AAOS Foot & Ankle MCQs (Set 1): Trauma & Degenerative Disorders | ABOS Review

Key Takeaway
This high-yield question set, Set 1, for AAOS and ABOS board exams, focuses on critical foot and ankle orthopedics. It covers common trauma, degenerative conditions, biomechanics, and surgical management principles crucial for comprehensive review and exam preparation.
AAOS Foot & Ankle MCQs (Set 1): Trauma & Degenerative Disorders | ABOS Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
Question 2
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
Question 3
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?
Explanation
Question 4
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
Question 5
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
Question 6
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
Question 7
Removal of both hallucal sesamoids should be reserved as a salvage procedure because of the high incidence of which of the following postoperative complications?
Explanation
Question 8
A 35-year-old man who snowboards sustained the injury shown in Figures 4a through 4c. What is the mechanism of injury?
Explanation
Question 9
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm3, a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm3. Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
Question 10
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?
Explanation
Question 11
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
Question 12
What is the most common foot deformity associated with myelomeningocele?
Explanation
Question 13
Where is the watershed zone for tarsal navicular vascularity?
Explanation
Question 14
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?
Explanation
Question 15
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Explanation
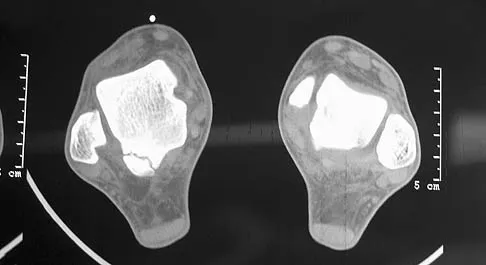
Question 16
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
Question 17
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of
Explanation
Question 18
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
Question 19
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include
Explanation
Question 20
The Lisfranc ligament connects the base of the
Explanation
Question 21
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
Question 22
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
Question 23
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?
Explanation
Question 24
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
Question 25
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a "pencil in cup" distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?
Explanation
Question 26
A 42-year-old recreational athlete sustains an acute Achilles tendon rupture. He elects for nonoperative management. Which of the following best describes his expected outcome compared to operative repair?
Explanation
Question 27
A 30-year-old active male presents with midfoot pain after an axial load injury to a plantarflexed foot. Weight-bearing radiographs demonstrate 4 mm of widening between the medial cuneiform and the base of the second metatarsal, with no associated fractures.
According to recent literature, what is the most appropriate surgical management for this patient?

Explanation
Question 28
A 42-year-old weekend warrior sustains an acute Achilles tendon rupture. He elects for non-operative management. What rehabilitation protocol modification has been shown to result in re-rupture rates comparable to operative management?
Explanation
Question 29
A 35-year-old male sustains a Hawkins Type III talar neck fracture. Which of the following blood vessels is the primary vascular supply to the talar body and is at greatest risk of disruption in this injury?
Explanation
Question 30
During an extensile lateral approach for the open reduction and internal fixation of a displaced intra-articular calcaneus fracture, a nerve is at risk of iatrogenic injury at the proximal and distal extents of the incision. Which nerve is this?
Explanation
Question 31
A 65-year-old male with end-stage ankle osteoarthritis presents for operative evaluation. He is requesting a total ankle arthroplasty (TAA). Which of the following is considered an absolute contraindication to TAA?
Explanation
Question 32
A 20-year-old collegiate track athlete complains of vague dorsal midfoot pain that worsens with sprinting. Plain radiographs are normal. A subsequent CT scan reveals an incomplete dorsal cortical fracture line in the navicular. What is the most appropriate initial management?
Explanation
Question 33
A 22-year-old collegiate basketball player sustains an acute Zone 2 fracture of the proximal fifth metatarsal. He wishes to return to play as soon as safely possible. What is the recommended treatment?
Explanation
Question 34
A 45-year-old female presents with a highly comminuted, displaced tibial pilon fracture and severe soft tissue swelling with fracture blisters.
What is the most appropriate initial step in her orthopedic management?

Explanation
Question 35
During the evaluation of a rotational ankle fracture, a syndesmotic injury is suspected. Which of the following radiographic parameters on an AP or mortise radiograph is most diagnostic of syndesmotic instability?
Explanation
Question 36
A 55-year-old male presents with dorsal foot pain localized to the first metatarsophalangeal (MTP) joint. Examination reveals a dorsal osteophyte and pain primarily at the end-ranges of dorsiflexion, with preserved mid-range motion (Coughlin Stage 2 Hallux Rigidus). Non-operative measures have failed. What is the most appropriate surgical treatment?
Explanation
Question 37
A 58-year-old patient with long-standing, poorly controlled diabetes presents with an acutely swollen, erythematous, and warm unilateral foot. Radiographs demonstrate periarticular fragmentation and debris at the tarsometatarsal joints. Elevation of the limb for 10 minutes leads to resolution of the erythema. What is the best initial management?
Explanation
Question 38
A 14-year-old boy is evaluated for recurrent ankle sprains and a rigid, painful flatfoot. On physical exam, subtalar motion is severely restricted. Which radiographic view is most sensitive for diagnosing the most likely pathology?
Explanation
Question 39
A 50-year-old overweight female presents with progressive flattening of her left medial longitudinal arch. Examination reveals an inability to perform a single-leg heel raise and forefoot abduction with >30% talonavicular uncoverage on radiographs, but the hindfoot remains manually correctable. What is the appropriate surgical classification and treatment?
Explanation
Question 40
A 28-year-old skier sustained a sudden dorsiflexion and inversion injury. She reports a painful popping sensation behind the lateral malleolus. Examination reveals swelling posterior to the fibula and the tendons subluxate anteriorly during resisted eversion. This pathology is associated with failure of which structure?
Explanation
Question 41
A 25-year-old professional football player suffers a severe hyperdorsiflexion injury to his great toe. MRI reveals a complete rupture of the plantar plate. Which of the following is considered a relative indication for surgical repair over non-operative management in this athlete?
Explanation
Question 42
When comparing outcomes of Total Ankle Arthroplasty (TAA) versus ankle arthrodesis for end-stage ankle osteoarthritis, TAA has been shown in long-term studies to have which of the following relative advantages?
Explanation
Question 43
A 24-year-old snowboarder lands hard following a jump, sustaining a forceful dorsiflexion and inversion injury to the ankle. He has lateral ankle pain mimicking a severe sprain, but radiographs reveal a fracture. Which of the following fractures is pathognomonic for this mechanism?
Explanation
Question 44
A 38-year-old female sustains a trimalleolar ankle fracture. The posterior malleolus fracture involves 35% of the articular surface and is displaced. Current biomechanical evidence suggests that which method provides the most stable fixation for this fragment?
Explanation
Question 45
A 13-year-old boy presents with ankle pain after an external rotation injury. Radiographs show a Salter-Harris III fracture of the anterolateral distal tibia. Which ligament's avulsion force is responsible for this specific fracture pattern?
Explanation
Question 46
A 45-year-old runner with recalcitrant plantar fasciitis undergoes a complete surgical release of the plantar fascia. Post-operatively, she complains of new-onset, severe lateral midfoot pain and a visibly flatter arch. This complication is most directly related to which of the following pathomechanical changes?
Explanation
Question 47
A 28-year-old man sustains a Hawkins type III talar neck fracture following a motor vehicle accident. He undergoes urgent closed reduction and subsequent definitive open reduction and internal fixation. Which of the following best describes his risk of developing avascular necrosis (AVN) of the talar body?
Explanation
Question 48
A 35-year-old male sustains a purely ligamentous Lisfranc injury. Current evidence suggests that when compared to open reduction and internal fixation (ORIF), primary arthrodesis of the first, second, and third tarsometatarsal joints for this specific injury pattern results in:
Explanation
Question 49
A 45-year-old woman complains of painful bunions. Weight-bearing radiographs reveal a hallux valgus angle (HVA) of 38 degrees and an intermetatarsal angle (IMA) of 16 degrees. There is no hypermobility of the first tarsometatarsal joint. What is the most appropriate surgical management?
Explanation
Question 50
A 55-year-old male presents with dorsal midfoot and first toe pain. Examination reveals a palpable dorsal osteophyte and restricted, painful dorsiflexion of the first metatarsophalangeal (MTP) joint. Radiographs show moderate joint space narrowing with large dorsal osteophytes, but the plantar joint space is preserved. He has failed nonoperative management. What is the most appropriate surgical treatment?
Explanation
Question 51
A 50-year-old woman presents with medial ankle pain and a progressively flattening arch. She is able to perform a single-leg heel rise but it is weak and painful. She has a flexible flatfoot deformity. Nonoperative management with a custom orthosis has failed. What is the most appropriate surgical intervention?
Explanation
Question 52
A 58-year-old diabetic patient presents with a swollen, erythematous, and warm right foot without open ulcerations. Laboratory studies show normal white blood cell count and slightly elevated ESR. Radiographs demonstrate fragmentation and subluxation of the midfoot. What is the most appropriate initial management?
Explanation
Question 53
In the Sanders classification for intra-articular calcaneus fractures, the severity and type are determined primarily by which of the following radiographic or advanced imaging views?
Explanation
Question 54
Which of the following is true regarding functional bracing (early functional rehabilitation) compared to surgical repair for acute Achilles tendon ruptures?
Explanation
Question 55
A 21-year-old collegiate basketball player sustains a fracture of the fifth metatarsal base located at the metaphyseal-diaphyseal junction. The fracture extends into the fourth-fifth intermetatarsal articulation. He wishes to return to play as soon as safely possible. What is the recommended treatment?
Explanation
Question 56
A 42-year-old female presents with severe pain in the forefoot, often described as feeling like she is walking on a pebble. The pain is worst in narrow shoes and relieves when barefoot. Examination reveals a palpable click when the metatarsal heads are squeezed together while applying plantar pressure to the webspace. Which webspace is most commonly affected?
Explanation
Question 57
A 62-year-old woman with end-stage post-traumatic ankle osteoarthritis is considering total ankle arthroplasty (TAA). Which of the following is considered an absolute contraindication to TAA?
Explanation
Question 58
A 45-year-old man sustains a high-energy closed tibial pilon fracture. There is severe soft tissue swelling and fracture blisters over the medial and anterior ankle. What is the most appropriate initial management strategy?
Explanation
Question 59
A 24-year-old football player sustains a hyperextension injury to his first MTP joint. He has severe pain, ecchymosis, and inability to bear weight. MRI demonstrates complete disruption of the plantar plate and sesamoid complex with proximal retraction of the sesamoids. What is the most appropriate management?
Explanation
Question 60
A 48-year-old male runner complains of heel pain that is worst with the first few steps in the morning. Examination reveals point tenderness at the medial tuberosity of the calcaneus. Initial management has included rest, NSAIDs, and a prefabricated shoe insert, with minimal improvement after 4 weeks. What is the most appropriate next step in management?
Explanation
Question 61
Tarsal tunnel syndrome involves entrapment of the tibial nerve or its branches. The boundaries of the tarsal tunnel include the medial malleolus anteriorly, the calcaneus laterally, and which structure superficially?
Explanation
Question 62
A 19-year-old track athlete presents with insidious onset of vague dorsal midfoot pain. Radiographs are normal, but an MRI confirms a stress fracture of the tarsal navicular without displacement. What is the initial treatment of choice?
Explanation
Question 63
A 22-year-old female ballet dancer presents with posteromedial ankle pain, exacerbated by going en pointe. She notes a triggering sensation in her great toe. Which of the following is the most likely diagnosis?
Explanation
Question 64
Which of the following intraoperative tests is most reliable for diagnosing latent syndesmotic instability following fixation of a lateral malleolus fracture?
Explanation
Question 65
A 68-year-old male presents with an acute Achilles tendon rupture sustained while playing tennis. He has a past medical history of hypertension and well-controlled diabetes. He is moderately active but prefers avoiding surgery. Which of the following is the most appropriate management, considering current evidence regarding nonoperative versus operative treatment in this demographic?
Explanation
Question 66
A 55-year-old construction worker presents with end-stage post-traumatic ankle osteoarthritis. He has failed standard NSAID therapy and intra-articular corticosteroid injections. He wishes to delay surgery. Which of the following orthotic modifications is most effective for alleviating his pain during ambulation?
Explanation
Question 67
A 24-year-old athlete sustains a purely ligamentous Lisfranc injury involving the first, second, and third tarsometatarsal joints with 3 mm of diastasis, as seen on weight-bearing radiographs.
Based on current literature, which of the following surgical interventions provides the best long-term functional outcome?
Explanation
Question 68
A 42-year-old man undergoes open reduction and internal fixation of a displaced intra-articular calcaneus fracture via an extensile lateral approach. Which of the following patient factors most significantly increases the risk of the most common postoperative complication associated with this approach?
Explanation
Question 69
A 30-year-old male is involved in a motor vehicle collision and sustains a Hawkins type III fracture of the talar neck. Which of the following best describes the joint dislocations associated with this specific injury pattern?
Explanation
Question 70
A 60-year-old woman complains of severe pain and stiffness in her great toe that limits her walking. Examination reveals less than 10 degrees of dorsiflexion at the first metatarsophalangeal (MTP) joint and mid-arc pain. Radiographs demonstrate severe joint space narrowing, a large dorsal osteophyte, and subchondral sclerosis. What is the gold standard operative treatment?
Explanation
Question 71
A 22-year-old soccer player sustains an external rotation injury to his right ankle. Standard non-weight-bearing mortise and AP radiographs reveal no fractures and normal clear space parameters. However, the squeeze test is positive. What is the most appropriate next step to rule out a latent syndesmotic injury?
Explanation
Question 72
A 19-year-old Division I collegiate basketball player sustains an acute, non-displaced fracture of the proximal fifth metatarsal at the metaphyseal-diaphyseal junction (Zone 2). To minimize the risk of nonunion and facilitate the most rapid return to play, which of the following is the best treatment option?
Explanation
Question 73
A 54-year-old woman presents with progressive flattening of her left foot and medial ankle pain. Examination shows a flexible flatfoot, inability to perform a single-limb heel rise, and excessive forefoot abduction. Radiographs show greater than 40% talonavicular uncoverage. What surgical reconstruction is most appropriate?
Explanation
Question 74
A 61-year-old male with poorly controlled type 2 diabetes presents with a globally swollen, erythematous, and warm right foot. He denies trauma. Pulses are palpable, and sensation to a 5.07 Semmes-Weinstein monofilament is absent. Radiographs show periarticular debris and early fragmentation at the tarsometatarsal joints. His ESR and CRP are normal. What is the most appropriate initial management?
Explanation
Question 75
An 8-week post-operative radiograph of a 32-year-old male who underwent open reduction and internal fixation for a Hawkins Type III talar neck fracture demonstrates a subchondral radiolucent band in the dome of the talus. What is the clinical significance of this radiographic finding?
Explanation
Question 76
A 35-year-old construction worker falls from a ladder and sustains a severely displaced, intra-articular calcaneus fracture. He is scheduled for open reduction and internal fixation utilizing a standard extensile lateral approach. During the horizontal limb of the incision, which of the following structures is at greatest risk of iatrogenic injury?
Explanation
Question 77
A 24-year-old collegiate football player hyperplantarflexes his foot with an axial load during a tackle. Weight-bearing radiographs reveal a 'fleck sign' and 3 mm of widening between the medial and middle cuneiforms. What is the primary ligamentous restraint that has been disrupted?
Explanation
Question 78
A 65-year-old woman with post-traumatic end-stage ankle osteoarthritis is being evaluated for a total ankle replacement (TAR). Which of the following conditions is considered an absolute contraindication for this procedure?
Explanation
Question 79
A 22-year-old elite basketball player sustains an acute, non-displaced fracture at the metaphyseal-diaphyseal junction of the fifth metatarsal (Zone 2). To minimize his time away from play and risk of nonunion, what is the most appropriate management?
Explanation
Question 80
A 40-year-old male sustains an acute, closed Achilles tendon rupture while playing tennis. He is discussing operative repair versus non-operative management with early functional rehabilitation. Based on recent literature, what is the most accurate statement regarding outcomes?
Explanation
Question 81
A 55-year-old female presents with progressive medial ankle pain and an acquired flatfoot deformity. Examination reveals a flexible hindfoot valgus, inability to perform a single-leg heel rise, and significant forefoot abduction (Stage IIb posterior tibial tendon dysfunction). Which combination of procedures is most appropriate?
Explanation
Question 82
A 45-year-old woman presents with a symptomatic hallux valgus deformity. Radiographs demonstrate a hallux valgus angle (HVA) of 38 degrees, an intermetatarsal angle (IMA) of 18 degrees, and hypermobility at the first tarsometatarsal (TMT) joint. What is the most appropriate surgical treatment?
Explanation
Question 83
A 50-year-old man presents with dorsal pain in his great toe, especially during terminal stance phase. Examination reveals pain at the extremes of dorsiflexion, but no pain during mid-range motion. Radiographs reveal dorsal osteophytes at the first MTP joint with mild to moderate joint space narrowing (Coughlin and Shurnas Grade 2). What is the recommended primary surgical intervention after failed conservative care?
Explanation
Question 84
A 38-year-old man sustains a severe, high-energy axial load injury to his distal tibia resulting in a highly comminuted, displaced intra-articular pilon fracture. The soft tissues are markedly swollen with early fracture blister formation. What is the most appropriate initial management?
Explanation
Question 85
A 58-year-old male with poorly controlled diabetes presents with a unilaterally erythematous, warm, and swollen foot. He denies any trauma. Radiographs reveal early fragmentation, periarticular debris, and subluxation of the tarsometatarsal joints. There are no open ulcers. What is the most appropriate initial management?
Explanation
Question 86
A 20-year-old cross-country runner presents with an insidious onset of dorsal midfoot pain. Initial radiographs are unremarkable, but an MRI demonstrates a non-displaced fracture in the central third of the tarsal navicular. What is the most appropriate treatment?
Explanation
Question 87
A 24-year-old athlete sustains an axial load injury to a plantarflexed foot. Non-weight-bearing radiographs of the foot are interpreted as normal, but the patient has severe midfoot pain and cannot bear weight. What is the next best step in evaluation?
Explanation
Question 88
A 62-year-old woman complains of dorsal midfoot pain and limited toe-off during gait. Examination reveals severe pain with hallux dorsiflexion, which is limited to less than 10 degrees. Radiographs show diffuse joint space loss across the entire first metatarsophalangeal joint (Coughlin Stage 3) and prominent dorsal osteophytes. She has failed rigid shoe modifications. What is the best operative management?
Explanation
Question 89
A 55-year-old woman presents with progressive flattening of her left foot and medial ankle pain. Examination reveals a flexible hindfoot valgus, an inability to perform a single-leg heel rise, and a positive 'too-many-toes' sign. Conservative management has failed. What is the most appropriate surgical intervention?
Explanation
Question 90
A 38-year-old recreational athlete sustains an acute Achilles tendon rupture. He is counseled on nonoperative versus operative management. Based on recent literature, which of the following is true regarding nonoperative management utilizing an early functional rehabilitation protocol compared to traditional operative repair?
Explanation
Question 91
A 58-year-old man with poorly controlled diabetes presents with a red, hot, swollen right foot for 2 weeks. He denies trauma or skin ulceration. Radiographs show soft tissue swelling but no bony destruction or periosteal reaction. Inflammatory markers are within normal limits. What is the most appropriate initial management?
Explanation
Question 92
A 28-year-old man undergoes open reduction and internal fixation of a supination-external rotation type IV ankle fracture. Intraoperatively, after rigid fixation of the lateral malleolus, the Cotton test demonstrates 4 mm of lateral shift of the fibula relative to the tibia. What is the next most appropriate step in management?
Explanation
None
