Dynamic Posterior Tibial Tendon Transfer for Foot Drop: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through the Posterior Tibial Tendon (PTT) transfer for foot drop. We meticulously cover patient selection, preoperative planning, and detailed intraoperative execution, including Achilles lengthening and PTT harvest. Emphasis is placed on comprehensive surgical anatomy, neurovascular protection, and precise tendon anchoring techniques. We discuss critical pearls and pitfalls, ensuring a thorough understanding of this complex reconstructive procedure for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive exploration of a highly specialized reconstructive procedure. Today, we are undertaking a comprehensive, intraoperative masterclass on the dynamic Posterior Tibial Tendon (PTT) transfer for the correction of foot drop. This procedure represents a challenging yet incredibly rewarding intersection of biomechanics, precise anatomical dissection, and functional rehabilitation. The operation aims to restore active dorsiflexion and balanced hindfoot eversion in patients suffering from the debilitating effects of a flaccid equinovarus deformity, transforming a rigid, dysfunctional appendage into a dynamic, plantigrade foot.



Foot drop is fundamentally defined by a profound loss of ankle dorsiflexion, frequently accompanied by a deficit in hindfoot eversion depending on the exact level of the neurological lesion. This pathology is most commonly secondary to common peroneal nerve palsy, often occurring at the fibular head due to trauma, iatrogenic injury, or external compression. However, the etiology can be far more proximal or systemic, encompassing L5 radiculopathy, severe sciatic nerve injury, cerebrovascular accidents (CVA), or progressive neuropathies such as Charcot-Marie-Tooth (CMT) disease. Regardless of the origin, the resulting muscular imbalance leads to a predictable and devastating cascade of biomechanical failures during the gait cycle.
Clinically, this manifests as a characteristic "slap foot" gait during initial contact, where the eccentric control of the dorsiflexors is lost, allowing the forefoot to strike the ground abruptly. During the swing phase, the patient exhibits a "steppage gait," necessitating exaggerated hip and knee flexion to clear the plantarflexed toes and prevent tripping. Over time, the unopposed pull of the robust gastrocnemius-soleus complex and the intact posterior tibial tendon drives the foot into a fixed equinovarus contracture. The psychological and energetic toll on the patient is immense, as walking becomes a conscious, exhausting effort fraught with the constant risk of falls.
Our ultimate surgical objective is to create a dynamic, functional transfer, not merely a static tenodesis. A tenodesis simply tethers the foot to prevent plantarflexion, but a dynamic transfer aims to restore active, voluntary motion. This ambitious goal mandates an intact and robust tibial nerve and, consequently, retained, high-grade PTT function. The procedure requires the patient's central nervous system to eventually undergo "phase conversion," learning to fire a native stance-phase muscle (the PTT) during the swing phase of gait. This masterclass will guide you through the meticulous surgical steps required to set the stage for this remarkable biomechanical adaptation.


Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a profound three-dimensional understanding of the lower extremity's compartmental anatomy is non-negotiable. The success of a dynamic PTT transfer relies entirely on navigating the intricate neurovascular geography of the leg and foot. The tibial nerve is the lifeline of this operation. Crucially, its function must be completely spared and intact, as it powers the deep posterior compartment muscles, including our donor workhorse, the PTT, as well as the superficial posterior compartment housing the gastrocnemius-soleus complex.

Conversely, the common peroneal nerve is the source of the deficit. Palsy of this nerve leads to a flaccid paralysis of the anterior compartment (tibialis anterior, extensor hallucis longus, extensor digitorum longus) and the lateral compartment (peroneus longus, peroneus brevis). The deep peroneal nerve, a major branch, courses distally between the tibialis anterior and extensor hallucis longus tendons, eventually resting directly on the dorsum of the midfoot, immediately deep to the extensor hallucis brevis. This nerve, along with the anterior tibial artery, forms the anterior neurovascular bundle, a structure at extreme risk during the creation of the interosseous window and the subsequent passage of the transferred tendon.
The Posterior Tibial Tendon (PTT) itself originates broadly on the posterior surface of the tibia, the posterior aspect of the interosseous membrane, and the medial fibula. It courses distally in the deep posterior compartment, transitioning into a robust tendon that passes directly posterior to the medial malleolus within its own synovial sheath. Its primary insertion is on the medial navicular tuberosity, but it sends crucial plantar slips to the cuneiforms, cuboid, and the bases of the second through fourth metatarsals. In its native state, it is the primary inverter of the hindfoot and a secondary ankle plantarflexor. By systematically harvesting and rerouting this tendon to the dorsum of the foot, we are fundamentally altering its moment arm, converting it into a primary dorsiflexor and everter.



The Interosseous Membrane (IOM) is a thick, obliquely oriented fibrous band connecting the tibia and fibula. The distal aspect of this membrane, blending into the tibiofibular syndesmosis, is narrow and unyielding. Creating a window through the IOM for tendon passage requires absolute precision. The window must be large enough to allow the PTT to glide without friction or impingement, yet carefully positioned to avoid catastrophic injury to the anterior neurovascular bundle lying directly on its anterior surface, or the peroneal artery branches coursing posteriorly. Furthermore, upon reaching the dorsum of the foot, the transferred tendon must be routed deep to the inferior extensor retinaculum to prevent biomechanical bowstringing and ensure an effective vector of pull for dorsiflexion.
Exhaustive Indications and Contraindications
The decision to proceed with a dynamic PTT transfer is not to be taken lightly; it requires a meticulous patient selection process. The absolute primary indication is a permanent, irreversible loss of active ankle dorsiflexion (foot drop) secondary to an isolated lower motor neuron lesion, most frequently a common peroneal nerve palsy. However, timing is the critical variable. Tendon transfers are strictly contraindicated until spontaneous recovery of nerve function has been definitively ruled out. In our institution, we mandate a minimum observation period of 12 to 18 months following the initial neurological insult. Serial clinical examinations must be corroborated by comprehensive electrodiagnostic studies (EMG/NCS) demonstrating a complete lack of reinnervation potentials in the anterior and lateral compartments.

Equally important is the rigorous assessment of the donor muscle. The PTT must demonstrate full 5/5 Medical Research Council (MRC) grade strength. It is a fundamental biomechanical rule of tendon transfers that a donor muscle will lose at least one full grade of strength following transposition due to the alteration of its native resting length and vector. Therefore, a PTT that is initially graded at 4/5 will likely degrade to a 3/5 postoperatively, resulting in a weak transfer that functions merely as a static tenodesis rather than providing dynamic, active swing-phase clearance. If the tibial nerve is also compromised, the procedure is strongly contraindicated.
The status of the foot and ankle joints is another paramount consideration. The joints must be supple and passively correctable to a neutral or slightly dorsiflexed position. A flexible equinovarus deformity is an ideal scenario, as the transfer will simultaneously restore dorsiflexion and rebalance the hindfoot. Conversely, a rigid, fixed deformity is a relative contraindication to an isolated tendon transfer. If a severe, unyielding equinus or varus contracture is present, the transfer will be placed under excessive, non-physiologic tension and will inevitably fail. In such cases, the fixed deformity must be addressed concurrently or in a staged fashion through aggressive soft tissue releases (e.g., Tendo Achilles Lengthening) or corrective bony osteotomies and arthrodeses.
| Category | Specific Clinical Parameters | Rationale / Surgical Implication |
|---|---|---|
| Absolute Indications | Irreversible common peroneal nerve palsy (>12-18 months post-injury); 5/5 PTT strength; Supple, passively correctable joints. | Ensures donor capability and prevents transfer failure due to opposing rigid contractures. |
| Relative Indications | Mild, flexible equinus contracture; Concomitant claw toe deformities. | Requires concurrent procedures (e.g., TAL, flexor tenotomies) to ensure success of the primary transfer. |
| Absolute Contraindications | Spasticity (e.g., cerebral palsy, upper motor neuron lesions); PTT strength < 5/5; Severe rigid arthritis of the midfoot/hindfoot. | Spasticity leads to unpredictable phase conversion; Weak donor results in failure; Rigid arthritis prevents necessary excursion. |
| Relative Contraindications | Pre-existing severe pes planovalgus (flatfoot); Significant sensory neuropathy (e.g., advanced diabetic neuropathy). | Harvesting the PTT in a flatfoot will exacerbate the deformity; Neuropathy impairs rehabilitation and phase conversion. |
Pre-Operative Planning, Templating, and Patient Positioning
The blueprint for a successful dynamic PTT transfer is drawn long before the patient enters the operating room. Preoperative planning begins with a highly detailed clinical examination focused on differentiating flexible from fixed deformities. The Silfverskiold test is mandatory. By assessing ankle dorsiflexion with the knee fully extended (tensioning the gastrocnemius) and then flexed (relaxing the gastrocnemius and isolating the soleus), we can precisely determine the anatomical source of any equinus contracture. If equinus persists in both positions, a combined gastrocnemius-soleus contracture exists, necessitating a formal Tendo Achilles Lengthening (TAL). If the equinus resolves with knee flexion, a selective gastrocnemius recession (Strayer procedure) is indicated.



Imaging studies, while sometimes secondary to the clinical exam in isolated nerve palsies, are critical for ruling out confounding pathologies. Weight-bearing anteroposterior, lateral, and mortise radiographs of the foot and ankle are scrutinized for occult degenerative joint disease, rigid bony deformities, or prior trauma that might impede the excursion of the transferred tendon. In cases where the etiology of the nerve palsy is ambiguous, or if there is clinical suspicion of a compressive lesion at the fibular head or within the lumbar spine, Magnetic Resonance Imaging (MRI) is obtained. MRI can also be utilized to evaluate the cross-sectional area and fatty infiltration of the PTT muscle belly, providing a morphological correlate to the clinical strength assessment.
Patient positioning and anesthetic management are critical intraoperative variables. The procedure is performed under general anesthesia, and we absolutely insist on complete, profound neuromuscular blockade (paralysis) throughout the critical tensioning phases of the operation. Any residual intrinsic muscle tone will artificially alter the resting tension of the foot, leading to disastrous under-tensioning or over-tensioning of the transferred tendon. The patient is positioned supine on the operating table.



We routinely place a substantial bolster under the ipsilateral hip. This internal rotation of the lower extremity provides optimal exposure to the lateral aspect of the leg, which is essential for safely creating the interosseous window and retrieving the tendon into the anterior compartment. A well-padded thigh tourniquet is applied and, following meticulous exsanguination with an Esmarch bandage, inflated to 300-350 mmHg. A completely bloodless surgical field is not a luxury here; it is a strict requirement for identifying the delicate, life-sustaining neurovascular structures adjacent to the interosseous membrane and the dorsum of the foot.
Step-by-Step Surgical Approach and Fixation Technique
Addressing the Equinus Contracture
The surgical journey commences by ensuring the foundation is level. If the preoperative Silfverskiold test indicated a fixed equinus contracture, we must address it immediately. Attempting to tension a dorsiflexion transfer against a tight Achilles tendon is a guaranteed recipe for failure. Depending on the severity and specific muscle involvement, we perform either a gastrocnemius recession or a formal Tendo Achilles Lengthening (TAL).


For a global gastrocnemius-soleus contracture, we utilize the Hoke triple hemisection technique. We make three small, staggered transverse incisions—approximately 1 to 2 centimeters in length—along the medial aspect of the Achilles tendon. Through the proximal incision, a blunt instrument is used to hemisect the anterior half of the tendon. The middle incision allows for a posterior hemisection, and the distal incision mirrors the proximal anterior cut. By gently but firmly dorsiflexing the ankle, the tendon fibers slide and lengthen with a palpable, satisfying "give." The absolute goal is to achieve neutral to 5 degrees of dorsiflexion. We must exercise extreme caution; over-lengthening the Achilles will result in a devastating, iatrogenic calcaneus gait that is functionally far worse than the initial foot drop.
Posterior Tibial Tendon (PTT) Harvest
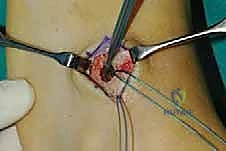
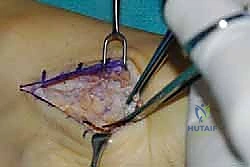
With the ankle now supple, we turn our attention to harvesting the donor tendon. We employ a multi-incision technique to minimize soft tissue morbidity and preserve the paratenon where possible. The first incision is made distally, a 4-centimeter longitudinal approach directly over the medial navicular tuberosity, following the medial border of the midfoot. Dissection is carried down through the subcutaneous tissues to identify the thick, glistening PTT sheath.



The sheath is incised longitudinally. Here, the anatomical complexity of the PTT insertion is revealed. It does not merely attach to the navicular; it sends robust plantar slips to the spring ligament, the cuneiforms, and the metatarsal bases. To maximize the excursion and length of our graft, we must meticulously dissect and release these plantar extensions. Using a combination of sharp dissection and a periosteal elevator, the tendon is sharply detached from its bony insertions. A heavy, non-absorbable locking whipstitch (e.g., #2 FiberWire or similar high-tensile suture) is immediately placed into the distal stump of the harvested tendon to secure control and facilitate subsequent passage.
Proximal Dissection and Interosseous Routing
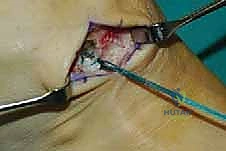
The next phase requires retrieving the tendon into the proximal leg. A second longitudinal incision, approximately 5 centimeters long, is made on the medial aspect of the distal third of the calf, roughly 10 to 15 centimeters proximal to the medial malleolus, lying just posterior to the medial border of the tibia. Dissection proceeds through the deep fascia to enter the deep posterior compartment. The PTT muscle belly and tendon are identified. By applying gentle traction to the distal whipstitch, the tendon is identified proximally and carefully pulled out of its retromalleolar sheath into the medial calf wound.


Now, we must create the critical pathway for transfer: the interosseous window. A third incision is made on the anterolateral aspect of the leg, at the same proximal-distal level as the medial calf incision. Dissection is carried down between the tibialis anterior and the extensor digitorum longus to expose the anterior surface of the interosseous membrane. This is the most dangerous step of the procedure. The anterior tibial artery and deep peroneal nerve lie intimately against the anterior aspect of the IOM. Using a blunt curved clamp or a specialized tendon passing instrument, a large, generous window (at least 3-4 centimeters in length) is bluntly created through the membrane from anterior to posterior, staying as close to the fibula as safely possible to avoid the neurovascular bundle.



The passing instrument is advanced through the window into the medial calf incision. The whipstitch of the PTT is grasped, and the tendon is smoothly drawn through the interosseous membrane into the anterior compartment. It is imperative to ensure that the muscle belly itself, not just the tendon, sits within the window to prevent postoperative scarring, adhesions, and tethering that would destroy the dynamic nature of the transfer. The tendon should glide effortlessly when pulled.
Distal Fixation and Precise Tensioning
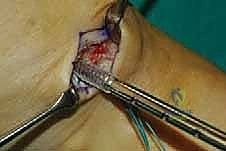
The final and most critical phase is fixation and tensioning. A fourth incision is made over the dorsum of the midfoot, centered over the lateral cuneiform. The lateral cuneiform is the preferred target for fixation as it provides an optimal vector to restore both dorsiflexion and balanced eversion, counteracting the inherent varus tendency of the foot drop. Dissection is carried down to the bone, carefully protecting the superficial peroneal nerve branches and the dorsalis pedis artery. The inferior extensor retinaculum is identified.



A subcutaneous tunnel is created from the anterolateral leg incision down to the dorsal midfoot incision. Crucially, the tendon passing instrument must be routed deep to the inferior extensor retinaculum. The PTT is then passed distally. Passing the tendon deep to the retinaculum prevents catastrophic bowstringing across the ankle joint, ensuring the mechanical advantage is directed towards lifting the foot rather than lifting the skin.



For fixation, we utilize a robust bio-tenodesis or interference screw system. A guide pin is placed centrally into the lateral cuneiform, and a blind tunnel is reamed to the appropriate diameter matching the harvested PTT (typically 6.0 to 8.0 mm). The tendon is drawn into the tunnel. Now comes the moment of truth: tensioning. The ankle is held in maximal achievable dorsiflexion (typically 10 to 15 degrees past neutral), and the hindfoot is held in slight eversion. While maintaining this absolute maximal tension, the interference screw is deployed into the osseous tunnel, locking the tendon securely against the cortical and cancellous bone. The tension must be uncomfortably tight; the natural tendency of all tendon transfers is to stretch and relax postoperatively. If it looks "just right" on the table, it will be too loose in six months.



Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the dynamic PTT transfer is fraught with potential complications, primarily related to biomechanical failure or neurovascular compromise. The most common cause of functional failure is incorrect tensioning.
Clinical & Radiographic Imaging Archive