AAOS Foot & Ankle MCQs (Set 4): Ankle Fractures & Hindfoot Deformities | Board Review
Key Takeaway
This high-yield question set for the AAOS/ABOS exams focuses on critical Foot & Ankle topics. It covers the diagnosis, classification, and management of various ankle fractures, complex hindfoot deformities, and principles of diabetic foot care. Ideal for board preparation and OITE revision.
AAOS Foot & Ankle MCQs (Set 4): Ankle Fractures & Hindfoot Deformities | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
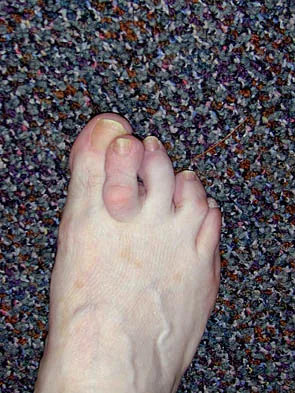
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?
Explanation
Question 2
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
Question 3
In the treatment of all magnitudes of bunionette deformities, what is the most common complication associated with lateral condylectomy of the fifth metatarsal head?
Explanation
Question 4
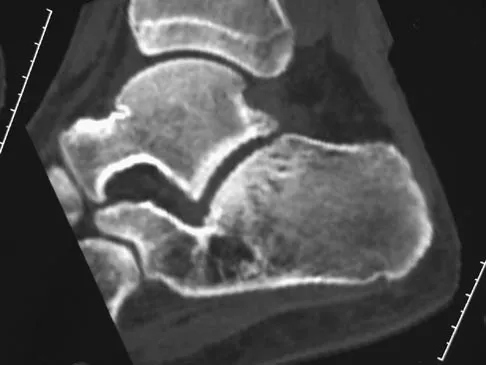
A 17-year-old patient sustained a closed calcaneal fracture when he jumped off of a roof 2 years ago, and he underwent nonsurgical management at the time of injury. The patient now reports lateral hindfoot pain that is worse with weight-bearing activities. Anti-inflammatory drugs and orthoses have failed to provide relief. Coronal and sagittal CT scans are shown in Figures 36a and 36b. What is the best course of action?
Explanation
Question 5
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
Question 6
Figures 37a and 37b show the clinical photographs of a 43-year-old patient with type I diabetes mellitus who has a stump ulcer after undergoing successful transtibial amputation 1 year ago. Which of the following is considered the most predictable method of healing the ulcer and preventing recurrent ulceration?
Explanation
Question 7
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Question 8
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
Question 9
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
Question 10
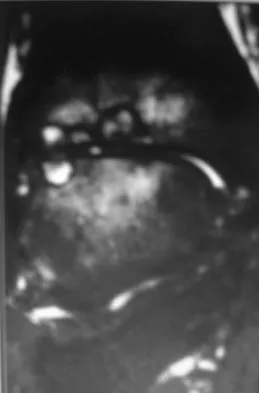
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
Explanation
Question 11
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
Question 12
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
Question 13
A 35-year-old woman has had significant pain and swelling in the left medial ankle inferior to the medial malleolus for the past 8 months. Physical therapy, brace and orthotic management, and immobilization have failed to provide relief. She is now requesting a more aggressive option to assist in pain relief. Clinical photographs and radiographs are seen in Figures 42a through 42f. Following exposure, a complete rupture of the posterior tibial tendon is visible. What is the most appropriate surgical reconstruction?
Explanation
Question 14
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
Question 15
A 65-year-old woman with a history of diabetes mellitus and plantar ulcers has an erythematous and swollen right foot and ankle. Despite IV antibiotics, the erythema spreads to her lower calf within 24 hours. She has a systolic blood pressure of 80/55 mm Hg and a pulse rate of 120. Laboratory studies show a creatinine level of 1.5 mg. Initial management should consist of
Explanation
Question 16
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
Question 17
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
Explanation
Question 18
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Question 19
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
Explanation
Question 20
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
Question 21
A 30-year-old man has chronic pain, joint stiffness, and symmetrical polyarthropathy but no significant synovitis. Examination reveals enlargement of the second and third metatarsal heads. Radiographs show chondrocalcinosis of the ankles and bony enlargement of the midfoot; no marginal erosions are evident at the metatarsophalangeal level. What is the most likely diagnosis?
Explanation
Question 22
The strongest biomechanical construct for open reduction and internal fixation of a talar neck fracture uses what interval and entry point?
Explanation
Question 23
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
Question 24
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
Question 25
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Explanation
Question 26
When utilizing an anterolateral approach to the distal tibia for open reduction and internal fixation of a pilon fracture, which neurologic structure is at greatest risk of iatrogenic injury during the superficial surgical dissection?
Explanation
Question 27
Which of the following parameters measured on a standard anteroposterior (AP) or mortise radiograph is considered the most reliable indicator of syndesmotic widening?
Explanation
Question 28
A 55-year-old woman presents with a painful, flexible flatfoot deformity and an inability to perform a single-leg heel raise.
Clinical examination reveals severe forefoot abduction with 'too many toes' sign. Which of the following procedures is most appropriate to specifically address the forefoot abduction component of her deformity?

Explanation
Question 29
In the Sanders classification of intra-articular calcaneal fractures, the primary prognostic variable that determines the classification type is the number and location of fracture lines through which of the following structures?
Explanation
Question 30
A 35-year-old man sustains a severe ankle injury. Radiographs reveal a fracture-dislocation where the proximal fibular fragment is irreducible by closed means.
Intraoperative exploration demonstrates entrapment of the fibula behind the posterior tubercle of the distal tibia. What is the diagnosis?
Explanation
Question 31
A 24-year-old man presents with a symptomatic cavovarus foot deformity. A Coleman block test is performed, during which the first ray is allowed to drop off the block, and the hindfoot corrects to a neutral alignment. This finding indicates that the hindfoot varus is primarily driven by which of the following?
Explanation
Question 32
A 14-year-old boy presents with frequent ankle sprains and a rigid, flat foot. CT imaging confirms a middle facet talocalcaneal coalition. If nonoperative management fails, what is the generally accepted threshold of joint involvement above which a subtalar or triple arthrodesis is recommended over surgical resection?
Explanation
Question 33
According to the Lauge-Hansen classification, which of the following represents the correct sequential order of structural injury in a Supination-External Rotation (SER) ankle fracture?
Explanation
Question 34
A 45-year-old man sustains an ankle fracture. Radiographs and CT scan demonstrate a lateral malleolus fracture and a posterior malleolus fracture involving 35% of the tibial articular surface with step-off. According to current biomechanical and clinical guidelines, what is the most appropriate management of the posterior malleolus?
Explanation
Question 35
During open reduction and internal fixation of a Weber C ankle fracture, the surgeon needs to evaluate the syndesmosis. Which intraoperative method is considered the most reliable indicator of syndesmotic instability requiring fixation?
Explanation
Question 36
A 65-year-old patient with long-standing, poorly controlled diabetes mellitus and severe peripheral neuropathy presents with a displaced bimalleolar ankle fracture. To minimize the high risk of complications, which modification to standard operative management is most appropriate?
Explanation
Question 37
A 30-year-old man presents with a high-energy closed ankle injury. The ankle is grossly deformed and irreducible in the emergency department. Radiographs demonstrate the proximal fragment of the fibula entrapped posterior to the lateral tubercle of the distal tibia. What is the correct diagnosis?
Explanation
Question 38
A 55-year-old woman presents with a painful, unilateral flatfoot deformity. She is unable to perform a single-leg heel rise, but manual testing reveals that her subtalar joint remains mobile and reducible. What is the most appropriate surgical treatment?
Explanation
Question 39
In a patient with Charcot-Marie-Tooth disease who presents with a progressive, flexible cavovarus foot deformity, the plantarflexed first ray is primarily driven by the relative overpull of which specific muscle?
Explanation
Question 40
A 40-year-old man presents with severe lateral hindfoot pain 2 years after nonoperative management of a displaced intra-articular calcaneus fracture. Examination reveals subtalar stiffness and subfibular impingement. Radiographs show a healed calcaneal malunion with loss of Bohler's angle and advanced subtalar arthritis. What is the best surgical option?
Explanation
Question 41
According to the Lauge-Hansen classification, what is the correct sequential order of tissue injury in a supination-external rotation (SER) ankle fracture?
Explanation
Question 42
A 14-year-old boy presents with a rigid flatfoot and a history of recurrent ankle sprains. Clinical suspicion is high for a calcaneonavicular coalition. Which radiographic view is most sensitive and specific for demonstrating this specific coalition?
Explanation
Question 43
A 15-year-old girl is evaluated for a painful, rigid flatfoot. A lateral weight-bearing radiograph demonstrates a continuous, dense osseous outline extending from the talar dome down to the sustentaculum tali (the "C-sign"). This radiographic finding strongly suggests which underlying condition?
Explanation
Question 44
A 35-year-old man sustains a high-energy, closed tibial pilon fracture. At presentation, there is massive soft tissue swelling and multiple clear fracture blisters over the medial ankle. What is the most appropriate initial orthopaedic management?
Explanation
Question 45
When utilizing lag screws for the internal fixation of a transverse medial malleolus fracture, what is the optimal trajectory of the screws to maximize interfragmentary compression and avoid articular penetration?
Explanation
Question 46
A 22-year-old woman is being evaluated for a symptomatic cavovarus foot deformity. A Coleman block test is performed by having the patient stand with her lateral heel and foot on a wooden block, allowing the first metatarsal to hang freely. During this maneuver, her hindfoot varus completely corrects to neutral. What does this indicate?
Explanation
Question 47
A 62-year-old woman has severe, long-standing, medial and lateral ankle pain with a progressive flatfoot deformity. Examination shows a fixed, rigid planovalgus deformity, and radiographs demonstrate significant joint space narrowing and subchondral sclerosis in the subtalar and talonavicular joints. What is the most definitive surgical intervention?
Explanation
Question 48
A 40-year-old patient presents with a severe ankle injury. Radiographs show a transverse fracture of the medial malleolus and a comminuted, bending-type fracture of the fibula located above the level of the syndesmosis. Which Lauge-Hansen classification does this pattern most accurately fit?
Explanation
Question 49
When counseling a patient on the choice between operative and nonoperative management for an acute Achilles tendon rupture using modern, early-functional rehabilitation protocols, operative treatment is statistically associated with a higher risk of which of the following?
Explanation
Question 50
A 28-year-old woman reports persistent lateral foot pain 4 weeks after an inversion injury initially diagnosed as an ankle sprain. She has maximal point tenderness about 2 cm anterior and inferior to the lateral malleolus. Radiographs reveal a minimally displaced fracture of the anterior process of the calcaneus. This fracture usually occurs via avulsion of which ligament?
Explanation
Question 51
A 35-year-old man sustains an ankle fracture. Radiographs show a posterior malleolar fragment involving 30% of the articular surface with posterior subluxation of the talus. What is the most appropriate surgical approach for direct visualization and isolated fixation of this fragment?
Explanation
Question 52
A 42-year-old roofer falls from a ladder and sustains a displaced intra-articular calcaneus fracture
. According to the Sanders classification, which of the following radiographic views is primary for determining the grade of the fracture?
Explanation
Question 53
A 50-year-old male presents with a high-energy closed pilon fracture accompanied by severe soft tissue swelling, fracture blisters, and skin tenting. What is the most appropriate initial management step?
Explanation
Question 54
A 55-year-old woman presents with medial ankle pain and a progressive flatfoot deformity. She has a flexible hindfoot valgus and is unable to perform a single-leg heel raise. Nonoperative management has failed. What is the most appropriate surgical intervention?
Explanation
Question 55
A 62-year-old female presents with severe, rigid planovalgus deformity and lateral hindfoot pain secondary to subfibular impingement. Radiographs show significant subtalar and talonavicular arthritis. What is the most appropriate definitive treatment?
Explanation
Question 56
During open reduction and internal fixation of a Weber C ankle fracture, the surgeon suspects a syndesmotic injury. Which of the following intraoperative tests is considered the most reliable for evaluating syndesmotic instability?
Explanation
Question 57
A patient with a history of a conservatively managed calcaneus fracture presents 1 year later with persistent lateral midfoot pain exacerbated by walking on uneven ground. Examination reveals tenderness localized to the lateral column. Which joint is most likely responsible for these symptoms?
Explanation
Question 58
A 28-year-old male undergoes ORIF for a displaced talar neck fracture. At 8 weeks postoperatively, an AP radiograph shows a subchondral radiolucent band in the talar dome. What does this finding indicate?
Explanation
Question 59
A 16-year-old boy presents with progressive bilateral cavovarus foot deformities. Neurological examination reveals weakness in foot dorsiflexion and eversion. In Charcot-Marie-Tooth disease, which muscle imbalance is the primary driver of this forefoot-driven hindfoot varus deformity?
Explanation
Question 60
A patient presents with a severe cavovarus deformity. A Coleman block test is performed, and the hindfoot completely corrects to a neutral alignment when the first metatarsal is allowed to drop off the block. What does this indicate about the deformity?
Explanation
Question 61
A 30-year-old male presents with a severely deformed ankle following a twisting injury. Closed reduction in the emergency department is unsuccessful. Radiographs show a posterior fracture-dislocation of the fibula behind the posterior tubercle of the distal tibia. What is the most likely diagnosis?
Explanation
Question 62
A 60-year-old patient with poorly controlled diabetes mellitus and severe peripheral neuropathy sustains a bimalleolar ankle fracture. To prevent fixation failure and Charcot arthropathy, what modification to standard surgical technique is recommended?
Explanation
Question 63
A 14-year-old boy sustains a Salter-Harris III fracture of the anterolateral distal tibial epiphysis
. Which of the following ligaments is responsible for avulsing this fragment?

Explanation
Question 64
A 45-year-old female presents with an isolated lateral malleolus fracture and medial joint line tenderness. A gravity stress radiograph demonstrates 6 mm of medial clear space widening. Which of the following statements regarding the medial injury is most accurate?
Explanation
Question 65
A 38-year-old male complains of anterior ankle impingement and difficulty fitting into standard shoes 2 years after conservative treatment of a calcaneus fracture. Which of the following best describes the typical components of a calcaneal malunion?
Explanation
Question 66
A 12-year-old boy presents with frequent ankle sprains and a rigid flatfoot. Radiographs show a "C sign", and CT confirms a middle facet talocalcaneal coalition. If nonoperative management fails and there is no significant arthritis, what is the best surgical option?
Explanation
Question 67
A 25-year-old athlete sustains a lateral subtalar dislocation. Closed reduction in the emergency department is unsuccessful. Which of the following anatomic structures is most commonly interposed and blocking reduction in this specific injury pattern?
Explanation
Question 68
A 45-year-old man undergoes ORIF for a Weber C ankle fracture with syndesmotic instability. Two cortical screws are placed across four cortices. Regarding syndesmotic screw fixation, what does the current orthopedic literature recommend?
Explanation
Question 69
When treating a trimalleolar ankle fracture, which of the following is the strongest absolute indication for operative fixation of the posterior malleolus?
Explanation
Question 70
A 65-year-old poorly controlled diabetic patient with peripheral neuropathy sustains a bimalleolar equivalent ankle fracture. What modification to the standard surgical protocol is most strongly recommended?
Explanation
Question 71
A 55-year-old woman presents with a flexible flatfoot deformity, unable to perform a single-leg heel raise. She has pain along the medial hindfoot. Imaging shows uncovering of the talonavicular joint but no arthritis. Conservative management has failed. Which of the following surgical procedures is most appropriate?
Explanation
Question 72
A 24-year-old man with Charcot-Marie-Tooth disease presents with a rigid bilateral cavovarus foot deformity and recurrent lateral ankle sprains. The Coleman block test demonstrates a flexible hindfoot that corrects to neutral when the first ray is off the block. What is the primary driver of his hindfoot varus deformity?
Explanation
Question 73
A 38-year-old construction worker falls from a ladder, sustaining an intra-articular calcaneus fracture. Radiographs reveal a decreased Böhler's angle and an increased angle of Gissane.
What is the primary anatomic goal of open reduction and internal fixation in this setting?
Explanation
Question 74
A 45-year-old man is 2 years status-post nonoperative management of a displaced intra-articular calcaneus fracture. He now presents with lateral hindfoot pain and difficulty walking on uneven ground. Physical examination reveals impingement of the fibula against the lateral calcaneal wall. What is the most appropriate definitive surgical intervention?
Explanation
Question 75
A 45-year-old man sustains a bimalleolar equivalent ankle fracture. Radiographs show a posterior malleolus fragment involving 15% of the articular surface. Intraoperatively, after fixing the lateral malleolus, the syndesmosis remains unstable. What is the most appropriate next step in management?
Explanation
Question 76
A 32-year-old male presents to the emergency department after a twisting injury to his ankle. The ankle is grossly deformed and irreducible in the trauma bay under procedural sedation. Radiographs demonstrate a fracture-dislocation. What is the most likely anatomic block to reduction in a classic Bosworth injury?
Explanation
Question 77
A 60-year-old female with long-standing, poorly controlled type 2 diabetes mellitus and profound peripheral neuropathy sustains a displaced bimalleolar ankle fracture. Which of the following surgical strategies is most appropriate to minimize the risk of post-operative failure?
Explanation
Question 78
A 24-year-old man with Charcot-Marie-Tooth disease presents with a progressive, bilateral cavovarus foot deformity. The Coleman block test demonstrates that the hindfoot varus corrects to neutral when the first ray is allowed to plantarflex off the block. What is the primary muscle imbalance driving this patient's forefoot deformity?
Explanation
Question 79
A 35-year-old roofer falls and sustains an isolated vertical fracture of the medial malleolus. Which of the following Lauge-Hansen injury mechanisms is most likely responsible for this specific fracture pattern?
Explanation
Question 80
A 55-year-old woman presents with severe medial ankle pain and a progressively flattening arch. On examination, she is unable to perform a single-leg heel rise. Radiographs demonstrate >40% uncoverage of the talonavicular joint and a flexible hindfoot valgus deformity. What is the most appropriate surgical management?
Explanation
Question 81
A 14-year-old boy presents with frequent ankle sprains and rigid, flat arches. Examination reveals significant restriction of subtalar motion. Lateral radiographs demonstrate a continuous osseous connection between the talus and calcaneus forming a "C-sign". Which facet of the subtalar joint is most commonly involved in this condition?
Explanation
Question 82
When evaluating an ankle mortise radiograph for a suspected syndesmotic injury, the medial clear space (MCS) is a critical parameter. Which of the following conditions definitively describes an abnormal medial clear space indicative of deep deltoid ligament disruption?
Explanation
Question 83
A 28-year-old male sustains a pronation-external rotation (PER) ankle fracture. Operative fixation of the fibula and medial malleolus is performed. Intraoperative stress testing reveals widening of the medial clear space, and a syndesmotic screw is planned. At what distance above the tibial plafond should the syndesmotic screw ideally be placed to biomechanically optimize stabilization without violating the joint capsule?
Explanation
Question 84
A 55-year-old female presents with Stage IIB posterior tibial tendon dysfunction (flexible pes planovalgus with >30% uncoverage of the talar head). She has failed conservative management. Surgical reconstruction is planned, including a flexor digitorum longus (FDL) transfer and medial displacement calcaneal osteotomy (MDCO). What additional procedure is most critical to correct the forefoot abduction deformity?
Explanation
Question 85
A 35-year-old male sustains an acute ankle injury after a fall. Radiographs demonstrate a displaced distal fibula fracture with fixed posterior subluxation of the talus. Closed reduction in the emergency department under conscious sedation is unsuccessful. What anatomic structure is most likely impeding the reduction of the fibula?
Explanation
Question 86
A 24-year-old male with Charcot-Marie-Tooth disease presents with a progressive bilateral cavovarus foot deformity. The Coleman block test demonstrates that the hindfoot varus is flexible and completely corrects when the first metatarsal is allowed to drop off the block. What is the primary driving force for the hindfoot varus in this patient?
Explanation
Question 87
A 14-year-old boy sustains an ankle injury while skateboarding. Radiographs show a Salter-Harris III fracture of the anterolateral distal tibia. Which ligament is responsible for the avulsion of this specific fracture fragment?
Explanation
Question 88
A 42-year-old man presents with chronic lateral hindfoot pain and difficulty walking on uneven ground, 18 months after nonoperative treatment of a displaced intra-articular calcaneus fracture. Examination reveals restricted subtalar motion and subfibular impingement. Radiographs show a healed calcaneus with loss of Bohler's angle, lateral wall blow-out, and subtalar arthritis. What is the most appropriate surgical management?
Explanation
None
