Proximal Tibial Opening Wedge Osteotomy: A Masterclass in Limb Realignment

Key Takeaway
This masterclass provides an exhaustive, real-time guide to proximal tibial opening wedge osteotomy. We'll meticulously cover comprehensive surgical anatomy, detailed preoperative planning, and granular intraoperative execution, emphasizing neurovascular protection and precise bone cuts. Fellows will learn to navigate common pitfalls, manage complications, and optimize patient outcomes for knee realignment and stability.
Comprehensive Introduction and Patho-Epidemiology
Proximal Tibial Opening Wedge Osteotomy (HTO) represents a cornerstone in the orthopedic surgeon’s armamentarium for joint preservation, having evolved significantly from its historical iterations. Originally popularized in the mid-20th century as a closing wedge technique for isolated medial compartment arthrosis, the procedure has undergone a profound paradigm shift. Today, the medial opening wedge technique is the gold standard, offering a highly versatile, powerful method for addressing a broad spectrum of complex knee pathologies. This evolution has been driven by advancements in rigid internal fixation, a deeper understanding of lower extremity biomechanics, and the rising demand for joint-preserving options in younger, highly active patient populations.
The underlying pathophysiology necessitating an HTO is fundamentally rooted in mechanical overload. In a neutrally aligned lower extremity, the mechanical weight-bearing axis passes slightly medial to the center of the knee joint, distributing approximately 60% of the load to the medial compartment. However, in the presence of a varus deformity, this mechanical axis shifts further medially. This exacerbates the adduction moment at the knee during the stance phase of gait, leading to exponential increases in focal contact pressures on the medial articular cartilage. Over time, this relentless mechanical overload overwhelms the chondrocytes' reparative capacity, precipitating a cascade of cartilage degradation, subchondral sclerosis, and eventual unicompartmental osteoarthritis.
Epidemiologically, symptomatic varus gonarthrosis disproportionately affects middle-aged patients who maintain high occupational or recreational demands. These individuals often present with a biological age that precludes arthroplasty, yet they suffer from debilitating pain and functional limitations. Furthermore, the modern orthopedic landscape frequently encounters patients with combined pathologies, such as chronic ligamentous insufficiency coupled with malalignment. In these complex scenarios, the varus deformity not only accelerates joint degeneration but also places insurmountable stress on ligamentous reconstructions.
Consequently, the modern application of the opening wedge HTO extends far beyond isolated arthritis. It is now routinely employed synergistically with cartilage restoration procedures, such as autologous chondrocyte implantation (ACI), osteochondral allograft transplantation (OCA), and meniscal allograft transplantation (MAT). By surgically altering the mechanical alignment of the lower extremity and shifting the weight-bearing axis toward the relatively pristine lateral compartment, the HTO creates a biologically and mechanically favorable environment. This offloading is absolutely critical; without it, the newly implanted cartilage or meniscal tissue would be subjected to the same destructive sheer and compressive forces that destroyed the native tissue, inevitably leading to early graft failure.
Detailed Surgical Anatomy and Biomechanics
Fellows, before any incision is made, a masterful, three-dimensional understanding of the regional anatomy is paramount. This procedure demands absolute precision to achieve the desired biomechanical correction and, more importantly, to avoid devastating iatrogenic injury. The medial approach to the proximal tibia requires meticulous navigation through several distinct anatomical layers. Superficially, the saphenous nerve and its accompanying vein course along the medial aspect of the knee, providing sensation to the anteromedial leg. These structures are highly vulnerable during the initial skin incision and superficial fascial dissection; iatrogenic neuroma formation here is a notorious cause of persistent postoperative pain.
Deep to the subcutaneous tissues, the pes anserine tendons (sartorius, gracilis, and semitendinosus) insert on the anteromedial tibia. The gracilis and semitendinosus lie deep to the sartorius fascia and must be meticulously identified, mobilized, and protected with a retractor. Directly deep to the pes anserinus lies the superficial medial collateral ligament (sMCL). The sMCL is a robust, broad structure that firmly attaches to the proximal tibia. A critical step in the opening wedge HTO is the meticulous subperiosteal release of the distal sMCL fibers from the tibia. Failure to adequately release the sMCL will tether the medial compartment, preventing the osteotomy from opening symmetrically and drastically increasing the risk of a lateral hinge fracture during the correction phase.


The posterior and lateral neurovascular structures represent the "danger zones" of this procedure. Directly posterior to the proximal tibia, separated only by the popliteus muscle and a thin layer of periosteum, lie the popliteal artery and the tibial nerve. Aggressive posterior penetration with a saw blade, drill bit, or osteotome can lead to catastrophic limb-threatening hemorrhage or permanent neuropathy. Laterally, the common peroneal nerve wraps around the fibular neck. While primarily at risk during lateral closing wedge procedures, excessive manipulation or over-penetration of guide pins during a medial opening wedge can still compromise this nerve. Furthermore, the anterior tibial artery branches from the popliteal artery and passes anteriorly through the interosseous membrane; rogue screws directed too far laterally and distally can impale this vessel.
The Osteology of the Proximal Tibia
A critical anatomical detail that frequently confounds less experienced surgeons is the cross-sectional geometry of the proximal tibia. At the level of the osteotomy, the tibia is not a perfect cylinder, but rather a distinct triangle. The apex of this triangle is the tibial tubercle anteriorly, while the broad base is formed by the posterior tibial cortex. This geometric reality has profound implications for the execution of the osteotomy. If a surgeon makes a perfectly parallel cut anteriorly and posteriorly and opens the wedge uniformly, they will inadvertently increase the posterior tibial slope.
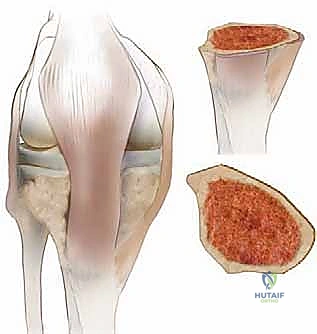

To maintain the native sagittal slope, the anterior portion of the osteotomy must be opened significantly less than the posterior portion—typically, the anterior gap should be approximately one-half to one-third the height of the posterior gap. Visualizing the cut is essential: imagine impacting a wedge into a triangular block. If the wedge is placed parallel to the base on one side, it will not touch the superior aspect evenly. Therefore, when impacting osteotomes or a calibrated spreader, the instrument must be driven deeper posteriorly than anteriorly. This prevents unintended deviations from the meticulously calculated preoperative plan.
Biomechanics of the Sagittal Plane
Beyond coronal plane realignment, the high tibial osteotomy provides a powerful mechanism to subtly alter the sagittal slope of the tibia, which is a critical determinant of dynamic knee stability. The native posterior tibial slope typically ranges from 7 to 10 degrees. Altering this slope directly impacts the resting tension and dynamic strain on the cruciate ligaments. By deliberately increasing the anterior opening of the wedge relative to the posterior opening, the surgeon can decrease the posterior tibial slope.

Decreasing the slope flattens the tibial plateau, which biomechanically reduces anterior tibial translation under axial load. This is highly advantageous in patients with chronic anterior cruciate ligament (ACL) deficiency, as it protects a concurrent or future ACL reconstruction. Conversely, intentionally increasing the posterior tibial slope (by opening the posterior aspect of the wedge significantly more than the anterior) decreases posterior tibial translation. This maneuver is specifically utilized to aid patients with posterior cruciate ligament (PCL) deficiency. A surgical warning must be strictly heeded: unknowingly increasing the tibial slope in an ACL-deficient knee will paradoxically worsen the patient's instability, highlighting the absolute necessity of rigorous, multi-planar preoperative planning.
Exhaustive Indications and Contraindications
The success of a proximal tibial opening wedge osteotomy is inextricably linked to meticulous patient selection. The procedure is not a panacea for all knee pain; rather, it is a highly specific intervention designed for a well-defined subset of pathologies. The "ideal" candidate is typically a physiologically young (under 60 years of age), highly active, non-obese patient suffering from unicompartmental medial knee pain that correlates directly with a demonstrable varus mechanical axis deviation. These patients must possess an intact lateral compartment and a functional patellofemoral joint to absorb the transferred load.
The classic indication is malalignment with isolated medial compartment arthrosis. These patients present with varus malalignment and symptomatic medial joint space narrowing, having failed exhaustive conservative measures including physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular injections. Another critical indication is malalignment combined with dynamic instability. Patients exhibiting a significant varus thrust during the stance phase of gait, particularly in conjunction with ACL or posterolateral corner (PLC) injuries, require an HTO to neutralize the deforming forces. Correcting the alignment is absolutely crucial to protect subsequent or concurrent soft-tissue reconstructions from excessive strain and catastrophic failure.


Furthermore, HTO is increasingly indicated as a mandatory adjunct for cartilage restoration procedures in the medial compartment. When performing autologous chondrocyte implantation (ACI), microfracture, or osteochondral grafting, it is paramount to create a mechanically favorable environment. If a focal chondral defect is repaired but the limb remains in varus, the relentless compressive forces will rapidly destroy the delicate graft. Offloading the newly repaired tissue by shifting the mechanical axis laterally significantly improves the graft's chances of successful integration and long-term survivorship.
Conversely, contraindications must be respected to avoid predictable clinical failures. Advanced age coupled with low functional demands generally points toward total knee arthroplasty (TKA) as a more reliable, definitive solution. Tricompartmental osteoarthritis, or significant degeneration of the contralateral (lateral) compartment, is an absolute contraindication; shifting the mechanical load into an already compromised lateral compartment will merely trade medial pain for lateral pain and accelerate global joint destruction. Inflammatory arthritides, such as rheumatoid arthritis, are also contraindications due to the systemic, progressive nature of the disease and the high likelihood of eventual pan-articular involvement.
| Parameter | Indications for Opening Wedge HTO | Contraindications for Opening Wedge HTO |
|---|---|---|
| Patient Profile | Physiologically young, highly active, non-obese | Advanced age (>65), low demand, severe obesity (BMI >35) |
| Arthrosis Status | Isolated medial compartment OA (Kellgren-Lawrence I-III) | Tricompartmental OA, severe lateral compartment OA |
| Ligamentous Status | Varus thrust, ACL/PCL/PLC deficiency requiring protection | Severe, uncorrectable multi-ligamentous instability without planned reconstruction |
| Joint Mobility | Arc of motion >90 degrees, flexion contracture <10 degrees | Stiff knee (Arc of motion <70 degrees), severe flexion contracture (>15 degrees) |
| Patellofemoral Joint | Asymptomatic or mild, non-limiting PFJ changes | Severe, highly symptomatic patellofemoral degenerative disease |
| Systemic Disease | Healthy bone stock, normal inflammatory markers | Inflammatory arthritides (e.g., Rheumatoid Arthritis), active infection, heavy smoking |
Pre-Operative Planning, Templating, and Patient Positioning
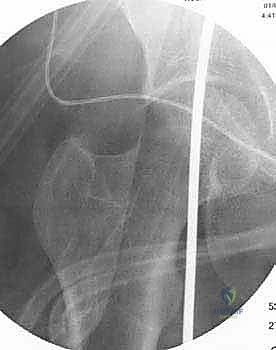
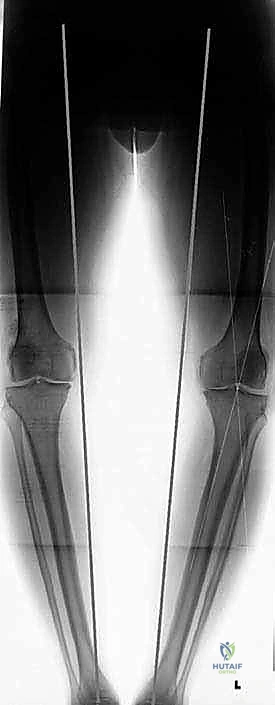
The hallmark of a masterfully executed high tibial osteotomy is rigorous, uncompromising preoperative planning. The margin for error is measured in millimeters and single degrees; thus, "eyeballing" the correction intraoperatively is an unacceptable practice. Planning begins with the acquisition of high-quality, standardized radiographs. The foundational image is the bilateral standing, full-length, hip-to-ankle anteroposterior (AP) radiograph. This long-leg cassette allows for the precise calculation of the mechanical axis of the lower extremity, defined by a line drawn from the center of the femoral head to the center of the tibiotalar joint.




In addition to the long-leg views, standard knee series must be obtained, including AP, lateral, and Merchant views. Crucially, Bilateral Posteroanterior (PA) 45-degree Flexed Views (the Rosenberg View) are mandatory. The Rosenberg view is highly sensitive for detecting posterior condylar joint space narrowing, which is frequently missed on standard extension AP views. Flexing the knee to 45 degrees provides a tangential view of the weight-bearing zone of the femoral condyles, often revealing advanced arthritic changes that might otherwise alter the surgical plan or contraindicate the procedure entirely.
Once the imaging is secured, templating is performed using either traditional acetate overlays or, more commonly, advanced digital orthopedic software. The goal is to calculate the precise wedge opening required to shift the mechanical weight-bearing line (WBL) to the desired coordinate on the tibial plateau. For isolated medial OA, the target WBL is typically the "Fujisawa point," located at 62.5% of the tibial width (measured from medial to lateral). Using the Miniaci method, a hinge point is selected at the lateral tibial cortex, and the angle subtended by the current mechanical axis and the planned mechanical axis dictates the exact millimeter opening required at the medial cortex.



Patient positioning in the operating theater must facilitate both surgical access and unobstructed fluoroscopic imaging. The patient is placed supine on a radiolucent operating table. A lateral post or sandbag is positioned to allow the knee to rest comfortably in approximately 30 to 40 degrees of flexion, which relaxes the posterior neurovascular structures and moves them further away from the osteotomy site. A sterile tourniquet is applied to the proximal thigh. The C-arm fluoroscope must be positioned on the contralateral side, draped sterilely, and tested prior to incision to ensure perfect AP and lateral views of the proximal tibia can be obtained without adjusting the patient's leg.
Step-by-Step Surgical Approach and Fixation Technique
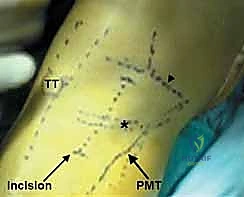
The surgical execution of the opening wedge HTO requires a methodical, step-wise approach, balancing aggressive correction with meticulous soft-tissue handling. An oblique or longitudinal incision is made over the anteromedial aspect of the proximal tibia, starting just distal to the joint line and extending distally for approximately 6 to 8 centimeters. The subcutaneous tissue is bluntly dissected to identify the sartorial fascia. The pes anserine tendons are identified, carefully mobilized, and retracted distally and posteriorly using a blunt Hohmann retractor.
The superficial medial collateral ligament (sMCL) is then exposed. Using electrocautery or a periosteal elevator, the tibial insertion of the sMCL is sharply released from the posteromedial crest of the tibia. This release must extend distally enough to allow the osteotomy to open without tethering, typically 4 to 5 centimeters distal to the joint line. A radiolucent retractor is then carefully passed subperiosteally along the posterior cortex of the tibia to protect the neurovascular bundle. This retractor must remain in constant contact with the bone to prevent the popliteal vessels from slipping anteriorly into the path of the saw blade.



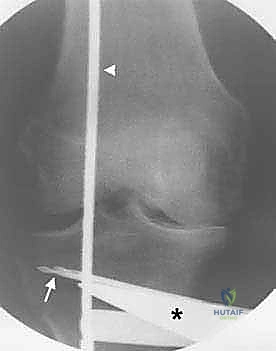
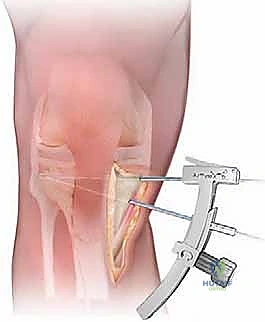
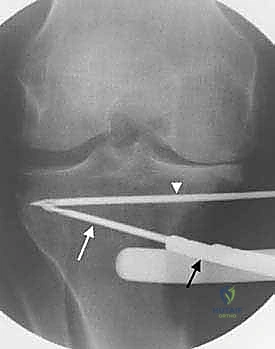
Under strict fluoroscopic guidance, a guide pin is introduced at the medial cortex, approximately 4 centimeters distal to the medial joint line. The pin is directed obliquely toward the lateral hinge point, which is ideally located at the superior tip of the proximal tibiofibular joint, leaving a 10 to 15-millimeter bridge of intact lateral cortical bone. A second guide pin is often placed parallel to the first to dictate the cutting plane. An oscillating saw is then used to cut the medial, posterior, and anterior cortices just inferior to the guide pins. The cut is typically biplanar; the primary horizontal cut is stopped short of the anterior tibial tubercle, and an ascending vertical cut is made behind the tubercle to preserve the extensor mechanism's attachment.


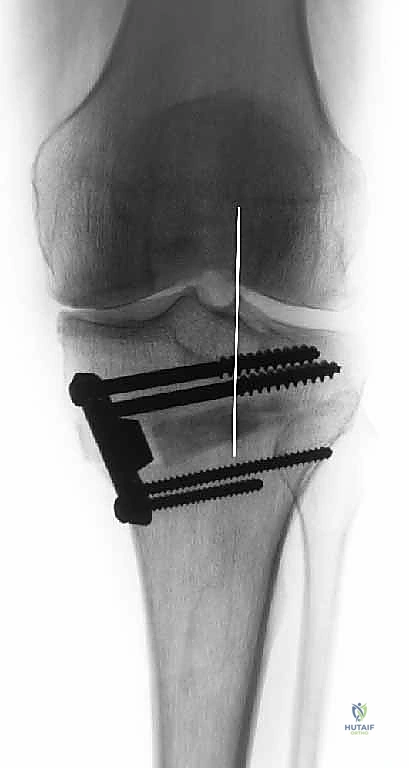
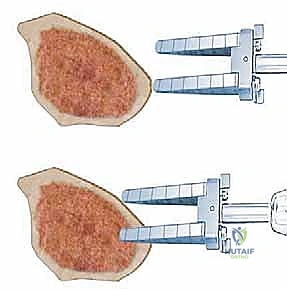
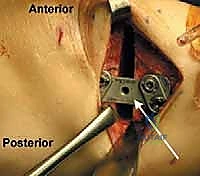
Once the cortices are breached, stacked osteotomes or a calibrated mechanical spreader are inserted into the osteotomy site. The wedge is opened gradually, millimeter by millimeter, allowing the lateral cortical hinge to undergo plastic deformation rather than catastrophic brittle fracture. The surgeon must constantly monitor the anterior and posterior gap distances, applying the "triangular tibia" rule to maintain the desired sagittal slope. Once the pre-calculated gap height is achieved, an alignment rod is used fluoroscopically to confirm that the mechanical axis has been successfully translated to the Fujisawa point.


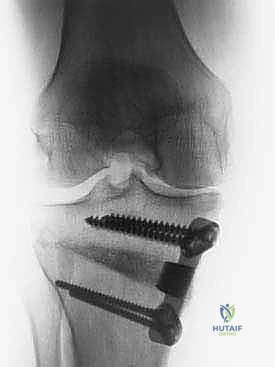
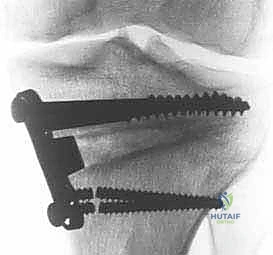
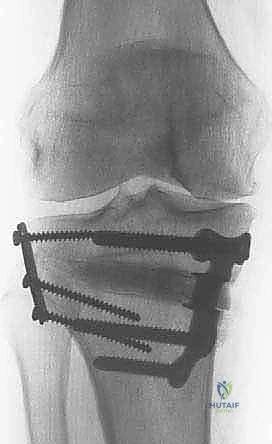
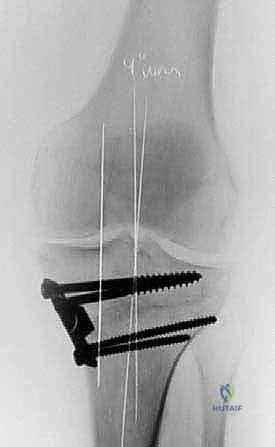
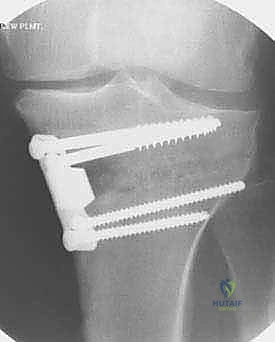
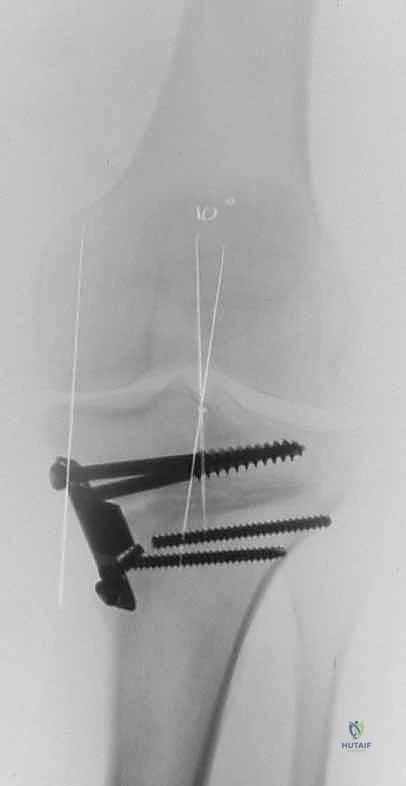
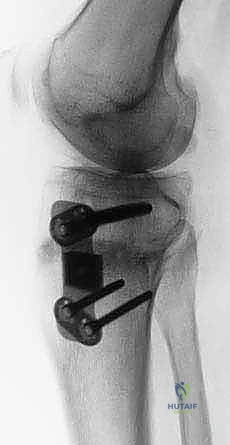
Rigid internal fixation is immediately applied to secure the correction. Modern techniques heavily favor anatomically contoured, rigid locking plate systems (e.g., TomoFix). The plate is positioned over the anteromedial tibia, and locking screws are sequentially placed into the proximal and distal fragments. Depending on the size of the gap (typically those exceeding 10-12 millimeters) and patient biology, the void may be grafted. Options include structural allograft wedges, cancellous autograft harvested from the iliac crest, or synthetic osteoconductive bone substitutes. The wound is then copiously irrigated and closed in layers over a suction drain.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the opening wedge HTO carries a distinct complication profile that the orthopedic surgeon must be prepared to manage. The most frequent intraoperative complication is a fracture of the lateral cortical hinge, occurring in up to 10-15% of cases. Takeuchi et al. classified these fractures into three types, with Type I (fracture extending into the joint) and Type II (fracture extending distally into the lateral cortex) being the most problematic. If a lateral hinge fracture is recognized intraoperatively, the surgeon must immediately alter the fixation strategy. This typically requires the placement of a lateral lag screw or a secondary lateral neutralization plate to prevent postoperative loss of correction and varus collapse.
Nonunion and delayed union represent significant postoperative hurdles, particularly in patients with poor biology, smokers, or those with massive correction gaps (>15mm) left ungrafted. The incidence of nonunion ranges from 1% to 4%. Patients presenting with persistent pain at the osteotomy site beyond 4 to 6 months, coupled with radiographic evidence of a persistent radiolucent line or hardware failure, require aggressive intervention. Salvage management for aseptic nonunion typically involves revision surgery, exchange to a more robust fixation construct, and the addition of copious autologous bone graft (iliac crest or reamer-irrigator-aspirator harvest) to stimulate osteogenesis.

Neurovascular injuries are rare but potentially devastating. Popliteal artery laceration is the most feared complication, emphasizing the absolute necessity of the posterior retractor. If arterial injury is suspected (evidenced by pulsatile bleeding or loss of distal pulses), immediate vascular surgery consultation and exploration are mandatory. More commonly, patients may experience neuropraxia or neuroma formation of the saphenous nerve due to surgical retraction or entrapment in scar tissue. This is often self-limiting but may require neuropathic pain modulators or, rarely, surgical neurolysis if conservative measures fail.
Infection, both superficial and deep, occurs in approximately 2-5% of cases. Superficial wound dehiscence or cellulitis can often be managed with oral antibiotics and local wound care. However, a deep peri-prosthetic infection necessitates a formal return to the operating room for irrigation and debridement. If the osteotomy is healed, the hardware should be removed. If the osteotomy is not healed, the surgeon faces a complex dilemma: retain the hardware and attempt suppressive intravenous antibiotics, or remove the hardware, place an antibiotic spacer or external fixator, and stage the reconstruction.
| Complication | Estimated Incidence | Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Lateral Hinge Fracture | 10% - 15% | Aggressive wedge opening, poor hinge position, dense cortical bone | Intraoperative: Lateral lag screw or lateral neutralization plate. Postop: NWB, close radiographic monitoring. |
| Delayed Union / Nonunion | 1% - 4% | Smoking, large gaps (>12mm) without graft, thermal necrosis from saw | Revision rigid fixation, autologous bone grafting (ICBG), bone stimulator. |
| Loss of Correction | 2% - 5% | Unrecognized hinge fracture, early weight-bearing, inadequate plate strength | Revision osteotomy if symptomatic; conversion to TKA if concurrent severe joint degeneration exists. |
| Saphenous Neuritis | 5% - 10% | Aggressive superficial retraction, transverse skin incisions | Gabapentinoids, local corticosteroid injections, surgical neurolysis/excision for refractory neuromas. |
| Deep Infection | 1% - 3% | Diabetes, obesity, prolonged operative time | I&D, targeted IV antibiotics. Hardware retention if unhealed; hardware removal if united. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a high tibial osteotomy is as critical to the final outcome as the surgical execution itself. The protocol must delicately balance the mechanical protection of the healing osteotomy with the biological necessity of early joint mobilization to prevent arthrofibrosis. Phase I (Weeks 0-6) focuses on protection and early motion. Depending on the rigidity of the fixation construct and the presence of a lateral hinge fracture, weight-bearing is typically restricted. Most modern protocols utilizing rigid locking plates allow for toe-touch weight-bearing (TTWB, approx. 20 lbs) immediately postoperatively. Continuous passive motion (CPM) or early active-assisted range of motion (ROM) is initiated on postoperative day one, with a goal of achieving 90 degrees of flexion by week two and full extension immediately.