Orthopedic Board Exam Set 787: 100 High-Yield MCQs for ABOS & OITE
14 Apr 2026
106 min read
86 Views
Key Takeaway
This page offers 100 randomized, high-yield orthopedic board review questions (MCQs) for ABOS, OITE, and FRCS exams. Practice Set 787 helps surgeons test their knowledge, identify areas for improvement, and master essential concepts, ensuring comprehensive preparation for their certification and in-training assessments.
Minimally Invasive Plate Osteosynthesis (MIPO...
00:00
Start Quiz
Question 1High Yield
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Explanation
Explanation
20b 20c The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
References:
- Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 2High Yield
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Explanation
Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.
Question 3High Yield
What is the most common cause of errors that harm patients?
Explanation
Explanation
The AMA report identified communication breakdown as the most common cause of errors that harm patients. It is extremely important to learn to communicate effectively with your patients. Understanding cultural and language differences helps avoid communication errors. Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007. American Medical Association ethical force program report: "Improving communication - Improving care", 2006
References:
- http://www.ama-assn.org/ama/pub/category/16245.html.
Question 4High Yield
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
Explanation
The obturator artery lies closest to the transverse acetabular ligament. The femoral artery is closest to the anterior rim of the acetabulum. No named vessel lies within the substance of the gluteus minimus or superior to the piriformis tendon. The medial femoral circumflex artery lies medial or deep to the quadratus femoris muscle. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, Figure 7-53, p 346.
References:
- Callaghan JJ, Rosenberg AG, Rubash HE: The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, p 705.
Question 5High Yield
The arrow in Figure 39 is pointing to which of the following ligaments?
Explanation
The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The scapholunate interosseous ligament stabilizes the scapholunate joint. The ulnolunate ligament originates from the base of the ulnar styloid and inserts in the lunate. The ulnotriquetral ligament originates from the base of the ulnar styloid and inserts on the triquetrum. The ulnolunate and the ulnotriquetral ligaments are important stabilizers to the ulnar side of the wrist. The short radiolunate ligament originates on the volar ulnar margin of the distal radius and inserts in the ulnar margin of the lunate. Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 6High Yield
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
Explanation
With the notable exception of fusion for degenerative spondylolisthesis and scoliosis, there is a paucity of evidence on the indications for spinal fusion in patients undergoing laminectomy for spinal stenosis. However, it is generally recommended that if the spine is destabilized (for example by removal of one complete facet joint or by an iatrogenic pars fracture), spinal fusion should be considered. Although fusion can be considered for a very long laminectomy, a two-level laminectomy does not represent, by itself, a clear indication for the addition of a spinal fusion. The repair of a dural tear and the use of nicotine by the patient play no role in the determination of whether or not to add fusion to a laminectomy procedure. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Question 7High Yield
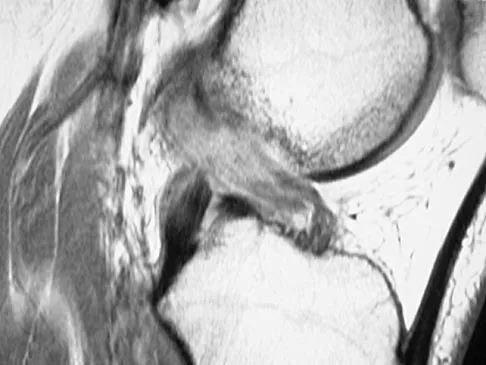
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of

Explanation
The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal. Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Question 8High Yield
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
Explanation
Alendronate is a second-generation bisphosphonate, and it can cause epigastric distress in up to 30% of patients. This side effect can be minimized by gradually building up to therapeutic doses over a period of 4 to 8 weeks. Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
References:
- Lane JM, Sandhu HS: Osteoporosis of the spine, in Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 227-234.
Question 9High Yield
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 um/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
Explanation
Studies on older systems, as well as newer designs, have confirmed that metal-on-metal bearing surfaces undergo linear wear of 2 to 5 um per year. Ceramic bearing surfaces produced with recent technology perform even better, with a wear rate of 0.5 to 2.5 um per year. Clinical wear rates of metal-on-crosslinked polyethylene have not yet been determined. McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
References:
- Schmalzried TP, Callaghan JJ: Wear in total hip and knee replacements. J Bone Joint Surg Am 1999;81:115-136.
Question 10High Yield
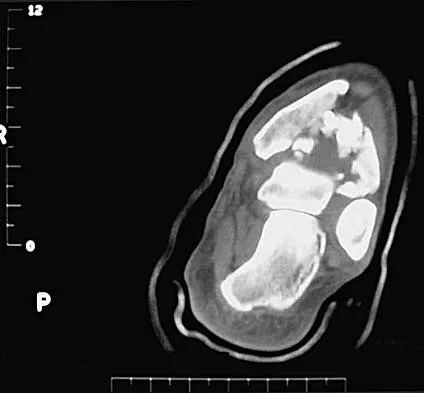
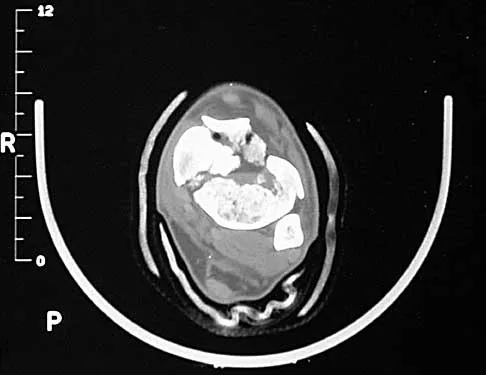
Figures 24a through 24c show the coronal T1-weighted, T2-weighted fat-saturated, and T1-weighted fat-saturated gadolinium MRI scans of the proximal thigh of a 52-year-old woman who reports a mass in the medial thigh and groin area. She notes that the fullness has grown in size over the course of many months. Based on these findings, what is the most likely diagnosis?
Explanation
Explanation
24b 24c The images show a complex, lobular lesion of the thigh that has signal characteristics that follow fat. The size of the lesion, the areas of stranding within the mass, along with mild uptake on the gadolinium sequences and the mild edema within the lesion on the T2-weighted image make liposarcoma the most likely diagnosis and simple intramuscular lipoma far less likely. All other diagnoses listed would not follow fat characteristics shown on the MRI sequences.
References:
- Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 11High Yield
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
Explanation
The most important consequence of a displaced talar neck fracture after closed or open treatment is malunion. Because displacement of the talar neck is associated with displacement of the subtalar joint, any malunion leads to intra-articular incongruity or malalignment of the subtalar joint. Varus malunion is common when there is comminution of the medial talar neck. This results in pain, osteoarthritis, and hindfoot deformity that requires further treatment. Because of these complications, it is imperative that all displaced talar neck fractures are reduced anatomically; fragmented fractures may require bone grafting to maintain the length and rotation of the neck. Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
References:
- Raaymakers EL: Complications of talar fractures, in Tscherne H, Schatzker J (eds): Major Fractures of the Pilon, the Talus, and Calcaneus: Current Concepts of Treatment. Berlin, Springer-Verlag, 1993, pp 137-142.
Question 12High Yield
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?
Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 13High Yield
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of
Explanation
Explanation
Congenital dislocation of the knee is an uncommon deformity that varies in presentation from simple hyperextension to complete anterior dislocation of the tibia on the femur. Treatment varies with the age at presentation and the severity of the deformity. Most authors recommend early nonsurgical management. A recent study of 24 congenital knee dislocations in 17 patients found that satisfactory results were obtained in most instances using closed treatment. Based on their findings, the authors concluded that immediate reduction or serial casting should be performed when the patient is seen early after birth. If the patient is seen late and correction cannot be achieved by serial casting, traction followed by closed or open reduction may be necessary. Early percutaneous quadriceps recession has been described for complex congenital knee dislocations associated with underlying disorders, such as arthrogryposis and Ehlers-Danlos syndrome. Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259. Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
References:
- Roy DR, Crawford AH: Percutaneous quadriceps recession: A technique for management of congenital hyperextension deformities of the knee in the neonate. J Pediatr Orthop 1989;9:717-719.
Question 14High Yield
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80 degrees. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62 degrees. One year later, the mean gain was 33 degrees. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
Question 15High Yield
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
Explanation
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker. Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270. Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
References:
- Allain J, Goutallier D, Glorion C: Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-852.
Question 16High Yield
Figure 15 shows the radiograph of an active 60-year-old woman. Which of the following variables is considered the strongest contraindication to a unicompartmental knee arthroplasty in this patient?
Explanation
Explanation
Unicompartmental arthroplasty of the knee for single compartment arthrosis has recently become more popular. Contraindications to unicompartmental knee arthroplasty include fixed varus or valgus deformity of more than 5 degrees, restricted range of motion, fixed flexion contracture, joint subluxation of 5 mm or greater, and arthrosis of the opposite and/or patellofemoral compartment. Cossey AJ, Spriggins AJ: The use of computer-assisted surgical navigation to prevent malalignment in unicompartmental knee arthroplasty. J Arthroplasty 2005;20:29-34. Iorio R, Healy WL: Unicompartmental arthritis of the knee. J Bone Joint Surg Am 2003;85:1351-1364.
References:
- Argenson JN, Chevrol-Benkeddache Y, Aubaniac JM: Modern unicompartmental knee arthroplasty with cement: A three to ten-year follow-up study. J Bone Joint Surg Am 2002;84:2235-2239.
Question 17High Yield
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
Explanation
The posterior interosseous nerve is located adjacent to the radial neck, placing it at risk for a traction injury with a dislocation of the proximal radius. The typical neurapraxia that results can be expected to resolve with observation within the first 6 to 12 weeks. If recovery is not clinically evident by 3 months, neurophysiologic studies are indicated. Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
References:
- Stein F, Grabias SL, Deffer PA: Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am 1971;53:1432-1436.
Question 18High Yield
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
Question 19High Yield
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
Explanation
The proposed mechanisms by which steroids such as methylprednisolone are thought to prevent neurologic deterioration by limiting secondary insult, include: decreasing the area of ischemia in the cord, reducing TNF-alpha expression and NF-kB binding activity, decreasing free radical oxidation and thus stabilizing cell and lysosomal membranes, and checking the influx of calcium into the injured cells, thus reducing cord edema. Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.
Question 20High Yield
Which of the following statements best describes results that have been reported with roentgen stereophotogrammetric analysis (RSA)?
Explanation
Explanation
Migration of total hip femoral components has been measured by RSA, a technique that affords accuracy of 2 degrees and 0.5 mm. Several published studies on total hip arthroplasty femoral components have established the importance of this technique. Both cemented and cementless components migrate, with the rate of migration suggesting the adequacy of fixation of a component. Migration of 1 mm to 2 mm (occurring in either the varus-coronal plane and retroversion-transverse plane, or both) has been associated with a higher risk of loosening of the component.
References:
- Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 100.
Question 21High Yield
When performing a total knee arthroplasty using modular components, what is the minimum recommended thickness of an ultra-high molecular weight polyethylene insert for a tibial component?
Explanation
Explanation
Polyethylene wear has been identified as a major contributor to failure of total knee implants, of which thickness is an important factor. Several studies have shown that the minimum thickness should be 6 to 8 mm. While Wright and Bartel have shown that 6 to 8 mm has been recommended as the minimum thickness of an ultra-high molecular weight polyethylene insert for a tibial component in total knee arthroplasty, more recent work by Meding and associates and Worland and associates has verified the clinical efficacy of 4 mm of polyethylene in compression-molded anatomic graduated nonmodular components. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Wright TM, Bartel DL: The problem of surface damage in polyethylene total knee components. Clin Orthop 1991;273:261-263. Meding JB, Ritter MA, Faris PM: Total knee arthroplasty with 4.4 mm of tibial polyethylene: 10-year followup. Clin Orthop 2001;388:112-117.
References:
- Worland RL, Johnson G, Alemparte J, Jessup DE, Kennan J, Norambuena N: Ten to fourteen year survival and functional analysis of the AGC total knee replacement system. Knee 2002;9:133-137.
Question 22High Yield
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?
Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 23High Yield
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?
Explanation
Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
References:
- Badelon O, Bensahel H, Mazda K, et al: Lateral humeral condylar fractures in children: A report of 47 cases. J Pediatr Orthop 1988;8:31-34.
Question 24High Yield
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?
Explanation
The eccentric metaphyseal location, skeletal maturity, narrow zone of transition, and lack of symptoms suggest a benign process and are consistent with a healed nonossifying fibroma. These lesions typically fill in (ossify) with skeletal maturity, eventually remodeling and disappearing. Radiographic monitoring is indicated. Biopsy is not recommended unless the lesion changes radiographically. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393. Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Question 25High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include

Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 26High Yield
A 21-year-old man has mild but persistent aching pain in his left proximal thigh during impact loading activities. He denies pain at rest and has no other symptoms. Figures 34a through 34e show the radiographs and T1-weighted, T2-weighted, and gadolinium MRI scans of the left hip. What is the most likely diagnosis?
Explanation
Explanation
34b 34c 34d 34e The radiographs show a centrally located radiolucent lesion with cortical thinning and mild osseous expansion; these findings are the hallmarks of a simple bone cyst. Whereas this particular lesion does not demonstrate sclerosis, the distinct margin of this lesion with sharp transition to normal bone is common. The MRI scans reveal a purely cystic lesion with bright T2 signal, and the gadolinium image shows the classic rim enhancement of cystic lesions. Fibrous dysplasia with cystic degeneration might have a very similar appearance and should be considered in the differential diagnosis. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035. May DA, Good RB, Smith DK, et al: MR imaging of musculoskeletal tumors and tumor mimickers with intravenous gadolinium: Experience with 242 patients. Skeletal Radiol 1997;26:2-15.
References:
- Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 4023-4034.
Question 27High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 28High Yield
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
BMPs signal through the activation of a transmembrane serine/threonine kinase receptor that leads to the activation of intracellular signaling molecules called SMADs. There are currently eight known SMADs, and the activation of different SMADs within a cell leads to different cellular responses. The other mediators are not believed to be directly involved with BMP signaling. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 29High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 30High Yield
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient's desire to return to sport?
Explanation
Explanation
Injuries to the MCL usually result from repetitive high valgus stress on the medial aspect of the elbow joint due to overhead throwing or racquet sports. Excessive stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing. Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
References:
- Altchek DW, Andrews JR (eds): The Athlete's Elbow. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 91.
Question 31High Yield
Bisphosphonates are indicated in the treatment of osteoporosis in patients who have a DEXA T-score of
Explanation
Explanation
Bisphosphonates are indicated in the treatment of osteoporosis. They have been shown to reduce the incidence of vertebral and extremity fractures in patients with a T-score of less than -1.
Question 32High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of

Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 33High Yield
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of


Explanation
Results of treatment of subscapularis rupture are best when immediate repair is performed. When the cause of the anterior instability is the result of rupture of the subscapularis tendon and the component position is acceptable, revising the position of the component is unnecessary. Restoring the coracoacromial arch and subacromial decompression are related to superior instability and rotator cuff pathology, respectively, and would not correct the instability caused by subscapularis rupture. Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Question 34High Yield
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?
Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 35High Yield
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity. Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Question 36High Yield
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
The rhomboideus major and minor muscles are innervated by the dorsal scapular nerve, which is supplied entirely by the C5 nerve root. The dorsal scapular nerve arises just distal to the dorsal root ganglion of the C5 nerve root. A functioning rhomboid muscle indicates that an injury involving C5 nerve root fibers must be postganglionic or distal to the C5 dorsal root ganglion. Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Question 37High Yield
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
The patient has a moderately displaced distal diaphyseal fracture of the fifth metatarsal, and the most appropriate treatment is brief immobilization and symptomatic management. Attempts at closed reduction are unlikely to appreciably alter the position of the fracture. Surgical techniques for either reduction of the fracture or fixation have not been shown to result in improved functional outcomes. O'Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: "Dancer's Fracture." Am J Sports Med 1996;24:240-243. DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Question 38High Yield
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
Numerous causes of tarsal tunnel syndrome have been reported. The most favorable outcomes from release of the tarsal tunnel are in patients who have a space-occupying lesion (eg, ganglion, lipoma, or neurilemoma). While electrodiagnostic studies may be abnormal preoperatively, there is a low correlation between clinical outcome and electromyographic findings. Intrinsic weakness is a late finding in long-standing nerve dysfunction. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 39High Yield
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?
Explanation
Explanation
23b Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening. Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496. Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
References:
- Martin SD, Zurakowski D, Thornhill TS: Uncemented glenoid component in total shoulder arthroplasty: Survivorship and outcomes. J Bone Joint Surg Am 2005;87:1284-1292.
Question 40High Yield
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
Explanation
14b 14c The PA view of the wrist shows a pisiform fracture. Pisiform fractures constitute 1% to 3% of all carpal bone fractures. This fracture can be further evaluated with a carpal tunnel view or a supination oblique view of the wrist. Initial management should consist of immobilization with a short arm cast. If nonsurgical measures fail, bony excision is warranted. Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
References:
- Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 41High Yield
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
Explanation
When a lateral condylectomy alone is performed for all bunionette deformities, a high recurrence rate is expected. Lateral condylectomy should be used alone when the primary deformity is an enlarged lateral condyle of the fifth metatarsal head. In cases with significant divergence of the fifth metatarsal shaft in relationship to the fourth metatarsal shaft or with lateral bowing of the distal fifth metatarsal shaft, the lateral fifth metatarsal prominence will not be effectively reduced and recurrent symptoms and deformity are expected. Transfer metatarsalgia and/or dislocation of the metatarsophalangeal joint can infrequently occur with excessive metatarsal head excision. Arthrosis of the metatarsophalangeal joint has not been frequently reported. Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465. Kelikian H: Deformities of the lesser toe, in Kelikian H (ed): Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA, WB Saunders, 1965, pp 327-330.
Question 42High Yield
Which of the following factors is a significant predictor of reoperation following open reduction and internal fixation of intertrochanteric fractures with a sliding-compression hip-screw device?
Explanation
Explanation
As shown by Palm and associates from the Hip Fracture Study group, the integrity of the lateral femoral cortex in intertrochanteric hip fractures is a significant predictor of reoperation. Baumgartner and associates have shown that a tip-apex distance of greater than 25 mm is associated with a high risk of femoral head cut-out. Lastly, intertrochanteric hip fractures can be described as standard obliquity or reverse obliquity when describing the fracture pattern. Mechanistically, a reverse obliquity pattern is important to recognize because it reflects the presence or absence of a lateral buttress to which the proximal fracture fragment may compress. Palm H, Jacobsen S, Sonne-Holm S, et al: Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J Bone Joint Surg Am 2007;89:470-475. Sadowski C, Lübbeke A, Saudan M, et al: Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: A prospective, randomized study. J Bone Joint Surg Am 2002;84:372-381.
Question 43High Yield
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
Explanation
The great medullary artery originates as a direct or indirect branch of the left posterior intercostal artery, usually between T8 and T12. It becomes intradural and crosses over one to three disk spaces before turning to the midline where it anastomoses with the anterior spinal artery. Injury to this artery can result in devastating ischemia of the lower spinal cord. Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
References:
- Rogers FB, Osler TM, Shackford SR, Wald SL: Isolated stab wound to the artery of Adamkiewicz: Case report and review of the literature. J Trauma 1997;43:549-551.
Question 44High Yield
In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
Explanation
Explanation
In examining a traditional Muslim woman, a male physician should have another woman present, and the patient's husband, if possible. Only the affected limb or area needing examination should be exposed.
Question 45High Yield
The force generated by a muscle is most highly dependent on its
Explanation
Explanation
The cross-sectional area of a muscle determines to a great extent the force generated by the muscle. The force of a muscle contraction is controlled by the amount of myofibrils that contract; the greater the amount of contracting myofibrils, the greater the force of contraction. Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction. Muscle length affects contraction force through the Blix curve. The morphology of a muscle can affect the cross-sectional area by varying the angle of the fibers in relation to the force vector. Conditioning mostly affects duration and fatigability. Buckwalter JA, Mow VC, Ratcliffe A: Restoration of injured or degenerated articular cartilage. J Am Acad Orthop Surg 1994;2:192-201.
References:
- Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 683-716.
Question 46High Yield
A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?
Explanation
This deformity is early in the disease process. The foot is still flexible, as evidenced by correction with the Coleman block test. A simple dorsiflexion osteotomy of the first metatarsal should provide a plantigrade foot. More complex osteotomies are required later in the disease process when the foot is not flexible and the deformity does not correct with the Coleman block test. The patient may also require a tibialis anterior transfer later in the disease process but not at the present time. Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.
Question 47High Yield
The posterior circumflex humeral artery and the axillary nerve usually lie in a space bordered superiorly by the
Explanation
Explanation
The quadrangular space is bordered superiorly by the teres minor, medially by the long head of the triceps, laterally by the humerus, and inferiorly by the teres major. The posterior circumflex humeral artery and the axillary nerve lie in this space. Rockwood CA Jr, Matsen FA III: The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 70-71.
References:
- Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 401-402, 407.
Question 48High Yield
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of
Explanation
This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity. Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Question 49High Yield
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18 degrees of valgus compared with 3 degrees of valgus on the opposite side. Management should now include
Explanation
The development of a valgus deformity after this type of fracture is a well-known occurrence, and the patient's parents should be informed about this risk. In a patient who is age 4 years, the natural history is one of gradual correction by the development of a physiologic varus deformity at the distal tibial physis; therefore, no active intervention is needed at this time. Bracing has no effect on the deformity, and the child is too young for any procedure on the growth plate. Proximal tibial osteotomy is reserved until the patient nears skeletal maturity because of the risk of recurrence of the deformity. Lateral stapling can be done near skeletal maturity if the deformity persists, but this is unlikely to be necessary. Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Question 50High Yield
A 21-year-old man has had progressive right knee pain for the past 2 months that is exacerbated with weight-bearing activities. A plain radiograph and an MRI scan are shown in Figures 43a and 43b. A biopsy specimen is shown in Figure 43c. According to the Enneking staging system of tumor classification, the lesion should be classified as what stage?
Explanation
Explanation
43b 43c The lesion is an eccentric lytic bone lesion within the epiphyseal-metaphyseal end of the proximal tibia. There is geographic destruction with a "fading border" extending to the articular cartilage. There is no matrix formation or periosteal reaction. The MRI scan shows cortical destruction with extension into the soft tissue. According to the Enneking staging system, benign lesions are stage 1, 2, or 3; malignant lesions are stage I, II, or III. Benign stage 1 lesions are latent; stage 2 are active; and stage 3 are benign aggressive. The histology shows a benign giant cell tumor. Given the cortical breakthrough shown on the MRI scan, the lesion should be classified as stage 3. Enneking WF: Clinical musculoskeletal pathology, in Enneking WF (ed): Appendix A. Gainesville, FL, Storter Publishing, 1986, pp 451-466.
References:
- Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Question 51High Yield
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
Explanation
Indications for open reduction of glenoid intra-articular fractures include those fractures with a 5-mm articular surface displacement or when the humeral head is subluxated with the fracture fragment. Kavanaugh and associates and Leung and Lam have shown that the posterior approach with plate fixation is best for most glenoid fractures, including the Ideberg type II fracture shown here. The anterior approach is best used for anterior rim and transverse fractures. Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484. Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
References:
- Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 52High Yield
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?
Explanation
The patient has hypertrophic arthritis, which is a strong risk factor for heterotopic bone formation. The remaining complications are possible but do not have the same significant risks. Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Question 53High Yield
Figure 42 shows the sagittal T2-weighted MRI scan of a patient's right knee. These findings are most commonly seen with a complete tear of the
Explanation
Explanation
The MRI scan reveals disruption of the lateral capsule and ligaments with fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions. LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
References:
- Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 54High Yield
A 25-year-old man injures his shoulder while skiing. Examination reveals increased passive external rotation, pain in the cocked position, and a positive lift-off test. What is the most likely diagnosis?
Explanation
Explanation
A positive lift-off test and increased passive external rotation are diagnostic of a subscapularis tear or detachment. Although a similar injury could produce anterior instability, this will test the integrity of the subscapularis. A locked dislocation has limited passive movement. A ruptured biceps tendon will most likely produce ecchymosis and findings similar to supraspinatus trauma. Internal impingement is not associated with subscapularis weakness. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
References:
- Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 55High Yield
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
All of the factors listed contribute to some extent to the pull-out strength of lumbar pedicle screws, but bone mineral density correlates most precisely. Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Question 56High Yield
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?



Explanation
Based on these findings, the most likely diagnosis is fibrous dysplasia. Twenty percent of patients with fibrous dysplasia have multifocal disease. The lesions show a typical ground glass appearance. Fibrous dysplasia frequently involves the diaphysis of the long bones. There is no associated soft-tissue mass and no periosteal reactions to these lesions, suggesting a benign lesion. The histology shows proliferating fibroblasts in a dense collagen matrix. Trabeculae are arranged in an irregular or "Chinese letter" appearance. Osteogenic sarcoma and Ewing's sarcoma have a much different radiographic appearance of malignant osteoid and small round blue cells. Periosteal chondroma does occur in the proximal humerus but is not typically multifocal. It appears as a surface lesion with saucerization of the underlying bone and a bony buttress adjacent to the lesion. Some patients with multifocal lesions have associated endocrine abnormalities (McCune-Albright syndrome). Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Question 57High Yield
A 30-year-old woman has pain in her right hand. The radiograph, CT scan, and biopsy specimen are seen in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Explanation
38b 38c An enchondroma is the most common primary tumor of the long bones of the hand. The lesion is usually asymptomatic and often is detected when there is a pathologic fracture. Shimizu K, Kotoura Y, Nishijima N, Nakamura T: Enchondroma of the distal phalanx of the hand. J Bone Joint Surg Am 1997;79:898-900.
References:
- Takigawa K: Chondroma of the bones of the hand: A review of 110 cases. J Bone Joint Surg Am 1971;53:1591-1600.
Question 58High Yield
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?

Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 59High Yield
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
The patient has posttraumatic arthritis of the elbow; therefore, the treatment of choice is hardware removal and soft-tissue releases with splinting to avoid recurrence of contractures. The combination of pain and stiffness in an elbow that has sustained significant joint surface damage renders it unresponsive to simple soft-tissue releases and heterotopic bone excision. Joint distraction and interposition arthroplasty offer the possibility of maintaining motion and relieving pain as a later salvage procedure. Joint replacement should not be performed in young, active, strong individuals because the prosthesis will fail quickly and complications will develop. Synovectomy and radial head excision are not indicated. Morrey BF: Distraction arthroplasty: Clinical applications. Clin Orthop 1993;293:46-54.
Question 60High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 61High Yield
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
Explanation
Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
References:
- Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 62High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with


Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 63High Yield
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?
Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 64High Yield
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?

Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 65High Yield
During total knee arthroplasty, what component position aids in proper tracking and stability of the patellar component?
Explanation
Explanation
The femoral component should be implanted with enough external rotation to facilitate patellar tracking. Proper tracking requires a normal Q angle and is affected by axial and rotational alignment of the femur and tibia. An excessive Q angle can result from internal rotation of either component, medialization of the tibial tray, or lateralization of the patellar component. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
References:
- Lonner JH, Lotke PA: Aseptic complications after total knee arthroplasty. J Am Acad Orthop Surg 1999;7:311-324.
Question 66High Yield
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of
Explanation
The findings are classic for a pectoralis major tendon avulsion. Deformity of the anterior axillary fold is a classic finding, and ecchymosis down the arm suggests that the injury is at the humeral attachment rather than at the musculotendinous junction. Good external rotation strength indicates that function in the supraspinatus and infraspinatus has been preserved. The treatment of choice for a tendon avulsion in a young individual is early surgical repair. Conversely, if the injury is within the muscle or at the musculotendinous junction, initial nonsurgical management is recommended. If the location of the injury cannot be determined by physical examination, then MRI of the pectoralis major can be helpful. Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 67High Yield
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 68High Yield
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of
Explanation
Explanation
41b Open reduction and internal fixation of distal humeral fractures in elderly patients often fails. These fractures characteristically have a very small distal segment and poor bone quality, resulting in failure of fixation and nonunion. Nonunion is often painful and functionally debilitating. Total elbow arthroplasty provides good results when used for distal humeral fractures in elderly patients with osteopenic bone and fracture patterns thought to be irreconstructable. Long arm casting may result in union, but the resulting stiffness is unacceptable for an active patient. Elbow arthrodesis has few indications. A sling and range-of-motion exercises will often result in a painful and debilitating nonunion at the fracture site. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
References:
- Obremskey WT, Bhandari M, Dirschl DR, et al: Internal fixation versus arthroplasty of comminuted fractures of the distal humerus. J Orthop Trauma 2003;17:463-465.
Question 69High Yield
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
Explanation
The best method of preventing wrong-site surgery is for the surgeon to initial the surgical site in the preoperative holding area after discussion and confirmation of the site with the patient. This should be done before sedating medications are administered. A recent study found that patient noncompliance with specific preoperative instructions to mark the site with a "yes" at home was surprisingly high; only 59% of the patients marked the extremity correctly and 37% made no mark. Noncompliance was higher in those with workers' compensation claims (70%) and those with previous related surgery (51%). DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
References:
- American Academy of Orthopaedic Surgeons. Advisory Statement: Wrong-site Surgery. Document 1015, 2002 Sept. www.aaos.org/wordhtml/papers/advismt/wrong.htm.
Question 70High Yield
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?
Explanation
Explanation
Persistent Horner's sign (ptosis, myosis, and anhydrosis) is a sign of proximal injury, usually avulsion of the roots from the cord which disrupts the sympathetic chain. Root rupture or avulsion proximal to the myelin sheath has less chance of healing. Two-month-old infants with persistent weakness in the other areas described may still have a good prognosis for recovery. Concurrent clavicle fracture has been shown to have no prognostic value. Clarke HM, Curtis CG: An approach to obstetrical brachial plexus injuries. Hand Clin 1995;11:563-581.
References:
- Narakas AO: Injuries to the brachial plexus, in Bora FW (ed): The Pediatric Upper Extremity: Diagnosis and Management. Philadelphia, PA, WB Saunders, 1986, p 247.
Question 71High Yield
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 72High Yield
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
While injury of the distal radial metaphysis is a rather common occurrence, the incidence of physeal arrest is only about 4% to 5% of patients. While injury of the distal physis of the ulna is rare, the incidence of physeal arrest is greater than 50% in fractures of this structure. These patients need to be followed closely both clinically and radiographically to look for the signs of distal ulnar/physeal arrest such as loss of the prominence of the ulna and ulnar deviation of the hand. Radiographically, progressive shortening of the ulna is observed. Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Question 73High Yield
Which of the following is considered the most important factor in eliminating infection in chronic osteomyelitis?
Explanation
Explanation
The most important factor in eliminating infection in chronic osteomyelitis is a complete debridement of the compromised bone and soft tissue. Antibiotics should be used in conjunction with surgical debridement. However, the foundation of treating infected bone is removal of the diseased tissue. Cierny G III, Cook WG, Mader JT: Ankle arthrodesis in the presence of ongoing sepsis: Indications, methods, and results. Orthop Clin North Am 1989;20:709-721. Cierny G, Zorn EZ: Arthrodesis of the tibiotalar joint for sepsis. Foot Ankle Clin 1996;1:177-197.
References:
- Richter D, Hahn MP, Laun RA, Ekkernkamp A, Muhr G, Osterman PA: Arthrodesis of the infected ankle and subtalar joint: Technique, indications and results of 45 consecutive cases. J Trauma 1999;47:1072-1078.
Question 74High Yield
The postoperative neurologic prognosis of a patient who has a tumor that is compressing the spinal cord and causing a neurologic deficit depends primarily on the
Explanation
Explanation
The tumor biology, location, and pretreatment neurologic status are the best predictors of a patient's postoperative neurologic prognosis. Between 60% to 90% of patients who are ambulatory at the time of diagnosis will retain this ability after treatment. Location is important in that less space is available for the cord in the thoracic spine. Lesions located in vascular watershed regions may disrupt the vascular supply of the cord. Weinstein JN: Differential diagnosis and surgical treatment of primary benign and malignant neoplasms, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 1, pp 829-860.
References:
- Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 75High Yield
A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
Explanation
Explanation
Severe valgus deformity is frequently accompanied by hypoplasia of the lateral femoral condyle. Posterior referencing instrumentation can substantially internally rotate the femoral component with respect to the transepicondylar axis and Whiteside's line. The femoral component malrotation must be corrected to properly address this problem. Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.
References:
- Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 1995;321:168-172.
Question 76High Yield
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of
Explanation
Explanation
The radiograph shows an avulsion fracture, or "sleeve fracture," of the distal pole of the patella. The distal fragment is much larger than it appears on the radiograph because it largely consists of cartilage; therefore, excision of the fragment is contraindicated. The treatment of choice is open reduction and tension band fixation to correct patella alta and restore the extensor mechanism. Maguire JK, Canale ST: Fractures of the patella in children and adolescents. J Pediatr Orthop 1993;13:567-571.
References:
- Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990;10:721-730.
Question 77High Yield
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
Explanation
The bright signal on the T2-weighted MRI scan suggests fluid. The multiloculated appearance in proximity to the proximal tibiofibular joint suggests that the most likely diagnosis is a ganglion. They typically increase and decrease in size and can be diagnosed by the classic gelatinous fluid obtained through needle aspiration. Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
References:
- Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 78High Yield
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?
Explanation
Cervical myelopathy involves compression of the spinal cord and presents as an upper motor neuron disorder. Patients commonly have extremity spasticity and problems with ambulation and balance. Hoffman's sign is often present and is elicited by suddenly extending the distal interphalangeal joint of the middle finger; reflexive finger flexion represents a positive finding. The extremities are usually hyperreflexic with myelopathy. With cervical radiculopathy (lower motor neuron disorder), reflexes are hyporeflexic, and patients report pain along a dermatomal distribution. A hyperactive jaw jerk reflex indicates pathology above the foramen magnum or in some cases, systemic disease. Flaccid paraparesis suggests a lower motor neuron problem. Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Question 79High Yield
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?
Explanation
Explanation
1b 1c The radiographs and CT scan reveal osteoarthritis with posterior subluxation and posterior bone loss. Total shoulder arthroplasty with reaming of the high side to neutralize the glenoid surface has been shown to yield better results than hemiarthroplasty. The amount of bone loss in this patient does not require posterior glenoid augmentation. Reverse total shoulder arthroplasty is indicated for rotator cuff tear arthropathy; therefore, it is not applicable. Arthroscopic debridement has yielded poor results with advanced osteoarthritis and posterior subluxation. Results from glenoid osteotomy have been variable and glenoid osteotomy is not indicated with associated osteoarthritis. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
References:
- Rodosky MW, Bigliani LU: Indications for glenoid resurfacing in shoulder arthroplasty. J Shoulder Elbow Surg 1996;5:231-248.
Question 80High Yield
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
Explanation
18b Epithelioid sarcoma is the most common soft-tissue sarcoma in the hand and most commonly occurs in young adults. The tumors can be superficial and may become ulcerated. Deeper lesions are often attached to tendons, tendon sheaths, or fascial structures. These are usually minimally symptomatic. The biopsy specimen reveals the typical appearance of a nodular pattern with central necrosis. They can mimic a necrotizing granulomatous process. Usually there are chronic inflammatory cells along the margin of the tumor nodules. This biopsy specimen does not have the clear cells necessary for a clear cell carcinoma or sarcoma. Nora's tumor is a bizarre parosteal osteochondromatous proliferation (BPOP) first described in 1983 by the pathologist, Nora. The lesion is defined as a reactive heterotopic ossification and is mostly found in the hands or feet of adults in the third decade of life. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
References:
- Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 81High Yield
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Explanation
The radiograph shows osteochondritis dissecans (OCD) of the capitellum, one manifestation of "pitcher's elbow." The lesion is nondisplaced, and healing is possible if the inciting throwing activities are curtailed. Long arm cast treatment may be reasonable for the noncompliant patient but should not exceed 6 weeks duration. Surgical treatment is indicated for loose bodies or cartilage flaps. Elbow OCD lesions are now being seen in younger children as more participate in organized sports, especially baseball and gymnastics. Bauer M, Jonsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160. Takahara M, Ogino T, Sasaki I, et al: Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop 1999;363:108-115.
References:
- Byrd JW, Jones KS: Arthroscopic surgery for isolated capitellar osteochondritis dissecans in adolescent baseball players: Minimum three-year follow-up. Am J Sports Med 2002;30:474-478.
Question 82High Yield
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?

Explanation
The patient has a global loss of motion that has failed to improve with 6 months of nonsurgical treatment; because he has reached a plateau, further nonsurgical management will likely be ineffective. Revision in the form of an open release is indicated to lyse intra- and extra-articular adhesions; subscapularis lengthening may be done concurrently as needed. Revising to a smaller head can be considered if adequate motion is not achieved. The radiographs reveal an adequate neck cut with appropriate seating of the component. Removing the glenoid component will decrease capsular tension but will probably increase pain because of the lack of glenoid resurfacing. Increasing humeral retroversion will not improve motion. Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Question 83High Yield
Which of the following types of displaced posterior pelvic disruptions must undergo anatomic reduction and internal fixation to ensure the best clinical outcome?
Explanation
Although all of the above displaced injuries require reduction, the sacroiliac joint dislocation is a ligamentous injury. Without fixation, healing is unlikely and the result will be a painful dislocation. Both Holdsworth and Tile showed that the sacroiliac joint must be reduced anatomically and stabilized. The injuries through bone will unite fairly rapidly and, if reduced and stabilized with traction or external fixation, will generally result in an acceptable outcome unless modified by other associated problems such as neurologic injury. Tile M: Fractures of the Pelvis and the Acetabulum. Baltimore, MD, Williams and Wilkins, 1995. Holdsworth F W: Dislocation and fracture dislocation of the pelvis. J Bone Joint Surg Br 1948;30:461-465.
Question 84High Yield
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?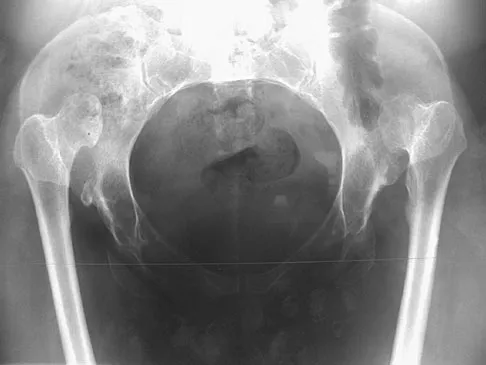
Explanation
The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve. Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Question 85High Yield
The gluteus maximus is innervated by which of the following nerves?
Explanation
Explanation
The inferior gluteal nerve supplies the gluteus maximus muscle. The superior gluteal nerve supplies the gluteus medius, gluteus minimus, and tensor fascia lata muscles. The femoral nerve supplies the quadriceps, sartorius, and pectineus muscles. The pudendal nerve is primarily a sensory nerve.
References:
- Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 146-147.
Question 86High Yield
A 58-year-old man with type 1 diabetes mellitus is seen in the emergency department and he reports a 3-day history of a red swollen foot but no history of trauma. Examination reveals that the skin is intact, and the patient has discomfort with passive range of motion at the ankle, hindfoot, and midfoot joints. He denies any fever. Laboratory studies show a WBC count of 7,800/mm3, an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 23, and a serum glucose of 100. A radiograph and MRI scans are shown in Figures 16a through 16c. What is the next most appropriate step in management?
Explanation
Explanation
16b 16c Whereas it is difficult to distinguish between cellulitis, septic joint, osteomyelitis, and early Eichenholtz stage 1 Charcot, the presence of a fracture in the absence of ulcerations with a normal WBC count and serum glucose strongly indicates that the described symptoms are due to an early Charcot process alone. A technetium Tc 99m scan alone would not be helpful; however, the addition of a sulfur colloid marrow scan or indium In 111 scan may be more specific to rule out infection, though it is not warranted here. Total contact casting with non-weight-bearing or limited weight bearing during Eichenholtz stage 1 when the foot is warm, erythematous, and swollen is advised to help prevent deformity. Alternatively, stabilization with pneumatic bracing may also be considered. While some authors have proposed early fixation or arthrodesis for Eichenholtz stage 1, the gold standard is still total contact casting with no to limited weight bearing until the swelling resolves and evidence of consolidation is seen on radiographs. Trepman E, Nihal A, Pinzur MS: Current topics review: Charcot neuropathy of the foot and ankle. Foot Ankle Int 2005;26:46-63. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 123-134.
References:
- Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 87High Yield
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
Explanation
With the arm in the abducted, externally rotated position, the anterior band of the inferior glenohumeral ligament complex moves anteriorly, preventing anterior humeral head translation. Both the coracohumeral ligament and the superior glenohumeral ligament restrain the humeral head to inferior translation of the adducted arm, and to external rotation in the adducted position. The middle glenohumeral ligament is a primary stabilizer to anterior translation with the arm abducted to 45 degrees. The posterior band of the inferior glenohumeral ligament complex resists posterior translation of the humeral head when the arm is internally rotated. Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
References:
- Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 88High Yield
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
Explanation
1b The patient has a discrete callus that overlies a prominent medial sesamoid. Calluses typically occur in response to increased pressure on the skin. Initial treatment should be directed at reducing local pressure with a felt pad. Sesamoid shaving is indicated if the felt pad fails to provide relief. Sesamoidectomy should be reserved for refractory callus given the potential complications of transfer metatarsalgia or callus and hallux valgus. A first metatarsal dorsiflexion osteotomy is more appropriate for a diffuse callus that fails to respond to nonsurgical management. Cryoablation and topical salicylic acid are appropriate for plantar warts, which have a rougher appearance with multiple, small black spots in the lesion. Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
References:
- Mann RA, Mann JA: Keratotic disorders of the plantar skin. Instr Course Lect 2004;53:287-302.
Question 89High Yield
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?




Explanation
The radiographs reveal phleboliths on the volar side of the forearm consistent with hemangioma. The MRI scan reveals a rather well-circumscribed in size, irregular in shape, intramuscular soft-tissue mass in the volar aspect of the distal right forearm within the flexor group musculature. The mass demonstrates heterogeneous mixed signal intensity in both T1- and T2-weighted sequences with increased signal intensity on the T1, suggesting fat within the tumor, typical of hemangioma. The postgadolinium-enhanced sequences demonstrate heterogeneous enhancement. The MRI findings are consistent with a soft-tissue hemangioma. Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Question 90High Yield
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Explanation
The symptoms, physical findings, and laboratory studies are most consistent with a diagnosis of infectious sacroiliitis, usually caused by Staphylococcus aureus. Initial radiographs will be normal, and the diagnosis of sacroiliitis is often delayed. A technetium Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip. Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop 1993;287:98-106.
References:
- Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 91High Yield
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?

Explanation
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit. Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
Question 92High Yield
Which of the following is a recognized consequence of hip fusion?
Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 93High Yield
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
Explanation
17b 17c Osteofibrous dysplasia frequently presents at a very young age, usually less than 10 years. In most patients, it involves the anterior cortex of the tibial shaft and minor anterior bowing of the tibia is frequently seen. The lesion is unpredictable in nature, but local recurrence is very high in patients who undergo surgery before 15 years of age. Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
References:
- McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 94High Yield
Figures 10a through 10c show the radiographs of an 85-year-old man who underwent a revision total knee arthroplasty for loosening of the tibial component 6 months ago. He now reports a mildly uncomfortable mass on the anterior part of the knee joint. Examination reveals 95 degrees of motion and good quadriceps strength, and he can ambulate with minimal pain with a walker. History reveals chronic lymphocytic leukemia for which he is taking antineoplastic medication. Culture of the mass aspirate grew Candida albicans on two separate occasions. The patient and the family strongly prefer nonsurgical management. If long-term suppression is chosen as treatment, what advice should be given to the patient and family?
Explanation
Explanation
10b 10c In patients with infected implants, treatment usually involves debridement and exchange of the infected components. In rare cases, when there is severe comorbidity and immune system compromise, as there is with this patient, a form of chronic suppression is indicated. This patient's function is quite satisfactory and, even though there is only a 21% to 38% chance of success (Hirawaka as quoted by Mulvey and Thornhill), an attempt at suppression therapy is indicated. The patient must be followed closely to monitor the potential complications of long-term antifungal therapy and to monitor the integrity of the joint, looking for bone or soft-tissue destruction. Because the patient has satisfactory motion and quadriceps strength, no bracing or other assistive device (except for the walker he is now using) is indicated.
References:
- Mulvey TJ, Thornhill TS: Infected total knee arthroplasty, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1857-1890.
Question 95High Yield
A 48-year-old woman with a history of a spinal cord injury as a teenager, has unilateral weakness in the left lower extremity. She has used an ankle-foot orthosis for many years without difficulty but recently has had a recurrent painful callus beneath the great toe that has been recalcitrant to nonsurgical management. Examination reveals intact sensation with an intractable plantar keratosis (IPK) beneath the first metatarsal head. Motor examination reveals no active ankle or great toe dorsiflexion, and 4/5 plantar flexion strength at the ankle and great toe. Passive ankle dorsiflexion is 10 degrees, whereas passive plantar flexion is 40 degrees. Passive great toe dorsiflexion is 30 degrees and plantar flexion is 10 degrees. Foot alignment on standing is normal. Radiographs are shown in Figures 47a and 47b with a marker beneath the IPK. Based on her request for surgical treatment, what is the most appropriate procedure?
Explanation
Explanation
47b Passive dorsiflexion is adequate to accommodate standing erect without excessive pressure, and a gastrocnemius recession may lead to more instability. Complete excision of the medial sesamoid could lead to an iatrogenic hallux valgus deformity. She does not have a cock-up toe deformity; therefore, a flexor hallucis longus tendon transfer is not warranted. There is no significant foot deformity; therefore, a dorsiflexion osteotomy is not warranted. The appropriate procedure is planing of the plantar half of the medial sesamoid, thereby preserving its function while diminishing the excessive pressure. Grace DL: Sesamoid problems. Foot Ankle Clin 2000;5:609-627. Mizel MS, Miller RA, Scioli MW (ed): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 135-150.
Question 96High Yield
A 50-year-old woman has a painful hallux valgus and a painful callus beneath the second metatarsal head. A radiograph is shown in Figure 46. To correct these problems, treatment of the great toe deformity should consist of
Explanation
The patient has a significant hallux valgus and instability of the first ray, causing transfer metatarsalgia to the second metatarsal head. Therefore, the best procedure is fusion of the metatarsal cuneiform joint with soft-tissue realignment of the first metatarsophalangeal joint. This procedure provides the best chance of relieving symptoms under the second metatarsal head, as well as correcting the hallux valgus.
Question 97High Yield
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Progressive hip subluxation occurs in up to 50% of children with spastic quadriparesis. The subluxation is the result of chronic muscle hypertonicity, especially in the adductor muscle group. In time, the constant muscle tension will lead to dislocation, dysplastic changes in the acetabulum, and erosive changes in the cartilage of the femoral head. Many of these children will experience pain. Two recent studies have shown that early soft-tissue releases can successfully prevent progressive subluxation in children who are younger than age 4 years and who have a Reimers index (migration index) of less than 40%. Botulinum toxin A injections may reduce tone in the adductors for 4 to 6 months, but it is difficult to inject into the iliopsoas. Additionally, there are no long-term studies documenting the efficacy of botulinum toxin A to treat progressive hip subluxation in patients who have spastic quadriparesis. In general, proximal femoral osteotomy, combined with soft-tissue release as necessary, is indicated in older children (older than age 4 years) with progressive subluxation. Although selective dorsal rhizotomy has been used in nonambulatory patients, outcomes are less well documented than in ambulatory patients. There are no studies documenting the effect of selective dorsal rhizotomy on progressive hip subluxation in nonambulatory children. Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
Question 98High Yield
Examination of a 7-year-old girl with myelomeningocele reveals calcaneal deformities of both feet. She ambulates on both extremities wearing ankle-foot orthoses and has no upper extremity aids. She has grade 5/5 motor strength to the tibialis anterior muscles and absent motor strength to the triceps surae. There is no varus or valgus deformity of the hindfoot, and the skin over the heels is intact; however, mild callosities are present. Management should consist of
Explanation
Explanation
A calcaneal deformity of the foot may occur in children who have low lumbar myelomeningocele. Strong dorsiflexors overcome a weak or absent gastrocnemius-soleus complex, leading to downward growth of the calcaneal apophysis. The deformity is usually progressive and does not respond to nonsurgical management. Most authorities recommend transfer of the tibialis anterior muscle through the interosseous membrane to the posterior aspect of the calcaneus. This procedure has been reported to be effective in limiting progression of the deformity. An extra-articular subtalar arthodesis, a treatment option for valgus deformity of the hindfoot, is not indicated. Similarly, Achilles tendon tenodesis to the fibula, an option for managing valgus of the ankle, is not indicated. Calcaneal osteotomy may be used in older children with severe calcaneal deformity. Stott NS, Zionts LE, Gronley JK, Perry J: Tibialis anterior transfer for calcaneal deformity: A postoperative gait analysis. J Pediatr Orthop 1996;16:792-798.
References:
- Georgiadis GM, Aronson DD: Posterior transfer of the anterior tibial tendon in children who have a myelomeningocele. J Bone Joint Surg Am 1990;72:392-398.
Question 99High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?
Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 100High Yield
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Explanation
The radiograph shows medial migration of the cementless acetabular component, strongly suggesting acetabular discontinuity with a combined segmental and cavitary medial deficiency. The treatment of choice is a morcellized or structural graft, supported with a reconstructive cage bridging the pelvic discontinuity, and a cemented cup. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon