ABOS Part I Orthopaedic Surgery Board Review: CECS & MTP Joint Instability Questions | Part 22150
Key Takeaway
This module offers 20 advanced multiple-choice questions mirroring the ABOS Part I and AAOS OITE examinations. It covers high-yield clinical teaching cases, focusing on Chronic Exertional Compartment Syndrome (CECS) and Second MTP Joint Instability, including diagnosis, surgical management, and rehabilitation protocols for orthopaedic residents and practitioners.
ABOS Part I Orthopaedic Surgery Board Review: CECS & MTP Joint Instability Questions | Part 22150
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male long-distance runner presents with a 6-month history of bilateral lower leg pain. The pain is described as a deep, aching tightness in the posteromedial calf, which consistently begins after approximately 15 minutes of running and progressively worsens, forcing him to stop. The pain resolves completely within 10-15 minutes of rest. He denies any numbness or tingling. Physical examination reveals tenderness along the posteromedial tibia, but no palpable mass or crepitus. Dorsiflexion and plantarflexion are full and pain-free at rest. Radiographs are negative for stress fracture. He has tried activity modification, orthotics, and physical therapy without significant improvement. Given this presentation, which of the following is the MOST likely diagnosis?
Explanation
Correct Answer: C
The patient's symptoms are classic for Chronic Exertional Compartment Syndrome (CECS), specifically involving the deep posterior compartment. The key features are exercise-induced pain and tightness that consistently begin after a specific duration of activity, progressively worsen, and resolve completely with rest. The location of pain (deep posteromedial calf) points to the deep posterior compartment. The failure of conservative management and negative radiographs further support this. While MTSS (A) also presents with exertional pain along the posteromedial tibia, it typically involves periostitis or bone stress and often has a more diffuse, less 'tight' quality, and may not resolve as quickly or completely with rest. A tibial stress fracture (B) would typically cause localized pain that is present at rest or with minimal activity, and would likely be visible on radiographs or bone scan. Popliteal artery entrapment syndrome (D) would present with exertional leg pain, but it is primarily vascular claudication, often described as cramping, and may be associated with diminished pulses post-exercise. Tibialis Posterior tendinopathy (E) would cause pain with specific movements (inversion, plantarflexion) and tenderness directly over the tendon, and while exertional, the 'tightness' and rapid resolution with rest are more indicative of CECS.
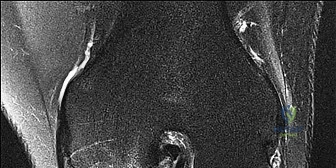
Question 2
A 35-year-old athlete is undergoing diagnostic workup for suspected deep posterior chronic exertional compartment syndrome. The image below depicts a cross-section of the lower leg. Which labeled structure represents the primary muscle responsible for dynamic arch support and is a key component of the deep posterior compartment?

Explanation
Correct Answer: B
The image shows a cross-section of the lower leg. Structure B, located deep in the posterior compartment and originating from the interosseous membrane and posterior surfaces of the tibia and fibula, represents the Tibialis Posterior muscle. The case description explicitly states that the Tibialis Posterior is the primary inverter and plantarflexor of the foot, essential for dynamic arch support. Structure A is likely the Flexor Digitorum Longus, C is the Flexor Hallucis Longus, D is the Soleus, and E is the Gastrocnemius. While FDL and FHL are also in the deep posterior compartment, the Tibialis Posterior is specifically highlighted for its role in dynamic arch support.
Question 3
A 22-year-old collegiate soccer player presents with exertional deep posterior leg pain. Intracompartmental pressure measurements are performed during a treadmill test that reproduces his symptoms. Which of the following pressure profiles, measured in mmHg, would be diagnostic for deep posterior chronic exertional compartment syndrome (CECS) requiring surgical consideration?
Explanation
Correct Answer: B
The case outlines the standardized diagnostic criteria for CECS, which include: Resting pressure > 15 mmHg, 1-minute post-exercise pressure > 30 mmHg, and 5-minute post-exercise pressure > 20 mmHg. Option B (Resting: 18, 1-minute post-exercise: 35, 5-minutes post-exercise: 25) is the only option that meets all three of these criteria. Option A fails the 1-minute post-exercise criterion. Option C fails all three criteria. Option D fails the 1-minute post-exercise criterion. Option E fails the 5-minute post-exercise criterion. It is crucial that these measurements reproduce the patient's symptoms during the exercise provocation.
Question 4
A 32-year-old military recruit has been diagnosed with deep posterior chronic exertional compartment syndrome (CECS) based on classic symptoms and positive intracompartmental pressure measurements. He has undergone 6 months of dedicated conservative therapy, including activity modification, physical therapy, and orthotics, but continues to experience debilitating pain that prevents him from performing his duties. Which of the following is the strongest indication for proceeding with surgical fasciotomy?
Explanation
Correct Answer: C
The strongest indication for operative intervention for deep posterior CECS is the failure of non-operative management for a minimum of 3-6 months, coupled with persistent and debilitating exertional deep posterior leg pain. While patient desire (A) is important, it's not the primary medical indication. A resting pressure of 16 mmHg (B) alone is not sufficient; the dynamic post-exercise pressures are more critical for diagnosis, and the overall picture of failed conservative care is paramount for surgical indication. MRI findings of muscle edema (D) are non-specific and not diagnostic for CECS. Exclusion of other pathologies like stress fracture (E) is a necessary step in the diagnostic workup, but it is not an indication for surgery itself; rather, it confirms the diagnosis of CECS by ruling out alternatives.
Question 5
During a medial deep posterior fasciotomy, the surgeon has made the skin incision and carefully retracted the great saphenous vein and saphenous nerve. The medial gastrocnemius and soleus muscles have been retracted posteriorly and laterally. The image below shows the next critical anatomical layer encountered. Which structure, indicated by the arrow, is the primary target for surgical release in this procedure?

Explanation
Correct Answer: C
The image depicts a surgical view after retracting the soleus muscle. The arrow points to the glistening, dense fascial layer that encapsulates the deep posterior compartment muscles. This is the deep transverse crural fascia, which is the primary target for release in a deep posterior fasciotomy. The case explicitly states: 'After retracting the soleus muscle, the surgeon will visualize a glistening, dense fascial layer. This is the deep transverse crural fascia, which encloses the deep posterior compartment. This is the primary target for release.' The tibial nerve (A) and posterior tibial artery (B) lie immediately superficial to this fascia and must be carefully identified and protected, not incised. The Flexor Digitorum Longus muscle (D) is one of the muscles within the compartment, which will bulge once the fascia is released. The interosseous membrane (E) forms the anterior boundary of the deep posterior compartment and is not the structure being incised from this medial approach.
Question 6
During a medial deep posterior fasciotomy for chronic exertional compartment syndrome, meticulous dissection is crucial to protect vital neurovascular structures. Which of the following statements accurately describes the anatomical relationship of the tibial nerve and posterior tibial vessels relative to the deep transverse crural fascia?
Explanation
Correct Answer: C
The case explicitly states: 'Crucially, the tibial nerve and posterior tibial artery and veins lie immediately superficial to this deep transverse fascia, nestled between the soleus and the deep compartment muscles.' This anatomical relationship is critical for safe surgical technique, as the surgeon must identify and protect these structures before incising the deep transverse fascia. Options A and B are incorrect as the neurovascular bundle is not deep to or embedded within the fascia to be incised. Option D is incorrect as these structures are associated with the deep posterior compartment, not the superficial posterior compartment anterior to the gastrocnemius. Option E is incorrect as they are not located in the lateral compartment.
Question 7
A 25-year-old female undergoes an uncomplicated medial deep posterior fasciotomy for chronic exertional compartment syndrome. During her 6-week post-operative follow-up, she expresses concern about a visible bulge along the posteromedial aspect of her calf, which is soft and non-tender. She has no pain or neurological symptoms. Based on the case information, what is the most appropriate management for this finding?
Explanation
Correct Answer: C
The case lists muscle herniation as a common complication of fasciotomy, stating: 'Often unavoidable as a consequence of fascial release. Usually asymptomatic and requires no specific treatment. May cause cosmetic concern; rarely requires fascial repair (with risk of recurrence) or mesh repair for significant symptoms.' Given that the patient is asymptomatic and has no pain or neurological symptoms, reassurance is the most appropriate management. Immediate surgical repair (A) is generally not indicated for asymptomatic herniation due to the risk of recurrence and potential for re-creating compartment syndrome. MRI (B) is unnecessary if the patient is asymptomatic and there are no signs of recurrence. A compression brace (D) might be used for cosmetic concerns but is not a primary medical management for an asymptomatic herniation. Aggressive scar massage (E) is for scar management, not for reducing muscle herniation.
Question 8
A 20-year-old athlete is 3 days status post-medial deep posterior fasciotomy. The incision is clean and dry, and pain is well-controlled with oral medication. According to the immediate post-operative rehabilitation protocol outlined in the case, which of the following is the most appropriate instruction for this patient?
Explanation
Correct Answer: D
The 'Phase 1 Immediate Post-Operative (Days 0-14)' section of the rehabilitation protocol states: 'Gentle Range of Motion (ROM): Ankle plantarflexion and dorsiflexion within pain-free limits. Toe flexion and extension. Gentle ankle circumduction. No forceful stretching of the posterior compartment muscles.' Therefore, performing gentle ankle ROM is appropriate. Forceful stretching (A) is explicitly contraindicated in this phase. Light jogging (B) is part of intermediate rehabilitation (Weeks 6-12). The protocol states 'Usually immediate full weight-bearing as tolerated' (C), so strict non-weight-bearing is incorrect. Progressive resistance exercises (E) are initiated in Phase 2 (Weeks 2-6) and advanced in Phase 3 (Weeks 6-12).
Question 9
A 29-year-old professional dancer is 12 weeks post-medial deep posterior fasciotomy and is progressing well through rehabilitation. She is eager to return to full dance activities, which involve high-impact movements and agility. According to the advanced rehabilitation protocols, which of the following is a key criterion for her safe return to sport?
Explanation
Correct Answer: C
The 'Phase 4 Advanced Rehabilitation & Return to Sport (Weeks 12+)' section outlines the criteria for return to sport: 'Full pain-free ROM and strength symmetry (isokinetic testing if available). Ability to perform sport-specific drills without symptoms. Achieve pre-injury fitness levels. Psychological readiness.' Therefore, the ability to perform sport-specific drills without symptoms and achieving pre-injury strength symmetry are key criteria. Completion of 12 weeks (A) is a timeline, not a functional criterion. Absence of pain during light walking (B) is a much earlier milestone. A negative repeat intracompartmental pressure test (D) is not a standard criterion for return to sport post-fasciotomy. Subjective feeling of readiness with mild residual tightness (E) is insufficient and could lead to re-injury or recurrence.
Question 10
A 40-year-old recreational runner is considering treatment options for objectively diagnosed deep posterior chronic exertional compartment syndrome. He asks about the likelihood of success with conservative management. Based on the summary of key literature, what is the typical success rate for conservative management in patients with symptomatic, objectively diagnosed CECS?
Explanation
Correct Answer: C
The 'Summary of Key Literature / Guidelines' section explicitly states: 'Literature consistently supports an initial trial of conservative management for CECS... However, the success rate for conservative management of symptomatic, objectively diagnosed CECS (especially with pressures meeting surgical criteria) is generally low, often quoted in the range of 10-30%.' This highlights why surgical intervention is frequently necessary for definitive relief in these patients. Options A, B, and E represent high success rates, which are typically associated with surgical outcomes, not conservative management for objectively diagnosed CECS. Option D is incorrect as the literature provides a clear consensus on the low efficacy of conservative management for objectively diagnosed CECS.
Question 11
A 52-year-old female presents with chronic pain and progressive deformity of her second toe. She reports difficulty wearing shoes and a painful callosity under the second metatarsal head. Physical examination reveals dorsal subluxation of the second MTP joint and a positive vertical stress test. She has a history of hallux valgus deformity that was surgically corrected 5 years ago. Which of the following is the MOST likely primary contributing factor to her current second MTPJ instability?
Explanation
Correct Answer: C
The case explicitly states that common etiologies include 'Iatrogenic: Over-aggressive first ray surgery can lead to transfer load.' Hallux valgus correction is a common first ray surgery. In this patient's history, the prior hallux valgus surgery is a direct and highly probable cause of transfer metatarsalgia, leading to increased stress on the second MTPJ and subsequent instability. While a long second metatarsal (Morton's toe) is a known biomechanical risk factor, the vignette provides a more specific and recent iatrogenic cause. Acute trauma, inflammatory arthritis, and general degenerative changes are less likely to be the primary contributing factor given the specific history provided.
Question 12
A 48-year-old active female presents with a 6-month history of progressive pain and instability in her second MTP joint. MRI confirms a Grade 2 plantar plate tear. During surgical repair, the surgeon notes the tear is located at the proximal attachment of the plantar plate. This location is anatomically significant because the plantar plate most commonly tears where it attaches to which of the following structures?
Explanation
Correct Answer: A
The 'Surgical Anatomy & Biomechanics' section, under 'Plantar Plate,' clearly states: 'Tears most commonly occur at its proximal attachment to the metatarsal neck due to repetitive tensile and shear forces.' This proximal attachment is a critical point of vulnerability for the plantar plate, making it the most frequent site of injury in second MTPJ instability. The distal insertion is into the base of the proximal phalanx, and while the plantar plate blends with collateral ligaments, its primary tear location is at the metatarsal neck.
Question 13
A 60-year-old patient presents with a 9-month history of forefoot pain, worse with activity, and a feeling of "something shifting" in her second toe. On physical examination, the second toe is noted to be slightly dorsally elevated, and a painful callosity is present plantarly beneath the second metatarsal head. When performing the vertical stress test (Lachman test), the examiner stabilizes the metatarsal head and applies dorsal pressure to the proximal phalanx. An increase in dorsal translation compared to the adjacent toes is observed. Which of the following imaging findings would MOST directly correlate with this clinical finding and confirm the primary pathology?
Explanation
Correct Answer: C
The 'Pre-Operative Planning & Patient Positioning' section describes the Lachman Test (Vertical Stress Test) as indicating 'plantar plate insufficiency.' The text further states that 'Magnetic Resonance Imaging (MRI): The gold standard for assessing soft tissue structures, particularly the plantar plate. MRI can directly visualize plantar plate tears (most commonly at the metatarsal neck insertion), synovitis, and bone marrow edema.' Therefore, an MRI showing a significant plantar plate tear directly correlates with the positive vertical stress test and confirms the primary pathology of instability. While dorsal subluxation on a lateral radiograph is a consequence of plantar plate failure, and other radiographic findings may be associated, the MRI provides direct visualization of the soft tissue injury responsible for the instability.
Question 14
A 55-year-old female has been undergoing conservative management for second MTPJ instability for 6 months, including custom orthotics, activity modification, and NSAIDs. Despite these measures, she continues to experience debilitating pain, has developed a progressive hammer toe deformity of the second toe, and reports significant difficulty with shoe wear and daily activities. Physical examination reveals an irreducible dorsal subluxation of the second MTP joint. Which of the following is the MOST compelling indication for operative intervention in this patient?
Explanation
Correct Answer: C
The 'Indications for Operative Intervention' section lists several key criteria for surgery. The most compelling indications in this vignette are 'Irreducible dorsal subluxation or dislocation: Clinical assessment reveals a fixed or severely subluxed/dislocated MTP joint that cannot be manually reduced...' and 'Progressive deformity: Development or progression of a hammer toe/claw toe deformity directly attributable to MTPJ instability...' While persistent pain despite conservative care (Option B) is a general indication, the presence of irreducible subluxation and progressive deformity signifies a structural failure that is unlikely to respond to further non-operative measures. A painful callosity (Option A) is a symptom, not a primary indication for surgery. Patient preference (Option D) is considered but not a primary clinical indication. A Grade 1 plantar plate attenuation (Option E) typically responds to conservative management and would not warrant surgery in isolation.
Question 15
A surgeon is performing a second MTPJ plantar plate repair via a dorsal approach, as depicted in the image.
After incising the skin and subcutaneous tissue, which of the following structures must be meticulously identified and protected to prevent iatrogenic injury during the initial dissection to expose the extensor mechanism?

Explanation
Correct Answer: C
The 'Detailed Surgical Approach / Technique' section, under 'Dissection & Internervous Planes,' explicitly states: 'Meticulously identify and protect the dorsal digital nerves (medial and lateral branches of the second common digital nerve) and veins, retracting them safely.' The dorsal approach, as shown in the image, necessitates careful attention to these superficial neurovascular structures to avoid complications such as numbness, paresthesias, or painful neuromas. The other options are either located more deeply (deep transverse metatarsal ligament, flexor digitorum longus tendon, lumbrical muscles) or on the plantar aspect of the foot (plantar digital nerves), and thus are not the primary structures at risk during the initial dorsal skin and subcutaneous dissection.
Question 16
A 40-year-old male undergoes surgical repair for chronic second MTPJ instability with a significant plantar plate tear and a long second metatarsal. In addition to direct plantar plate repair, a Weil osteotomy is performed. What is the primary biomechanical purpose of performing a Weil osteotomy in this context?
Explanation
Correct Answer: C
The 'Adjunct Procedures' section, specifically under 'Weil Osteotomy,' states its purpose: 'Decompresses the MTP joint, allows easier reduction, reduces load on the metatarsal head, and can correct sagittal plane deformity.' By shortening the metatarsal, the Weil osteotomy effectively elevates the metatarsal head, thereby reducing the pressure on the plantar plate and the metatarsal head itself. This decompression is crucial for alleviating pain, promoting healing of the plantar plate repair, and preventing recurrence, especially in cases with a long second metatarsal. It does not increase plantar plate tension, lengthen the metatarsal, or directly correct PIP joint contractures (though it can help with MTPJ alignment which influences the toe's overall position). It is performed via a dorsal approach, not to facilitate a plantar approach.
Question 17
A 35-year-old dancer develops progressive second MTPJ instability. Her condition is attributed to repetitive microtrauma and biomechanical overload. Understanding the dynamic stabilizers of the MTP joint is crucial. Which of the following intrinsic muscles primarily contributes to second MTPJ stability by pulling the toe into flexion and helps maintain the plantar plate's stable fulcrum?
Explanation
Correct Answer: C
The 'Dynamic Stabilizers' section highlights the role of intrinsic foot muscles. It specifically states: 'The second lumbrical, in particular, contributes to second MTPJ stability by pulling the toe into flexion.' It further explains that when the plantar plate is compromised, these intrinsic muscles (lumbricals and interossei) 'lose their stable fulcrum,' leading to unopposed extensor pull and dorsal subluxation. The lumbricals' action of MTPJ flexion is critical for maintaining the stability of the joint and counteracting the dorsal pull of the extensor tendons. While interossei also contribute to MTPJ flexion and stability, the lumbrical is specifically mentioned for its role in second MTPJ stability.
Question 18
A 58-year-old patient undergoes a second MTPJ plantar plate repair combined with a Weil osteotomy for a long second metatarsal. Six months post-operatively, she complains of new, persistent pain under the third metatarsal head, which was not present before surgery. Physical examination confirms tenderness and a new callosity under the third metatarsal head. This complication is MOST likely due to which of the following?
Explanation
Correct Answer: B
The 'Complications & Management' section, specifically the table, addresses 'Persistent/Transfer Metatarsalgia.' It describes this as 'Pain beneath the operated metatarsal head (if inadequate shortening or insufficient plantar plate repair) or beneath an adjacent metatarsal head (transfer metatarsalgia), typically the third metatarsal, due to over-shortening of the second metatarsal (Weil osteotomy).' Over-shortening the second metatarsal shifts the weight-bearing load to the adjacent (often third) metatarsal head, leading to new pain and callosity. Inadequate shortening would lead to persistent pain under the second metatarsal, not transfer pain to the third. Recurrence of instability or neuroma would present differently.
Question 19
A 45-year-old patient is 3 weeks post-operative from a second MTPJ plantar plate repair with a Weil osteotomy and temporary K-wire fixation. The K-wire is still in place. According to the standard rehabilitation protocol described, which of the following activities is MOST appropriate for this patient at this stage?
Explanation
Correct Answer: C
The 'Post-Operative Rehabilitation Protocols' section, under 'Immediate Post-Operative Protection,' clearly states: 'Weight-Bearing: Strictly non-weight-bearing (NWB) on the operative foot.' It also emphasizes: 'Avoid any active or passive motion of the operated MTP joint or toe.' At 3 weeks post-op with a K-wire still in place, the joint and osteotomy are still healing and require protection. K-wire removal and progression to protected weight-bearing and gentle ROM typically occur at 4-6 weeks. Full weight-bearing, active MTPJ ROM, cycling with toe engagement, or aggressive stretching would be premature and risk disrupting the repair or osteotomy.
Question 20
Based on the "Summary of Key Literature / Guidelines" section, which of the following statements best reflects the current consensus regarding the surgical management of symptomatic second MTPJ instability with a significant plantar plate tear?
Explanation
Correct Answer: D
The 'Summary of Key Literature / Guidelines' section explicitly states: 'advancements in imaging, especially MRI, have confirmed the high prevalence of plantar plate tears as the primary pathology... The strong correlation between clinical instability, radiographic dorsal subluxation, and MRI-confirmed plantar plate pathology is well-established.' It also reiterates: 'MRI: The gold standard for assessing soft tissue structures, particularly the plantar plate.'
Let's evaluate the other options:
- A) Non-operative management is effective for advanced cases with irreducible subluxation: This is incorrect. The text states non-operative measures 'often fail to address the underlying structural instability in advanced cases' and that surgery is indicated for 'irreducible dorsal subluxation.'
- B) A plantar approach is preferred for direct visualization and repair of the plantar plate: This is incorrect. The text states: 'The dorsal approach is the most common, offering good visualization of the joint and allowing for concomitant procedures.'
- C) Direct plantar plate repair alone is sufficient, and concomitant Weil osteotomy is rarely indicated: This is incorrect. The text notes: 'Concomitant Weil osteotomy of the second metatarsal is frequently performed, especially in cases with a long second metatarsal or significant dorsal subluxation. It serves to shorten the metatarsal, decompress the MTPJ, and facilitate plantar plate repair.'
- E) Long-term outcomes are generally poor due to high recurrence rates and persistent pain: This is incorrect. The text states: 'The long-term outcomes of successful plantar plate repair combined with appropriate adjunct procedures show high patient satisfaction, significant pain reduction, and functional improvement, with recurrence rates ranging from 10-20%.' While recurrence can occur, overall outcomes are generally good.
Question 21
A 24-year-old female runner complains of severe right leg pain after 20 minutes of running. Intracompartmental pressures are measured. Which of the following values is diagnostic for chronic exertional compartment syndrome (CECS) according to the Pedowitz criteria?
Explanation
Question 22
A 55-year-old female presents with pain at the plantar aspect of the second metatarsophalangeal (MTP) joint and a progressive medial deviation of the second toe. This crossover toe deformity is primarily driven by the attenuation and failure of which of the following structures?
Explanation
Question 23
A 28-year-old marathon runner undergoes isolated anterior compartment fasciotomy for chronic exertional compartment syndrome. Postoperatively, he complains of new-onset numbness in the first dorsal web space of his foot and weakness in great toe extension. Which nerve was most likely injured during the procedure?
Explanation
Question 24
What is the most common complication following a standard Weil distal metatarsal shortening osteotomy performed for second MTP joint instability?
Explanation
Question 25
According to the modified Pedowitz criteria, which of the following intracompartmental pressure measurements is diagnostic for chronic exertional compartment syndrome (CECS)?
Explanation
Question 26
A 24-year-old collegiate runner is diagnosed with isolated anterior chronic exertional compartment syndrome. Before considering surgical fasciotomy, the patient is advised to alter her running biomechanics. Which of the following gait modifications is MOST likely to decrease the intracompartmental pressure in her anterior compartment?
Explanation
Question 27
A 55-year-old female presents with progressive pain and a "crossover" deformity of her second toe.
The pathoanatomy of this condition primarily involves attenuation or rupture of which of the following structures?
Explanation
Question 28
A 28-year-old military recruit undergoes an isolated lateral compartment fasciotomy for chronic exertional compartment syndrome. Postoperatively, he complains of numbness over the dorsum of his foot but has intact sensation in the first web space. Which nerve was most likely injured, and where does it typically pierce the deep fascia to become superficial?
Explanation
Question 29
A 45-year-old woman complains of forefoot pain localized to the plantar aspect of the second metatarsophalangeal (MTP) joint, describing a sensation of "walking on a marble." Which of the following physical examination maneuvers is MOST sensitive for diagnosing the suspected pathology?
Explanation
Question 30
When performing an open fasciotomy for deep posterior chronic exertional compartment syndrome via a medial approach, the incision is typically placed 1-2 cm posterior to the posteromedial border of the tibia. Which structure must be identified and protected during this approach?
Explanation
Question 31
A 60-year-old female undergoes a Weil osteotomy of the second metatarsal and a plantar plate repair for a rigid crossover toe deformity. Postoperatively, she develops a "floating toe" complication. What biomechanical consequence of the Weil osteotomy primarily contributes to this complication?
Explanation
Question 32
A 21-year-old male track athlete presents with severe bilateral calf cramping and numbness in the soles of his feet after sprinting. His resting compartment pressures are normal. Examination reveals diminished pedal pulses upon forceful active plantarflexion against resistance. What is the most appropriate next step in diagnosis?
Explanation
Question 33
A 50-year-old active female complains of second MTP joint pain. Non-weight-bearing radiographs are normal. An MRI is ordered to evaluate for a plantar plate tear.
At which anatomic location does the plantar plate most commonly tear?
Explanation
Question 34
A 30-year-old marathon runner undergoes measurement of compartment pressures for suspected chronic exertional compartment syndrome. The catheter is inserted 3 cm lateral to the tibial crest in the proximal third of the leg. Which of the following muscles is located within the compartment being tested?
Explanation
Question 35
A 24-year-old female runner complains of severe aching in her anterior legs after running 2 miles. Symptoms resolve 30 minutes after cessation of activity. Pre- and post-exercise intracompartmental pressures are measured. According to the Pedowitz criteria, which of the following resting (pre-exercise) pressure measurements is considered diagnostic for chronic exertional compartment syndrome (CECS)?
Explanation
Question 36
A 21-year-old collegiate cross-country athlete is diagnosed with anterior chronic exertional compartment syndrome (CECS). He wishes to avoid surgery. Which of the following gait modifications has been shown to decrease forces in the anterior compartment and potentially alleviate his symptoms?
Explanation
Question 37
A 45-year-old woman presents with pain at the plantar aspect of her second metatarsophalangeal (MTP) joint. She notes that her second toe has recently started to deviate medially. Which of the following physical examination maneuvers is most specific for diagnosing the suspected pathology?
Explanation
Question 38
A 28-year-old male is undergoing an open fasciotomy for lateral chronic exertional compartment syndrome. During the approach, the surgeon must be careful to avoid a nerve that typically exits the crural fascia in the distal third of the leg. This nerve provides sensory innervation to which of the following areas?
Explanation
Question 39
Which of the following muscle combinations correctly identifies the contents of the deep posterior compartment of the leg, which is often implicated in medial tibial stress syndrome and chronic exertional compartment syndrome?
Explanation
Question 40
A 55-year-old female presents with severe pain and a crossover deformity of the second toe. Imaging and exam confirm a complete plantar plate tear. She is scheduled for a direct plantar plate repair and a Weil osteotomy. What is the primary mechanical purpose of adding the Weil osteotomy in this setting?
Explanation
Question 41
A 24-year-old long-distance runner presents with bilateral exertional leg pain. Dynamic intracompartmental pressures are measured to evaluate for chronic exertional compartment syndrome (CECS). According to the Pedowitz criteria, which of the following isolated pressure measurements is considered diagnostic for CECS?
Explanation
Question 42
A 28-year-old soccer player undergoes an isolated lateral compartment fasciotomy for CECS. Postoperatively, he reports decreased sensation over the dorsum of his foot, but sensation in the first dorsal webspace remains intact. Which structure was most likely injured during the procedure?
Explanation
Question 43
The plantar plate is a critical static stabilizer of the lesser metatarsophalangeal (MTP) joints, functioning to resist dorsal translation of the proximal phalanx. What is the primary distal bony attachment of the plantar plate?
Explanation
Question 44
A 55-year-old female presents with a progressive crossover toe deformity of her second toe, which rests in a dorsomedial position over the hallux. What is the typical sequence of soft tissue structural failure that leads to this specific deformity?
Explanation
Question 45
A 21-year-old triathlete reports anterior shin pain and numbness in the first dorsal webspace of his foot after running 2 miles. The symptoms resolve with 20 minutes of rest. Which compartment is affected, and what conservative intervention is most likely to lower its exertional pressures?
Explanation
Question 46
A 60-year-old female undergoes a Weil osteotomy of the second metatarsal for chronic MTP joint instability. At her 6-month follow-up, she complains of a "floating toe" that does not touch the ground when standing. What biomechanical alteration caused this complication?
Explanation
Question 47
A 25-year-old male presents with recurrent anterior compartment CECS one year after undergoing a single-incision anterior/lateral fasciotomy. What is the most common anatomic reason for recurrent anterior compartment syndrome following operative release?
Explanation
None
