Askew LJ, An KN, Dobyns JH: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418-421.
References:
- Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 82High Yield
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
Explanation
Explanation
2b 2c The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 83High Yield
A 50-year-old man with metastatic renal cell carcinoma has right hip pain. A radiograph and CT scan are shown in Figures 48a and 48b. The first step in management should consist of

Explanation
These lesions are extremely vascular and can cause uncontrolled intraoperative bleeding; therefore embolization is the appropriate first treatment. Because the radiograph and CT scan show a lytic lesion in the supra-acetabular region that affects the weight-bearing dome and medial wall, the next step in treatment would most likely be a total hip arthroplasty and acetabular reconstruction. Treatment with bisphosphonates and radiation therapy will not prevent an acetabular fracture. Cementoplasty is an emerging technique in which cement is injected percutaneously into a lesion, but no long-term results have been reported. Radiofrequency ablation of bone metastases is also an emerging technique that provides palliative pain control. Layalle I, Flandroy P, Trotteur G, Dondelinger RF: Arterial embolization of bone metastases: Is it worthwhile? J Belge Radiol 1998;81:223-225.
Question 84High Yield
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Explanation
The radiograph reveals a "bony mallet injury." As the distal phalanx is not volarly subluxated, extension splinting, similar to a classic mallet injury without bony involvement, is appropriate. If there is volar subluxation associated with a large bony fragment, surgical intervention is appropriate. Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Question 85High Yield
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of

Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 86High Yield
Which of the following is most commonly associated with an open clavicular fracture?
Explanation
Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 87High Yield
A 33-year-old woman sustains a C6 burst fracture diving into a swimming pool, resulting in a complete spinal cord injury. The canal compromise is shown in Figures 8a and 8b. Functional recovery would be maximized with
Explanation
Explanation
8b Although the patient has sustained a complete spinal cord injury, an anterior decompression, even performed late, can gain an additional level of root function. In the quadriplegic patient, this can mean the difference between dependent and independent function. Posterior procedures do not afford adequate access to the retropulsed bony fragments compromising the canal. Bohlman HH, Anderson PA: Anterior decompression and arthrodesis of the cervical spine: Long-term motor improvement. Part I: Improvement in incomplete traumatic quadriparesis. J Bone Joint Surg Am 1992;74:671-682.
References:
- Benz R, Abitbol JJ, Ozanne S, Garfin SR: Cervical burst fractures, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 300-330.
Question 88High Yield
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include
Explanation
Explanation
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures. Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780. Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362. Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
References:
- Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
Question 89High Yield
Figure 7 shows the AP radiograph of a 60-year-old man who has had pain in the thigh for past 6 months. History reveals that he underwent hip replacement 1 year ago. The radiographic changes are most likely the result of what process?
Explanation
Explanation
The arrows in the radiograph point to circumferential radiolucencies that strongly support the diagnosis of septic loosening. Radiolucent lines that occur in such a short time are also typical of an infection. Garvin KL, Hanssen AD: Infection after total hip arthroplasty: Past, present, and future. J Bone Joint Surg Am 1995;77:1576-1588.
References:
- Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 90High Yield
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
Anterior superior iliac spine avulsion fractures are caused by sudden, forceful contractions of the sartorius and tensor fascia lata. These injuries occur in young athletes through the growth plate with the hip extended and the knee flexed, such as while sprinting or swinging a baseball bat. The athlete will often report a pop or snap at the time of injury. Displaced fractures usually can be seen on radiographs. CT or MRI can be obtained to confirm the diagnosis. In most patients, nonsurgical management consisting of rest and protected weight bearing yields satisfactory outcomes. Surgery is usually reserved for fractures with displacement of more than 3 cm and painful nonunions. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 91High Yield
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of
Explanation
Explanation
Chronic dislocation of the patella is occasionally seen in patients with Down syndrome. In early childhood, patellar realignment may restore stability of the patellae. In later childhood, bony changes in the patellar groove interfere with stability, even if surgical realignment is performed. Realignment can also lead to increased knee pain postoperatively. In asymptomatic patients who are able to extend their knees, continued observation is the management of choice. Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
References:
- Mendez AA, Keret D, MacEwen GD: Treatment of patellofemoral instability in Down's syndrome. Clin Orthop 1988;234:148-158.
Question 92High Yield
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?
Explanation
Most humeral fractures will heal with nonsurgical functional brace management. When the initial pain has subsided in a coaptation splint, the patient is converted to a functional brace and allowed to use the arm for activities. The fracture should heal within 6 weeks to 12 weeks with acceptable results. Surgery is indicated if there is vascular injury, open injury, floating elbow, chest injury, bilateral humeral fractures, or if a reduction cannot be obtained or maintained. The surgical treatment of choice is either antegrade reamed locked intramedullary nailing or plate osteosynthesis. Plate osteosynthesis appears to offer better results with respect to union, function, and risk of complications. Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Question 93High Yield
When performing a gastrocnemius recession, what structure should be protected?
Explanation
Explanation
When performing a gastrocnemius slide at the tendinous portion of the gastrocnemius insertion, the sural nerve and saphenous vein, which tend to run midline posterior at this level, must be protected and retracted laterally. An anatomic study of the sural nerve at this level localized the nerve superficial to the deep fascia overlying the gastrocnemius in 42.5% of the cases; deep to the superficial fascia in 57.5% of the cases, and directly applied to the gastrocnemius tendon in 12.5% of cases. Pinney SJ, Sangeorzan BJ, Hanen ST Jr: Surgical anatomy of the gastrocnemius resection (Strayer procedure). Foot Ankle Int 2004;25:247-250.
Question 94High Yield
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?


Explanation
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint. Renoult B, Lataste A, Jonon B, et al: Sternoclavicular joint infection in hemodialysis patients. Nephron 1990;56:212-213.
Question 95High Yield
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
Explanation
22b The radiograph reveals either a fractured or bipartite sesamoid. The bone scan shows asymmetrically increased uptake over the medial sesamoid. Given the history and physical examination, a stress fracture is the most likely diagnosis. Medial sesamoidectomy reliably improves pain, and athletes return to sports on an average of 7 weeks after excision. Immobilization typically requires more than 4 to 8 weeks and is not always successful; however, it would be appropriate management for a patient who is not an elite athlete. Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
References:
- Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 96High Yield
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
Explanation
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker. Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270. Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
References:
- Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 97High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 98High Yield
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?
Explanation
Explanation
Several large clinical studies have shown that the most common problem after elastic nailing of a femoral shaft fracture is persistent pain and irritation at the nail insertion site. Unacceptable shortening and malunion are very rare in a 7-year-old patient. Rotational malalignment also is unusual. Osteonecrosis has been reported in solid antegrade nailing but not with elastic nailing of femoral shaft fractures in skeletally immature patients. Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777. Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
References:
- Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 99High Yield
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
Explanation
49b Lacerated radial nerves are associated with open humeral fractures. All open humeral fractures with radial nerve palsy should be managed with radial nerve exploration and skeletal stabilization. Closed humeral fractures with associated radial nerve palsy usually have an intact nerve with neurapraxia. Most of these patients recover without surgical treatment. If the patient has multiple injuries, skeletal stabilization may be indicated to improve mobilization. For an isolated closed humeral fracture with a radial nerve palsy, the treatment of choice is splinting for 1 to 2 weeks, followed by a humeral fracture brace. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
References:
- Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 100High Yield
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Explanation
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis. Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon