Orthopedic Board Review MCQs (2026 Edition) - Part 3

Orthopedic Board Review MCQs (2026 Edition) - Part 3
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). At the 2-week follow-up, the parents report the infant has stopped kicking the affected leg. On examination, the knee is held in flexion, and the infant demonstrates absent active knee extension, though passive motion is full and pain-free. What is the most appropriate next step in management?
Explanation
Question 2
During the ilioinguinal approach for an acetabular fracture, significant hemorrhage is encountered upon dissecting over the superior pubic ramus. This bleeding is most likely originating from an anastomotic vessel connecting the obturator system and which of the following vessels?
Explanation
Question 3
Which zone of articular cartilage contains the highest concentration of proteoglycans and the lowest concentration of water?
Explanation
Question 4
A 15-year-old boy presents with progressive, severe diaphyseal tibial pain that is characteristically worse at night and rapidly relieved by ibuprofen.
Radiographs show a dense sclerotic cortical thickening with a small radiolucent nidus. Which of the following best describes the pathophysiologic mechanism of this pain?

Explanation
Question 5
A 14-year-old gymnast presents with persistent lower back pain. Radiographs demonstrate an isthmic spondylolisthesis at L5-S1. If this patient's slip progresses to a high-grade slip (>50%), which of the following spinopelvic parameters is most likely to be significantly elevated as a compensatory mechanism to maintain sagittal balance?
Explanation
Question 6
In total hip arthroplasty (THA), the use of highly cross-linked polyethylene (HXLPE) has significantly reduced wear rates compared to conventional polyethylene. However, the process of cross-linking via irradiation alters the material's mechanical properties. Which of the following best describes a mechanical trade-off associated with high-dose irradiation cross-linking?
Explanation
Question 7
A 60-year-old man undergoes an arthroscopic massive rotator cuff repair. During the procedure, the surgeon releases the coracohumeral ligament to mobilize the retracted supraspinatus tendon. The coracohumeral ligament plays a critical biomechanical role in restricting which of the following shoulder motions?
Explanation
Question 8
Following a Zone II flexor tendon repair of the index finger in a 30-year-old construction worker, the surgeon opts for an early active motion protocol. Which of the following core suture techniques provides the highest initial tensile strength and resistance to gap formation?
Explanation
Question 9
A 55-year-old patient with long-standing, poorly controlled type 2 diabetes presents with an acutely swollen, red, and warm left foot. Radiographs demonstrate early fragmentation and periarticular debris at the tarsometatarsal joints. Which of the following pro-inflammatory cytokines/pathways is considered the primary driver of osteoclastogenesis and bone resorption in the acute phase of Charcot neuroarthropathy?
Explanation
Question 10
A 22-year-old male sustains a closed comminuted tibial shaft fracture. Twelve hours post-admission, he develops severe pain out of proportion to the injury, exacerbated by passive stretch of the hallux. Intracompartmental pressure monitoring is performed. Which of the following pressure measurements is generally considered the threshold for performing an emergency four-compartment fasciotomy?
Explanation
Question 11
Which of the following classes of nerve injury, according to the Sunderland classification, represents a complete disruption of axons and endoneurium, while the perineurium and epineurium remain intact?
Explanation
Question 12
A 13-year-old obese male presents with a 3-week history of left thigh pain and a limp. Examination reveals obligate external rotation upon flexing the left hip. Radiographs confirm a stable Slipped Capital Femoral Epiphysis (SCFE). During in situ single-screw fixation, to minimize the risk of avascular necrosis (AVN), the screw should ideally be positioned in which quadrant of the femoral head?
Explanation
Question 13
A 45-year-old woman presents to the emergency department with acute onset of severe lower back pain, bilateral sciatica, saddle anesthesia, and urinary retention with overflow incontinence. An emergent MRI confirms a massive L4-L5 central disc herniation.
What is the pathophysiologic mechanism leading to the bladder dysfunction in this syndrome?

Explanation
Question 14
In native knee kinematics, 'femoral rollback' is the posterior translation of the femoral contact point on the tibia during deep flexion, which increases clearance and allows greater flexion. Which structure is the primary anatomic driver of this obligatory posterior rollback?
Explanation
Question 15
A 28-year-old professional baseball pitcher presents with vague, deep shoulder pain and decreased throwing velocity. An MR arthrogram demonstrates a detachment of the superior labrum from anterior to posterior, with the biceps anchor completely detached from the glenoid. According to the Snyder classification, what type of SLAP tear is this?
Explanation
Question 16
A 65-year-old man presents with generalized bone pain, fatigue, and a recent pathological fracture of his proximal humerus. Laboratory workup reveals hypercalcemia and anemia. Serum protein electrophoresis shows a monoclonal spike. Radiographs demonstrate multiple 'punched-out' lytic lesions in his skull and pelvis. Which of the following is the most definitive diagnostic test to confirm the underlying primary pathology?
Explanation
Question 17
When utilizing a lag screw for interfragmentary compression in fracture fixation, which of the following mechanical properties most effectively increases the pull-out strength of the screw in cancellous bone?
Explanation
Question 18
A 75-year-old female undergoes retrograde intramedullary nailing for a supracondylar femur fracture (AO/OTA 33-A1).
To avoid an intra-articular deformity, the starting point for the nail must be perfectly collinear with the anatomical axis of the femur. Which of the following describes the correct starting point for a retrograde femoral nail?
Explanation
Question 19
In the Ponseti method for the treatment of idiopathic clubfoot, a specific sequence of deformity correction is strictly followed to avoid creating a midfoot breach (rocker-bottom deformity). Which of the following represents the correct sequential order of correction?
Explanation
Question 20
A 40-year-old cyclist presents with numbness and tingling confined entirely to the volar aspect of the ring and small fingers, with profound weakness of the intrinsic hand muscles. Sensation on the dorsal aspect of the ulnar hand is completely normal.
At which anatomical location is the ulnar nerve most likely compressed?

Explanation
Question 21
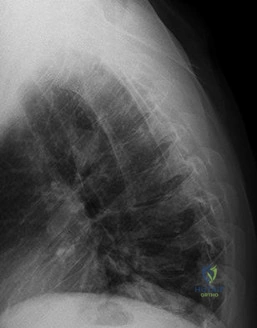
A 12-year-old obese male presents with chronic left groin pain and an obligatory slip into external rotation with passive hip flexion. Radiograph of the hip is shown.
Which of the following represents the strongest indication for prophylactic in situ pinning of the contralateral, asymptomatic hip in a patient with a Slipped Capital Femoral Epiphysis (SCFE)?
Explanation
Question 22
Which of the following anatomical landmarks is the correct target for the optimal placement of a circumferential pelvic sheet or binder to reduce an open book pelvic ring injury in the trauma bay?
Explanation
Question 23
A 22-year-old collegiate football player sustains a valgus and twisting injury to his knee. MRI confirms a complete proximal tear of the medial collateral ligament (MCL) and an anterior cruciate ligament (ACL) rupture. What is the most appropriate initial management protocol?
Explanation
Question 24
Denosumab is increasingly utilized in the treatment of unresectable or recurrent Giant Cell Tumor (GCT) of bone. What is its exact mechanism of action?
Explanation
Question 25
A 35-year-old male presents with a swollen, exquisitely tender index finger 3 days after sustaining a puncture wound.
Suppurative flexor tenosynovitis is suspected. Which of the following is NOT a classic Kanavel sign?

Explanation
Question 26
A 40-year-old driver is involved in a high-speed motor vehicle collision, sustaining a traumatic spondylolisthesis of the axis (Hangman's fracture). Imaging shows severe angulation and >3 mm of translation with bilateral facet dislocations. According to the Levine-Edwards classification, this is a Type III fracture. What is the primary mechanism of injury?
Explanation
Question 27
A 55-year-old male who underwent a ceramic-on-ceramic total hip arthroplasty 3 years ago presents to the clinic complaining of a loud 'squeaking' sound coming from his hip when he walks. He denies pain. Which of the following component malpositions is most strongly associated with this complication?
Explanation
Question 28
A 24-year-old equestrian falls from a horse, trapping her foot in the stirrup.
A Lisfranc injury is suspected based on midfoot swelling and plantar ecchymosis. The primary Lisfranc ligament anatomically connects which two osseous structures?

Explanation
Question 29
Demineralized bone matrix (DBM) is widely used as a bone graft substitute in spinal fusions. Based on its biological composition, which of the following properties does DBM possess?
Explanation
Question 30
A 10-year-old boy sustains a Salter-Harris II fracture of the distal femur. Despite an anatomic closed reduction and casting, the patient develops a significant leg length discrepancy 2 years later. Which of the following is the approximate historical rate of physeal growth arrest associated with distal femoral physeal fractures?
Explanation
Question 31
A 35-year-old construction worker falls from a ladder, sustaining an intra-articular calcaneus fracture.
If an extensile lateral approach is utilized for open reduction and internal fixation, which anatomical structure is at highest risk of injury during the elevation of the inferior aspect of the full-thickness flap?
Explanation
Question 32
A 19-year-old competitive swimmer presents with bilateral shoulder pain and a sensation of subluxation. Clinical examination reveals a positive sulcus sign and generalized ligamentous laxity. Following an intensive 6-month physical therapy regimen focusing on periscapular and rotator cuff stabilization, she remains highly symptomatic. What is the most appropriate surgical intervention?
Explanation
Question 33
A 65-year-old female presents with severe thoracic back pain, fatigue, and anemia. Workup reveals multiple lytic bone lesions without sclerotic rims. Which cytokine is primarily responsible for the marked osteoclast activation and resulting osteolytic lesions in this disease process?
Explanation
Question 34
A 22-year-old male falls on an outstretched hand and sustains a proximal pole scaphoid fracture. The risk of avascular necrosis is high due to the retrograde nature of the scaphoid's blood supply. Which artery provides the primary blood supply to the proximal pole of the scaphoid?
Explanation
Question 35
A 70-year-old male with confirmed cervical spondylotic myelopathy undergoes a thorough neurologic examination. The examiner elicits a positive Hoffman's sign. This finding indicates a lesion involving which of the following neurologic tracts?
Explanation
Question 36
In the pathogenesis of aseptic loosening following total joint arthroplasty, submicron particulate polyethylene debris is generated and subsequently phagocytosed by local macrophages. Which of the following is the primary downstream effector cell directly responsible for the resulting periprosthetic bone resorption (osteolysis)?
Explanation
Question 37
A 40-year-old weekend warrior feels a distinct 'pop' in his heel while playing basketball.
A Thompson test is positive, confirming an acute Achilles tendon rupture. If the patient and surgeon agree on nonoperative management, which of the following describes the most appropriate and modern evidence-based protocol?

Explanation
Question 38
When analyzing the biomechanical properties of a viscoelastic orthopedic implant, the device is subjected to a constant applied load over a prolonged period. The material demonstrates a progressive, time-dependent increase in deformation. What is the correct biomechanical term for this phenomenon?
Explanation
Question 39
A 4-week-old female infant is currently undergoing treatment with a Pavlik harness for developmental dysplasia of the hip (DDH). At the 2-week follow-up appointment, the mother notes that the infant has stopped kicking her left leg, and the knee rests in a persistently extended position. What is the most likely iatrogenic cause of this finding?
Explanation
Question 40
During the open reduction and internal fixation of a 3-part proximal humerus fracture via a standard deltopectoral approach, preservation of the primary blood supply to the humeral head is a critical consideration. According to modern anatomical perfusion studies (e.g., Hettrich, Brooks), which vessel provides the vast majority of the blood supply to the humeral head?
Explanation
Question 41
A 65-year-old man presents with progressive clumsiness in his hands and difficulty walking. Examination reveals hyperreflexia in the lower extremities and a positive Hoffmann's sign.
MRI demonstrates severe canal stenosis at C5-C6. If this patient has a pure C6 radiculopathy superimposed on his myelopathy, which of the following physical exam findings would most likely be present?
Explanation
Question 42
A 12-year-old boy presents with a left-sided slipped capital femoral epiphysis (SCFE). He is noticeably short for his age and has a documented history of hypothyroidism. What is the most appropriate management regarding his completely asymptomatic, radiographically normal contralateral right hip?
Explanation
Question 43
A 32-year-old male presents with a slow-growing, painful mass in his left thigh. MRI reveals a deep soft tissue mass adjacent to the knee joint. Biopsy demonstrates a biphasic tumor with both epithelial and spindle cell components. Which of the following cytogenetic abnormalities is pathognomonic for this sarcoma?
Explanation
Question 44
Articular cartilage consists of multiple distinct histologic zones, each contributing to its unique biomechanical properties. Which of the following characteristics best describes the deep zone of normal adult articular cartilage?
Explanation
Question 45
A 28-year-old man sustains a talar neck fracture following a motor vehicle collision. Six weeks postoperatively, a plain radiograph reveals a subchondral radiolucent band in the dome of the talus (Hawkins sign).
What does this radiographic finding indicate?
Explanation
Question 46
In the surgical management of a 'terrible triad' injury of the elbow (elbow dislocation, radial head fracture, and coronoid fracture), which of the following sequences is the standard recommended approach for reconstruction to restore stability?
Explanation
Question 47
During a primary total knee arthroplasty (TKA), trial components are inserted. The knee is symmetric and stable in full extension, but the flexion space is excessively tight, preventing full flexion. Which of the following surgical modifications is the most appropriate next step to correct this mismatch?
Explanation
Question 48
The Lisfranc ligament is a critical structure for midfoot stability. Between which two bones does the primary, most substantial band (interosseous portion) of the Lisfranc ligament course?
Explanation
Question 49
In the surgical management of developmental dysplasia of the hip (DDH), various pelvic osteotomies can be utilized to improve coverage.
Which of the following best describes the biomechanical principle of a Pemberton osteotomy?
Explanation
Question 50
The anterior cruciate ligament (ACL) consists of two distinct functional bundles: the anteromedial (AM) and posterolateral (PL) bundles. Which of the following best describes the biomechanical function and tensioning of these bundles during knee range of motion?
Explanation
Question 51
A 30-year-old woman presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the distal femur. Biopsy confirms a Giant Cell Tumor (GCT) of bone.
Denosumab is considered for neo-adjuvant treatment to consolidate the tumor rim. What is the specific cellular target of denosumab in the pathogenesis of this tumor?
Explanation
Question 52
A 25-year-old male sustains a Pauwels type III (vertical) femoral neck fracture. Biomechanically, what is the primary mode of failure for this specific fracture pattern if treated inadequately with three parallel cancellous lag screws?
Explanation
Question 53
During primary repair of a Zone II flexor tendon laceration in the hand, preserving the integrity of the flexor tendon sheath and pulley system is imperative to ensure optimal finger kinematics. Biomechanically, which two pulleys are the most critical to preserve or reconstruct to prevent bowstringing of the flexor tendons?
Explanation
Question 54
A 68-year-old female presents with severe neurogenic claudication. Imaging reveals an L4-L5 degenerative spondylolisthesis.
In the pathogenesis of this condition, the facet joints typically undergo remodeling and become more sagittally oriented. This orientation most directly permits which type of abnormal motion?
Explanation
Question 55
A 40-year-old recreational athlete sustains an acute complete Achilles tendon rupture. Based on high-quality randomized controlled trials (e.g., Willits et al.), which of the following statements is true regarding non-operative management utilizing an early functional rehabilitation protocol compared to traditional open surgical repair?
Explanation
Question 56
In orthopedic implant manufacturing, the mechanical properties of an alloy dictate its behavior within the host bone. Which of the following standard solid metallic biomaterials exhibits the lowest modulus of elasticity, thereby minimizing stress shielding when utilized as a diaphyseal stem?
Explanation
Question 57
A 16-year-old female undergoes medial patellofemoral ligament (MPFL) reconstruction for recurrent lateral patellar instability.
To ensure proper graft isometry during knee flexion, where must the femoral attachment of the graft be placed anatomically?
Explanation
Question 58
A 2.5-year-old boy presents with progressive bilateral genu varum and an asymmetric waddling gait. Standing long-leg radiographs demonstrate medial metaphyseal beaking and a metaphyseal-diaphyseal angle (MDA) of 20 degrees bilaterally. What is the most appropriate initial management?
Explanation
Question 59
A 19-year-old male presents with deep, boring thigh pain that is significantly worse at night and dramatically relieved by oral ibuprofen. A CT scan is obtained
demonstrating a 1 cm radiolucent nidus surrounded by dense, reactive sclerotic cortical bone in the femoral diaphysis. What is the primary biochemical mediator responsible for this characteristic pain pattern?
Explanation
Question 60
In the surgical treatment of complex intra-articular distal radius fractures, a volar marginal fragment involving the lunate facet (the 'lunate drop-out' or 'Melone' fragment) is notoriously difficult to capture with standard fixed-angle volar locking plates. Failure to secure this specific fragment most commonly results in which of the following complications?
Explanation
Question 61
During a Kocher-Langenbeck approach for an acetabular fracture, the surgeon must be mindful of protecting the sciatic nerve. What is the optimal positioning of the lower extremity to minimize tension on the sciatic nerve during retraction?
Explanation
Question 62
A 24-year-old rugby player undergoes a Latarjet procedure for recurrent anterior shoulder instability with 25% glenoid bone loss. During the transfer of the coracoid process, which of the following nerves is at greatest risk of injury and must be carefully protected?
Explanation
Question 63
A 28-year-old male sustains a knee injury during a soccer tackle. Physical examination reveals a positive dial test at 30 degrees of knee flexion with 15 degrees of increased external rotation compared to the contralateral side. At 90 degrees of knee flexion, the external rotation is symmetric bilaterally. Which of the following structures is most likely injured?
Explanation
Question 64
A 9-year-old boy whose weight is in the 95th percentile presents with groin pain and an obligatory external rotation of the hip with passive flexion. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Given the patient's age, which of the following underlying conditions should be investigated?
Explanation
Question 65
Which of the following biomechanical parameters has the most significant influence on increasing the pullout strength of a pedicle screw in spinal fixation?
Explanation
Question 66
A 6-year-old child sustains a severely displaced Type III supracondylar humerus fracture. Upon arrival, the hand is pink but pulseless. After closed reduction and percutaneous pinning, the hand remains pink and pulseless. Doppler ultrasound confirms biphasic signals in the palmar arch. What is the most appropriate next step in management?
Explanation
Question 67
A 35-year-old male presents with a deep, painless mass in the distal thigh. A core needle biopsy reveals a biphasic histologic pattern composed of epithelial and spindle cells. Cytogenetic analysis is most likely to identify which of the following translocations?
Explanation
Question 68
During a primary total knee arthroplasty (TKA), the surgeon evaluates the trial components and finds that the knee is perfectly balanced and symmetric in full extension, but significantly tight in 90 degrees of flexion. Which of the following adjustments is the most appropriate next step to balance the knee?
Explanation
Question 69
A 45-year-old poorly controlled diabetic patient presents with an acutely swollen, erythematous, and warm right foot. There are no open ulcers. Radiographs demonstrate periarticular debris, fragmentation, and subluxation at the tarsometatarsal joints. What is the most appropriate initial management?
Explanation
Question 70
During an open Latarjet procedure for recurrent anterior shoulder instability, the coracoid process is osteotomized and transferred. Which of the following neural structures must be meticulously protected as it enters the conjoint tendon approximately 3-5 cm distal to the coracoid tip?
Explanation
Question 71
Which of the following statements correctly describes the cellular pathophysiology of a Giant Cell Tumor (GCT) of bone?
Explanation
Question 72
In a patient undergoing revision of a metal-on-metal total hip arthroplasty, intraoperative findings include a cystic pseudotumor. Histopathology of the periprosthetic tissue reveals a pronounced perivascular lymphocytic infiltrate. This finding is most characteristic of which condition?
Explanation
Question 73
An anterior cervical discectomy and fusion (ACDF) is planned via the Smith-Robinson approach. Which fascial interval is utilized, and why is the right-sided approach considered to have a higher risk to the recurrent laryngeal nerve?
Explanation
Question 74
A 12-year-old boy undergoes in situ single screw fixation for a stable slipped capital femoral epiphysis (SCFE). Over the next 6 months, he develops severe hip stiffness, pain, and a concentric loss of joint space on radiographs. This complication is most strongly associated with which intraoperative error?
Explanation
Question 75
A 25-year-old male is brought to the trauma bay after a motorcycle accident. He has an open-book pelvic ring injury with hemodynamic instability. To effectively close the pelvic volume, a circumferential pelvic sheet or binder should be placed at the level of the:
Explanation
Question 76
A patient with Scapholunate Advanced Collapse (SLAC) wrist presents for surgical intervention. Radiographs reveal advanced osteoarthritis at the radioscaphoid and capitolunate joints, but the radiolunate joint is completely spared. Which of the following procedures is most appropriate?
Explanation
Question 77
During the posteromedial approach for fixation of a split-depression medial tibial plateau fracture, the optimal surgical interval to expose the posterior aspect of the medial tibial condyle is between the medial head of the gastrocnemius and which anterior structure?
Explanation
Question 78
An athlete undergoes anterior cruciate ligament (ACL) reconstruction. Post-operatively, he complains of anterior knee pain and a lack of terminal extension. MRI demonstrates the graft impinging against the intercondylar roof in extension. Which technical error is the most likely cause of this complication?
Explanation
Question 79
A 28-year-old painter accidentally discharges a high-pressure paint gun against the volar tip of his index finger. He presents 2 hours later with a small puncture wound, mild swelling, minimal pain, and intact capillary refill. What is the most appropriate management?
Explanation
Question 80
When initiating the Ponseti method of serial casting for an infant born with idiopathic talipes equinovarus (clubfoot), what is the correct sequence of deformity correction?
Explanation
Question 81
A 65-year-old male with long-standing ankylosing spondylitis presents to the emergency department after a ground-level fall. He complains of severe lower neck pain but has no focal neurologic deficits. Initial anteroposterior and lateral plain radiographs of the cervical spine show flowing osteophytes but no obvious fracture. What is the most critical next step?
Explanation
Question 82
Which of the following is considered an absolute indication for operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 83
A patient sustains an isolated, closed transverse fracture of the humeral shaft. During non-operative management with a functional brace, primary healing occurs via endochondral ossification. If rigid internal fixation with a compression plate had been used instead, bone healing would primarily depend on which of the following cellular processes?
Explanation
Question 84
A 25-year-old professional baseball pitcher presents with vague, deep shoulder pain and clicking during the late cocking phase of throwing. He is diagnosed with a Type II Superior Labrum Anterior and Posterior (SLAP) tear. What is the primary biomechanical mechanism causing this pathology in this patient population?
Explanation
None
