Distal Femoral Extension Osteotomy and Patellar Advancement for Crouch Gait

Key Takeaway
Join us in the OR for a masterclass on correcting crouch gait through distal femoral extension osteotomy and patellar advancement. We'll meticulously cover patient selection, precise surgical anatomy, detailed intraoperative steps, critical pearls for success, and comprehensive postoperative management to restore optimal knee function and improve ambulation in complex neuromuscular conditions like cerebral palsy.
Comprehensive Introduction and Patho-Epidemiology
Crouch gait represents one of the most mechanically devastating and therapeutically challenging ambulatory patterns encountered in the realm of pediatric orthopedic surgery and neuro-orthopedics. Defined kinematically by excessive and persistent knee flexion during the stance phase of the gait cycle, this pathology is predominantly observed in patients with spastic diplegic cerebral palsy, though it may also manifest in other neuromuscular conditions such as myelomeningocele. The transition from a dynamic, spasticity-driven crouch in early childhood to a rigid, fixed musculoskeletal deformity in adolescence marks a critical juncture where conservative management fails, and complex surgical intervention becomes an absolute necessity.
The patho-epidemiology of crouch gait is intrinsically linked to the concept of "lever arm dysfunction" and the failure of the plantarflexion-knee extension couple. In a physiologically normal gait pattern, the soleus muscle acts to decelerate the forward progression of the tibia over the plantigrade foot during mid-to-late stance. When the soleus is compromised—often iatrogenically through overzealous heel cord lengthening or intrinsically due to profound weakness—the tibia translates anteriorly unrestrained. This anterior translation shifts the ground reaction force (GRF) vector posterior to the knee joint center, generating a massive external flexion moment. To prevent collapse, the quadriceps must fire continuously and forcefully throughout stance, leading to rapid fatigue, increased energy expenditure, and progressive muscle failure.
As this pathological biomechanical environment persists into adolescence, structural adaptations occur. The two-joint muscles, including the hamstrings, rectus femoris, and gastrocnemius, develop severe musculotendinous contractures. Conversely, the critical one-joint postural muscles, particularly the gluteus maximus, vastus medialis/lateralis, and soleus, become chronically elongated and profoundly weakened. The relentless, heightened quadriceps contraction against a flexed knee exponentially increases patellofemoral joint reaction forces. Over time, this constant tensile stress elongates the patellar tendon, resulting in severe patella alta. The patella loses its mechanical advantage as a fulcrum, and the extensor mechanism becomes functionally incompetent, culminating in a fixed knee flexion deformity and an inability to achieve terminal extension, clinically recognized as an extensor lag.
The definitive surgical management of this complex, multi-level pathology requires a comprehensive approach, most effectively addressed through a distal femoral extension osteotomy (DFEO) combined with patellar tendon advancement (PTA). This masterclass chapter delineates the precise anatomical considerations, rigorous preoperative planning, meticulous surgical execution, and phased rehabilitation necessary to safely restore the mechanical axis, tension the extensor mechanism, and salvage the ambulatory capacity of these complex patients.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the regional anatomy and the altered biomechanics of the spastic, contracted knee is paramount before undertaking a distal femoral extension osteotomy and patellar advancement. The surgical field encompasses the distal femoral metaphysis, the complex neurovascular anatomy of the popliteal fossa, and the intricate architecture of the anterior extensor mechanism.
Osteology and the Distal Femoral Physis
The distal femur is the primary site of our corrective osteotomy. We operate within the metaphyseal region, a highly vascularized zone of cancellous bone that affords rapid healing but requires precise implant purchase. In skeletally immature patients, the distal femoral physis is a critical landmark; it is the most active growth plate in the human body, contributing approximately 70% of the longitudinal growth of the femur and 40% of the total leg length (averaging 9-10 mm per year). The osteotomy must be meticulously planned and executed just proximal to this physis to avoid catastrophic growth arrest, which could lead to severe leg length discrepancies or angular deformities. In mature patients, the physeal scar serves as our distal boundary.
The geometry of the distal femur, specifically the relationship between the anterior cortex, the posterior condyles, and the epicondylar axis, dictates our implant positioning. The lateral femoral epicondyle serves as the entry point for our seating chisel and guidewire. The anterior cortex of the distal femur is relatively flat, while the posterior aspect diverges into the medial and lateral condyles, creating the intercondylar notch. Understanding this trapezoidal cross-section is essential when planning the wedge resection to ensure cortical apposition and rotational stability.
The Popliteal Fossa and Neurovascular Perils
The posterior aspect of the distal femur is intimately related to the popliteal fossa, a region fraught with neurovascular hazards that are profoundly exacerbated by the presence of a fixed flexion contracture. The popliteal artery, popliteal vein, and tibial nerve lie in close proximity to the posterior capsule of the knee and the posterior cortex of the femur. In a chronically flexed knee, these structures become contracted and tethered.
When performing an extension osteotomy, simply hinging the femur open anteriorly or closing a wedge posteriorly without concomitant femoral shortening places immense, potentially devastating traction on the sciatic nerve and the popliteal neurovascular bundle. This stretch can result in profound ischemic injury or neurapraxia. Therefore, the fundamental biomechanical principle of this procedure in the setting of severe contractures (>15-20 degrees) is to incorporate a shortening component into the osteotomy. By resecting a trapezoidal segment of bone rather than a simple wedge, we achieve "tension-free extension," decompressing the posterior structures while simultaneously correcting the angular deformity.
Patellofemoral Biomechanics and the Extensor Mechanism
The patellofemoral joint operates as a complex biomechanical pulley system. The patella increases the lever arm of the quadriceps force, maximizing mechanical advantage during knee extension. In crouch gait, the persistent flexion dramatically alters this dynamic. Patellofemoral joint reaction forces (PFJRF) are calculated by the formula: PFJRF = 2 * Quadriceps Force * sin(knee flexion angle / 2). As the knee remains flexed during weight-bearing, the required quadriceps force skyrockets, and the resultant PFJRF can exceed 7-8 times body weight.
This chronic, immense stress leads to plastic deformation and elongation of the patellar tendon, resulting in patella alta. The patella migrates proximally, often sitting entirely above the trochlear groove (loss of containment), which severely diminishes its mechanical advantage and contributes to the clinical extensor lag. Furthermore, this abnormal stress concentration frequently leads to fragmentation or stress fractures at the inferior pole of the patella, a pathognomonic finding in severe cerebral palsy crouch gait. Patellar advancement aims to physically translate the insertion of the patellar tendon distally, restoring the normal Insall-Salvati ratio, re-engaging the patella within the trochlea, and re-tensioning the quadriceps to eradicate the extensor lag.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of success in neuro-orthopedic surgery. The decision to proceed with a DFEO and PTA must be embedded within a comprehensive, single-event multilevel surgery (SEMLS) plan, addressing all primary and secondary lever arm dysfunctions simultaneously.
Indications for DFEO and PTA
The primary indication for this combined procedure is a patient with a neuromuscular disorder, most commonly spastic diplegic cerebral palsy, who exhibits a rigid, fixed knee flexion deformity that is refractory to conservative measures such as physical therapy, orthotics (AFOs/KAFOs), and serial casting. Clinically, this is defined as a fixed flexion contracture greater than 10 to 15 degrees, measured meticulously with a goniometer during an examination under anesthesia (EUA).
Concomitantly, the presence of patella alta and a significant knee extensor lag are absolute indications for the patellar advancement component. These patients typically fall within Gross Motor Function Classification System (GMFCS) levels I, II, or III, where the primary goal is the preservation and optimization of independent or assistive ambulation. Occasionally, the procedure is indicated in GMFCS level IV patients to facilitate standing transfers, improve wheelchair positioning, and alleviate severe anterior knee pain caused by patellar stress fractures or severe chondromalacia.
Contraindications and Cautions
Contraindications are equally critical to recognize to prevent disastrous postoperative functional decline. Severe, unaddressed hip flexion contractures represent a major contraindication; correcting the knee to full extension while the hip remains locked in flexion will force the patient's trunk forward, severely compromising balance and potentially leading to an inability to ambulate. Similarly, uncorrected severe foot and ankle deformities (e.g., profound equinovalgus or rigid planovalgus) that preclude a stable plantigrade foot will undermine the foundational mechanics required for the newly extended knee to function.
Profound, irreversible weakness of the primary extensor muscles (quadriceps and gluteus maximus) is a relative contraindication. If the underlying motor units are incapable of powering the newly aligned limb, the patient may lose their previous, albeit pathological, method of ambulation. Severe osteopenia, frequently seen in non-ambulatory or marginally ambulatory patients, is a technical contraindication that requires careful consideration, as it severely compromises the purchase of our fixation implants (blade plates or locking screws), increasing the risk of catastrophic hardware failure or loss of correction.
| Category | Indications | Contraindications |
|---|---|---|
| Clinical Presentation | Fixed knee flexion contracture > 15° | Dynamic crouch fully correctable with Botox/casting |
| Extensor Mechanism | Severe patella alta; Knee extensor lag | Normal patellar height; Competent extensor mechanism |
| Functional Status | GMFCS Levels I - III (Ambulatory decline) | Profound, global extensor weakness (Quad/Gluteal) |
| Concomitant Deformity | Addressed concurrently in SEMLS | Uncorrected severe hip flexion contracture |
| Bone Quality | Adequate bone stock for fixation | Severe, untreated osteopenia (relative) |
Pre-Operative Planning, Templating, and Patient Positioning
The execution of a flawless osteotomy begins weeks before the patient enters the operating theater. Rigorous preoperative planning, utilizing advanced kinematic data and precise radiographic templating, dictates the exact angles, wedge sizes, and hardware required.
Comprehensive Assessment and Gait Analysis
Clinical examination provides the foundation, but three-dimensional computerized gait analysis is the gold standard for quantifying the dynamic components of crouch gait. Kinematic data in the sagittal plane will graphically demonstrate the lack of terminal knee extension during stance and the degree of excessive flexion at initial contact. Kinetic data will reveal the persistent internal knee extensor moment, confirming the massive energy demands placed on the quadriceps. Electromyography (EMG) is utilized to assess the firing patterns of the rectus femoris and hamstrings, determining if concomitant spasticity management (e.g., fractional lengthening) is required.
Furthermore, gait analysis is critical for identifying rotational malalignments. Excessive femoral anteversion and external tibial torsion frequently accompany crouch gait, exacerbating lever arm dysfunction. If significant femoral anteversion is present, the distal femoral osteotomy can be modified to include a derotational component, addressing two deformities through a single bony cut.
Radiographic Templating and EUA
High-quality, standardized radiographs are mandatory. A true lateral radiograph of the knee, obtained with the patient supine and the knee forced into maximum extension (often utilizing a bolster under the ankle or distal tibia), is critical for measuring the true bony fixed flexion deformity. This angle dictates the size of the extension wedge to be removed. Patellar height is quantified using the Insall-Salvati ratio or the Koshino index to plan the exact distance of distal advancement required. Long-leg alignment films are scrutinized for any coronal plane deformities (varus or valgus) that must be corrected simultaneously.
Templating is performed meticulously. As a general surgical heuristic, 1 degree of angular correction corresponds to approximately 1 millimeter of wedge base at the anterior cortex, though this varies based on the anteroposterior diameter of the patient's femur. The examination under anesthesia (EUA) is the final, non-negotiable step before incision. With muscle tone abolished by paralytics, the surgeon confirms the absolute degree of fixed contracture, assesses the true range of motion, and finalizes the surgical blueprint.
Optimal Patient Positioning
The patient is positioned supine on a radiolucent operating table. This positioning is paramount as it affords simultaneous, unhindered access to both the lateral distal femur for the osteotomy and the anterior knee for the patellar advancement.
The operative extremity is prepped and draped entirely free, allowing the surgeon to manipulate the limb through a full, unrestricted range of motion. This mobility is essential for assessing the reduction of the osteotomy and evaluating the tension of the extensor mechanism post-advancement.

A sterile pneumatic tourniquet is applied as proximal on the thigh as possible to maximize the surgical working area while providing a bloodless field. This is critical when performing subperiosteal dissection near the posterior neurovascular structures. The fluoroscopy (C-arm) unit must be positioned contralateral to the operative side, ready to swing in for true anteroposterior (AP) and lateral projections without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands absolute precision, respect for soft tissue envelopes, and rigid biomechanical fixation. The procedure is conceptually divided into the distal femoral extension osteotomy and the subsequent patellar advancement.
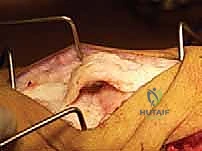
I. Distal Femoral Extension Osteotomy: Exposure and Preparation
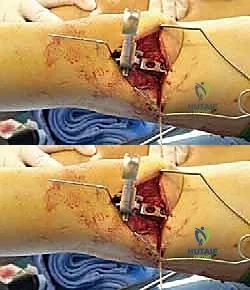
Following exsanguination and tourniquet inflation, a longitudinal lateral incision is made, extending 8 to 10 cm proximally from the lateral epicondyle, centered over the distal femoral metaphysis. The fascia lata is incised sharply in line with the skin incision. We utilize a vastus-splitting or vastus-elevating approach. Using a Cobb elevator, the vastus lateralis is meticulously elevated from its origin on the lateral intermuscular septum and retracted anteriorly.
This subperiosteal dissection is critical; it must be completely bloodless and remain strictly deep to the periosteum to protect the perforating vessels and the muscle belly. Once the lateral, anterior, and posterior cortices are exposed, blunt, curved, circumferential subperiosteal retractors (such as Chandler or Hohmann retractors) are carefully placed. The posterior retractor is the most critical instrument in the field at this moment—it must sit flush against the posterior femoral cortex, acting as a physical shield to protect the popliteal artery, vein, and tibial nerve from the oscillating saw.
II. Guidewire Placement and Chisel Seating
The accuracy of the initial guidewire dictates the success of the entire osteotomy. We utilize a 90-degree adolescent or adult AO blade plate, depending on patient size. The entry point is the anterior half of the lateral femoral epicondyle, just proximal to the distal femoral physis (or physeal scar).
Under AP fluoroscopy, the guidewire is driven parallel to the joint line. Crucially, the C-arm must be orthogonal to the tibia, not the flexed femur. The guidewire must be perfectly perpendicular to the mechanical axis of the tibia in the coronal plane to avoid inducing iatrogenic varus or valgus.
Switching to the lateral fluoroscopic view, the seating chisel guide is introduced. The angle of the chisel guide relative to the femoral shaft is the most critical geometric maneuver of the procedure. The chisel guide must be aligned perfectly parallel to the anterior crest of the tibia.


By aligning the chisel parallel to the tibia, the angle created between the chisel and the femoral shaft exactly equals the degree of the fixed flexion deformity. The seating chisel is then driven into the distal metaphysis over the guidewire, creating the track for the blade plate.
III. The Osteotomy and Deformity Correction
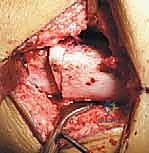
With the chisel track established, the osteotomy is performed. For severe contractures (>15 degrees), a simple anterior closing wedge is insufficient and dangerous due to posterior neurovascular tethering. Instead, we perform a shortening extension osteotomy.

Two cuts are made with an oscillating saw under continuous saline irrigation to prevent thermal necrosis. The distal cut is made parallel to the chisel track. The proximal cut is made perpendicular to the femoral shaft. The distance between these two cuts at the anterior cortex determines the degree of extension, while the distance at the posterior cortex determines the amount of femoral shortening.

Once the trapezoidal bone segment is carefully removed, the knee is gently extended. The posterior cortex must not act as a hinge that distracts the posterior structures; rather, the distal fragment should translate slightly posteriorly and proximally, decompressing the popliteal fossa.
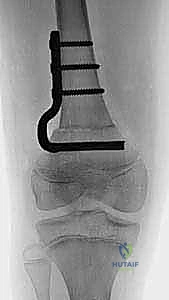
IV. Fixation and Patellar Advancement
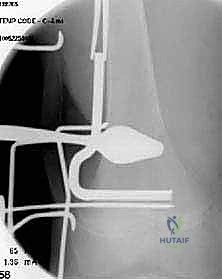
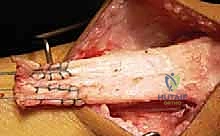
The pre-selected 90-degree blade plate is inserted into the pre-cut chisel track in the distal fragment.

As the knee is brought into full extension, the side plate of the implant is approximated to the lateral cortex of the proximal femoral shaft.

The osteotomy is compressed using an articulated tension device, and the plate is rigidly secured to the proximal fragment with bicortical screws.
With the femur now straight, attention turns to the anterior knee. A midline or parapatellar incision exposes the extensor mechanism.

In skeletally immature patients, we absolutely cannot violate the tibial tubercle apophysis with a bony block transfer. Therefore, a soft tissue advancement is performed. The patellar tendon is sharply detached from its insertion, or a coronal Z-lengthening/imbrication technique is utilized. The patella is pulled distally into the trochlear groove, restoring the Insall-Salvati ratio to approximately 1.0.
The tendon is rigidly repaired using heavy, non-absorbable transosseous sutures through the proximal tibial metaphysis (distal to the apophysis).

The knee is flexed to 30-40 degrees to confirm secure fixation without excessive tension that could lead to rupture or severe chondromalacia.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and execution, DFEO and PTA are major interventions with a recognized complication profile. The surgical team must be acutely aware of these risks and prepared to execute salvage protocols immediately.
Neurovascular Compromise
The most devastating complication is injury to the posterior neurovascular bundle. Direct laceration by the oscillating saw is rare if circumferential retractors are utilized correctly. However, traction neurapraxia (specifically of the sciatic or tibial nerve) or arterial spasm/intimal tear due to stretching is a significant risk if adequate femoral shortening is not achieved during the correction of severe contractures. Incidence of transient nerve palsy ranges from 2% to 5%. If a patient awakens with a profound neurologic deficit, immediate removal of the cast/brace and slight flexion of the knee to relieve tension is mandatory. If vascular compromise is suspected (loss of pulses, poor capillary refill), emergent vascular surgery consultation and exploration are required.
Hardware Failure and Nonunion
Given the massive lever arms and forces crossing the knee joint, loss of fixation or delayed union/nonunion can occur, particularly in patients with severe osteopenia or those who are non-compliant with postoperative weight-bearing restrictions. The incidence of nonunion is generally low (<3%) given the metaphyseal location of the osteotomy, but hardware pullout can occur. Salvage management requires revision open reduction and internal fixation (ORIF), often utilizing longer, locking plates, bone grafting (autograft or allograft), and potentially extending the period of rigid immobilization.
Extensor Mechanism Complications
Complications related to the patellar advancement include patellar tendon rupture, avulsion of the repair, or over-tensioning leading to severe patellofemoral pain and chondrolysis. Over-tensioning can also restrict knee flexion, severely impacting the swing phase of gait. If the tibial tubercle apophysis is inadvertently violated in a growing child, a premature anterior growth arrest can occur, leading to a progressive, iatrogenic genu recurvatum deformity. This requires complex reconstructive surgery, potentially including proximal tibial osteotomies, to salvage the mechanical axis.
| Complication | Estimated Incidence | Etiology / Risk Factor | Salvage / Management Strategy |
| :--- | :--- | :--- |
