
AAOS & ABOS Foot & Ankle Board Review MCQs (Set 2): Ankle Fractures, Lisfranc, Diabetic Foot
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 15a and 15b show the radiographs of an 18-year-old mountain biker who came off of a 15-foot ramp and sustained an injury to his ankle. Because the local rural hospital had no orthopaedic surgeon available, he was transported to a Level 1 emergency department 10 hours after his initial injury. Examination reveals that the injury remains closed. Management should consist of
Explanation
Question 2
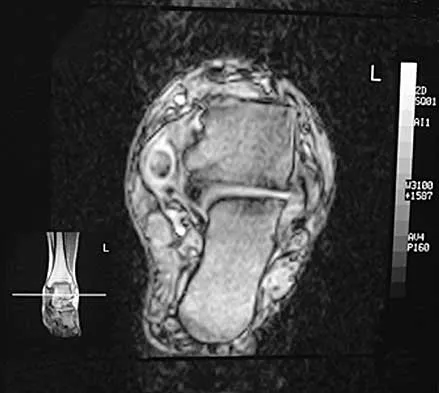
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?
Explanation
Question 3
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
Question 4
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of
Explanation
Question 5
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of
Explanation
Question 6
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Explanation
Question 7
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of
Explanation
Question 8
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
Question 9
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?
Explanation
Question 10
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
Question 11
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Explanation
Question 12
Which of the following is considered the most important factor in eliminating infection in chronic osteomyelitis?
Explanation
Question 13
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Explanation
Question 14
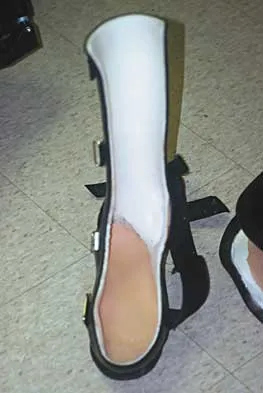
What type of brace is shown in Figures 22a and 22b?
Explanation
Question 15
A 23-year-old man has pain and a callus beneath the second metatarsal head. Initial management should consist of
Explanation
Question 16
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
Question 17
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
Question 18
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?
Explanation
Question 19
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
Question 20
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
Question 21
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of
Explanation
Question 22
The Keller proximal phalanx resection procedure is most useful for which of the following conditions?
Explanation
Question 23
An active 60-year-old man is evaluated 4 years following surgical correction of a hallux valgus deformity. The patient reports that a hallux varus deformity developed rapidly following his initial surgery. Conservative management consisting of wider shoes, toe strapping, and anti-inflammatory drugs has failed to provide relief. Examination reveals a hallux varus deformity with restricted painful motion of the metatarsophalangeal joint and callus formation under the second metatarsal head. What is the next most appropriate step in management?
Explanation
Question 24
A newborn has been referred for evaluation of a deformed foot. Prenatal and birth history are unremarkable. Examination reveals a rocker bottom appearance to the foot, and a longitudinal arch cannot be created. A palpable lump is appreciated on the plantar medial surface. What is the best course of action?
Explanation
Question 25
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?
Explanation
Question 26
A 28-year-old male sustains an unstable syndesmotic injury requiring screw fixation. Which of the following ligaments provides the greatest contribution to the stability of the distal tibiofibular syndesmosis?
Explanation
Question 27
A 45-year-old female sustains a closed twisting injury to her right ankle. Radiographs demonstrate a displaced supination-external rotation (SER) IV ankle fracture. During surgical fixation, what is the most critical biomechanical factor in restoring normal tibiotalar contact area and pressures?
Explanation
Question 28
A 35-year-old male sustains a trimalleolar ankle fracture. The posterior malleolus fragment involves 15% of the articular surface. Following rigid fixation of the medial and lateral malleoli, intraoperative stress testing reveals persistent syndesmotic instability. What is the most biomechanically stable method to address this?
Explanation
Question 29
A 60-year-old diabetic patient undergoes open reduction and internal fixation for a displaced bimalleolar ankle fracture.
What postoperative protocol modification is most strongly recommended for this patient compared to a non-diabetic patient?

Explanation
Question 30
A 28-year-old male sustains a high-energy closed tibial pilon fracture with severe fracture blisters and massive soft tissue swelling. What is the most appropriate initial management?
Explanation
Question 31
A 30-year-old female presents with an irreducible ankle fracture-dislocation after a skiing accident. Radiographs reveal the proximal fibular fragment is entrapped behind the posterior tubercle of the distal tibia. What is the eponymous name for this specific injury pattern?
Explanation
Question 32
A 40-year-old male presents 8 months after non-operative treatment of an ankle fracture. He complains of chronic lateral pain and instability. Radiographs show a healed fibula that is shortened and externally rotated, with a widened medial clear space. What is the most appropriate surgical management?
Explanation
Question 33
In a suspected midfoot injury, subtle widening is noted between the 1st and 2nd metatarsal bases.
The critical Lisfranc ligament, responsible for stability in this region, anatomically connects which two structures?

Explanation
Question 34
A 35-year-old female sustains a purely ligamentous Lisfranc injury with 3 mm of diastasis between the medial cuneiform and 2nd metatarsal. Based on recent prospective randomized trials, what is the recommended surgical management for optimal functional outcomes?
Explanation
Question 35
A 19-year-old athlete complains of severe midfoot pain after an axial load was applied to his plantarflexed foot. Non-weight-bearing radiographs in the emergency department are normal. What is the most appropriate next step in diagnosis?
Explanation
Question 36
During open reduction and internal fixation of a severe, multi-column Lisfranc fracture-dislocation, what is the universally accepted correct sequence of reduction and fixation?
Explanation
Question 37
A 55-year-old male presents with severe midfoot pain and a progressive planovalgus deformity. He was diagnosed with a 'foot sprain' 1 year ago. Radiographs demonstrate advanced degenerative changes at the tarsometatarsal joints with lateral subluxation. What is the most appropriate surgical treatment?
Explanation
Question 38
A 58-year-old male with long-standing, poorly controlled diabetes presents with a red, hot, swollen foot. He has bounding pedal pulses and intact skin. Radiographs show early fragmentation and subluxation of the midfoot. What is the most appropriate initial management?
Explanation
Question 39
A 62-year-old female with neuropathy presents with a chronic, uninfected plantar forefoot ulcer beneath the 3rd metatarsal head. It is classified as Wagner Grade 1. What intervention has the highest level of evidence for achieving ulcer healing?
Explanation
Question 40
A 50-year-old diabetic male has a chronic plantar midfoot ulcer overlying a rocker-bottom deformity. An MRI is ordered to differentiate chronic inactive Charcot osteoarthropathy from osteomyelitis. Which MRI finding is most specific for osteomyelitis rather than Charcot changes alone?
Explanation
Question 41
A diabetic patient is being evaluated for a minor forefoot amputation due to a non-healing distal ulcer. Which of the following non-invasive vascular parameters represents the minimum threshold predictive of reliable wound healing?
Explanation
Question 42
A 65-year-old diabetic patient has a recurrent uninfected plantar ulcer beneath the 1st metatarsal head despite optimal orthotics. Examination demonstrates 5 degrees of ankle plantarflexion with the knee extended, but 15 degrees of dorsiflexion with the knee flexed. What is the most appropriate surgical adjunct to aid in offloading?
Explanation
Question 43
A 52-year-old diabetic male has a stable, rigid midfoot Charcot deformity with a prominent plantar-medial bony bossing. He has developed 3 recurrent, non-infected ulcers over this specific prominence despite custom total contact orthotics. What is the most appropriate surgical management?
Explanation
Question 44
A 40-year-old female sustains a pronation-abduction (PAB) ankle fracture. According to the Lauge-Hansen classification system, what represents the first stage (Stage I) of this specific injury mechanism?
Explanation
Question 45
Total contact casting (TCC) is considered the gold standard for offloading diabetic plantar foot ulcers. Which of the following is an absolute contraindication to the application of a TCC?
Explanation
Question 46
A subtle radiographic finding indicative of a Lisfranc injury is the "fleck sign". This sign represents a bony avulsion of the Lisfranc ligament from which of the following anatomic locations?
Explanation
Question 47
A 62-year-old diabetic male has a recurrent, non-healing plantar ulcer under the first metatarsal head despite 12 weeks of total contact casting. Ankle dorsiflexion is -10 degrees with the knee extended and -10 degrees with the knee flexed. Which of the following is the most appropriate surgical treatment to facilitate ulcer healing?
Explanation
Question 48
In the surgical management of a trimalleolar ankle fracture, anatomic reduction and internal fixation of the posterior malleolus is most strongly indicated to achieve which of the following biomechanical goals?
Explanation
Question 49
A 45-year-old construction worker sustains a purely ligamentous Lisfranc injury involving the 1st, 2nd, and 3rd tarsometatarsal (TMT) joints. What is the most appropriate definitive management?
Explanation
Question 50
A 55-year-old female with poorly controlled type 2 diabetes presents with a red, hot, swollen left foot. Radiographs show soft tissue swelling and mild osteopenia but no fractures. MRI shows diffuse marrow edema without focal fluid collections. Her ESR and CRP are normal. What is the most appropriate initial management?
Explanation
Question 51
Which of the following radiographic parameters is the most accurate and reliable indicator of a syndesmotic injury on standard weight-bearing ankle radiographs?
Explanation
Question 52
A 28-year-old male sustains a twisting injury to his foot. Radiographs demonstrate a small bony avulsion fragment in the space between the bases of the first and second metatarsals. This fragment represents an avulsion of a structure that originates from which of the following bones?
Explanation
Question 53
Which of the following magnetic resonance imaging (MRI) findings is the most sensitive and specific for distinguishing osteomyelitis from acute Charcot neuroarthropathy in the diabetic foot?
Explanation
Question 54
According to the Lauge-Hansen classification, a Supination-Adduction stage II ankle fracture typically presents with which of the following distinct fracture patterns?
Explanation
Question 55
A 65-year-old patient with severe peripheral neuropathy and diabetes sustains a bimalleolar ankle fracture. Which surgical strategy is most appropriate to minimize the risk of catastrophic fixation failure and secondary Charcot arthropathy?
Explanation
Question 56
A 32-year-old athlete complains of persistent midfoot pain after a fall. Non-weight bearing radiographs in the emergency department appear normal. What is the next best step to evaluate for a subtle Lisfranc injury?
Explanation
Question 57
A patient requires a Syme amputation for a severe diabetic forefoot infection. Which of the following technical steps is absolutely essential for a successful outcome and a durable, weight-bearing stump?
Explanation
Question 58
A 40-year-old sustains an ankle injury. Radiographs reveal a widened medial clear space and a short oblique fracture of the fibula 6 cm proximal to the joint line. According to Lauge-Hansen, what was the first structure injured in this sequence?
Explanation
Question 59
A 58-year-old diabetic male presents with a deep plantar ulcer extending to the joint capsule, but with no bone involvement, no abscess, and no gangrene. According to the Wagner classification, what grade is this ulcer?
Explanation
Question 60
A patient presents with a severe ankle injury where the proximal fibular fragment is entrapped behind the posterior tubercle of the tibia, rendering closed reduction impossible. Which mechanism is primarily responsible for this specific injury pattern (Bosworth fracture-dislocation)?
Explanation
Question 61
The primary osseous stability of the midfoot is provided by the interlocking 'keystone' configuration of the tarsometatarsal joints. Which anatomical structure forms this critical keystone?
Explanation
Question 62
A 60-year-old diabetic patient presents with a chronic, rigid, 'rocker-bottom' foot deformity (Eichenholtz Stage III) and a recurrent midfoot plantar ulcer under the cuboid. Nonoperative management with a CROW boot has failed multiple times. What is the most appropriate surgical intervention?
Explanation
Question 63
The 'logsplitter' injury of the ankle is best described by which of the following pathomechanical processes?
Explanation
Question 64
A 35-year-old male is 2 years out from an open reduction and internal fixation of a severe Lisfranc injury. He now complains of severe, localized midfoot pain with weight-bearing. Radiographs show advanced degenerative changes at the 2nd and 3rd TMT joints. Management should consist of:
Explanation
Question 65
A 50-year-old diabetic woman has severe flexible claw toe deformities and recurrent distal tip ulcerations on digits 2-4. She has palpable pulses and a normal ABI. What is the most appropriate prophylactic surgical procedure to heal the ulcers and prevent recurrence?
Explanation
Question 66
A 65-year-old poorly controlled diabetic patient sustains a closed, displaced bimalleolar equivalent ankle fracture. What is the most appropriate surgical strategy compared to a non-diabetic patient?
Explanation
Question 67
Which of the following accurately describes the primary attachment sites of the Lisfranc ligament?
Explanation
Question 68
A 30-year-old male sustains a purely ligamentous Lisfranc injury. Weight-bearing radiographs demonstrate 4 mm of diastasis between the first and second metatarsal bases without fracture. Which of the following is the most appropriate definitive management?
Explanation
Question 69
A 55-year-old diabetic patient presents with a swollen, erythematous, and warm right foot without an open ulcer. Radiographs show fragmentation and subluxation of the midfoot. ESR and WBC are normal. What is the most appropriate initial management?
Explanation
Question 70
In the operative management of a trimalleolar ankle fracture, traditional guidelines indicate fixation of the posterior malleolus if the fragment involves what minimum percentage of the articular surface?
Explanation
Question 71
A 60-year-old diabetic male has a recurrent neuropathic ulcer under the first metatarsal head. He has a rigid equinus deformity with limited ankle dorsiflexion. What is the best surgical intervention to prevent recurrence after ulcer healing?
Explanation
Question 72
A 25-year-old male sustains an ankle injury. Radiographs reveal a fracture-dislocation of the ankle. During closed reduction in the emergency department, the ankle remains irreducible. What is the most likely anatomic block to reduction?
Explanation
Question 73
A 62-year-old diabetic patient with a chronic midfoot ulcer presents with erythema and swelling. Radiographs show bone destruction. Which of the following is the most reliable imaging modality to differentiate acute Charcot neuroarthropathy from osteomyelitis?
Explanation
Question 74
During ORIF of a supination-external rotation type IV ankle fracture, the surgeon suspects a syndesmotic injury. After fixing the fibula, what intraoperative maneuver is best to test the integrity of the syndesmosis?
Explanation
Question 75
A patient presents with a painful, swollen midfoot after a fall from a horse. Plain anteroposterior radiographs reveal a small avulsion fracture in the space between the base of the first and second metatarsals. What is this radiographic finding called and what does it signify?
Explanation
Question 76
A patient undergoes a transmetatarsal amputation (TMA) for a gangrenous diabetic foot infection. Post-operatively, the patient is at highest risk for developing which of the following foot deformities?
Explanation
Question 77
A 40-year-old female sustains an ankle fracture. Radiographs show a transverse fracture of the lateral malleolus at the level of the joint line and a vertical fracture of the medial malleolus. Which Lauge-Hansen classification best describes this injury pattern?
Explanation
Question 78
Regarding lower extremity amputations in diabetic patients, which level of amputation requires the least increase in energy expenditure for ambulation compared to normal gait?
Explanation
Question 79
A 35-year-old patient presents with chronic lateral ankle pain 2 years after nonoperative treatment of an ankle fracture. Radiographs reveal a malunion with lateral talar shift. Disruption of which radiographic line on the AP view is the most sensitive indicator of fibular shortening?
Explanation
Question 80
A 28-year-old male sustains a severe crush injury to his midfoot. Radiographs show a divergent Lisfranc fracture-dislocation with significant comminution of the cuboid (nutcracker fracture). When performing ORIF, what is the primary goal of managing the lateral column (4th and 5th TMT joints)?
Explanation
Question 81
A 35-year-old construction worker undergoes open reduction and internal fixation for a highly comminuted bimalleolar equivalent ankle fracture with syndesmotic disruption. Intraoperatively, the syndesmosis is reduced and stabilized with two trans-syndesmotic screws. What is the most accurate imaging modality to assess the accuracy of the syndesmotic reduction postoperatively?

Explanation
Question 82
A 24-year-old collegiate football player presents with severe midfoot pain after an axial loading injury to a plantar-flexed foot. Non-weight-bearing radiographs in the emergency department show no fractures or malalignment. What is the most appropriate next step in diagnosis?
Explanation
Question 83
A 55-year-old poorly controlled diabetic patient presents with a red, hot, and swollen left foot. Radiographs are negative for fracture or overt destruction. Which of the following clinical findings best differentiates acute Charcot neuroarthropathy from a deep infection?
Explanation
Question 84
Current orthopedic literature suggests that direct open reduction and internal fixation of a posterior malleolus fracture fragment, as opposed to percutaneous AP screw fixation or nonoperative management, offers which of the following distinct biomechanical advantages?
Explanation
Question 85
A 30-year-old recreational athlete sustains a purely ligamentous Lisfranc injury involving the first, second, and third tarsometatarsal (TMT) joints. What surgical intervention has been shown in recent prospective literature to yield the most favorable functional outcomes and lowest reoperation rate for this specific injury pattern?
Explanation
Question 86
A 62-year-old diabetic patient is successfully treated for an infection associated with a Wagner Grade 3 plantar ulcer beneath the first metatarsal head. Clinical examination reveals a severe equinus contracture. Which of the following adjunctive surgical interventions will best prevent recurrence of the ulcer?
Explanation
Question 87
A 65-year-old patient with long-standing, poorly controlled diabetes mellitus and peripheral neuropathy sustains an unstable bimalleolar ankle fracture. Which of the following modifications to the standard surgical protocol is most appropriate?
Explanation
Question 88
During the surgical exposure and reduction of a Lisfranc fracture-dislocation, an understanding of the local anatomy is critical. The primary Lisfranc ligament connects which of the following two structures?
Explanation
Question 89
A 58-year-old diabetic man requires a transmetatarsal amputation for a non-healing, gangrenous toe wound. Preoperative non-invasive vascular testing is ordered to predict wound healing. Which of the following parameters is generally accepted as the minimum threshold indicating adequate perfusion for healing of the amputation?
Explanation
Question 90
A 40-year-old male sustains an irreducible fracture-dislocation of the right ankle following a fall from a height. The injury is classified as a Bosworth fracture-dislocation. Which of the following anatomic blocks to reduction is the hallmark of this injury?
Explanation
Question 91
A patient with long-standing diabetes presents with a markedly swollen, warm, and erythematous foot. Radiographs demonstrate severe periarticular debris, joint dislocation, and fragmentation of the midfoot bones.
According to the Eichenholtz classification of Charcot neuroarthropathy, this represents which stage?
Explanation
Question 92
Based on the classic biomechanical studies by Ramsey and Hamilton regarding ankle congruency following a fracture, 1 mm of lateral talar shift results in approximately what percentage decrease in tibiotalar contact area?
Explanation
Question 93
What is the most common mechanism of injury that results in a longitudinal Lisfranc fracture-dislocation in an athletic population?
Explanation
Question 94
A Total Contact Cast (TCC) is considered the gold standard for offloading plantar diabetic foot ulcers. What is its primary biomechanical mechanism of action in promoting ulcer healing?
Explanation
Question 95
A diabetic patient presents with a midfoot ulcer and deep soft tissue swelling. Which of the following MRI findings is most indicative of osteomyelitis rather than acute Charcot neuroarthropathy?
Explanation
Question 96
During the operative treatment of a complex ankle fracture, an avulsed bony fragment is identified attached to the anterior inferior tibiofibular ligament (AITFL). If this fragment originated from the tibia, it is anatomically referred to as the:
Explanation
Question 97
According to the Lauge-Hansen classification system, what is the sequence of injury in a Pronation-Abduction (PA) Stage III ankle fracture?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding foot-ankle-2000-set-2-mcqs-3940