Orthopedic Board Review: Mock Exam Set 405 – 100 High-Yield MCQs
14 Apr 2026
105 min read
111 Views
Key Takeaway
This page offers 100 high-yield orthopedic board review questions designed to help surgeons master their ABOS, OITE, and FRCS exams. Our randomized multiple-choice questions (MCQs) cover essential concepts, providing a comprehensive practice test experience. Sharpen your knowledge and boost your confidence for precision outcomes.
Medial Approach Applied: Surgical Anatomy for...
00:00
Start Quiz
Question 1High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 2High Yield
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of
Explanation
Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation. Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
References:
- Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 3High Yield
Examination of a 30-year-old professional singer who has persistent neck and shoulder pain reveals a positive Hoffman's sign and clonus because of anterior C2-3 cord compression. The MRI scan shown in Figure 11a and the cervical CT scan shown in Figure 11b reveal focal anterior cord compression at the C2-3 level. Which of the following surgical approaches would least affect her professional career?
Explanation
Explanation
11b Protection of the superior laryngeal nerve is critical in a professional singer. The nerve is easily injured with retraction when using vertical extension of common anterior surgical approaches to gain exposure to the C2-3 level. McAfee and associates reported on 17 patients with C1-2 and C2-3 pathology. They used a modified submandibular approach as an anterior retropharyngeal exposure with modification of the superior extension of the Smith-Robinson technique that allows visualization of the superior laryngeal nerve and surrounding structures. No incidences of superior laryngeal nerve injury were recorded. The transoral approach should be avoided because of the high rate of infection and limited exposure. McAfee PC, Bohlman HH, Reilly LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surgery Am 1987;69:1371-1383.
References:
- Lu J, Ebraheim NA, Nadim Y, Huntoon M: Anterior approach to the cervical spine: Surgical anatomy. Orthopedics 2000;23:841-845.
Question 4High Yield
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
Explanation
18b 18c The MRI scans reveal an enlarged posterior tibial tendon, with degenerative signal within the tendon and an excessive amount of fluid in its sheath. This is a type II tear, as noted by Conti and associates, which is the most commonly seen tear. Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
References:
- Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 5High Yield
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
Explanation
Differentiating between a midfoot sprain and Lisfranc diastasis is critical in the management of the athlete with an acute injury to the midfoot. Greater than 2 mm of displacement between the first and second metatarsals on a weight-bearing radiograph is an indication for anatomic reduction with internal fixation of the tarsometatarsal joints. If no subluxation is noted, treatment should consist of a non-weight-bearing cast for 6 weeks, followed by a gradual return to activity. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
References:
- Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 6High Yield
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?


Explanation
The images show a lobulated, eccentric, well-marginated lesion that is typical of a nonossifying fibroma. The lesion is slightly expansile, and the CT scan findings show that the lesion is very well marginated and the cortex is disrupted, which is a common finding. None of the characteristics of this lesion is aggressive in nature. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 7High Yield
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
Explanation
44b 44c The treatment of choice for proximal pole scaphoid fractures is open reduction and internal fixation with a differential pitch screw via a dorsal approach. Healing rates of 100% have been reported for these acute fractures. Casting results in slow healing, with recommendations including 16 weeks or more in a cast. Vascularized bone grafts are not indicated for acute fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
References:
- Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 8High Yield
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?
Explanation
Explanation
The A2 and A4 pulleys are considered the most important parts of the pulley system. If these two structures are preserved, 80% of finger flexion can be maintained. If the pulley system is not left intact or is not reconstructed, "bow-stringing" of the flexor tendons occurs with loss of full flexion. The A2 pulley is over the proximal phalanx and the A4 pulley is over the middle phalanx. Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg Am 1988;13:473-484.
References:
- Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 9High Yield
According to the Third National Acute Spinal Cord Injury Study (NASCIS 3), what is the recommended protocol for a patient who sustained a spinal cord injury 7 hours ago?
Explanation
NASCIS 2 established the recommended doses of methylprednisolone for spinal cord injury. This included an initial bolus of 30 mg/kg over 1 hour, followed by an infusion of 5.4 mg/kg/h for an additional 23 hours. If the injury was more than 8 hours old, the methylprednisolone was not recommended. NASCIS 3 changed the dosing schedule based on the time from injury. If the time from injury to treatment was less than 3 hours, the standard protocol was followed (30 mg/kg bolus followed by 5.4 mg/kg/h for 23 hours). If the time from injury to treatment was between 3 and 8 hours, the infusion was continued at 5.4 mg/kg for an additional 23 hours (48 hours total). In this situation with a time of injury 7 hours ago, treatment should consist of a bolus and further steroid therapy for 48 hours. Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 10High Yield
A 30-year-old woman injured the ring finger of her nondominant hand while playing baseball 5 weeks ago. She now reports pain and limited motion of the proximal interphalangeal (PIP) joint. A lateral fluoroscopy image is shown in Figure 36. Treatment of the PIP joint should consist of
Explanation
Explanation
The patient has a neglected PIP joint fracture-dislocation with comminution involving more than 40% of the volar articular surface of the middle phalanx. Volar plate arthroplasty has been advocated for the treatment of acute unstable and chronic dorsal fracture-dislocations. The volar plate is incised laterally and released from the collateral ligaments. The volar fragments of the middle phalanx are removed and a trough is created for advancement of the volar plate, which is secured with sutures secured on the dorsum of the middle phalanx beneath the extensor mechanism. Dionysian E, Eaton RG: The long-term outcome of volar plate arthroplasty of the proximal interphalangeal joint. J Hand Surg Am 2000;25:429-437. Eaton RG, Malerich MM: Volar plate arthroplasty of the proximal interphalangeal joint: A review of ten years' experience. J Hand Surg Am 1980;5:260-268.
Question 11High Yield
What region of the thoracic curve is most dangerous for pedicle screw insertion while performing a posterior fusion for adolescent idiopathic scoliosis?
Explanation
Morphologic and anatomic studies confirm the pedicle is smaller on the concave side of thoracic curves. The dura is also closer to the pedicle on the concave side of the curves. Liljenqvist U, Allkemper T, Hackenberg L, et al: Analysis of vertebral morphology in idiopathic scoliosis with use of magnetic resonance imaging and multiplanar reconstruction. J Bone Joint Surg Am 2002;84:359-368.
Question 12High Yield
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Explanation
Explanation
15b 15c The MRI scans reveal a large posterior paralabral cyst associated with a posterior-superior labral tear. The cyst appears as a well-defined, smoothly marginated mass with low signal intensity on T1-weighted MRI scans and with high signal intensity on T2-weighted MRI scans. MRI also reveals changes in the supraspinatus and infraspinatus muscles secondary to denervation, including decreased muscle bulk and fatty infiltration. MRI has the added advantage, compared with other imaging modalities, of detecting intra-articular lesions, such as labral tears, which are frequently associated with ganglion cysts of the shoulder. In this case of a professional baseball player with a space-occupying lesion causing nerve compression with an associated labral tear, the treatment of choice is arthroscopic decompression of the cyst and repair of the tear. Acromioplasty would not address the primary pathology in this patient. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
References:
- Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 13High Yield
A 23-year-old man has pain and a callus beneath the second metatarsal head. Initial management should consist of
Explanation
The initial treatment of metatarsalgia with or without the presence of an intractable keratosis should be conservative. Simple paring of the callus with elevation of the metatarsals may suffice. A prefabricated "off-the-shelf" orthosis or felt pad can be used before investing in a custom orthosis. The use of medicated pads can lead to greater amounts of keratosis and should be avoided. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 163-173.
Question 14High Yield
A 74-year-old man reports progressive left hip pain with weight-bearing activities. A radiograph is shown in Figure 30. What is the most likely underlying diagnosis?
Explanation
Explanation
The radiograph shows enlargement of the bone, coarse trabeculation, a blastic appearance, and thickening of the cortex, revealing the classic appearance of Paget's disease in the sclerotic phase, the most common presentation. While lymphoma may present as a blastic lesion, it will not have the same enlargement, coarse trabeculation of bone, and the significant sclerosis seen here. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 211-215.
References:
- Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 1947-2000.
Question 15High Yield
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
The placement of ACL graft with respect to its femoral and tibial attachments has a significant effect on its function. Evidence has shown that if the graft is placed in the over-the-top position, the graft will become lax in flexion and more taut with extension. Conversely, if the graft is placed too anterior on the femoral side, it will tighten in flexion and become lax in extension. Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342. Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Question 16High Yield
A 54-year-old man undergoes uneventful anterior cervical diskectomy and interbody fusion at C4-5 for focal disk herniation and C5 radiculopathy. At the 3-week follow-up examination, the patient reports a persistent cough. Pulmonary evaluation reveals a mild but persistent aspiration. Laryngoscopy reveals partial paralysis of the left vocal cord, most likely caused by
Explanation
Explanation
The exact anatomic event responsible for vocal cord paralysis associated with anterior cervical surgery remains a question. Apfelbaum and associates, in an excellent review of 900 anterior cervical surgeries, identified 30 patients with vocal cord paralysis, 3 of which were permanent. They showed that retractors placed under the longus coli for anterior cervical exposures can compress the laryngeal-tracheal branches within the larynx against the tented endotracheal tube rather than the recurrent laryngeal nerve, which is extrinsic to the larynx. By releasing the endotracheal cuff and allowing the tube to recenter itself after placement of the retractors, they were able to decrease vocal cord injury from 6.4% to 1.7%. Jewett and associates suggested that a left-sided approach may result in a lower incidence of injury. Endotracheal intubation is the second most common cause of vocal cord injury, with an incidence of approximately 2%. Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve paralysis during anterior cervical spine surgery. Spine 2000;25:2906-2912.
References:
- Jewett BA, Menico GA, Spengler DM, Coleman SC, Netterville JL: Vocal Cord Paralysis Following Anterior Cervical Spine Surgery. Paper presented at the annual meeting or the Cervical Spine Research Society, December 2000, Charleston SC, Paper #7.
Question 17High Yield
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm3. Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of
Explanation
Explanation
This clinical situation requires careful analysis because some data suggest infection and some a noninfectious inflammatory process. Bilateral hip involvement, the absence of significant fluid collection or fever, the streptozyme level, and the history of upper respiratory infection all suggest poststreptococcal toxic synovitis as the most likely cause for the clinical presentation. In the first 24 hours, this type of presentation might warrant incision and drainage given uncertainty of the diagnosis and the risks associated with missing an infection. However, 5 days after onset, surgery is not warranted, especially given that the patient remains afebrile and her symptoms are improving. Cardiology consultation would be appropriate. There is no evidence to suggest slipped capital femoral epiphysis. Treatment with antibiotics is not advised because there is no bacteriologic data on which to base treatment. De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
References:
- Haueisen DC, Weiner DS, Weiner SD: The characterization of "transient synovitis of the hip" in children. J Pediatr Orthop 1986;6:11-17.
Question 18High Yield
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus?
Explanation
Explanation
Clavicular fractures are occasionally complicated by injury to the brachial plexus. A displaced bone fragment pressing on the posterior cord proximal to the upper subscapularis nerve would account for these findings. Jobe CM, Coen MJ: Gross anatomy of the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
References:
- Barbier O, Malghem J, Delaere O, et al: Injury to the brachial plexus by a fragment of bone after fracture of the clavicle. J Bone Joint Surg Br 1997;79:534-536.
Question 19High Yield
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
Explanation
54b 54c The Merchant radiograph shows a lateral patellar shift with total polyethylene failure, resulting in a metal-on-metal bearing. This problem is associated with metal-backed patellar components. Component fixation appears solid, and no osteolysis is evident. Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593. Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
References:
- Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 20High Yield
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Explanation
Ceramic-on-ceramic bearing surfaces have superior tribological properties and show lower linear wear than metal-on-metal implants. However, because of their lower strength and vulnerability to fracture, design considerations constrain the neck-length options available to ensure optimal taper fit.
Question 21High Yield
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Long-term survivorship studies have attempted to clarify patient factors related to good outcomes in HTO. One particular study showed that a patient age of less than 50 years was related to good outcomes in those who had good preoperative knee flexion. The same study found no relation between HTO failure and the presence of postoperative infection or deep venous thrombosis. The presence of a lateral tibial thrust is a contraindication to performing this surgery. As expected, good patient selection is critical to obtaining good long-term results with HTO. Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 22High Yield
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
Laminectomy is associated with the highest risk of iatrogenic paraplegia because retraction on the cord is necessary for visualization, but retraction is difficult because of tethering of the intradural dentate ligaments. All of the other approaches allow for access to the disk herniation through an angle that avoids the cord itself, although other limitations may exist. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Question 23High Yield
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of

Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 24High Yield
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
In a recent study on restoration of motion following zone I and zone II flexor tendon repairs in children, age was found to have no effect on the results of zone II tendon repairs. Early passive motion offered no better results than immobilization for 3 weeks. Immobilization for more than 4 weeks correlated with poorer results.
Question 25High Yield
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
The tibiofibular overlap is measured between the medial border of the fibula and the lateral border of the anterior tibial tubercle. Plain radiographic assessment of the distal tibiofibular syndesmosis requires AP and mortise views. The following criteria have been used as the normal limits in adults: a talocrural angle of + or - 83 degrees with up to 5 degrees of normal difference between both sides, a medial clear space of less than 4 mm, a talar tilt of less than 2 mm, a tibiofibular clear space of less than 5 mm, a tibiofibular overlap of greater than or equal to 0 mm, and a talar subluxation that is a subjective assessment of congruity of the tibial articular surface and the talar dome; any incongruity is abnormal. It has been recommended to obtain the first three measurements on the mortise view and the other three on the AP view. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 26High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature. Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233. Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526. Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
References:
- Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 27High Yield
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
Explanation
The radiograph shows a type V acromioclavicular joint injury. Type V injuries involve disruption of the acromioclavicular and coracoclavicular ligaments. Type I injuries involve a sprain of the acromioclavicular joint ligaments. Type II injuries involve disruption of the acromioclavicular joint ligaments; the coracoclavicular ligaments are partially injured. Sternoclavicular ligaments stabilize the medial clavicle and the sternum; they are not damaged with acromioclavicular joint dislocations. Fukuda K, Craig EV, An KN, et al: Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 1986;68:434-439.
References:
- Bosworth B: Complete acromioclavicular dislocation. N Engl J Med 1949;241:221-225.
Question 28High Yield
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 29High Yield
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?
Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time of less than 6 hours. Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Question 30High Yield
A patient with a 5-cm synovial sarcoma located in the distal portion of the rectus femoris muscle undergoes excision of the mass. The procedure is performed through a 10-cm longitudinal incision. Only a portion of the rectus femoris is removed; the vast majority of the muscle is preserved. The plane of dissection is beyond the reactive zone, and the pathology reveals that the margins are negative. This procedure is classified as
Explanation
Explanation
The patient underwent a wide resection, which involves excision of the tumor along with a cuff of normal tissue that completely surrounds the tumor. The plane of resection is beyond the reactive zone. A radical resection involves removal of the entire affected muscle from origin to insertion. In a marginal excision, the plane of dissection is through the reactive zone of the tumor. A marginal excision is generally considered inadequate surgery for high-grade sarcomas. In an intralesional resection, the plane of dissection is through the tumor. Excision within the reactive zone but beyond the tumor is the same as a marginal excision. Enneking WF: Staging of musculoskeletal neoplasms, in Current Concepts of Diagnosis and Treatment of Bone and Soft Tissue Tumors. Heidelberg, Germany, Springer-Verlag, 1984.
References:
- Simon MA, Springfield D: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998.
Question 31High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 32High Yield
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
Explanation
Ecchymosis on the medial side of the ankle is distributed in the posterior tibialis tendon sheath location, posterior to the medial malleolus, and extending inferiorly to the tendon's attachment on the navicular. MRI is the imaging study of choice to determine the extent of tendon damage. MRI will also help assess the deltoid ligament. Bone scans and CT are helpful in identifying osteochondral fractures and occult fractures; however, these studies are not indicated for this patient. Peroneal tendons are located lateral on the ankle. Arthroscopy of the ankle joint would not be helpful in assessing the posterior tibial tendons. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 307-317.
References:
- Rosenberg ZS, Cheung Y, Jahss MH, Noto AM, Norman A, Leeds NE: Rupture of the posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 1988;169:229-235.
Question 33High Yield
For halo traction, what is the preferred site for anterior pin placement?
Explanation
The safe zone for anterior halo pin insertion is marked laterally by the anterior border of the temporalis muscle (to avoid penetration of this muscle and relative thin cortex of the skull). Medially, the pin should be placed 4.5 cm lateral to the midline to avoid injury to the supraorbital nerve or the frontal sinus. The safe area is marked superiorly by the head equator to avoid cephalad migration of the pin and inferiorly by the supraorbital ridge to prevent displacement or penetration into the orbit.
Question 34High Yield
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of
Explanation
Explanation
As long as the patient is alert and cooperative, an attempt can be made to reduce the dislocation. This should not be attempted in a patient who is obtunded, comatose, or uncooperative. If any neurologic changes are noted during the reduction maneuver, the attempt should be stopped, appropriate radiographic studies obtained, and open reduction and stabilization planned in the operating room.
References:
- Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case reports. J Bone Joint Surg Am 1991;73:1555-1560.
Question 35High Yield
A 29-year-old woman reports shoulder pain after sustaining a minor fall 6 weeks ago. She has a history of celiac sprue. Radiographs of the forearm and shoulder are shown in Figures 53a and 53b. Which of the following serum abnormalities would be expected?
Explanation
Explanation
53b Celiac sprue results in rapid gastrointestinal transit and fatty stools that impair the absorption of calcium and vitamin D and result in nutritional-deficiency osteomalacia with secondary hyperparathyroidism. The radiographs show marked osteopenia with brown tumors. A pathologic fracture is seen in the proximal humerus through a large brown tumor. Serum findings include low or normal calcium, low phosphate, elevated alkaline phosphatase, low 1,25(OH)2D, and increased PTH levels. Secondary hyperparathyroidism is associated with a variety of conditions including malabsorption syndromes. Potts JT: Parathyroid hormone: Past and present. J Endocrinol 2005;187:311-325. Corazza GR, Di Stefano M, Maurino E, et al: Bones in coeliac disease: Diagnosis and treatment. Best Pract Res Clin Gastroenterol 2005;19:453-465.
References:
- Mankin HJ, Mankin CJ: Metabolic bone disease: An update. Instr Course Lect 2003;52:769-784.
Question 36High Yield
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
Explanation
A facet dislocation that cannot be reduced in an alert, awake patient with some preservation of cord function requires MRI to evaluate the disk prior to a reduction under anesthesia. The presence or absence of a disk herniation must be assessed, as this factor may influence the method of reduction. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262. Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
References:
- Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 37High Yield
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
References:
- Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.
Question 38High Yield
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
Explanation
Explanation
20b 20c 20d 20e The radiographic findings are classic for synovial chondromatosis because of the small calcified opacities within the joint surrounding the synovium. The histologic findings show cartilaginous foci of metaplasia, which may be markedly cellular. However, unlike low-grade chondrosarcoma, it lacks cellular and nuclear pleomorphism. Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
References:
- Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 39High Yield
When planning revision of a total hip arthroplasty where an acetabular reconstruction will be required, what prerequisite is important to ensure long-term success of a cementless component?
Explanation
In bone defects where host bone support is less than 50%, the failure rate is 70% at 5.1 years. The presence or absence of columns or hip position is of relatively little importance if the supportive bone is not present in at least 50% of the surface area around the future acetabular implant.
Question 40High Yield
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include
Explanation
Explanation
57b 57c This is a classic bilateral facet dislocation. When there is no evidence of a disk herniation, treatment should include careful skeletal traction, closed reduction, and posterior fusion. There is no role for anterior procedures. These fractures are unstable and require surgical intervention. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.
Question 41High Yield
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Explanation
Explanation
If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson's fracture. Patients with this type of injury usually require fusion. Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
References:
- Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 42High Yield
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 43High Yield
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the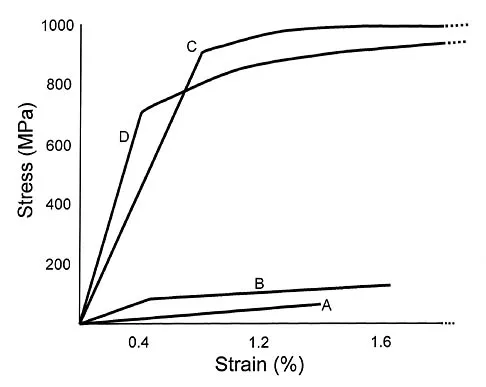
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Question 44High Yield
Bioabsorbable polymers are used in a wide range of orthopaedic devices, including anchors, staples, pins, plates, and screws. What is the primary drawback for bioabsorbable implants?
Explanation
A number of bioabsorbable polymers are used in orthopaedic applications, and all have in common reports of foreign body reactions, which occur in more than 50% of patients in some series. In general, the high cost of these polymers is offset by the elimination of a second surgery to remove the implant. Bioabsorbable polymers are low strength in comparison to metallic alloys but of sufficient strength for many orthopaedic applications. The elastic modulus is not as high as many other orthopaedic biomaterials, making them suitable for applications where lower stiffness is an asset. Ambrose CG, Clanton TO: Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-177.
Question 45High Yield
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 46High Yield
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Question 47High Yield
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
Ankle arthrodesis for posttraumatic ankle arthrosis provides reliable pain relief. However, the long-term sequela of joint arthrodesis is the development of arthrosis in the surrounding joints. Over time, following ankle arthrodesis, the ipsilateral hindfoot and midfoot joints show signs of joint space wear, and this may be symptomatic. With a stable ankle arthrodesis, progressive limb-length discrepancy or talar osteonecrosis is not expected. Ankle arthrodesis has not been definitively linked to ipsilateral knee arthritis or contralateral ankle arthritis. Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 48High Yield
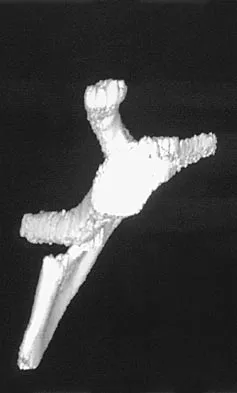
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of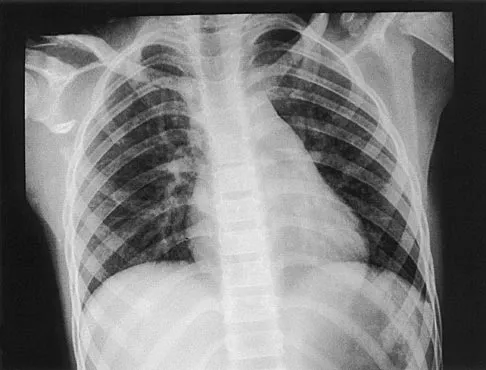


Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 49High Yield
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of

Explanation
In a patient with known metastatic disease, the surgeon must rule out additional lesions throughout the femur prior to surgical management. Lesions located in the diaphysis or in the peritrochanteric region may influence the surgical procedure. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 50High Yield
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?


Explanation
Malignant fibrous histiocytoma (MFH) is the most common soft-tissue sarcoma. MFH typically presents as a large mass, deep to the fascia with heterogeneous signal on MRI. The MRI scans show a heterogeneous lesion in the posterior thigh. There is significant high signal uptake on the T2-weighted image. The histology shows malignant histiocytic cells with marked atypia and pleomorphism. Histology of a hematoma would show only old hemorrhage and some granulation tissue. Lipoma and liposarcoma are both seen as a fat-containing lesion on histology. No significant fat tissue is seen in this histologic specimen. Histology of myositis ossificans would show bone formation. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 51High Yield
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of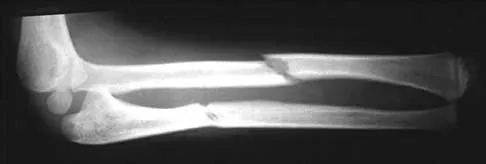
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 52High Yield
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the
Explanation
Explanation
From birth until the age of 4 years, the primary blood supply to the femoral head is from the medial and lateral circumflex arteries that traverse the femoral neck. After the age of 4 years, the contribution of the lateral femoral circumflex artery, which traverses the anterior portion of the femoral neck, becomes negligible. The posterosuperior and posteroinferior retinacular vessels, branches of the medial femoral circumflex artery, become the primary blood supply to the epiphysis. The contribution of the artery of the ligamentum teres is minimal after the age of 4 years. Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
References:
- Ogden JA: Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am 1974;56:941-950.
Question 53High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
References:
- Fritz RL, Perrin DH: Cold exposure injuries: Prevention and treatment. Clin Sports Med 1989;8:111-128.
Question 54High Yield
What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon's canal seen in Figure 17?
Explanation
Explanation
The lesion lies in zone II of the ulnar tunnel. In that zone the deep motor branch of the ulnar nerve is susceptible to compression. Distal to the hook of the hamate, the motor branch of the ulnar nerve dives deep to innervate the interossei as it begins to move from an ulnar to radial direction. Because of its course, it has little or no give in response to a mass effect from the floor of Guyon's canal. Ganglions are the most common cause of ulnar nerve entrapment in the wrist. Lesions in zone I can affect both sensory and motor aspects of the ulnar nerve as well as the motor innervation of the hypothenar muscles. Lesions at the elbow or mid-to-proximal forearm are associated with dorsal hand numbness and tingling. Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.
References:
- Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Question 55High Yield
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
Because the patient has significant arthritis, arthrodesis is the treatment of choice. Adding a bone graft will prevent further shortening and add length to her toe, resulting in improved cosmesis. A cheilectomy will not alleviate her arthritis pain. The toe is too short for an effective Moberg phalangeal dorsiflexion osteotomy. A Waterman first metatarsal dorsal osteotomy will not address the degenerative joint disease or shortening. Silastic arthroplasty may help, but there is the risk of additional problems with foreign body reaction and a significant risk of failure known to occur with Silastic materials. Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Question 56High Yield
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Explanation
Explanation
The radiograph shows a fabella, a sesamoid bone that is usually found within the tendon of the lateral head of the gastrocnemius. It can be confused with a loose body on radiographs. It occurs in 18% of patients and is often bilateral. Anderson JE (ed): Grant's Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, pp 4-69.
References:
- Weissman BNW, Sledge CB (ed): Orthopaedic Radiology. Philadelphia, PA, WB Saunders, 1986, p 514.
Question 57High Yield
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
The compaction of FDBA is faster than that of fresh-frozen bone. The maximal stiffness reached by both materials when tested was the same (55 MPa), but the FDBA required fewer impactions to achieve that stiffness. Because it is easier to impact, the FDBA may be mechanically more efficient than the fresh-frozen bone in surgical conditions. The brittleness of irradiated FDBA, caused by loss of the capacity to absorb energy in a plastic way, increases the compactness and stiffness of morcellized grafts. The failure rate of fusion in adolescent idiopathic scoliosis has been shown to be much higher in FDBA than in either iliac crest bone graft or composite autograft with demineralized bone matrix. There is a greater erosive surface response to allograft when compared to autograft or frozen allograft, with a larger number of osteoclast and osteoblast nuclei seen microscopically. Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand 2004;75:309-314. Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Question 58High Yield
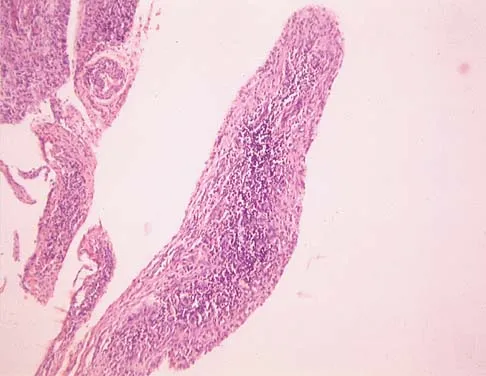
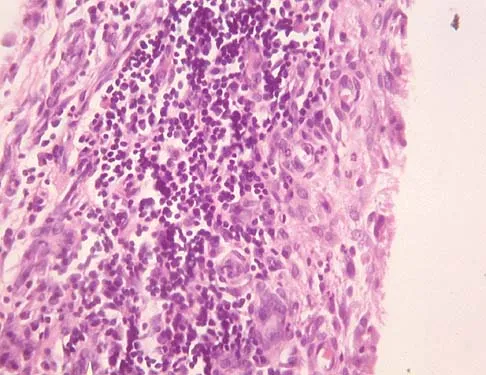
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?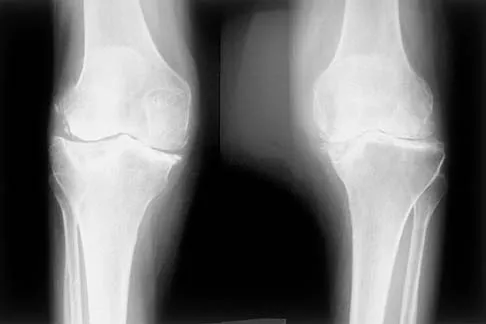
Explanation
Rheumatoid arthritis is an inflammatory arthritis that usually involves multiple joints. Radiologic findings of periarticular erosion, osteopenia, and minimal osteophyte formation favor rheumatoid arthritis over osteoarthritis. Pigmented villonodular synovitis and Charcot arthropathy are more often considered monoarticular diseases. There are no radiographic findings of Paget's disease.
Question 59High Yield
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 60High Yield
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
Explanation
The patient has a bipartite patella. The line between the fragment and the main patella is smooth and sclerotic, indicating a chronic, not acute, entity. The location is classic for a bipartite patella, not a tumor. Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
References:
- Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
Question 61High Yield
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
Explanation
The stretching of the graft occurs over time as the graft is loaded. Time-dependent deformation under load is called creep and is common in viscoelastic materials such as ligament tissue. Creep can occur under both static and cyclic load conditions; time-dependent deformation will occur as long as load is applied to the tissue. Similarly, when a graft is initially tensioned to a given deformation at surgery, the load generated in the graft will decrease over time; this behavior is called stress relaxation and also is indicative of a viscoelastic material. Water content may affect the viscoelastic properties by changing the friction between collagen fibers, but studies have shown little difference in water content between grafts and normal ligaments. Fatigue failures may manifest themselves through damage to the ligament tissue, but this would require higher loads than are routinely experienced by grafts. Elastic stretch is recoverable and, therefore, does not contribute to a permanent stretch. Similarly, gross failure at the attachment would not cause a stretch, but rather a catastrophic instantaneous instability. Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
References:
- Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O'Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 62High Yield
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of
Explanation
Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
References:
- Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 63High Yield
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
Explanation
Explanation
This is an example of a missed deep posterior compartment syndrome that typically presents 6 months after the injury with progressive clawing due to necrosis, scarring, and contracture of the posterior tibial tendon, flexor digitorum longus, and flexor hallucis longus. Treatment consists of debridement of necrotic muscle and scar tissue with corresponding tendon excision. After debridement and posterior capsule release, if the equinus is relieved with knee flexion, a gastrocnemius slide may be performed. Otherwise, the lengthening should be at the level of the Achilles tendon. Bracing will not address the claw toes. Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213. Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.
Question 64High Yield
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a "pencil in cup" distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?
Explanation
The patient's clinical picture is considered the classic presentation for psoriatic arthritis. The other answers are not applicable for the constellation of findings. Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1691-1693.
Question 65High Yield
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?
Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 66High Yield
A 3-year-old boy had been treated with serial casting for a right congenital idiopathic clubfoot deformity. The parents are concerned because the child now walks on the lateral border of the right foot. Examination shows that the foot passively achieves a plantigrade position with neutral heel valgus and ankle dorsiflexion to 15 degrees. The forefoot inverts during active ankle dorsiflexion. Mild residual metatarsus adductus is present. Management should now consist of
Explanation
Explanation
Dynamic midfoot supination that is the result of peroneal weakness is a common residual problem after cast correction or surgical reconstruction of a congenital idiopathic clubfoot. Dynamic supination is unlikely to resolve spontaneously. Most parents do not want to use brace support forever. Transfer of the posterior tibialis to the dorsum of the foot has shown poor results in clubfeet. Preferred treatments include: 1) transfer of the entire anterior tibialis tendon to the lateral cuneiform, or 2) split transfer of the anterior tibialis tendon to the cuboid or to the peroneus brevis tendon. Kuo KN, Hennigan SP, Hastings ME: Anterior tibial tendon transfer in residual dynamic clubfoot deformity. J Pediatr Orthop 2001;21:35-41. Garceau GJ: Anterior tibial tendon transfer for recurrent clubfoot. Clin Orthop 1972;84:61-65.
References:
- Miller GM, Hsu JD, Hoffer MM, et al: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 67High Yield
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
Explanation
The spleen is the most common organ injured in the abdomen as the result of blunt trauma. It is also the most common cause of death because of an abdominal injury. The liver is the second most commonly injured organ. Injury to the other organs is rare. The diagnosis can be made with CT. Treatment ranges from observation to splenectomy, depending on the severity of injury. Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
References:
- Kibler WB (ed): ACSM's Handbook for Team Physician. Philadelphia, PA, Williams & Wilkins, 1996, p 151.
Question 68High Yield
A Trendelenburg gait is most likely to be seen in association with
Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 69High Yield
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?

Explanation
Because the patient has chronic pain, a possible lateral recess stenosis of the C7 root, and no neurologic deficits, keyhole foraminotomy is the treatment of choice for decompressing the exiting nerve root and offering an early return to play, especially when using a muscle-splitting posterior approach. Henderson and associates reported excellent results with posterolateral foraminotomy in patients with radicular symptoms. Although anterior cervical diskectomy and fusion is equally effective in the long term, a period of 6 to 12 weeks is required to allow the anterior fusion to heal prior to a return to play. Chen and associates reported that keyhole foraminotomy maintains cervical motion segment dynamics better than compared to anterior limited diskectomy and foraminotomy or anterior diskectomy with fusion. Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512. Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Question 70High Yield
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90 degrees, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of
Explanation
Explanation
Hemihypertrophy or hemihypotrophy is usually idiopathic, and either the leg or the entire side of the body may be involved. In the infant or young child, it is often difficult to determine which side is abnormal if the condition is mild. Because of the association of Wilms' tumor with hemihypertrophy, these patients should undergo a yearly renal ultrasound until at least age 5 years. Other conditions that may exhibit hemihypertrophy include Klippel-Trenaunay-Weber syndrome, Proteus syndrome, and neurofibromatosis. In this patient, the mild hemihypertrophy is idiopathic. Because of the normal spinal examination and absence of neurologic findings, an MRI scan is unnecessary. The absence of clinical and radiographic evidence of hip dysplasia makes both an ultrasound of the hips and application of a Pavlik harness unnecessary. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193. Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
References:
- Beals RK: Hemihypertrophy and hemihypotrophy. Clin Orthop 1982;166:199-203.
Question 71High Yield
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
Explanation
Animal studies assessing the influence of fibrin glue supplementation have detected a markedly greater inflammatory response at the site of application. An increased incidence of infection and delays in healing were not noted. Cain JE Jr, Rosenthal HG, Broom MJ, Jauch EC, Borek DA, Jacobs RR: Quantification of leakage pressures after durotomy repairs in the canine. Spine 1990;15:969-970.
References:
- Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Question 72High Yield
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they
Explanation
The patient has sacral agenesis. Clinical signs include the classic dimpling over the buttocks and the characteristic lower extremity deformities. Imperforate anus is often associated with this disorder. Although motor function correlates with the level of vertebral defect, sensation is usually intact. This is important therapeutically, because patients are not as prone to pressure sores as are those with myelodysplasia. Kyphosis may develop in many patients with lumbosacral agenesis, but lordosis is unusual. Latex allergy and progressive neural deterioration may occur in patients with either myelodysplasia or sacral agenesis but is more common in the former.
Question 73High Yield
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
Explanation
Paucytopenia is a common problem in patients with metastatic disease. Causes include chemotherapy, external beam radiation, marrow replacement by tumor, and anemia of chronic disease. There is no correlation with decreased calcium and a decrease in hematopoiesis. Supportive care with granulocyte-colony stimulating factor (G-CSF) and neupogen can stimulate hematopoiesis.
References:
- Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 74High Yield
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?
Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 75High Yield
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Symptoms of activity-related low back pain, physical findings of pain with extension, lateral bending, and resuming an upright position, and relative hamstring tightness are consistent with spondylolysis. While the initial diagnostic work-up should include plain radiographs of the lumbosacral spine, the findings may be negative because it can take weeks or months for the characteristic changes to become apparent. SPECT has been a useful adjunct in the diagnosis of spondylolysis when plain radiographs are negative. Since the patient's pain is activity related and she is otherwise healthy, evaluation for infection is not indicated. Because the neurologic examination is normal, electromyography, nerve conduction velocity studies, and MRI are not indicated. CT can be used in those instances in which SPECT and bone scans are negative. Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110. Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211. Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Question 76High Yield
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
Explanation
The most frequently described entrapment of the deep peroneal nerve is the anterior tarsal tunnel syndrome. This syndrome refers to entrapment of the deep peroneal nerve under the inferior extensor retinaculum. Entrapment can also occur as the nerve passes under the tendon of the extensor hallucis brevis. Compression by underlying dorsal osteophytes of the talonavicular joint and an os intermetatarseum (between the bases of the first and second metatarsals) have previously been described in runners. Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
References:
- Schon LC, Mann RA: Diseases of the nerves, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 1, pp 675-677.
Question 77High Yield
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?
Explanation
The resultant spasticity and weakness (paresis) following a cerebrovascular accident leads to muscle imbalance that commonly results in contracture of the shoulder in adduction, internal rotation, and varying degrees of forward flexion. In addition, the elbow is usually flexed and the forearm pronated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 78High Yield
Which of the following muscle tendons inserts just lateral to the long head of biceps tendon on the proximal humerus?
Explanation
The pectoralis major insertion is just lateral to the long head of the biceps tendon. Medial to the biceps is the insertion for the teres major and latissimus dorsi. The short head of the biceps originates on the coracoid process. The subscapularis inserts on the lesser tuberosity just medial to the biceps.
Question 79High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to
Explanation
Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
References:
- Stasikelis PJ, Sullivan CM, Philips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155.
Question 80High Yield
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
Explanation
The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Question 81High Yield
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?
Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 82High Yield
A 25-year-old man has chronic back pain that has been slowly worsening. He has no constitutional symptoms, and he denies any previous medical problems. Examination shows a tall lean build with no objective neurologic findings or skin lesions. Figure 32 shows a T2-weighted sagittal MRI scan. What is the most likely diagnosis?
Explanation
The MRI scan shows significant dural ectasia, which is seen in more than 60% of patients with Marfan syndrome. It is also relatively common in patients with neurofibromatosis, but this patient has no skin lesions. It has also been described in Ehlers-Danlos syndrome but is less common. Ahn NU, Sponseller PD, Ahn UM, Nallamshetty L, Kuszyk BS, Zinreich SJ: Dural ectasia is associated with back pain in Marfan' syndrome. Spine 2000;25:1562-1568.
Question 83High Yield
Which of the following best characterizes bone mineralization?
Explanation
Mineralization occurs at the site of hole zones between the collagen fibrils. Crystals begin from the necessary ions of the lattice that come together with the correct orientation to form the first stable crystal. Formation of this critical nucleus is the most energy-demanding step of crystallization. Enzymes within the extracellular matrix vesicles degrade inhibitors such as adenosine triphosphate, pyrophosphate, and proteoglycans found in the surrounding extracellular matrix. Bone mineral consists of numerous impurities (carbonate, magnesium) that are more soluble, allowing the bone to act as a reservoir for calcium, phosphate, and magnesium ions. Crystals may form by addition of ions or ion clusters to the critical nucleus in many directions, with 'kink' sites forming to branch and exponentially proliferate the crystals. Macromolecules facilitate formation of the critical nucleus and increasing local concentrations of necessary ions. Once the crystals are formed and proliferating, macromolecules bind to the surface and block the growth of the crystal, regulating size, shape, and number of crystals. Lian JB, Stein GS, Canalis E, et al: Bone formation: Osteoblast lineage cells, growth factors, matrix proteins, and the mineralization process, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 14-29.
Question 84High Yield
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of
Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 85High Yield
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include
Explanation
The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure. Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238. Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 86High Yield
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
Explanation
A common side effect of interscalene nerve block for shoulder surgery is the blockade of the ipsilateral phrenic nerve. This, in turn, results in paresis of the diaphragm and up to a 30% reduction in pulmonary function volumes. Therefore, interscalene nerve block generally is not recommended for patients whose respiratory function is compromised. Other relative and absolute contraindications for interscalene nerve blocks include allergy to local anesthetics, infection at the injection site, uncontrolled seizure disorder, coagulation abnormality, and preexisting neurologic injury. Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.
References:
- Misamore GW, Sallay PI: A prospective analysis of the safety and efficacy of interscalene brachial plexus block anesthesia for shoulder surgery. J Shoulder Elbow Surg 2007;16:e39.
Question 87High Yield
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
Explanation
Metastatic lesions to bone are usually located in the axial and proximal appendicular skeleton. Metastases below the elbow and knee are rare, but when they do occur they are most commonly from lung carcinoma. Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
References:
- Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 88High Yield
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be

Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 89High Yield
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?
Explanation
Explanation
The MRI scan shows disruption of the subscapularis muscle. Subscapularis rupture is associated with weakness in internal rotation as shown with a positive lift-off test as described by Gerber and Krushell. The belly press test also has been shown to be a useful clinical test for this problem. Weakness in external rotation and abduction is more consistent with supraspinatus and infraspinatus tears. Deltoid atrophy is associated with an axillary nerve injury. Loss of biceps contour is associated with rupture of the long head of the biceps. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Greis PE, Kuhn JE, Schultheis J, et al: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 90High Yield
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?
Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 91High Yield
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
Explanation
A herniated cervical disk at C5-6 causes a C6 radiculopathy. There are eight cervical nerve roots and seven cervical vertebrae, and C8 exits between the C7 and T1 vertebrae. The C6 nerve root typically innervates the biceps and wrist extensor. The deltoid is predominantly innervated by C5. The wrist flexor and triceps are predominantly innervated by C7. Grip strength is predominantly a function of C8.
References:
- Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 92High Yield
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
The most common cause of recurrent dislocation following total hip arthroplasty continues to be component malposition. Component malposition should be addressed prior to any other treatment options, such as increasing soft-tissue tension with increased femoral offset or greater trochanteric advancement. A larger femoral head size may help, but correcting the component malposition should give more predictable results. A retroverted acetabular component should be revised to 15 degrees to 20 degrees of anteversion, matching the patient's anatomy with an abduction angle close to 45 degrees. Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343. Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Question 93High Yield
Which of the following is considered a major characteristic of hyaluronate?
Explanation
Hyaluronate is a naturally occurring compound that is the backbone of the central core of the proteoglycan aggregate. Cartilage is made of two principal tissue structures. The connective tissue component includes collagen, which forms the framework for structural strength and elasticity. The proteoglycan aggregate provides a unique property of water incorporation and friction reduction capabilities. Hyaluronate forms the base or central core of the aggregate on which a link protein binds a protein core. Chondroitin sulfate and keratin sulfate are then bound to this protein core, forming the terminal extension of the aggregate. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78. Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Question 94High Yield
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
On T1-weighted images, the posterior cruciate ligament is a low-signal (black) structure that courses from the posterior aspect of the tibia to the medial femoral condyle. The posterior cruciate ligament can appear as arcuate, U-shaped, or kinked. The other structures have similar signal but different anatomic locations. Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Question 95High Yield
A 36-year-old man has a moderate-sized left paracentral L5-S1 disk herniation with compression of the S1 nerve. Examination will most likely reveal sensory changes at what location?
Explanation
Explanation
Because the left paracentral L5-S1 disk herniation is compressing the left S1 nerve root, the patient will have numbness along the lateral border and plantar surface of the foot. Numbness along the anterior thigh stopping at the knee is consistent with an L3 radiculopathy. Sensory changes at the dorsum of the foot and great toe normally signify an L5 distribution; the medial leg signifies an L4 distribution. Perianal numbness involves the S2-S5 nerve roots. Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman and Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, vol 1, pp 629-634.
References:
- Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton- Century-Crofts, 1976, pp 249-254.
Question 96High Yield
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of

Explanation
Because the patient has clinical and radiographic signs of AC arthritis and subacromial impingement, the treatment of choice is anterior acromioplasty and distal clavicle excision. Arthroscopic acromioplasty alone would not address the AC arthritis. The rotator cuff is intact; therefore, rotator cuff repair is not indicated. An open Mumford procedure would address the AC arthritis only and not the impingement symptoms. Immobilization might lead to stiffness of the shoulder and is not recommended for treating impingement.
Question 97High Yield
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
Explanation
Following any closed fracture, the most important determinant for the timing of surgery is the condition of the soft tissues and especially the skin. The best determinant of appropriate soft-tissue condition is the presence of wrinkling of the skin (wrinkle sign) at the site of the incision. A wrinkle sign is present when all the interstitial edema has left the skin; this may take up to 14 to 21 days of elevation. Any abrasion must be epithelialized so that there are no bacteria left at the site. To date, no other method of soft-tissue viability measurement has been shown to be of any clinical benefit. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
References:
- Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 98High Yield
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 99High Yield
What is the most frequent complication following primary total hip arthroplasty?
Explanation
Thromboembolic disease can occur in up to 58% of unprotected patients and up to 20% of protected patients depending on the type of prophylaxis used, even though most thrombi are small and have little clinical consequence. The primary goal of prophylaxis is to prevent symptomatic deep venous thrombosis and fatal pulmonary emboli. Dislocation has been reported in up to 10% of primary cases, but generally acceptable rates of less than 5% are the norm. Component loosening following primary total hip arthroplasty is rare prior to a 10-year follow-up, and 90% to 95% of patients should reach the 10-year follow-up without the need for revision for any reason. Metal hypersensitivity is unusual, and nickel found in cobalt-chromium alloys is the most common offending agent. Infection of primary total hip arthroplasty is less than 1%. Eftekhar N: Total Hip Arthroplasty. St Louis, MO, Mosby,1993, pp 1445-1676.
Question 100High Yield
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Explanation
Most closed simple dislocations are best managed with early range of motion. Posterior dislocation typically occurs through a posterolateral rotatory mechanism. When placed in pronation, the elbow has greater stability when the medial ligamentous structures are intact. In traumatic dislocations, MRI rarely provides additional information that will affect treatment. In elbows that remain unstable, primary repair is preferred over ligament reconstruction. Cast immobilization increases the risk of arthrofibrosis.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon