Orthopedic Board Review MCQs (2026 Edition) - Part 4

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Board Review MCQs (2026 Edition) - Part 4
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old female presents with progressive thoracolumbar scoliosis. Imaging reveals a Cobb angle of 65 degrees from T9-L3, with significant sagittal decompensation (T1 pelvic angle of 35 degrees, pelvic incidence 55 degrees, lumbar lordosis -30 degrees). She experiences worsening back pain and trunk shift. Prior bracing failed to halt progression.
Which of the following surgical strategies is most appropriate to address her deformity and sagittal balance?

Explanation
Question 2
A 28-year-old professional dancer presents with chronic groin pain, particularly with deep flexion and internal rotation. MRI with arthrogram reveals a large cam lesion with an alpha angle of 80 degrees, a pincer lesion with acetabular retroversion, and a superior labral tear with chondral delamination. Diagnostic injection provides temporary relief.
Given these findings, what is the most appropriate definitive management strategy?
Explanation
Option A (arthroscopic labral debridement and cam osteoplasty only) is insufficient as it fails to address the pincer lesion and the possibility of labral repair instead of debridement.
Option B (open surgical dislocation with acetabular osteotomy, femoral osteochondroplasty, and labral repair) is a more invasive option usually reserved for very complex deformities, severe articular damage requiring direct access, or cases where arthroscopic treatment has failed. For an active dancer with chronic but treatable FAI, arthroscopy is generally preferred as the first-line surgical treatment due to lower morbidity and faster recovery if successful.
Option D (conservative management) has already failed, and given the significant mechanical impingement and structural damage (chondral delamination), it is unlikely to provide long-term relief or prevent progression of arthritis.
Option E (Periacetabular osteotomy - PAO) is indicated for developmental dysplasia of the hip (DDH) to improve acetabular coverage, not typically for isolated FAI with acetabular retroversion. Acetabular retroversion is addressed by rim trimming (acetabuloplasty), not a PAO.
Question 3
A 72-year-old male presents with chronic, intractable right shoulder pain and inability to actively elevate his arm above 60 degrees. X-rays
show severe glenohumeral osteoarthritis with significant superior migration of the humeral head and erosion of the acromion, consistent with rotator cuff arthropathy (Hamada Type IV). He has no prior shoulder surgery. Which of the following arthroplasty options is most likely to restore functional range of motion and pain relief?

Explanation
Anatomic total shoulder arthroplasty (TSA) (Option B) relies on an intact, functional rotator cuff for stability and active motion. It is contraindicated in rotator cuff arthropathy because the deficient cuff cannot center the humeral head, leading to early failure, instability, and poor outcomes.
Hemiarthroplasty (Option A) also relies on the rotator cuff and often provides unpredictable pain relief and poor functional outcomes in the setting of rotator cuff arthropathy.
Shoulder arthrodesis (Option D) provides pain relief and stability but at the expense of motion, which is generally not preferred for an active patient unless other options are contraindicated or failed.
Debridement arthroplasty (Option E) is a palliative procedure for pain relief, often with limited functional improvement, and is typically reserved for low-demand patients or those unable to undergo more complex procedures.
Reverse total shoulder arthroplasty (rTSA) (Option C) is the treatment of choice for rotator cuff arthropathy. The rTSA design medializes the center of rotation and recruits the deltoid muscle to power abduction and elevation, compensating for the deficient rotator cuff. It reliably improves pain and restores functional active elevation in patients with rotator cuff arthropathy. Therefore, rTSA is the most appropriate option to restore functional range of motion and pain relief for this patient.
Question 4
A 35-year-old male sustained a high-energy knee injury in a motor vehicle collision. Clinical examination reveals a gross posterolateral rotatory instability, a positive dial test at 30 and 90 degrees, a grade III posterior sag, and an absent posterior drawer. Foot drop is noted. MRI confirms avulsion of the PCL from the tibia, rupture of the fibular collateral ligament (FCL), and injury to the popliteus tendon.
What is the most critical immediate concern that dictates the timing and approach to surgical management?

Explanation
Option A (post-traumatic arthritis) is a long-term complication but not an immediate concern dictating surgical timing.
Option B (common peroneal nerve injury) is critical. Foot drop indicates significant nerve dysfunction, which needs to be addressed promptly. Surgical exploration and nerve repair or neurolysis may be necessary, and the presence of this neurological deficit often influences the timing and urgency of surgical intervention. Early diagnosis and management of nerve injuries are crucial for potential recovery.
Option C (severity of PCL avulsion) is significant for surgical planning, but the nerve injury adds another layer of complexity and urgency.
Option D (early mobilization to prevent stiffness) is important post-surgery but is not the most critical immediate concern pre-operatively, especially when compared to acute nerve injury.
Option E (neurovascular compromise and compartment syndrome) is a critical immediate concern in any high-energy knee injury, especially dislocations. However, the question specifically states 'foot drop is noted,' identifying a definite neurological injury rather than just a potential for neurovascular compromise. If a popliteal artery injury was present, it would be the absolute highest priority, but a peroneal nerve injury is also very high priority. Given the options, the presence of an already identified foot drop makes the nerve injury the most critical factor listed that dictates the immediate approach to surgical management, potentially requiring specific nerve interventions concurrently with or preceding ligamentous reconstruction.
Question 5
A 58-year-old diabetic male presents with an acutely swollen, red, and warm left foot, without an open wound. Radiographs, shown here, reveal disorganized joint architecture, subluxation, and fragmentation of the midfoot bones, consistent with Charcot neuroarthropathy (Eichenholtz Stage 1). ESR and CRP are mildly elevated, and WBC count is normal. He reports numbness in both feet.
What is the cornerstone of initial non-surgical management for this condition?

Explanation
Total contact casting (TCC) (Option C) is considered the gold standard for offloading and immobilizing the acute Charcot foot. It distributes pressure evenly across the plantar surface, reduces stress on compromised areas, and accommodates swelling. This is a much more effective and crucial method of immobilization and offloading compared to rigid foot orthoses (Option B), which might be used in later, quiescent stages or for maintenance but are insufficient for the acute phase.
Option A (broad-spectrum oral antibiotics) is incorrect as there is no strong evidence of infection. While differentiation from infection can be challenging, the absence of an open wound and normal WBC count make it less likely to be the primary management.
Option D (immediate surgical stabilization) is generally reserved for severe instability, gross deformity that prevents bracing, or failed conservative management, and is typically not the first-line treatment for an acute Charcot foot.
Option E (NSAIDs and elevation) may help with swelling and pain but does not address the fundamental need for strict offloading and immobilization to protect the bone and joint architecture.
Question 6
A 65-year-old active female sustains a comminuted intra-articular distal humerus fracture (AO/OTA 13-C3) after a fall. She is neurovascularly intact.
Given her age and activity level, what is the preferred surgical approach to achieve a durable functional outcome?

Explanation
For an active 65-year-old, preserving native elbow mechanics is paramount. Open reduction and internal fixation (ORIF) with dual plating using perpendicular constructs (Option A) is considered the gold standard for these complex fractures in patients with good bone quality who are active. This technique provides the necessary stability to allow for early rehabilitation and optimize long-term functional outcomes. The perpendicular plates (often a medial column plate and a posterior or posterolateral plate) create a strong construct, resisting forces in multiple planes.
Total elbow arthroplasty (TEA) (Option B) is an option for distal humerus fractures, particularly in elderly, low-demand patients with osteoporotic bone or in cases of nonunion/malunion, where ORIF is unlikely to succeed. However, for an 'active' 65-year-old with presumably reasonable bone quality, preserving the native joint via ORIF is generally preferred, as TEAs have limitations in activity level and longevity.
Excision arthroplasty (Option C) leads to a flail and unstable elbow with poor function and is typically reserved for salvage in very low-demand, non-reconstructible cases, or severe infection.
Non-operative management (Option D) is generally not indicated for comminuted intra-articular fractures in active adults, as it often leads to severe stiffness, pain, and malunion/nonunion.
ORIF with a single lateral plate (Option E) is insufficient for a 13-C3 fracture, which involves both columns. Adequate fixation requires addressing both medial and lateral columns, usually with dual plating.
Question 7
A 2-year-old girl is diagnosed with unilateral developmental dysplasia of the hip (DDH). Radiographs, seen here, show a dislocated left hip with an acetabular index of 45 degrees and evidence of femoral head flattening. Attempts at closed reduction under general anesthesia are unsuccessful.
What is the most appropriate next step in management?

Explanation
Option A (repeat closed reduction with higher force) is contraindicated. Forceful reduction attempts in late-presenting DDH significantly increase the risk of avascular necrosis (AVN) of the femoral head.
Option B (observation) is incorrect; an unreduced dislocated hip will lead to severe long-term disability and degenerative arthritis.
Option C (open reduction with capsulorrhaphy and possibly femoral shortening osteotomy) is the most appropriate next step. Open reduction addresses the soft tissue impediments to reduction and allows for direct visualization of the femoral head and acetabulum. Capsulorrhaphy stabilizes the hip after reduction. Femoral shortening osteotomy is often required in older children (typically >18-24 months) to reduce tension on the femoral head after reduction, thereby reducing the risk of AVN and facilitating a stable reduction. Addressing the acetabular dysplasia (e.g., with a Dega or Salter osteotomy) may also be necessary at the time of open reduction or as a staged procedure, depending on the residual dysplasia after reduction.
Option D (Pavlik harness) is effective for reducible DDH in infants younger than 6 months and is ineffective and contraindicated for irreducible or late-presenting DDH in a 2-year-old.
Option E (Triple innominate osteotomy) is an acetabular redirection osteotomy typically performed for residual acetabular dysplasia in older children (usually 6-12 years) after successful hip reduction, not as a primary treatment for an irreducible dislocation in a 2-year-old.
Question 8
A 40-year-old construction worker presents with chronic wrist pain and weakness following a fall onto an outstretched hand 6 months ago. Radiographs demonstrate a scapholunate gap of 4mm and a dorsal intercalated segment instability (DISI) deformity. MRI confirms complete scapholunate ligament rupture.
Given the chronic nature and significant instability, what is the most appropriate surgical intervention to stabilize the wrist and preserve function?

Explanation
Option A (Primary scapholunate ligament repair) is indicated for acute, reducible scapholunate dissociations (typically within 3 weeks of injury) before chronic changes develop.
Option B (Scaphotrapeziotrapezoid (STT) fusion) is a limited wrist fusion, which can be considered for chronic SL instability, but often leads to stiffness and may not be sufficient to address the DISI deformity, especially with a complete rupture.
Option C (Four-corner fusion) involves fusing the capitate, hamate, triquetrum, and lunate. While it stabilizes the lunate and triquetrum, it does not address the degenerated scaphoid directly. It is often performed with scaphoid excision to treat scapholunate advanced collapse (SLAC) wrist, a late consequence of chronic SL dissociation, to prevent further collapse and pain by removing the damaged scaphoid and fusing the remaining carpal bones.
Option D (Scaphoid excision and four-corner fusion) is considered the gold standard treatment for symptomatic chronic scapholunate dissociation with early degenerative changes (SLAC wrist stage I or II). The scaphoid, which has lost its stable connection to the lunate and is subject to abnormal forces, is excised to eliminate its impingement, and the remaining carpal bones (capitate, hamate, triquetrum, lunate) are fused to provide stability and pain relief while preserving a reasonable range of motion. This approach directly addresses both the instability and the degenerative changes caused by the abnormal kinematics.
Option E (Radial styloidectomy) might be part of an overall procedure in SLAC wrist to address impingement between the scaphoid and radial styloid, but it is not a standalone treatment for the primary instability.
Question 9
A 68-year-old female presents with severe axial back pain and difficulty standing upright, progressively worsening over several years. Standing lateral radiographs show a C7 plumb line falling 8 cm anterior to the sacral promontory, a pelvic incidence of 60 degrees, and a lumbar lordosis of -20 degrees. Pelvic tilt is 35 degrees. She has significant compensatory knee flexion and hip extension.
According to current spinal deformity principles, which surgical maneuver is most likely to restore her sagittal balance and improve her functional outcome?
Explanation
Option A (Posterior spinal fusion T10-L5 with in-situ contouring) is unlikely to provide enough correction for such severe sagittal imbalance, particularly with a C7PL of 8cm anterior.
Option B (Lumbosacral fusion L2-S1 with L4-S1 ALIF) can provide some lordosis, but an ALIF alone may not be sufficient for severe fixed sagittal plane deformities requiring more significant correction. Furthermore, extending only to L2 may not address the entire thoracolumbar kyphosis contributing to the imbalance.
Option C (Posterior spinal fusion with instrumentation from T10-S1 with iliac fixation and an L4 pedicle subtraction osteotomy (PSO)) is the most appropriate choice. A PSO is a powerful osteotomy that allows for significant lordosis correction (typically 30-40 degrees at a single level). An L4 PSO is often chosen for its effectiveness in correcting lumbar kyphosis. Fusing from T10 to S1 with iliac fixation ensures that the entire affected segment is addressed, and distal fixation is robust enough to support the long construct and powerful correction. This comprehensive approach is necessary to achieve global sagittal balance and prevent distal junctional kyphosis.
Option D (Multiple Smith-Petersen osteotomies (SPOs) from T10-L5) provide less correction per level (5-10 degrees) than a PSO and typically require several levels to achieve substantial lordosis. While possible, a PSO at one level often provides a more reliable and larger correction for severe fixed deformities. Fusing only to L5 also risks distal junctional problems given the severity.
Option E (Decompression and isolated fusion at L4-L5) would not address the global sagittal imbalance.
Question 10
A 60-year-old male with a history of metastatic renal cell carcinoma (RCC) presents with acute onset, intractable left hip pain and inability to bear weight. Radiographs and MRI reveal a large lytic lesion involving the subtrochanteric region of the left femur, with cortical destruction and an impending pathologic fracture. His Enneking score for pain is 3, stability is 2, and function is 2. He has otherwise stable systemic disease and a good prognosis.
What is the most appropriate surgical management for this patient?

Explanation
Option A (EBRT only) is insufficient. While radiation can help with pain control, it does not provide immediate mechanical stability for an impending fracture in a high-load-bearing area like the subtrochanteric femur. RCC is also known to be radioresistant.
Option B (Prophylactic intramedullary nailing of the femur) would provide stability for an impending fracture and is a common approach for diaphyseal or less comminuted subtrochanteric lesions. However, for a large lytic lesion with cortical destruction in the subtrochanteric region due to RCC (which is known for poor healing and being very lytic), nailing alone might not be sufficient to prevent hardware failure or provide adequate local control, especially if significant bone is destroyed. It also might not provide full pain relief if the tumor is actively destroying bone.
Option C (Curettage and cementation with prophylactic fixation) might be suitable for smaller, contained lesions or those in less mechanically demanding areas, but for a large, load-bearing lytic lesion in the subtrochanteric region from RCC, it might not offer sufficient long-term stability and local control.
Option D (Resection of the subtrochanteric lesion and reconstruction with a proximal femoral endoprosthesis) is the most appropriate option. Given the large lytic lesion, cortical destruction, and the aggressive nature of RCC metastases in bone, a wide resection of the involved bone offers the best local tumor control. Reconstruction with a proximal femoral endoprosthesis provides immediate, durable mechanical stability, allows for immediate weight-bearing, and significantly improves pain and function. This approach is particularly indicated for large, destructive lesions in critical load-bearing areas, especially from radioresistant tumors in patients with a good prognosis.
Option E (Open biopsy followed by observation) is incorrect. A biopsy is needed for definitive diagnosis if not already confirmed, but observation is not appropriate given the impending fracture and severe symptoms. Surgical stabilization is necessary.
Question 11
A 70-year-old male presents with persistent knee pain, swelling, and purulent drainage 6 months after a total knee arthroplasty (TKA). Aspiration yields turbid fluid with 80,000 WBCs/µL, 95% neutrophils, and positive cultures for Staphylococcus aureus. His C-reactive protein (CRP) is 120 mg/L (normal < 5 mg/L), and ESR is 100 mm/hr. He has no other comorbidities. What is the most appropriate surgical management strategy for this patient?
Explanation
Option A (Debridement, antibiotics, and implant retention - DAIR) is generally reserved for acute PJI (within 3-6 weeks of surgery or acute hematogenous spread on a well-fixed, stable implant), with healthy soft tissues and susceptible organisms. Given the 6-month duration and purulent drainage, the biofilm is well-established, making DAIR highly unlikely to succeed.
Option B (Two-stage revision arthroplasty) is considered the gold standard for chronic PJI, especially with virulent organisms, established biofilms, and significant soft tissue involvement or unknown organisms. The first stage involves complete removal of all prosthetic components, extensive debridement, and placement of an antibiotic-loaded cement spacer. After a period of intravenous antibiotics and normalization of inflammatory markers, the second stage involves spacer removal and reimplantation of a new TKA. This approach has the highest success rates for eradicating infection while preserving the possibility of a functional knee joint.
Option C (One-stage revision arthroplasty) may be considered in highly selected cases of chronic PJI with less virulent organisms, good soft tissue envelopes, and known susceptibility to antibiotics, but it carries a higher risk of recurrent infection compared to two-stage revisions, especially with Staphylococcus aureus.
Option D (Chronic antibiotic suppression) is typically reserved for patients who are not surgical candidates, who have low-virulence organisms, or who have failed other surgical attempts, and it does not eradicate the infection, only attempts to control it.
Option E (Arthrodesis of the knee) is a salvage procedure considered when all other attempts to eradicate infection and reconstruct the joint have failed, or in patients with very poor bone stock/soft tissues, resulting in a stiff, fused knee.
Question 12
A 45-year-old male sustains a high-energy pelvic injury in a motorcycle accident. Initial assessment shows hemodynamic stability after resuscitation. AP pelvis radiograph
reveals a widely displaced symphysis pubis and bilateral sacral fractures involving Zone II (Denis classification). A CT scan confirms posterior ligamentous injury and sacroiliac joint disruption. Which of the following fixation constructs is generally considered the most stable for this type of injury?

Explanation
Effective stabilization of unstable pelvic ring injuries requires addressing both the anterior and posterior disruptions.
Option A (Symphyseal plating alone) only addresses the anterior instability and leaves the posterior instability unaddressed, leading to continued pelvic instability.
Option B (Anterior external fixator with sacral iliosacral screws) is a good option. An anterior external fixator provides anterior stabilization, and iliosacral screws provide robust posterior fixation. This is a common and effective construct for this type of injury.
Option C (Symphyseal plating with bilateral sacroiliac (SI) screw fixation) is generally considered the most stable and definitive fixation construct for severe anterior and posterior pelvic ring instability. Symphyseal plating provides strong compression and stability across the pubic symphysis. Bilateral SI screw fixation provides excellent stability for sacral fractures and SI joint disruptions, which are critical for restoring posterior pelvic ring integrity. While external fixation (Option B) can be effective, internal plating and screw fixation are often biomechanically superior and preferred for definitive management in stable patients.
Option D (Posterior tension band plating of the sacrum) is a technique for certain types of sacral fractures, but it may not provide sufficient stability for bilateral sacral fractures with SI joint disruption, and it does not address the anterior injury.
Option E (Isolated anterior external fixator) only addresses the anterior injury and is insufficient for posterior instability, similar to option A.
Question 13
A 48-year-old male with end-stage post-traumatic ankle arthritis, severe subtalar arthritis, and a mild equinus contracture presents for surgical management. He is a non-smoker, has no diabetes, and desires to maintain some motion. Clinical examination reveals significant tibiotalar and subtalar stiffness with pain. Radiographs
confirm advanced arthritis in both joints. What is the most appropriate surgical recommendation?
Explanation
Option A (Isolated total ankle arthroplasty - TAA) would address the ankle arthritis but not the subtalar arthritis, which is also described as 'severe.' A TAA in the presence of severe subtalar arthritis can lead to persistent pain from the subtalar joint, and the altered biomechanics might accelerate subtalar degeneration.
Option B (Isolated ankle arthrodesis) would fuse the ankle but not the subtalar joint, again leaving a source of pain. Also, it contradicts the patient's desire to maintain motion.
Option C (Pantalar arthrodesis) involves fusing the tibiotalar, subtalar, talonavicular, and calcaneocuboid joints. While it provides a pain-free, stable foot, it results in a completely rigid foot, eliminating all ankle and foot motion. This is a salvage procedure typically reserved for pan-articular arthritis, severe deformity, or failed previous surgeries, and it goes against the patient's desire to maintain some motion.
Option D (Total ankle arthroplasty combined with subtalar arthrodesis) is the most appropriate recommendation. This approach allows for motion preservation at the tibiotalar joint via TAA while simultaneously addressing the painful, arthritic subtalar joint with an arthrodesis. The equinus contracture can also be addressed during the surgical procedure (e.g., gastrocnemius recession or Achilles lengthening), which is critical for successful TAA outcomes. This combined procedure allows for pain relief, corrects deformity, and maintains a degree of ankle motion, which aligns with the patient's goals and addresses the extent of his disease.
Option E (Distraction arthroplasty of the ankle) is a joint-sparing procedure used for early to moderate ankle arthritis, aiming to regenerate cartilage or reduce pain. It is generally not indicated for end-stage arthritis with severe destruction and existing subtalar disease.
Question 14
A 68-year-old male presents with chronic, severe right shoulder pain and pseudoparalysis (inability to actively elevate the arm), despite extensive physical therapy and injections. MRI reveals a massive, retracted, irreparable posterosuperior rotator cuff tear with significant fatty infiltration (Goutallier Stage 3-4) of the supraspinatus and infraspinatus. Glenohumeral arthritis is mild (Samilson-Prieto Grade 1).
Which of the following treatment options is most likely to provide functional improvement and pain relief for this patient?

Explanation
Option A (Arthroscopic debridement and partial repair) is unlikely to provide significant functional improvement or lasting pain relief in a massive, irreparable, chronically retracted tear with severe fatty infiltration. The tissue quality and retraction make healing improbable.
Option B (Superior capsular reconstruction - SCR) is a reconstructive option for massive, irreparable rotator cuff tears without significant arthritis, particularly in younger, high-demand patients, aiming to restore the superior stabilizing force and prevent superior migration. However, in an older patient (68 years) with pseudoparalysis, rTSA often provides more reliable and predictable functional improvement.
Option C (Latissimus dorsi transfer) is primarily indicated for irreparable posterosuperior rotator cuff tears with intact subscapularis and anterior deltoid function, and particularly for restoration of active external rotation and flexion/abduction. It may improve active elevation and external rotation, but rTSA often provides superior and more reliable functional gains for pseudoparalysis, especially in older patients.
Option D (Reverse total shoulder arthroplasty - rTSA) is the most appropriate treatment for this patient. The rTSA design medializes the center of rotation and increases the deltoid lever arm, allowing the deltoid to effectively elevate and abduct the arm, thereby compensating for the irreparable rotator cuff deficiency and addressing the pseudoparalysis. It reliably provides pain relief and functional improvement in this specific scenario, even with mild glenohumeral arthritis. The image provided shows superior migration and possible acromial erosion, which are common findings in rotator cuff arthropathy, reinforcing the choice of rTSA.
Option E (Infraspinatus repair only) is insufficient as it doesn't address the massive, irreparable nature of the tear affecting both supraspinatus and infraspinatus, or the pseudoparalysis.
Question 15
A 42-year-old active male presents with medial knee pain and a varus deformity. Standing full-length radiographs confirm genu varum with mechanical axis deviation of 10mm into the medial compartment. There is isolated medial compartment osteoarthritis. The surgeon plans a medial opening wedge high tibial osteotomy (HTO). During the planning, what is the primary radiographic parameter used to achieve optimal load transfer through the lateral compartment?

Explanation
Option A (Weight-bearing line passing through the lateral third of the tibial plateau) is the correct target. The weight-bearing line (or mechanical axis) connects the center of the femoral head to the center of the ankle. For HTO, the aim is to shift this line laterally. Passing it through the lateral third of the tibial plateau (typically 62-65% of the tibial width from medial) ensures sufficient unloading of the medial compartment and optimal load transfer through the healthier lateral compartment, maximizing the longevity of the osteotomy.
Option B (Restoration of the anatomical femorotibial angle to 175 degrees) refers to the anatomical axis, not the mechanical axis, and doesn't directly dictate load transfer.
Option C (Achieving a HKA (Hip-Knee-Ankle) angle of 183 degrees) describes a valgus alignment, but the specific target is more precisely defined by the weight-bearing line's position on the tibial plateau rather than a generic HKA angle. While 183 degrees indicates 3 degrees of mechanical valgus, the target zone for the weight-bearing line is more refined.
Option D (Correction of the medial proximal tibial angle (MPTA) to 90 degrees) is an angle used in planning but is not the primary measure for final load distribution. A specific MPTA is targeted to achieve the desired mechanical axis shift, but the ultimate goal is where the weight-bearing line falls.
Option E (Targeting an overcorrection to 5 degrees of valgus) is a general statement about valgus correction. While overcorrection into valgus is intended, the specific endpoint is defined by the weight-bearing line's position, not just a degree of valgus, and 5 degrees might be too much or too little for an individual patient, depending on their specific anatomy and desired load shift.
Question 16
A 38-year-old male presents with a persistent painful tibial shaft nonunion 12 months after initial intramedullary nailing for a comminuted fracture. Radiographs
show sclerotic bone ends and no bridging callus. Infection workup (ESR, CRP, aspiration) is negative. He is a non-smoker. He has previously undergone nail exchange without success. What is the most appropriate next step in management for this refractory nonunion?

Explanation
Option B (Plate fixation with bone grafting) is a viable option for a nonunion, offering strong fixation and facilitating bone grafting. However, for a refractory nonunion that has failed IM nailing twice, particularly a comminuted fracture, the challenge may be significant bone defect or persistent poor biology. Plate fixation can be associated with higher rates of infection in the tibia compared to nailing.
Option C (External fixator with bone transport - Ilizarov technique) is often considered a highly effective method for refractory tibial nonunions, especially those with significant bone loss, deformity, or persistent poor biology that has failed other treatments. The Ilizarov method provides excellent stability, allows for gradual correction of deformity, compression at the nonunion site, and stimulates bone regeneration (distraction osteogenesis) to fill bone gaps and promote healing. This technique is particularly well-suited for cases where the bone ends are sclerotic and revascularization is a challenge, as it brings new, viable bone to the nonunion site. Given the failure of two IM nailing attempts, a more biologically potent and mechanically adaptable approach like the Ilizarov method is warranted.
Option D (Pulsed electromagnetic field (PEMF) stimulation) is a non-invasive adjunct therapy that can be used for nonunions, but it is typically used in conjunction with stable fixation or as a standalone treatment for early, less refractory nonunions. It is unlikely to be successful as a primary treatment for a complex nonunion that has failed two surgical interventions.
Option E (Amputation) is a salvage procedure for limb-threatening conditions or failed multiple reconstructions and is not indicated as the next step for a refractory nonunion that still has limb salvage potential.
Question 17
A 25-year-old athlete sustained a valgus and external rotation injury to his knee. Clinical examination reveals medial joint line tenderness, grade III valgus instability at 0 and 30 degrees, and increased external rotation of the tibia relative to the femur at 30 degrees of flexion (positive Dial test). MRI confirms a complete rupture of the superficial medial collateral ligament (sMCL), posterior oblique ligament (POL), and posteromedial capsule. The ACL and PCL are intact. What is the most critical biomechanical function of the POL in this injury pattern?
Explanation
Let's analyze the options:
Option A (Primary restraint to valgus stress at 30 degrees of flexion): The sMCL is the primary restraint to valgus stress at 30 degrees of flexion, while the deep MCL and POL act as secondary restraints. The POL primarily stabilizes against external rotation, not purely valgus stress.
Option B (Secondary restraint to anterior tibial translation): The POL can act as a minor secondary restraint to anterior tibial translation, but this is not its primary or most critical function in this injury pattern where external rotation instability is evident.
Option C (Primary restraint to posterior tibial translation): The PCL is the primary restraint to posterior tibial translation. The POL has a very minor role here.
Option D (Primary restraint to external rotation of the tibia at 30 degrees of flexion): This is the most critical biomechanical function of the POL. The POL, along with the deep MCL and posterior capsule, is a key component of the posteromedial corner (PMC) and plays a crucial role in resisting external rotation of the tibia, especially in 30 degrees of flexion. A complete rupture of the POL, as described, significantly contributes to the increased external rotation instability (positive Dial test) and often indicates a more severe medial injury than sMCL rupture alone. Given the clinical findings (increased external rotation), this function is paramount.
Option E (Primary restraint to internal rotation of the tibia): The POL does not primarily restrain internal rotation; other structures like the PCL and lateral collateral ligament are more involved.
Question 18
A 30-year-old male sustains a high-energy fall onto an outstretched hand, resulting in a perilunate dislocation. Post-reduction radiographs show an anatomical reduction of the lunate with respect to the radius, but the capitate remains dorsally displaced relative to the lunate.
What is the most accurate term for this specific post-reduction radiographic appearance, indicating persistent instability?

Explanation
Option A (Scapholunate dissociation) involves disruption of the scapholunate ligament, leading to a gap between the scaphoid and lunate and often a DISI deformity. While a perilunate injury often involves scapholunate ligament disruption, the specific finding described post-reduction is capitate-lunate incongruity.
Option B (Lunate dislocation) refers to the lunate itself being dislocated (typically volar) from both the radius and the capitate, forming a 'spilled teacup' sign on a lateral X-ray. The question states the lunate is reduced relative to the radius.
Option C (Capitolunate dissociation) precisely describes the condition where the capitate and lunate are no longer articulating correctly, despite the lunate being reduced to the radius. This implies persistent instability in the midcarpal joint.
Option D (Proximal carpal row instability) is a broad term that encompasses various instabilities within the proximal carpal row (e.g., scapholunate, lunotriquetral dissociation). While the described injury is a form of carpal instability, 'capitolunate dissociation' is more specific to the post-reduction radiographic finding.
Option E (Midcarpal instability) is also a broad term referring to instability between the proximal and distal carpal rows. Capitolunate dissociation is a specific manifestation of persistent midcarpal instability following a perilunate injury. However, 'capitolunate dissociation' is the most accurate and descriptive term for the specific radiographic finding of the capitate remaining displaced relative to the lunate after reduction of the lunate-radial articulation.
Question 19
A 75-year-old male with a known history of Paget's disease of bone involving the left femur presents with new onset severe pain in the affected thigh, refractory to NSAIDs and bisphosphonates. Radiographs show progressive cortical thickening and bowing of the femur, with a new, subtle transverse lucency in the lateral cortex. What is the most appropriate next diagnostic step?
Explanation
Option A (CT scan) can provide more detailed bony architecture but may not be as sensitive for early stress fractures or soft tissue changes.
Option B (Bone scintigraphy) would show increased uptake in the pagetic bone (hot spots), but it's a very sensitive but non-specific test. It might light up more intensely at the site of increased metabolic activity due to a stress fracture, but it wouldn't characterize the fracture line or any surrounding soft tissue injury as well as an MRI.
Option C (MRI of the femur) is the most appropriate next diagnostic step. MRI is highly sensitive for detecting stress fractures, subtle lucencies, and incomplete fractures that may be missed or poorly characterized on plain radiographs or CT. It can also differentiate between different causes of pain (e.g., stress fracture, malignant transformation to sarcoma, inflammatory changes, or simply exacerbation of Paget's activity) and assess soft tissue involvement. Confirming an incomplete fracture or impending fracture is crucial for guiding management, often leading to prophylactic fixation.
Option D (Measurement of serum alkaline phosphatase levels) is useful for monitoring disease activity in Paget's disease and response to bisphosphonates. However, it's a biochemical marker of bone turnover and will not directly diagnose or characterize a fracture. While a flare-up of Paget's could cause pain and elevate ALP, a new focal lucency points to a mechanical issue.
Option E (Biopsy of the lesion) would be indicated if there was suspicion of malignant transformation (e.g., osteosarcoma, which is a known but rare complication of Paget's disease). While a new, severe pain can sometimes raise this concern, a 'subtle transverse lucency' is more characteristic of an incomplete fracture. MRI would be the first step to better characterize the lesion before considering an invasive biopsy.
Question 20
A 28-year-old male involved in a high-speed motor vehicle collision presents with multiple injuries: a grade III open tibia fracture, a closed femoral shaft fracture, a displaced intra-articular calcaneus fracture, and severe blunt abdominal trauma with ongoing hemodynamic instability requiring massive transfusion. His initial GCS is 10, and his base deficit is -8. After initial resuscitation, what is the most appropriate early orthopedic management strategy?
Explanation
Option A (Immediate definitive fixation of all fractures) is inappropriate and potentially dangerous. This 'early total care' approach would subject a physiologically unstable patient to prolonged surgery, increasing the risk of the 'second hit' phenomenon, worsening systemic inflammation, and potentially leading to multiple organ failure or death. It is contraindicated in this scenario.
Option B (Damage control orthopedics (DCO) with external fixation of the tibia and femur, and temporizing calcaneal management) is the most appropriate strategy. DCO involves quick, temporary stabilization of long bone and pelvic fractures, typically with external fixators, to control hemorrhage, pain, and prevent further tissue damage. This allows the surgical team to address life-threatening injuries (like abdominal trauma) and stabilize the patient's physiology. Definitive fixation is then performed in a delayed fashion once the patient is physiologically stable. The open tibia fracture needs irrigation and debridement, and an external fixator would provide temporary stabilization. The calcaneal fracture, being intra-articular, is not emergent and can be managed with temporizing measures (e.g., splinting) until the patient's condition stabilizes.
Option C (Amputation) is a salvage procedure and is not indicated as the initial management unless the limb is unsalvageable or poses an immediate threat to life that cannot be managed by other means.
Option D (Skeletal traction) is a temporizing measure for long bone fractures but is less stable than external fixation and may not adequately control pain or allow for easy patient mobilization in a polytrauma setting, especially for an open fracture. It also doesn't address the need for surgical debridement of the open fracture.
Option E (Extensive débridement of the open tibia fracture, followed by definitive fixation of the tibia, and observation of other fractures) is problematic. While debridement of the open fracture is crucial, definitive fixation of the tibia in a hemodynamically unstable patient can still be a 'second hit.' The definitive fixation should be delayed, and other fractures should also be temporized, not just observed.
Question 21
A 65-year-old female presents with progressive back pain and increasing truncal imbalance. Her sagittal balance parameters show a Sagittal Vertical Axis (SVA) of +10 cm, Pelvic Incidence (PI) of 60 degrees, Lumbar Lordosis (LL) of -30 degrees, and Pelvic Tilt (PT) of 35 degrees. She has failed extensive conservative management.
Based on these radiographic parameters, what is the most appropriate surgical goal to restore optimal sagittal alignment?
Explanation
Question 22
A 45-year-old male sustains a high-energy trauma, resulting in an unstable pelvic ring injury classified as a Young-Burgess Type II APC (Anteroposterior Compression). Neurological examination reveals a partial L5-S1 radiculopathy on the affected side. After initial resuscitation, what is the MOST critical next step in management PRIOR to definitive surgical stabilization?
Explanation
Question 23
A 28-year-old professional athlete suffers a multi-ligamentous knee injury following a valgus contact force during a tackle. MRI confirms complete tears of the ACL, MCL (grade III), and posterior oblique ligament (POL). There is no common peroneal nerve palsy.
What is the optimal timing and surgical strategy for this injury pattern?

Explanation
Question 24
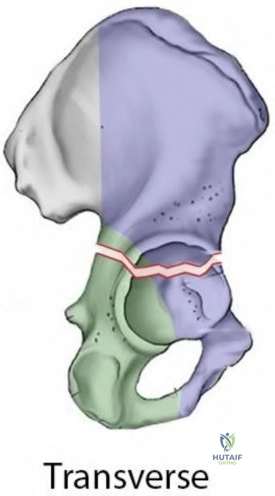
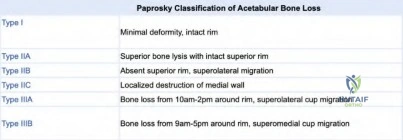
A 72-year-old male with a history of a cemented total hip arthroplasty (THA) 15 years ago presents with persistent groin pain and aseptic loosening of the acetabular component. Radiographs show significant acetabular osteolysis and a Paprosky Type IIIB defect.
Which of the following is the MOST appropriate reconstructive option for this acetabular defect?

Explanation
Question 25
A 13-year-old obese male presents with a 3-month history of right hip and knee pain, worsening with activity. Physical examination reveals a painful gait, decreased internal rotation, and external rotation with hip flexion (Drehmann sign). Radiographs show a right slipped capital femoral epiphysis (SCFE) with a moderate slip angle.
What is the MOST appropriate acute management for this patient?

Explanation
Question 26
A 35-year-old painter presents with chronic ulnar-sided wrist pain, particularly with gripping and rotational movements. Physical examination reveals tenderness over the triquetrum and lunate, a positive ulnar snuffbox test, and painful clicking. Radiographs, including specialized views, show widening of the scapholunate interval and a Terry Thomas sign.
What is the MOST likely diagnosis and initial management strategy?

Explanation
Question 27
A 58-year-old diabetic male with peripheral neuropathy presents with a rapidly progressing, painful, and deformed right foot. Physical examination reveals a warm, swollen, erythematous foot with a rocker-bottom deformity and collapse of the midfoot arch. Radiographs show fragmentation and dislocation of the tarsometatarsal joints, with evidence of osteolysis and new bone formation.
What is the primary goal of acute treatment for this condition?
Explanation
Question 28
A 24-year-old female presents with recurrent pain and swelling around her left knee. MRI reveals an expansile, lytic lesion in the distal femur, extending to the subchondral bone, with sclerotic margins. Biopsy confirms giant cell tumor of bone.
Which of the following adjuvant treatments is most effective in reducing local recurrence rates following intralesional curettage for this tumor?

Explanation
Question 29
Regarding bone graft substitutes, which of the following statements accurately describes the primary characteristic of an osteoinductive material?
Explanation
Question 30
A 68-year-old male undergoes a single-stage revision total knee arthroplasty (TKA) for a chronic prosthetic joint infection (PJI) caused by methicillin-resistant Staphylococcus aureus (MRSA). During the revision surgery, thorough debridement, implant removal, and placement of new implants with antibiotic-loaded cement are performed. What is the MOST crucial aspect of his postoperative antibiotic regimen?
Explanation
Question 31
A 70-year-old female presents with chronic pain and weakness in her right shoulder. She has a massive, irreparable rotator cuff tear involving the supraspinatus, infraspinatus, and subscapularis, with significant superior migration of the humeral head and glenohumeral arthritis (Hamada Type IV). Her functional goals include regaining ability to perform activities of daily living.
What is the most appropriate surgical intervention?

Explanation
Question 32
A 40-year-old male sustains a severe fall onto his outstretched hand, resulting in an elbow fracture-dislocation. Radiographs and CT scans reveal a posteromedial coronoid fracture (Regan & Morrey Type III), a radial head fracture (Mason Type III), and disruption of the lateral ulnar collateral ligament (LUCL).
This constellation of injuries is best described as what type of elbow instability?

Explanation
Question 33
A 55-year-old female presents with widespread musculoskeletal pain, muscle weakness, and proximal leg cramps. She has a history of bariatric surgery 5 years prior. Biochemical tests reveal low serum calcium, low serum phosphate, elevated alkaline phosphatase, and elevated parathyroid hormone. Radiographs show Looser zones (pseudofractures) in the femoral neck and pubic rami. Which of the following is the MOST likely underlying diagnosis?
Explanation
Question 34
A 2-year-old child is diagnosed with progressive early-onset scoliosis (EOS) with a main thoracic curve measuring 45 degrees, unresponsive to bracing. The child has significant truncal imbalance and documented respiratory compromise. What is the MOST appropriate surgical management strategy for this patient?
Explanation
Question 35
A 60-year-old male with a history of metastatic prostate cancer presents with sudden onset back pain and bilateral lower extremity weakness. MRI reveals a pathologic fracture of L4 with significant epidural compression of the cauda equina. He has Grade 3/5 motor strength in both legs. What is the MOST urgent surgical intervention indicated?
Explanation
Question 36
A 38-year-old runner presents with deep buttock pain radiating down the posterior thigh, exacerbated by prolonged sitting and running. Physical examination reveals tenderness over the piriformis muscle, pain with passive internal rotation of the hip in flexion, and normal straight leg raise. Electromyography (EMG) and nerve conduction studies (NCS) are unremarkable. What is the MOST likely diagnosis?
Explanation
Question 37
A 25-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture with significant soft tissue loss and exposed bone, after a motorcycle accident. He has no neurovascular compromise and no signs of systemic infection. After initial débridement, irrigation, and temporary external fixation, what is the MOST appropriate next step in surgical management for limb salvage?
Explanation
Question 38
A 32-year-old female presents with chronic anterior ankle pain, exacerbated by dorsiflexion, and occasional catching. Radiographs are normal, but an MRI reveals a small osteochondral defect (OCD) on the talar dome, and synovial hypertrophy suggestive of anterior impingement. Which arthroscopic procedure is MOST appropriate as the initial surgical intervention?
Explanation
Question 39
A 28-year-old female presents with persistent deep hip pain, particularly with flexion and internal rotation. MRI reveals a cam-type femoroacetabular impingement (FAI) and a labral tear. She has failed conservative management. What is the primary biomechanical goal of surgical intervention for this condition?
Explanation
Question 40
A 50-year-old female presents with burning pain, numbness, and tingling in the third and fourth toes of her left foot, worsened by wearing tight shoes and prolonged standing. Physical examination reveals tenderness in the third intermetatarsal space with a positive Mulder's sign. Radiographs are unremarkable. What is the MOST appropriate initial non-surgical management?
Explanation
Question 41
A 75-year-old female with a history of osteoporosis on long-term bisphosphonate therapy presents with sudden onset of severe right thigh pain after a low-energy fall. Radiographs reveal a transverse fracture of the subtrochanteric region of the right femur with medial cortical thickening ('beaking').
What is the most appropriate definitive surgical management for this fracture?

Explanation
Question 42
A 6-year-old child presents with a Limberg flap-like skin lesion on the anterior aspect of the lower leg following a severe open tibia fracture. The lesion is firm, hyperpigmented, and shows no signs of active infection. Biopsy reveals mature bone tissue within the soft tissues. What is the MOST likely diagnosis?
Explanation
Question 43
In evaluating a patient for chronic lower back pain with suspected facet joint arthropathy, which of the following imaging modalities is considered the 'gold standard' for diagnosing facet pain before considering invasive treatments?
Explanation
Question 44
A 45-year-old male with a history of recurrent ankle sprains develops chronic lateral ankle instability. Clinical examination reveals a positive anterior drawer test and talar tilt test. Imaging shows chronic attenuation of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL). He fails a trial of bracing and physical therapy. What is the MOST appropriate surgical procedure for definitive stabilization?
Explanation
Question 45
A 68-year-old male with a history of L3-S1 instrumented fusion presents with increasing back pain, progressive stooping posture, and difficulty ambulating. Clinical examination reveals a positive sagittal imbalance. A standing lateral spinopelvic radiograph is shown below.
Which radiographic parameter is MOST strongly correlated with functional outcome and satisfaction following surgical correction of adult spinal deformity with sagittal imbalance?

Explanation
Question 46
A 22-year-old female presents with chronic right hip pain and a diagnosis of symptomatic hip dysplasia. An AP pelvis radiograph is shown.
She is scheduled for a Bernese periacetabular osteotomy (PAO). Which intraoperative maneuver is CRITICAL for optimizing hip joint coverage and load distribution while minimizing impingement?
Explanation
Question 47
A 30-year-old football player sustains a high-energy knee injury resulting in a Schenck KD-III-M knee dislocation. Clinical examination reveals gross laxity to varus and valgus stress at 0 and 30 degrees of flexion, with a positive posterior drawer test. Popliteal pulses are palpable, but a common peroneal nerve palsy is present. An MRI of the knee is shown.
What is the MOST appropriate initial management strategy for this patient?
Explanation
Question 48
A 55-year-old male presents with persistent right thigh pain and swelling. An MRI reveals a large, ill-defined lesion in the distal femur suggestive of a high-grade sarcoma. Surgical planning is underway for a diagnostic biopsy. Which of the following principles regarding biopsy technique is MOST critical to ensure the success of a subsequent limb salvage procedure?
Explanation
Question 49
A 58-year-old male with a 20-year history of Type 2 Diabetes Mellitus presents with sudden onset of warmth, redness, and swelling in his left midfoot, without a clear history of trauma. He reports mild discomfort but no severe pain. Radiographs are obtained and are shown below.
The imaging shows early fragmentation and joint disorganization of the tarsometatarsal joints, consistent with Eichenholtz Stage I Charcot neuroarthropathy. What is the MOST critical initial management step?

Explanation
Question 50
A 72-year-old female with irreparable rotator cuff arthropathy undergoes a reverse total shoulder arthroplasty. Postoperatively, she develops progressive pain and decreased range of motion, and radiographs reveal significant scapular notching.
Which of the following design or surgical implantation strategies is MOST effective in reducing the incidence of scapular notching in reverse total shoulder arthroplasty?
Explanation
Question 51
A 28-year-old male falls from a ladder onto an outstretched hand, sustaining a high-energy wrist injury. Physical examination reveals a swollen, deformed wrist with significant pain and limited range of motion. Lateral radiographs of the wrist are obtained and show the following.
The radiographs confirm a dorsal perilunate dislocation. What is the MOST appropriate initial closed reduction maneuver for this injury?
Explanation
Question 52
An 11-year-old obese male presents with a 3-month history of left knee pain, which he attributes to 'growing pains.' He denies any specific trauma. On examination, he has an antalgic gait, and active range of motion of the left hip reveals significantly limited internal rotation and abduction. Radiographs of the hips (AP and frog-leg lateral views, as shown) are ordered.
The images show a stable Slipped Capital Femoral Epiphysis (SCFE) on the left. What is the MOST appropriate definitive treatment for this condition?

Explanation
Question 53
A 45-year-old patient is brought to the emergency department after a high-speed motor vehicle collision. He is hypotensive (BP 80/50 mmHg) and tachycardic (HR 125 bpm). Physical examination reveals a swollen and unstable pelvis. A bedside AP pelvis radiograph is obtained and is shown below.
The radiograph shows a significantly displaced open-book pelvic injury with widening of the pubic symphysis and disruption of the posterior sacroiliac ligaments. After initial ATLS resuscitation, what is the MOST immediate and critical orthopedic intervention to manage ongoing hemorrhage?

Explanation
Question 54
When considering various bone graft options for a critical-sized bone defect, understanding their biological properties is essential. Which of the following characteristics is uniquely provided by autogenous cancellous bone graft, making it superior to all other bone graft substitutes in terms of intrinsic biological activity?
Explanation
Question 55
A 35-year-old male sustains a fall onto an outstretched hand, resulting in a complex elbow injury. Clinical examination reveals gross instability. Radiographs confirm an elbow dislocation, a comminuted radial head fracture, and a coronoid process fracture.
This injury pattern is commonly referred to as the 'terrible triad' of the elbow. Which component of the terrible triad is MOST critical to reconstruct or repair to restore the primary anterior-posterior stability of the elbow joint?

Explanation
Question 56
A 65-year-old patient presents with a painful total knee arthroplasty (TKA) 2 years post-surgery. Inflammatory markers show ESR of 55 mm/hr and CRP of 45 mg/L. Joint aspiration yields purulent fluid. What is the MOST definitive diagnostic criterion for periprosthetic joint infection (PJI) according to the Musculoskeletal Infection Society (MSIS) 2018 criteria?
Explanation
Question 57
A 16-year-old female high school soccer player requires anterior cruciate ligament (ACL) reconstruction. After discussing various autograft options, the patient and her parents express concern about potential anterior knee pain and donor site morbidity, wishing to minimize these while maintaining robust graft strength. Which autograft choice is generally associated with the LOWEST incidence of anterior knee pain and excellent functional outcomes in young athletes?
Explanation
Question 58
A 40-year-old female presents with a 6-month history of chronic, dull ache in her right buttock, with occasional radiation to the posterior thigh, but not below the knee. The pain is exacerbated by prolonged standing, sitting, or weight-bearing on the affected side. Physical examination reveals tenderness over the right sacroiliac joint and positive distraction, compression, and FABER tests. Lumbar MRI is unremarkable. What is the MOST appropriate next step in confirming the diagnosis and guiding treatment for suspected sacroiliac joint dysfunction?
Explanation
Question 59
A 32-year-old construction worker presents with chronic radial-sided wrist pain, reduced grip strength, and limited range of motion following a fall 18 months prior. Radiographs show a scaphoid waist nonunion with dorsal intercalated segment instability (DISI) deformity and early degenerative changes in the radial scaphoid articulation. He previously underwent screw fixation with a non-vascularized bone graft, which failed to achieve union. What is the MOST appropriate surgical treatment for this symptomatic scaphoid nonunion with failed previous grafting and early arthrosis?
Explanation
Question 60
A pediatrician refers a 3-week-old infant due to a rigid 'rocker-bottom' deformity of the left foot. Physical examination reveals a dorsiflexed ankle, a prominent talar head on the plantar aspect, and a non-reducible midfoot and forefoot abduction. Lateral radiographs confirm congenital vertical talus (CVT) with dorsal dislocation of the navicular on the talar head. What is the MOST accepted initial primary treatment approach for congenital vertical talus?
Explanation
Question 61
A 35-year-old male sustains a high-energy motor vehicle accident resulting in an open tibia shaft fracture with extensive soft tissue loss and periosteal stripping (Gustilo-Anderson Type IIIB). Initial debridement and external fixation were performed 4 hours post-injury, and broad-spectrum antibiotics were initiated. The wound bed is clean but presents a large soft tissue defect. What is the optimal timing for definitive soft tissue coverage (e.g., free flap or rotational flap) in this Gustilo-Anderson Type IIIB open fracture?
Explanation
Question 62
A 14-year-old male presents with right distal femur pain. Imaging reveals a large, aggressive lesion. Biopsy confirms high-grade osteosarcoma. A full metastatic workup, including chest CT and bone scan, shows no evidence of distant disease. The tumor is intra-compartmental. According to the Enneking surgical staging system for malignant musculoskeletal tumors, what is the correct stage for this patient's tumor?
Explanation
In this scenario:
- High-grade osteosarcoma = G2
- Intra-compartmental = T1
- No distant metastasis = M0
Therefore, the tumor is classified as Stage IIA. Stage IIB would be a high-grade, extra-compartmental tumor without metastasis (G2T2M0).
Question 63
A 17-year-old female presents with a 1-year history of recurrent patellar dislocations after initial non-operative treatment failed. Physical examination reveals hyperlaxity and apprehension with lateral patellar translation. MRI of the knee (axial view shown) confirms severe trochlear dysplasia, patella alta, and a Tibial Tubercle-Trochlear Groove (TT-TG) distance of 18 mm.
Considering the comprehensive patellofemoral pathology, which combination of surgical procedures would BEST address the primary biomechanical deficiencies and reduce the risk of future dislocations?

Explanation
Question 64
In the context of promoting bone healing, various orthobiologic agents are utilized. These agents exert their effects through different mechanisms. Which of the following orthobiologics primarily acts by providing a demineralized osteoconductive scaffold rich in growth factors to stimulate local mesenchymal stem cells, rather than directly supplying viable osteoprogenitor cells?
Explanation
Question 65
A 68-year-old male presents with worsening back pain and progressive difficulty maintaining an upright posture. Clinical examination reveals a positive sagittal imbalance. Lateral standing radiographs are obtained, revealing the following spinal alignment parameters:
Pelvic incidence (PI) = 60°, Pelvic tilt (PT) = 30°, Sacral slope (SS) = 30°, Sagittal vertical axis (SVA) = +10 cm. Based on these findings, which of the following statements regarding his sagittal alignment is MOST accurate?
Explanation
Rationale for options:
A. His PI (60°) is within the high-normal range, not abnormally low.
B. An increased PT (30°) is a classic compensatory mechanism for positive sagittal balance, attempting to shift the center of gravity posteriorly. This is the correct statement.
C. A decreased sacral slope (30°) is indicative of pelvic retroversion, which is a sign of decompensated or compensating sagittal alignment, not a well-compensated one. A large sacral slope typically indicates a more upright pelvis and better compensation, if paired with appropriate lumbar lordosis.
D. SVA of +10 cm is significantly positive (normal is generally < 5 cm), indicating a significant sagittal imbalance, not normal limits.
E. Surgical correction typically aims to decrease pelvic tilt and increase sacral slope to improve global sagittal alignment, but the statement 'decrease pelvic tilt and increase sacral slope' is part of the correction strategy, whereas the initial question asks for the most accurate statement regarding his current alignment. The current PT indicates compensation.
Question 66
A 72-year-old female presents to the emergency department after a low-energy fall, complaining of severe right hip pain. She has a history of total hip arthroplasty (THA) performed 15 years prior. Radiographs reveal a periprosthetic femoral fracture involving the proximal femur around a well-fixed femoral stem, with a stable cement mantle, as shown in the image below. The fracture extends distal to the lesser trochanter but above the distal tip of the femoral component. There is no evidence of implant loosening.
According to the Vancouver Classification, which type of fracture does this MOST likely represent, and what is the generally recommended treatment?
Explanation
• Type A: Fractures involving the trochanteric region.
• Type B: Fractures around or just distal to the femoral stem.
• B1: Stable femoral component.
• B2: Loose femoral component.
• B3: Loose femoral component with poor femoral bone stock.
• Type C: Fractures well distal to the femoral stem.
Given the description of a 'well-fixed femoral stem' and a fracture around it, Vancouver B1 is the correct classification. The recommended treatment for Vancouver B1 fractures is open reduction and internal fixation (ORIF) with cerclage wires and plating to achieve stable fixation while preserving the well-fixed stem.
Rationale for options:
A. Type A involves the trochanters, which is not described. ORIF with tension band wiring is for trochanteric fractures, but not typically for periprosthetic fractures involving the stem.
B. Type B1 describes a stable femoral component with a fracture around it. ORIF with cerclage wires and plating is the standard treatment to stabilize the fracture while retaining the well-fixed prosthesis. This is the correct answer.
C. Type B2 involves a loose femoral component. Treatment for B2 fractures requires revision of the stem to a longer, often calcar-replacing or extensively coated, femoral stem to bypass the fracture.
D. Type B3 involves a loose femoral component with poor bone stock. This often necessitates extensive femoral reconstruction using massive allografts or highly specialized modular revision stems.
E. Type C fractures are well distal to the prosthesis, not around it. Treatment is typically ORIF with plating, bypassing the entire prosthesis.
Question 67
A 35-year-old male sustains a high-energy injury to his right ankle after falling from a significant height. Clinical examination reveals severe swelling and deformity, with palpable crepitus. Radiographs, shown below, demonstrate a comminuted fracture of the distal tibia articular surface with metaphyseal extension, but no significant fibular fracture. There is also disruption of the tibiofibular syndesmosis.
What is the most appropriate initial management strategy for this type of injury, specifically considering the soft tissue condition?

Explanation
The standard initial management for these high-energy pilon fractures is to stabilize the injury and protect the soft tissues. This typically involves emergent reduction (to minimize tension on skin) and application of a spanning external fixator from the tibia to the foot or calcaneus. This provides temporary stability, allows for soft tissue rest, reduces swelling, and facilitates serial wound checks. Definitive ORIF is then delayed until the 'wrinkle sign' appears, indicating resolution of significant soft tissue swelling, which often takes 7-14 days.
Rationale for options:
A. Immediate ORIF is contraindicated due to severe soft tissue swelling and high risk of complications.
B. Emergent reduction and application of a spanning external fixator, followed by serial examinations and delayed definitive fixation (typically after 7-14 days), is the cornerstone of management for high-energy pilon fractures with significant soft tissue injury. This is the correct answer.
C. While emergent reduction and splinting is a good initial step, a spanning external fixator provides superior stability and soft tissue protection for these severe fractures, making it more appropriate than just splinting.
D. Closed reduction and casting is generally insufficient for comminuted articular fractures and syndesmotic disruption, leading to poor anatomical reduction and high rates of post-traumatic arthritis.
E. Ankle arthrodesis is a salvage procedure considered for severe, unreconstructable articular comminution or failed prior attempts, not as the primary initial management for a reconstructable fracture.
Question 68
A 9-month-old female is diagnosed with a unilateral left developmental dysplasia of the hip (DDH) that failed Pavlik harness treatment despite good compliance. Clinical examination reveals a reducible but unstable hip. An anteroposterior pelvic radiograph confirms a dislocated hip with a severely dysplastic acetabulum and a high riding femoral head.
Given the age and failed conservative management, what is the MOST appropriate next step in management?

Explanation
At 9 months, the hip is typically still reducible, and soft tissue contractures are not as severe as in older children. A closed reduction aims to relocate the femoral head into the acetabulum, followed by immobilization in a hip spica cast, usually in the 'human' position (hip flexion 90-100°, abduction 45-60°, slight internal rotation). Arthrography is often performed during the procedure to confirm concentric reduction and identify any impediments to reduction.
Rationale for options:
A. Pavlik harness is typically ineffective and contraindicated after 6-9 months of age or after failure, due to increased stiffness and potential for avascular necrosis (AVN) with excessive force.
B. Closed reduction under general anesthesia with subsequent hip spica casting is the standard next step for failed Pavlik harness in an infant of this age with a reducible hip. This is the correct answer.
C. A triple innominate osteotomy is an acetabular redirection osteotomy performed in older children (typically > 18-24 months) or adolescents for residual dysplasia after successful reduction, not as the primary reduction method in an infant.
D. Open reduction and femoral shortening osteotomy is indicated for irreducible hips, severe dislocations, or older children (typically >12-18 months) where significant soft tissue contractures or bony deformities prevent closed reduction. At 9 months, closed reduction is usually attempted first unless there's clear evidence of irreducibility.
E. Traction may be used as a preparatory step for open or closed reduction in older infants (e.g., >12 months) to stretch soft tissues, but it is not followed by another Pavlik harness application after failed initial treatment.
Question 69
A 28-year-old professional athlete suffers a high-energy knee injury during a football game. Clinical examination reveals gross instability in multiple planes, a positive Lachman test, positive posterior sag sign, and a positive varus stress test at 30 degrees of flexion. MRI confirms complete tears of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and lateral collateral ligament (LCL), with associated posterolateral corner (PLC) injury.
What is the most critical principle guiding the surgical management of this acute multiligamentous knee injury?

Explanation
The posterolateral corner (PLC) is a crucial stabilizer. Unaddressed PLC injury can lead to failure of cruciate ligament grafts. Therefore, the PLC is often addressed first during reconstruction, or simultaneously with the other ligaments, to provide a stable foundation. Delaying surgery allows for significant scarring and increased difficulty in surgical repair/reconstruction, and may not lead to significant healing for completely torn ligaments.
Rationale for options:
A. Prioritizing only the ACL and staging others is generally not recommended for multiligament injuries, as the remaining instability will compromise graft integrity and overall knee function.
B. Delaying surgery for 6-12 weeks for all tears is often not ideal. While some isolated collateral ligament injuries can be managed non-operatively, complete multiligament injuries benefit from early definitive surgical intervention to minimize scarring, improve outcomes, and facilitate rehabilitation. However, a 'staged' approach is sometimes used if soft tissues are severely compromised, or if the patient presents late. For acute injuries, a single stage is often preferred if possible.
C. While many surgeons prefer to address all structures in a single stage, a staged approach for multiligament injuries is sometimes employed, especially for severe cases or if significant swelling/blistering is present. However, the principle of restoring stability is paramount. In acute repairs, the PLC structures are often addressed first or concurrently as their integrity is vital for success of cruciate reconstruction. This option specifically mentions addressing PLC before cruciate ligaments, which is a common practice in staged approaches, especially if there's severe soft tissue injury or the patient is not suitable for a single, lengthy procedure. Given the options, and the emphasis on PLC's importance, this points to a critical sequencing consideration.
D. Reconstructing all torn ligaments in a single stage is the current trend for acute multiligament injuries in athletes to restore overall knee stability. This is generally preferred when feasible. However, option C highlights the importance of the PLC.
E. This statement is incorrect. The ACL plays a significant role in knee stability, especially rotational stability, and its absence in a multiligamentous injury would lead to continued instability and poor long-term outcomes.
Question 70
A 40-year-old manual laborer presents with chronic right wrist pain, particularly with grip and heavy lifting, for the past 2 years. He reports a remote history of a fall on an outstretched hand. Clinical examination reveals localized tenderness over the anatomical snuffbox and painful wrist extension. Radiographs are obtained:
The radiographs show a scaphoid nonunion with associated dorsal intercalated segmental instability (DISI) pattern. What is the MOST appropriate surgical management for this stage of wrist pathology?

Explanation
At this stage, the primary goal is to address the nonunion and correct the carpal instability if possible, provided there is not severe widespread arthritic change. Percutaneous fixation is only for acute, undisplaced scaphoid fractures. Proximal row carpectomy (PRC) and four-corner arthrodesis are salvage procedures for wrists with established arthritis, which is not explicitly stated as widespread yet, but DISI pattern often implies impending or early arthritis at the radioscaphoid joint. Wrist arthrodesis is a more aggressive salvage for global wrist arthritis or instability.
Repair of the scaphoid nonunion with bone grafting (vascularized or non-vascularized) and internal fixation is the gold standard to achieve union and prevent progression of carpal collapse. Success in achieving union can prevent or slow the progression of arthritis and improve wrist kinematics. Given the chronic nature and DISI, a thorough reconstruction of the scaphoid with bone grafting is required.
Rationale for options:
A. Percutaneous screw fixation is suitable for acute, undisplaced scaphoid fractures or select cases of stable nonunions without significant deformity, not for chronic nonunion with DISI.
B. Proximal row carpectomy (PRC) is a salvage procedure for radioscaphoid arthritis with a healthy lunate facet of the capitate, not typically for nonunion without established advanced arthritis.
C. Scaphoid nonunion repair with bone graft (e.g., iliac crest or vascularized graft) and internal fixation (e.g., screw or K-wires) is the most appropriate treatment to achieve union, correct the DISI deformity, and restore carpal kinematics in cases of chronic nonunion with instability but without severe pan-carpal arthritis. This is the correct answer.
D. Four-corner arthrodesis (fusion of capitate, lunate, triquetrum, hamate, with scaphoid excision) is a salvage procedure performed for radioscaphoid arthritis or early midcarpal arthritis, typically when scaphoid nonunion has progressed to significant collapse with secondary arthritic changes. While DISI suggests progression, without explicit severe arthritis, scaphoid reconstruction is usually tried first.
E. Wrist arthrodesis (fusion of radius, carpals, metacarpals) is a last-resort salvage procedure for severe, diffuse wrist arthritis, instability, or failed previous surgeries, resulting in loss of motion but pain relief.
Question 71
A 12-year-old male presents with a painful, enlarging mass in his distal left femur. Biopsy confirms high-grade osteosarcoma. Staging studies reveal no evidence of metastatic disease. Imaging, including the provided X-ray, shows a large, mixed lytic and blastic lesion with cortical destruction and a soft tissue component.
The multidisciplinary tumor board recommends neoadjuvant chemotherapy followed by surgical resection. Considering limb salvage surgery, which of the following is the MOST critical principle to ensure oncologic success?

Explanation
Surgical margins are classified as:
• Intralesional: Entering the tumor.
• Marginal: Dissecting through the pseudocapsule or reactive zone.
• Wide: Resecting through healthy tissue well outside the reactive zone.
• Radical: Resection of the entire compartment containing the tumor.
A wide surgical margin is necessary to remove all gross and microscopic tumor, minimizing local recurrence. While functional outcome and limb length preservation are important considerations, they are secondary to the primary goal of tumor eradication. Compromising surgical margins significantly increases the risk of local recurrence, which can be devastating for the patient.
Rationale for options:
A. Achieving wide surgical margins through en bloc resection is paramount for oncologic success, meaning removal of the tumor in one piece with a cuff of healthy tissue. This is the correct answer. The functional outcome is important but secondary to tumor clearance.
B. While reconstruction with an expandable prosthesis is a common technique in pediatric limb salvage to manage growth discrepancy, it is a reconstructive principle, not the most critical principle for oncologic success. Oncologic success hinges on tumor removal with clear margins.
C. Adjuvant radiation therapy is generally not effective for osteosarcoma, which is often radioresistant. It is used in specific situations like positive margins, certain tumor types (e.g., Ewing sarcoma, chondrosarcoma), or palliative care, but it is not a primary component of osteosarcoma treatment to sterilize residual cells after an intended wide resection.
D. Performing an intra-articular resection for osteosarcoma is generally avoided unless the tumor is truly extra-articular or the joint itself is involved and necessitates joint sacrifice. An intra-articular approach risks tumor spillage and compromise of margins. The goal is an extra-articular or wide margin resection.
Question 72
A 65-year-old male with a history of diabetes, peripheral neuropathy, and end-stage renal disease presents with a warm, swollen, and deformed right midfoot that developed acutely after a minor twist. Radiographs reveal diffuse osteopenia, joint subluxation, and fragmentation of the navicular and cuneiform bones, consistent with a Charcot neuroarthropathy flare. He is currently non-ambulatory due to pain and instability. What is the most critical immediate management step for this patient?
Explanation
Rationale for options:
A. Immediate surgical stabilization is generally reserved for stable Charcot deformities with ulceration, severe instability that cannot be managed with bracing, or specific fracture patterns, and usually after the acute inflammatory phase has subsided. Operating during the acute inflammatory phase (Eichenholtz Stage I) carries high risks of nonunion, implant failure, and wound complications.
B. Custom orthotics are used for stable, chronic Charcot feet (Eichenholtz Stage III) to prevent recurrence and support the arch, but they are insufficient for an acute flare with active destruction and instability.
C. Total contact casting (TCC) is the cornerstone of immediate management for acute Charcot neuroarthropathy. It offloads the foot, prevents further trauma, and reduces inflammation. Strict non-weight-bearing is essential. This is the correct answer.
D. Systemic corticosteroids are not indicated for Charcot neuroarthropathy and may worsen glycemic control in a diabetic patient, increasing infection risk and potentially contributing to bone fragility.
E. Amputation is a last resort for severe, limb-threatening infection or unbraceable, chronic deformity with recurrent ulceration that fails all other salvage attempts, not an immediate step for an acute flare without overt infection.
Question 73
A 10-year-old child presents after a bicycle accident with transient weakness and paresthesias in both upper and lower extremities, which fully resolved within 2 hours. Neurological examination in the emergency department is now completely normal. Radiographs of the cervical spine, including flexion-extension views, are unremarkable, showing no evidence of fracture or instability.
What is the MOST appropriate next diagnostic step given the clinical presentation?

Explanation
SCIWORA in children is relatively common due to increased spinal elasticity compared to adults, allowing significant deformation of the spinal column and cord injury without bony fracture or ligamentous disruption visible on plain radiographs or CT. MRI can identify spinal cord contusions, edema, hemorrhage, or even ligamentous injury that causes transient compression.
Rationale for options:
A. Discharging without further imaging in a SCIWORA scenario is dangerous. Even with full resolution of symptoms, underlying cord pathology may predispose to recurrent or permanent injury with subsequent trauma.
B. MRI of the cervical spine is the MOST appropriate next diagnostic step. It is crucial for identifying underlying spinal cord abnormalities (contusion, edema, hemorrhage) or soft tissue/ligamentous injuries that explain the transient neurological symptoms, even if radiographs are normal. This is the correct answer.
C. A CT scan is excellent for bony detail but is unlikely to reveal additional information beyond plain radiographs for SCIWORA, as the definition implies no radiographic abnormality (which typically includes CT for bony architecture). It does not visualize the spinal cord or soft tissues as well as MRI.
D. While inpatient observation is warranted, it should be followed by definitive diagnostic imaging (MRI) to determine the cause of SCIWORA and guide long-term management.
E. Electrophysiological studies (EMG/NCS) are typically used to evaluate peripheral nerve or nerve root pathology in chronic conditions or radiculopathy, not for acute spinal cord injury evaluation.
Question 74
A 22-year-old male presents after a high-speed motor vehicle collision with severe pelvic pain. Physical examination reveals a shortened and externally rotated left lower extremity. There is a perineal laceration with suspicion of an open pelvic fracture. Initial pelvic radiographs are obtained:
The radiographs show widening of the left sacroiliac joint, a left sacral fracture, and disruption of the symphysis pubis. Hemodynamic instability is present, requiring ongoing resuscitation. What is the MOST critical immediate management step for this patient?

Explanation
The MOST critical immediate management step for an unstable pelvic fracture with hemodynamic instability is to reduce and stabilize the pelvic ring to decrease the pelvic volume, tamponade venous bleeding, and potentially reduce arterial bleeding. This is typically achieved rapidly in the emergency setting with a pelvic binder or sheet wrap. This immediate action aims to control hemorrhage, which is the leading cause of death in these patients.
While angiography and embolization may be necessary for ongoing arterial hemorrhage, it is usually performed after initial mechanical stabilization. Immediate internal fixation is a definitive step, not an immediate first step in an unstable patient. Diagnostic peritoneal lavage (DPL) or focused assessment with sonography for trauma (FAST) is important for assessing intra-abdominal injuries but not the primary pelvic stabilization step.
Rationale for options:
A. Formal internal fixation is definitive treatment, performed after initial resuscitation and temporary stabilization, typically in the operating room, not as an immediate emergency department step.
B. Pelvic angiography and embolization are crucial for arterial hemorrhage, but mechanical reduction of the pelvis (e.g., with a binder) should precede or occur concurrently to reduce overall pelvic volume and venous bleeding, which is more common.
C. Application of a pelvic binder or sheet wrap is the immediate, life-saving maneuver for an unstable pelvic ring injury with hemodynamic instability. It helps to close the 'open book' and reduce the pelvic volume, thereby tamponading venous hemorrhage. Emergent transfer to a specialized trauma center is also crucial. This is the correct answer.
D. DPL is part of the ATLS protocol to assess intra-abdominal injury, but pelvic stabilization takes precedence for control of hemorrhage originating from the pelvis.
Question 75
A 25-year-old male collegiate baseball pitcher presents with recurrent anterior shoulder dislocations. He has sustained three dislocations in the past year, all related to overhead throwing. Physical examination reveals apprehension with abduction and external rotation. Radiographs, including an axillary view, demonstrate a significant bony Bankart lesion and a Hill-Sachs lesion involving 20% of the humeral head articular surface.
Considering his age, activity level, number of dislocations, and the presence of significant glenoid bone loss, what is the MOST appropriate surgical intervention?
Explanation
For significant glenoid bone loss, the Latarjet procedure (coracoid transfer) is often considered the gold standard. It addresses both glenoid bone loss (by providing a bony block) and provides a sling effect (conjoined tendon of coracobrachialis and short head of biceps).
Rationale for options:
A. Arthroscopic Bankart repair alone is insufficient for significant bone loss (>20-25% glenoid bone loss), leading to high rates of recurrence in high-demand athletes.
B. Open Bankart repair with capsular shift is similar to arthroscopic repair in that it doesn't directly address significant bone loss, and thus has similar limitations in this specific scenario.
C. The Latarjet procedure involves transferring the coracoid process with its attached conjoined tendon to the anterior inferior glenoid. This provides both a bony block to anterior translation and a dynamic sling effect, effectively addressing significant glenoid bone loss and reducing recurrence rates, especially in high-demand athletes with recurrent instability and bone loss. This is the most appropriate choice.
D. The Remplissage procedure (filling the Hill-Sachs defect with the infraspinatus tendon) is typically used for engaging Hill-Sachs lesions without significant glenoid bone loss, or as an adjunct to Bankart repair when glenoid bone loss is borderline.
E. Thermal capsulorrhaphy has largely been abandoned due to high failure rates and potential for chondrolysis.
Question 76
A 16-year-old female presents with persistent pain, instability, and a 'giving way' sensation in her right knee, 18 months after sustaining a multi-ligamentous knee injury (ACL, MCL, PCL tears) that was treated non-operatively due to initial missed diagnosis. Radiographs show early degenerative changes. MRI confirms chronic laxity of all three ligaments. What is the MOST appropriate next step in management?
Explanation
For chronic multiligamentous knee instability with functional limitations, surgical reconstruction is indicated. Given the significant number of ligaments involved, a staged approach is often preferred over a single-stage reconstruction, especially in chronic cases. This allows for soft tissue healing and rehabilitation between stages, reducing the risk of complications associated with a very long single-stage surgery and potentially improving outcomes. The posterior side (PCL/PLC) is often addressed first, as it sets the foundation for knee stability and allows subsequent ACL reconstruction to be performed on a more stable base. The MCL can often heal with non-operative treatment, especially if medial opening is less than 5mm; however, in this chronic, unstable context, MCL reconstruction might also be needed.
Rationale for options:
A. Physical therapy is always important but insufficient to correct chronic multi-ligamentous mechanical instability.
B. A single-stage reconstruction of all three ligaments might be an option, but it's a very extensive procedure with higher risks in a chronic setting. A staged approach is often considered preferable for chronic cases.
C. A hinged knee brace may provide some stability but does not correct the underlying pathology or prevent progression of degenerative changes.
D. A staged reconstruction, typically addressing the PCL and MCL (or PLC) first to establish the posterior and medial stability, followed by the ACL, is a common and often preferred strategy for chronic multiligamentous knee injuries. This allows for recovery and rehabilitation between stages. This is the correct answer.
E. Arthrodesis is a salvage procedure for end-stage arthritis or failed reconstructions, not for early degenerative changes where reconstructive surgery is still feasible.
Question 77
A 48-year-old electrician presents with worsening bilateral shoulder pain and weakness, particularly with overhead activities. He reports chronic symptoms that have been progressive over several years. Physical examination reveals bilateral atrophy of the infraspinatus and supraspinatus muscles, marked weakness in external rotation and abduction, and positive 'horn blower's sign' on the right. MRI of the right shoulder confirms a massive, irreparable rotator cuff tear with significant fatty infiltration and retraction of the supraspinatus and infraspinatus tendons, and superior migration of the humeral head. What is the MOST appropriate surgical management option for this patient?
Explanation
In such cases, particularly in older, low-demand patients or when cuff tear arthropathy is present, Reverse Total Shoulder Arthroplasty (RTSA) is the gold standard. RTSA inverts the ball-and-socket anatomy, medializing and distalizing the center of rotation. This allows the deltoid muscle to become the primary elevator and external rotator of the arm, compensating for the deficient rotator cuff and restoring overhead function and pain relief.
Rationale for options:
A. Arthroscopic rotator cuff repair with augmentation is typically reserved for large but repairable tears, or when augmentation is needed to reinforce a borderline repair. It is ineffective for massive, irreparable tears with significant fatty infiltration and superior migration.
B. Reverse total shoulder arthroplasty (RTSA) is the procedure of choice for massive, irreparable rotator cuff tears with cuff tear arthropathy and pseudoparalysis. It reliably improves pain and function by changing the biomechanics of the shoulder. This is the correct answer.
C. Latissimus dorsi transfer is an option for younger, high-demand patients with irreparable posterosuperior rotator cuff tears who do not have significant cuff tear arthropathy, aiming to restore active external rotation and flexion. It's less effective with significant fatty infiltration and superior migration.
D. Superior capsular reconstruction is a newer technique for irreparable supraspinatus tears, often using an allograft or autograft, aiming to prevent superior humeral head migration and restore mechanics. While it can be considered, RTSA provides more predictable pain relief and functional improvement in the presence of established cuff tear arthropathy and global dysfunction.
E. Debridement and subacromial decompression is a palliative procedure for symptomatic impingement or partial tears but will not restore function in a massive, irreparable tear with superior migration.
Question 78
A 55-year-old obese male with poorly controlled diabetes and a history of previous methicillin-resistant Staphylococcus aureus (MRSA) bacteremia undergoes a total knee arthroplasty (TKA). Two weeks post-operatively, he develops increasing knee pain, swelling, warmth, and erythema. Aspiration of the knee joint yields purulent fluid. Synovial fluid analysis shows a WBC count of 90,000 cells/µL with 95% neutrophils, and a positive Gram stain for Gram-positive cocci. What is the MOST appropriate definitive surgical management approach for this acute periprosthetic joint infection (PJI) if the implant is deemed stable?
Explanation
For acute PJI (symptoms < 3-4 weeks from index surgery or hematogenous onset), if the implant is stable and there is no extensive osteomyelitis or sepsis, a debridement, antibiotics, and implant retention (DAIR) procedure is often considered. This involves irrigation and debridement, exchange of modular components (polyethylene liner), and prolonged culture-specific antibiotic therapy. However, the presence of MRSA, a highly virulent organism, makes DAIR less successful. While the question states 'if the implant is deemed stable', the aggressive nature of MRSA and the early onset of infection often lead to failure of DAIR, pushing towards a more aggressive approach.
A two-stage exchange arthroplasty is the gold standard for chronic PJI or acute PJI with virulent organisms or when DAIR has failed. It involves removal of all components, extensive debridement, placement of an antibiotic-loaded cement spacer, and 6-8 weeks of systemic antibiotics, followed by reimplantation of a new TKA once infection markers normalize. Given the context of a highly virulent organism (MRSA) and the severity of presentation, even with a 'stable' implant, a two-stage exchange carries a higher success rate than DAIR.
Rationale for options:
A. Immediate TKA revision with a two-stage exchange is often considered the most reliable approach for acute PJI caused by virulent organisms like MRSA, or if there's extensive soft tissue involvement, even if the implant is stable. The high virulence of MRSA makes DAIR success rates lower. This is the correct answer.
B. Irrigation and debridement (I&D) with polyethylene exchange and prolonged antibiotic therapy (DAIR) is an option for acute PJI, especially with less virulent organisms and a truly stable implant. However, its success rate is lower with MRSA. So, while an option, it's not the most appropriate definitive approach for MRSA in many centers.
C. Long-term suppressive oral antibiotic therapy without surgery is reserved for patients who are not surgical candidates, or for chronic low-grade infections, and is associated with persistent infection and limited success.
D. Arthrodesis is a salvage procedure for failed PJI treatment or severe irreparable destruction, sacrificing motion for infection eradication and pain relief.
E. Amputation is a last resort for uncontrolled, limb-threatening infection or sepsis that fails all other surgical and antibiotic treatments.
Question 79
A 14-year-old male with a history of slipped capital femoral epiphysis (SCFE) treated with in situ pinning 2 years ago, presents with new onset, severe right hip pain and inability to bear weight. Radiographs show no change in the pin position but reveal subtle flattening and sclerosis of the femoral head epiphysis, consistent with avascular necrosis (AVN). What is the MOST appropriate management strategy for this complication?
Explanation
At 14 years old, with established AVN (subtle flattening and sclerosis imply Ficat Stage III or IV, where collapse has occurred), conservative management is unlikely to alter the progression. Core decompression and bone grafting are typically for earlier stages of AVN (Ficat Stage I or II) without collapse. Total hip arthroplasty (THA) would provide pain relief and restore function, but it is generally deferred in such a young patient due to concerns about implant longevity and revision surgeries. Intertrochanteric osteotomy aims to rotate a healthy portion of the femoral head into the weight-bearing zone, which is not applicable if the entire epiphysis is affected by AVN. However, for a young patient with painful, collapsed AVN of the femoral head after SCFE, a hip fusion (arthrodesis) is often considered a durable option to relieve pain and provide a stable hip for a manual laborer, but it sacrifices motion. Given the options, a THA might be premature, and core decompression is too late. The question doesn't specify the extent of collapse, but 'flattening and sclerosis' implies a significant stage.
Let's re-evaluate the options given the age and complication.
A. Pin removal alone does not address the AVN.
B. Core decompression with bone grafting is indicated for early AVN (pre-collapse stages). Given 'flattening and sclerosis,' collapse has likely occurred, making core decompression less effective.
C. Total hip arthroplasty (THA) in a 14-year-old is a significant decision. While it would address the pain and dysfunction, it is generally deferred. However, if the collapse is severe and the pain is debilitating, and function is severely limited, THA may be the only option to restore function, especially if arthrodesis is not desired. Other options like intertrochanteric osteotomy for realignment are usually considered if there is some preserved cartilage and minimal collapse, or if the AVN is segmental. For diffuse collapse, THA is often considered. This is a tough question due to the age.
Let's consider the alternatives carefully. For significant collapse (flattening and sclerosis imply this), THA or arthrodesis are the main options. Arthrodesis would provide a durable, pain-free hip but eliminates motion. THA provides motion but has longevity concerns. In many cases of significant collapse and pain in a young patient, a THA is chosen to restore function. A salvage procedure like arthrodesis is also a valid consideration. Without knowing the extent of collapse more precisely, it's hard to be absolute.
However, based on high-yield board review, established AVN with collapse in a teenager often points towards either advanced salvage (THA, arthrodesis) or a reconstructive osteotomy if cartilage is preserved. Given the severe pain and inability to bear weight, conservative measures are insufficient. Core decompression is generally not effective for already collapsed heads.
Let's consider that THA, while often delayed, is often the ultimate solution for symptomatic, collapsed AVN in adolescents who can't tolerate fusion. Therefore, it may be the 'most appropriate' among the given choices, especially if function is paramount and the collapse is significant enough to preclude osteotomy.
Rethink: The question asks for MOST appropriate management. For a 14-year-old with established AVN of the femoral head after SCFE with flattening and sclerosis (implying Ficat Stage III-IV), the options are limited. While THA is a major surgery at this age, it offers pain relief and restored function. Arthrodesis is another option for pain relief and durability. Core decompression is for pre-collapse stages. Intertrochanteric osteotomies are usually for residual deformity after SCFE or for containment, not for established AVN with collapse. Therefore, of the given options, THA might be the most comprehensive for pain and function, despite age.
Correction: For severe, symptomatic AVN with collapse in a skeletally immature patient, an intertrochanteric osteotomy may be considered to rotate a viable portion of the femoral head into the weight-bearing zone if a significant viable portion remains. If the entire epiphysis is necrotic or severely collapsed, then THA or arthrodesis are the main options. However, given the young age, THA is often deferred. An alternative, sometimes performed, is a vascularized fibular graft if early enough, but this is not an option. For significant collapse, in situations where arthrodesis is not chosen, THA is often the choice for pain relief and functional restoration.
Let's re-evaluate the question with common board knowledge. If collapse has occurred, core decompression is out. Intertrochanteric osteotomy for AVN might be considered to offload the necrotic segment IF a viable segment exists. But for diffuse flattening and sclerosis, it's less likely to be successful. Therefore, between THA and observation/decompression/osteotomy, THA becomes the most definitive treatment for a painful, collapsed joint. While arthrodesis is a good choice for young heavy laborers for durability, it's not an option here. Therefore, THA is the most likely 'most appropriate' of the given options, despite the age, acknowledging that it's a difficult choice.
Final consideration: Avascular necrosis is a devastating complication. 'Flattening and sclerosis' implies Ficat stage III or IV. In such advanced stages in a young patient, salvage procedures that preserve motion are attempted but often fail, leading to THA. Given the limited options, and the severity of symptoms (inability to bear weight), THA offers the most predictable relief and functional outcome. The alternative would be fusion, which is not an option.
Question 80
A 32-year-old male presents with worsening neck pain, left upper extremity paresthesias, and progressive weakness, particularly in his left hand. Examination reveals intrinsic hand muscle atrophy and weakness (finger abduction/adduction and grip strength). Deep tendon reflexes are hyperreflexic in the lower extremities with a positive Babinski sign. MRI of the cervical spine shows severe central canal stenosis at C5-C6 and C6-C7 with spinal cord compression and T2 signal changes consistent with myelomalacia.
What is the MOST appropriate surgical management approach for this patient?
Explanation
The choice of surgical approach (anterior vs. posterior) and specific procedure depends on the number of levels involved, the location of compression (anterior vs. posterior), and spinal alignment.
• Anterior approaches (ACDF, ACCF): Best for 1-2 level anterior compression. ACDF at C5-C6 only would not address C6-C7 compression. ACCF is for more extensive anterior compression.
• Posterior approaches (laminectomy, laminoplasty, laminectomy and fusion): Better for multi-level posterior compression or when anterior compression is less significant or cannot be adequately addressed anteriorly.
In this case, significant central canal stenosis at two adjacent levels (C5-C6 and C6-C7) with myelopathy, a posterior approach (laminectomy with fusion or laminoplasty) is often preferred for multi-level compression. A simple laminectomy without fusion can lead to post-laminectomy kyphosis and instability, especially in younger patients, and is generally avoided for multi-level decompression in the presence of pre-existing instability or deformity. Laminoplasty is a motion-preserving procedure, but if instability or significant kyphosis is present or anticipated, fusion is indicated.
Given 'severe central canal stenosis at C5-C6 and C6-C7,' and myelomalacia, a comprehensive decompression is needed. Posterior laminectomy and fusion addresses both decompression and provides stability, making it a very robust option for multi-level myelopathy with potential for kyphosis. If the compression is primarily anterior at two levels, an anterior approach (like 2-level ACDF or ACCF + ACDF) would be considered. However, the axial image suggests central stenosis which can be addressed by posterior decompression. Without sagittal images showing lordosis or kyphosis, assuming a relatively neutral or kyphotic alignment (which often accompanies multi-level degenerative disease), posterior laminectomy with fusion is often chosen for comprehensive decompression and stability.
Rationale for options:
A. ACDF at C5-C6 only would not address the C6-C7 stenosis, leaving persistent compression.
B. Posterior cervical laminectomy without fusion is largely abandoned for multi-level decompression due to the high risk of post-laminectomy kyphosis and instability.
C. Cervical laminoplasty is an option for multi-level cervical myelopathy, aiming to decompress the cord while preserving motion. However, it is generally preferred when the patient has a neutral or lordotic sagittal alignment. If the patient has or develops kyphosis, laminoplasty may not provide adequate decompression or may worsen the deformity.
D. Posterior cervical laminectomy and fusion at C5-C7 (or appropriate levels) would provide adequate multi-level decompression of the spinal cord and maintain/restore spinal stability. This is a robust option for multi-level cervical myelopathy and is considered the most appropriate, especially if sagittal alignment is borderline or kyphotic. This is the correct answer.
E. Anterior cervical corpectomy and fusion (ACCF) at C5 and C6 would be a very extensive anterior procedure to address two levels, typically reserved for large anterior osteophytes or disc herniations spanning multiple vertebral bodies. While possible, posterior options for multi-level stenosis are often less morbid.
Question 81
A 4-year-old male is brought to the clinic for evaluation of an insensate, swollen, and progressively deforming right foot. His parents report a history of spina bifida and hydrocephalus requiring a shunt. Clinical examination reveals a rigid, rocker-bottom foot deformity with plantar ulceration and claw toes. Radiographs show significant midfoot collapse, fragmentation, and dislocation of the talonavicular and calcaneocuboid joints.
This presentation is most consistent with a neglected Charcot arthropathy of the foot, secondary to his underlying neurological condition. What is the MOST appropriate surgical management for this severe, rigid, and ulcerated deformity in a young, neuropathic patient?

Explanation
Conservative management (serial casting, orthotics) is generally ineffective for rigid, severe deformities, especially with ulceration, as it cannot correct the underlying bony instability and malalignment. Amputation is a salvage procedure, typically reserved for uncontrolled infection or unbraceable deformities failing all other attempts. Talectomy is primarily used for severe equinus deformity in resistant clubfoot or vertical talus, or for severe hindfoot deformity.
For severe, rigid, and unstable Charcot deformities in children, surgical reconstruction and arthrodesis are often necessary to achieve a plantigrade, stable foot that can be braced and protected from ulceration. Triple arthrodesis (fusion of talocalcaneal, talonavicular, and calcaneocuboid joints) is a common reconstructive procedure for such severe hindfoot and midfoot deformities. In cases of significant midfoot collapse (rocker-bottom), the surgical approach may involve a midfoot osteotomy and fusion (e.g., modified midfoot fusion or 'super-reconstruction') to correct the sag and stabilize the arch, often incorporating principles similar to a triple arthrodesis.
Rationale for options:
A. Serial casting and orthotics are useful for flexible deformities or as an adjunct, but insufficient for a rigid, ulcerated, severe Charcot foot.
B. Talectomy is used for severe equinus or fixed vertical talus, but not typically for a comprehensive reconstruction of a collapsed midfoot Charcot deformity.
C. Triple arthrodesis (fusion of subtalar, talonavicular, and calcaneocuboid joints) is a workhorse procedure for correcting rigid hindfoot and midfoot deformities, providing stability and a plantigrade foot suitable for bracing. Given the severe collapse and instability, a comprehensive fusion is often required. This is the correct answer.
D. Pantalus arthrodesis refers to an ankle and subtalar joint fusion. While relevant for ankle Charcot, the primary deformity described is midfoot collapse, which a triple arthrodesis addresses more directly.
E. Supramalleolar osteotomy is for correction of angular deformities of the distal tibia, not the primary treatment for a rigid, multi-joint foot collapse.
Question 82
A 3-year-old child presents with a high-grade open tibia and fibula fracture (Gustilo-Anderson Type IIIB) sustained in a motor vehicle accident. The fracture is severely comminuted, with extensive soft tissue loss and periosteal stripping. Initial debridement and application of an external fixator have been performed. What is the MOST critical next step in the definitive management plan to achieve fracture union and prevent infection?
Explanation
Rationale for options:
A. Early conversion to intramedullary nailing is a definitive bone fixation strategy but is secondary to achieving soft tissue coverage in a Type IIIB fracture. Nailing without adequate soft tissue coverage has a high infection risk.
B. Vascularized free tissue transfer (free flap) is the most appropriate next step for providing durable soft tissue coverage in a Gustilo-Anderson Type IIIB open fracture with extensive soft tissue loss. This is the correct answer.
C. Primary closure of the wound is typically not possible for Type IIIB injuries due to the extensive soft tissue defect, and attempting it would lead to tension and necrosis.
D. Daily wet-to-dry dressing changes are a form of wound care, but they are insufficient for definitively closing a large soft tissue defect in a Type IIIB fracture. They are used in initial debridement stages but not as a long-term solution for wound closure.
E. Initiation of oral antibiotics is insufficient for an acute, high-grade open fracture. Intravenous broad-spectrum antibiotics, typically covering Gram-positive and Gram-negative organisms (and anaerobes for Type III), are initiated immediately and continued for several days post-closure, often followed by oral antibiotics, but adequate surgical debridement and soft tissue coverage are more critical than antibiotic route for infection prevention.
Question 83
A 68-year-old male with long-standing rheumatoid arthritis presents with progressive wrist pain, swelling, and instability. Clinical examination reveals significant ulnar deviation of the wrist, dorsal subluxation of the extensor carpi ulnaris (ECU) tendon, and progressive rupture of multiple extensor tendons, leading to inability to extend the fingers (Vaughn-Jackson syndrome). Radiographs confirm severe carpal destruction, proximal carpal migration, and significant arthritis of the distal radioulnar joint (DRUJ). What is the MOST appropriate surgical management for this complex wrist pathology?
Explanation
Simple synovectomy or isolated tendon repair is insufficient for this advanced stage. Total wrist arthroplasty (TWA) is an option for pain relief and motion preservation, but it may be contraindicated in cases of significant bone loss, active infection, or high-demand patients, and its longevity in severe RA can be limited. Darrach procedure (distal ulna excision) addresses DRUJ pain but doesn't stabilize the wrist or reconstruct tendons. Sauve-Kapandji addresses DRUJ issues but not the carpal destruction or tendon ruptures.
Given the severe carpal destruction, progressive instability, and multiple tendon ruptures, wrist arthrodesis (fusion) is often the most reliable and durable surgical option to achieve pain relief, stability, and provide a stable platform for subsequent extensor tendon reconstruction. While it sacrifices motion, it provides a functional, pain-free wrist that can withstand loads and facilitate activities of daily living. Tendon reconstruction, often with transfers, is performed concurrently or in a staged fashion.
Rationale for options:
A. Dorsal wrist synovectomy and ECU stabilization are appropriate for early-stage RA with synovitis and tendon issues, but not for severe carpal destruction and multiple tendon ruptures.
B. Total wrist arthroplasty (TWA) aims to preserve motion but may be associated with higher rates of loosening or failure in severe rheumatoid arthritis with significant bone loss and instability. It is generally considered for lower-demand patients or less severe destruction.
C. Darrach procedure (distal ulna excision) addresses painful DRUJ arthritis but does not correct carpal instability, tendon ruptures, or generalized wrist arthritis.
D. Sauve-Kapandji procedure involves DRUJ arthrodesis with a distal ulna pseudarthrosis. It addresses DRUJ issues, but like the Darrach, does not correct the overall carpal instability, tendon ruptures, or the severe carpal destruction mentioned.
E. Wrist arthrodesis (fusion of the radius to the carpus and often to the third metacarpal) is the most definitive and durable solution for end-stage rheumatoid wrist with severe pain, deformity, instability, and tendon ruptures. It provides a stable, pain-free platform, allowing for improved grip and function after tendon reconstruction. This is the correct answer.
Question 84
A 15-year-old male presents with persistent anterior knee pain and a palpable tender mass just distal to the patella. He is active in basketball and gymnastics. Radiographs show fragmentation and irregularity of the patellar tendon insertion onto the tibial tuberosity, consistent with Osgood-Schlatter disease. Despite 6 months of conservative treatment including rest, NSAIDs, and physical therapy, his pain persists, significantly limiting his athletic activities. What is the MOST appropriate next step in management?
Explanation
Given the patient is 15 years old and still skeletally immature (implied by the active apophysis), the MOST appropriate next step is typically continued, often more intensive, conservative management. This could include further activity modification, specific bracing, eccentric quadriceps strengthening, or temporary immobilization. Corticosteroid injections are contraindicated due to the risk of tendon rupture.
Rationale for options:
A. Continued conservative management, with specific focus on activity modification, pain management, and physical therapy, remains the cornerstone until skeletal maturity. The condition is self-limiting and surgical intervention is typically reserved for those who have failed all conservative measures after skeletal maturity. This is the correct answer.
B. Surgical excision of ossicles and debridement of the patellar tendon insertion is a rare indication, reserved for patients who have persistent, debilitating pain from ununited ossicles after skeletal maturity and failed extensive conservative management.
C. Corticosteroid injection into the patellar tendon or tibial tuberosity is contraindicated due to the risk of tendon weakening, rupture, and skin atrophy.
D. Patellar tendon realignment surgery is typically for patellar instability, not for Osgood-Schlatter disease.
E. High tibial osteotomy is performed for unicompartmental knee osteoarthritis with varus deformity, not Osgood-Schlatter disease.
Question 85
A 62-year-old female presents with recurrent episodes of left hip dislocation following a primary total hip arthroplasty performed 3 months ago via a posterior approach. She has undergone two closed reductions. Clinical examination reveals no leg length discrepancy or neurovascular deficits. Radiographs, shown below, indicate appropriate acetabular and femoral component positioning without evidence of loosening.
Given the recurrent dislocations with well-positioned components, what is the MOST appropriate next surgical management strategy?
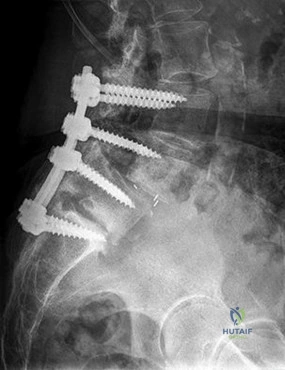
Explanation
A dual-mobility (DM) articulation is a common and effective solution for recurrent hip instability, particularly when component position is acceptable. It uses a small femoral head that articulates within a larger polyethylene liner, which then articulates within the acetabular cup. This 'ball-within-a-ball' design significantly increases the jumping distance required for dislocation, thereby enhancing stability.
Rationale for options:
A. Revision to a more constrained liner might increase stability but also significantly increases stress at the liner-shell interface and can lead to early failure or loosening. It is usually reserved for highly unstable hips where other options have failed, or when neuromuscular deficiencies are present.
B. Revision of the femoral component to a larger head size can increase jumping distance and stability, and is often considered a first-line solution. However, it may still not be sufficient for recurrent dislocations, especially if there are ongoing soft tissue issues or if the initial head size was already adequate for typical primary THA.
C. Conversion to a dual-mobility articulation offers a significant increase in stability and has shown excellent results in reducing dislocation rates in challenging cases, including recurrent dislocations with well-positioned components. It provides a larger 'effective' head size without increasing impingement risks as much as constrained liners. This is often the most appropriate and effective choice for recurrent dislocations when components are well-positioned. This is the correct answer.
D. Open reduction and repair of the posterior capsule might be indicated if the original repair was inadequate, but for recurrent dislocations after initial good repair, it may not be sufficient on its own without addressing the articulation.
E. Abductor advancement and trochanteric osteotomy might be considered for abductor insufficiency but are not the primary solution for recurrent dislocation from a biomechanical perspective of impingement/jumping distance.
Question 86
A 45-year-old male sustains a high-energy crush injury to his right forearm while operating heavy machinery. He presents with severe pain, swelling, and deformity. Clinical examination reveals open fractures of both the distal radius and ulna, significant soft tissue contamination, and signs of impending compartment syndrome. Distal neurovascular status is intact but diminished. What is the MOST critical immediate management step?
Explanation
The immediate management of such a critical injury follows ATLS principles and focuses on limb salvage:
1. Life over limb.
2. Debridement and infection control: For open fractures, urgent irrigation and debridement are paramount to minimize infection risk.
3. Fracture stabilization: Temporary stabilization, often with an external fixator, is necessary to prevent further soft tissue damage and facilitate subsequent care.
4. Soft tissue coverage and compartment syndrome management: Impending compartment syndrome requires emergent fasciotomies to prevent irreversible muscle and nerve damage. This is a limb-saving procedure.
Rationale for options:
A. Closed reduction and splinting are insufficient for open fractures, gross instability, and impending compartment syndrome.
B. Emergency open reduction and internal fixation (ORIF) is the definitive fixation, but not the immediate management, especially with significant contamination and impending compartment syndrome. The priority is debridement, stabilization, and fasciotomy.
C. Urgent irrigation and debridement, fracture stabilization (often with an external fixator as an initial step for temporary stabilization), and fasciotomies (for impending compartment syndrome) are the critical immediate steps in managing this complex, open, high-energy forearm injury. This is the correct answer.
D. While vascular injury is a concern with high-energy trauma, emergent fasciotomies are needed for compartment syndrome. A CT angiogram may be performed after limb-threatening conditions are addressed or as part of vascular repair.
E. Oral antibiotics are insufficient for open fractures; intravenous broad-spectrum antibiotics are required. Outpatient follow-up is inappropriate for such an acute emergency.
Question 87
A 35-year-old construction worker presents with chronic, debilitating pain and stiffness in his left ankle following a pilon fracture sustained 5 years ago, treated with ORIF. Radiographs, shown below, demonstrate severe post-traumatic ankle osteoarthritis with significant joint space narrowing, osteophytes, and subchondral sclerosis. He has failed extensive conservative management, including bracing, NSAIDs, and intra-articular injections.
Given his age, activity level, and the severity of his ankle arthritis, what is the MOST appropriate definitive surgical management?
Explanation
• Ankle arthrodesis (fusion): Historically the gold standard, providing reliable pain relief and stability but sacrificing motion. It's very durable for younger, high-demand patients.
• Total ankle arthroplasty (TAA): A motion-preserving option, increasingly popular with improved implant designs. It aims to reduce pain while maintaining functional motion. Ideal candidates are typically older, lower-demand patients with less deformity and good bone stock. However, in appropriately selected younger, active patients, TAA is now being considered more often.
Given his age (35), a relatively young and active patient, the choice between fusion and TAA can be complex. Historically, fusion would be preferred for a high-demand, young patient. However, modern TAA designs have improved significantly, and given the patient's desire for motion and the advancement in implants, TAA is increasingly offered to younger, active patients, carefully weighing the pros and cons against fusion. The term 'MOST appropriate' is key here.
Rationale for options:
A. Arthroscopic debridement and microfracture are for early, localized cartilage lesions, not end-stage arthritis.
B. Ankle distraction arthroplasty is an experimental or limited use technique for moderate arthritis, aimed at improving joint health, not for severe, end-stage arthritis.
C. Total ankle arthroplasty (TAA) is a viable option for end-stage ankle arthritis. While historically fusion was preferred for younger, active patients, modern TAA has expanded its indications to include younger patients who desire motion and have appropriate anatomy. It is a reasonable and increasingly common choice for patients seeking to preserve motion. This is the correct answer, reflecting current trends in ankle arthroplasty.
D. Ankle arthrodesis (fusion) is a very durable option for end-stage ankle arthritis, particularly for high-demand patients. It provides excellent pain relief but sacrifices motion. While a strong contender, TAA is a more contemporary approach for motion preservation in selected patients.
E. Supramalleolar osteotomy is for correction of ankle malalignment leading to arthritis (e.g., varus or valgus deformity) in cases of early or moderate, non-end-stage arthritis.
Question 88
A 17-year-old male presents with chronic, progressive right hip pain and a limping gait for the past 6 months. Physical examination reveals a restricted range of motion, particularly internal rotation and abduction, and a positive Trendelenburg sign. Radiographs show a flattened and irregular femoral head epiphysis with increased density and widening of the physeal plate, consistent with Legg-Calvé-Perthes disease (LCPD). He is classified as Catterall Group IV with poor prognosis factors (e.g., age > 8 years, lateral pillar collapse).
Given the advanced age (approaching skeletal maturity) and poor prognostic indicators, what is the MOST appropriate surgical management strategy to improve hip containment and long-term outcomes?

Explanation
For older children (typically > 8 years old) with severe LCPD and significant deformity, containment surgeries are often performed. Femoral varus osteotomy aims to redirect the femoral head into the acetabulum. Pelvic osteotomies (e.g., Salter, Dega, Pemberton) reshape the acetabulum. The choice depends on the specific deformity.
Given the poor prognostic factors and advanced age, achieving a perfectly spherical femoral head is challenging. A femoral varus osteotomy is designed to improve containment by bringing the lateral portion of the femoral head into the acetabulum, providing better coverage for the collapsing epiphysis. This can help prevent further collapse and improve congruence, even in older children with residual deformity.
Rationale for options:
A. Continued non-weight-bearing and abduction orthosis are typically for younger children (under 6-8 years) with LCPD during the early phases of the disease to maintain containment, and are ineffective for older children with established severe deformity.
B. Core decompression of the femoral head is used for avascular necrosis (AVN) in adults, not for LCPD.
C. Femoral varus osteotomy (or other containment osteotomies like pelvic osteotomy) is indicated for older children (typically > 8 years) with LCPD, especially those with poor prognostic factors, to improve containment and prevent further collapse. A varus osteotomy improves coverage of the femoral head within the acetabulum. This is the correct answer.
D. Pelvic osteotomy (e.g., Salter) is also a containment procedure, typically for younger children or those with a deficient acetabular roof. It's often used in conjunction with femoral osteotomies or alone, depending on the specific deformity. However, for a 17-year-old with established disease and potential for relative overcoverage laterally, a femoral osteotomy might be more precise.
E. Total hip arthroplasty (THA) is a salvage procedure for end-stage arthritis in adults or severely symptomatic, painful hips in younger adults after failed prior surgeries, and is premature as a primary management strategy for a 17-year-old with LCPD.
Question 89
A 70-year-old male with a history of recurrent left total hip arthroplasty (THA) dislocations and significant abductor deficiency presents for evaluation. He has previously undergone two revisions, including a constrained liner, but continues to dislocate. Radiographs indicate stable, well-positioned components. He is now considering further surgical intervention due to severe functional limitation and pain. What is the MOST appropriate management strategy to address his persistent instability?
Explanation
In such complex cases, particularly when simpler solutions like larger heads or dual mobility have failed or are deemed insufficient, further surgical options are limited. A dual-mobility articulation is generally excellent for recurrent instability, but the question states he has failed previous revisions, including a constrained liner. This implies a very high risk of dislocation.
For recurrent dislocations that persist after dual mobility or even constrained liners, and particularly with severe abductor deficiency (which removes a major dynamic stabilizer), further options include:
1. Abductor repair/reconstruction: If abductor deficiency is the primary cause.
2. Greater trochanteric advancement: To improve abductor lever arm.
3. Hip arthrodesis: As a salvage option, sacrificing motion for stability and pain relief.
4. Complete removal of components (Girdlestone arthroplasty): As a last resort for chronic infection or intractable pain/instability, leaving a pseudarthrosis.
Given the options, and the severe, persistent instability after multiple revisions (including constrained liner), an abductor repair and potentially gluteal muscle transfer (e.g., gluteus maximus or vastus lateralis transfer) is a reconstructive attempt to restore dynamic stability. This directly addresses the abductor deficiency, which is highlighted in the scenario. While arthrodesis is a salvage option, addressing the abductor deficiency offers a chance to maintain motion.
Rationale for options:
A. Repeat revision to a constrained liner with larger head is unlikely to be more successful given the failure of a previous constrained liner and the underlying abductor deficiency.
B. Revision to a dual-mobility articulation is a strong option for recurrent instability, but the scenario implies failure of even constrained liners, suggesting a dual-mobility might not be enough or was already tried if 'revisions' were comprehensive.
C. Open reduction with abductor tendon repair and gluteal muscle transfer directly addresses the underlying abductor deficiency, which is a significant contributor to instability, especially when components are well-positioned. This reconstructive approach aims to restore dynamic stability and function. This is the correct answer.
D. Placement of a hinged external fixator is not a definitive long-term solution for chronic THA instability.
E. Surgical arthrodesis of the hip joint is a salvage procedure that sacrifices motion for stability and pain relief. While an option for intractable instability, a reconstructive attempt to restore some motion (like abductor transfer) is usually preferred if feasible.
Question 90
A 28-year-old female sustains a crush injury to her dominant right hand. She develops a complete radial nerve palsy at the forearm level. After 6 months of observation and physical therapy, there is no evidence of motor recovery, and electrodiagnostic studies confirm a complete nerve transection. What is the MOST appropriate next surgical step to restore hand function?
Explanation
For a complete nerve transection with a gap, nerve grafting is the appropriate reconstructive technique. This involves harvesting a nerve graft (e.g., sural nerve) and coapting the ends to bridge the gap in the radial nerve. The goal is to provide a conduit for regenerating axons to cross the defect.
Rationale for options:
A. Nerve grafting of the radial nerve is the most appropriate surgical intervention for a complete radial nerve transection with a nerve gap, especially after 6 months where primary repair is unlikely due to retraction. This is the correct answer.
B. Primary repair of the radial nerve would be ideal if performed acutely after injury with minimal gap. After 6 months, significant retraction makes primary repair without tension highly improbable.
C. Tendon transfers are typically considered if nerve reconstruction (repair or graft) is not feasible, has failed, or if the time for reinnervation (usually 12-18 months) has passed without functional recovery. It is a salvage procedure, not the primary choice for an acute transection with a potentially reconstructible nerve.
D. Dynamic splinting is supportive care; continued observation for a complete transection after 6 months is inappropriate without surgical intervention.
E. Exploration and neurolysis are for nerve compression or scarring, not for complete transection.
Question 91
A 38-year-old male competitive runner presents with chronic left knee pain, swelling, and mechanical symptoms (catching/locking) that are worse with pivoting activities. MRI reveals a complex tear of the posterior horn of the medial meniscus, extending to the meniscocapsular junction, with radial components, suggesting a meniscal root tear. There is extrusion of the medial meniscus.
Given the patient's age, activity level, and the nature of the tear, what is the MOST appropriate surgical management?

Explanation
Arthroscopic repair of a meniscal root tear involves reattaching the avulsed root to its anatomical insertion site, typically using a transosseous technique or suture anchors. This aims to restore the hoop stress function, reduce tibiofemoral contact pressures, and prevent or delay the onset of osteoarthritis. Partial meniscectomy for root tears has been shown to lead to poor long-term outcomes, similar to total meniscectomy.
Rationale for options:
A. Arthroscopic partial meniscectomy for a meniscal root tear is contraindicated as it removes more meniscal tissue and does not restore the hoop stress function, leading to accelerated osteoarthritis. It is essentially equivalent to a total meniscectomy in terms of biomechanical consequences.
B. Arthroscopic repair of the meniscal root tear (e.g., using a pull-out suture technique) is the gold standard treatment for symptomatic, repairable meniscal root tears, especially in young, active patients, to restore meniscal function and prevent progression to osteoarthritis. This is the correct answer.
C. Total meniscectomy is an outdated procedure for meniscal tears, known to cause early osteoarthritis, and is inappropriate for this patient.
D. High tibial osteotomy (HTO) is considered for unicompartmental osteoarthritis with varus malalignment, often as an adjunct to meniscal repair in cases with significant malalignment, but not as the primary treatment for a meniscal root tear alone.
E. Non-operative management is typically for asymptomatic tears or those in older, low-demand patients without mechanical symptoms, and is generally not recommended for a young, active patient with symptomatic root tear and extrusion.
Question 92
A 5-year-old female presents with progressive bowing of her left leg. She has a history of prematurity and has been diagnosed with hypophosphatemic rickets (X-linked dominant). She has been on oral phosphate and calcitriol supplementation for 2 years, but her bowing deformity has worsened. Radiographs demonstrate severe genu varum deformity with widening and fraying of the physeal plates.
What is the MOST appropriate surgical management for her worsening deformity?

Explanation
For progressive angular deformities in skeletally immature children, guided growth techniques (also known as 'tethering' or 'hemi-epiphysiodesis') are the preferred method. This involves placing a plate and screws (e.g., tension band plating or 8-plate) on the convex side of the deformity. In genu varum (bow-leg), this means plating the medial side of the distal femur and/or proximal tibia. This slows growth on the medial side, allowing the lateral side to catch up, thereby gradually correcting the deformity over time. This avoids acute osteotomies, which carry higher risks of neurovascular injury, compartment syndrome, and recurrence, especially in patients with metabolic bone disease.
Rationale for options:
A. Continued medical management alone is insufficient as the deformity is worsening despite 2 years of treatment. While medical management is crucial, it may not prevent all deformities, and surgical intervention is needed for established angular deformities.
B. Placement of a guided growth plate (hemi-epiphysiodesis) on the medial side of the distal femur and proximal tibia is the most appropriate surgical intervention for progressive genu varum in a growing child with rickets, allowing for gradual, physiological correction. This is the correct answer.
C. Acute corrective osteotomy with internal fixation is an option for older children or severe, fixed deformities, but it is more invasive and carries higher risks (recurrence, neurovascular injury) compared to guided growth in a young, growing child, especially with underlying metabolic bone disease.
D. External fixator application for gradual correction (e.g., Ilizarov) is effective but generally reserved for very severe, multiplanar deformities, or limb lengthening, and is more cumbersome than guided growth for simple angular correction.
E. Amputation is a salvage procedure for severe, irreversible conditions, not indicated here.
Question 93
A 7-year-old male with a history of recurrent osteomyelitis in his left tibia presents with increasing pain, swelling, and erythema localized to the anterior mid-tibia. Radiographs show a sclerotic bone lesion with a central lucency and periosteal reaction, consistent with Brodie's abscess. Despite broad-spectrum intravenous antibiotics administered for 4 weeks, his symptoms have not resolved, and inflammatory markers remain elevated. What is the MOST appropriate next step in management?
Explanation
Surgical debridement, curettage of the abscess cavity, and removal of necrotic bone (sequestrum, if present) are the mainstays of treatment. Following debridement, the cavity can be packed with antibiotic-impregnated bone cement beads (e.g., PMMA beads with vancomycin/gentamicin) to provide high local concentrations of antibiotics. This is often followed by systemic culture-specific antibiotics.
Rationale for options:
A. Continuing intravenous antibiotics alone is unlikely to resolve the abscess, which is a walled-off lesion requiring surgical drainage and debridement.
B. Switching to oral antibiotics is inappropriate given the failure of IV antibiotics and persistent inflammation.
C. Surgical debridement and curettage of the lesion with antibiotic bead placement is the definitive treatment for a Brodie's abscess that has failed conservative management. This is the correct answer.
D. While chronic osteomyelitis can sometimes mimic tumors (and vice versa), the imaging findings described (sclerotic bone lesion with central lucency and periosteal reaction) are classic for Brodie's abscess. A CT may provide more detail but the immediate concern is infection management. Malignancy should always be considered in persistent bone lesions, but given the history of recurrent osteomyelitis and classic radiographic appearance, addressing the infection is paramount.
E. Amputation is a last resort for uncontrolled, limb-threatening infection or severe bone destruction, not for a localized Brodie's abscess.
Question 94
A 72-year-old male undergoes revision total knee arthroplasty (TKA) for aseptic loosening of the tibial component. During the surgery, a significant uncontained cavitary defect is identified in the proximal tibia, consistent with a Paprosky Type 2 bone defect. The defect extends to the metaphyseal bone but does not compromise the cortical rim for rotational stability. What is the MOST appropriate reconstructive option for this defect?
Explanation
For contained cavitary or segmental defects where the cortical rim provides support, metal augments (wedges or blocks) are the preferred reconstructive option. These augments restore the bone stock, provide a stable platform for the new component, and can be cemented or screwed into place. Cement packing alone is insufficient for structural defects, and uncemented stems with metal cones are typically for more severe, uncontained defects or when significant metaphyseal bone loss prevents stable fixation with augments.
Rationale for options:
A. Primary cement fixation alone is insufficient for a Paprosky Type 2 defect as it does not address the bone loss and could lead to early loosening.
B. Use of a metal augment (wedge or block) with cement fixation is the standard and most appropriate reconstructive technique for contained Paprosky Type 2 tibial bone defects in revision TKA. The augment restores the bone stock and provides a stable foundation. This is the correct answer.
C. Placement of an extensively porous-coated uncemented stem with a metal cone is typically used for more severe Paprosky Type 3 defects, where there is significant metaphyseal bone loss and compromise of the cortical rim, requiring extensive metaphyseal fixation.
D. Structural allograft reconstruction with a custom implant is reserved for very extensive, complex defects (Paprosky Type 4 or severe Type 3) with massive bone loss, often requiring custom components.
E. Methyl methacrylate cement packing alone is insufficient for a structural defect and would be prone to early failure.
Question 95
A 12-year-old female presents with persistent, severe left knee pain following an athletic injury. Radiographs are unremarkable. MRI, however, reveals a large osteochondral lesion on the lateral aspect of the medial femoral condyle, consistent with Osteochondritis Dissecans (OCD). The lesion is stable but significantly large (2.5 cm x 2.0 cm) and the patient is skeletally immature. What is the MOST appropriate surgical management for this lesion?
Explanation
For stable OCD lesions in skeletally immature patients that fail conservative management, or are deemed unlikely to heal spontaneously (e.g., large size), transarticular or retroarticular drilling is often the first-line surgical treatment. The goal of drilling is to stimulate blood flow and healing across the cartilage-bone interface without violating the articular cartilage surface (if transarticular drilling is used, care is taken not to penetrate the cartilage surface in multiple passes). Retroarticular drilling allows multiple drilling sites from outside the joint without disrupting the articular surface. The image is not provided, so the stability is based on the question text.
Rationale for options:
A. While initial non-operative management is standard for stable OCD, the 'persistent, severe pain' and 'significantly large' size after failure of 6 months non-operative care makes continued non-op less appropriate as the next step.
B. Arthroscopic debridement and microfracture are typically for unstable lesions, loose bodies, or focal chondral defects without a significant underlying bone defect, not for stable OCD with intact cartilage overlying the lesion.
C. Transarticular drilling (or retroarticular drilling) is the most appropriate surgical management for large, stable OCD lesions in skeletally immature patients that have failed conservative management, as it promotes healing of the lesion while preserving the articular cartilage. This is the correct answer.
D. Osteochondral autograft transplantation (OATs) is used for unstable or loose OCD lesions, or full-thickness chondral defects, typically in the adult or near-skeletally mature patient. It is more invasive than drilling and involves harvesting cartilage and bone from a non-weight-bearing area.
E. Autologous chondrocyte implantation (ACI) is also for large, full-thickness chondral defects, usually in adults, and is a two-stage procedure; it is not typically used for stable OCD lesions in skeletally immature patients.
Question 96
A 68-year-old male with severe, multi-level lumbar spinal stenosis and degenerative spondylolisthesis at L4-L5 presents with intractable neurogenic claudication and radicular pain despite extensive conservative treatment. MRI shows significant central canal stenosis and bilateral neuroforaminal stenosis at L4-L5 and L5-S1. Given his symptoms and radiographic findings, which surgical approach is MOST appropriate?
Explanation
For multi-level stenosis with degenerative spondylolisthesis, simple decompression alone (e.g., microdiscectomy, hemilaminectomy, or laminectomy without fusion) carries a high risk of increasing instability, progression of spondylolisthesis, and recurrence of symptoms. Therefore, decompression combined with instrumented fusion is generally recommended for degenerative spondylolisthesis, especially when multi-level or with instability.
A laminectomy and instrumented fusion from L4 to S1 would provide comprehensive decompression for the multi-level stenosis and stabilize the L4-L5 spondylolisthesis and the adjacent L5-S1 segment (which also has stenosis and benefits from fusion due to biomechanical changes). This is a well-established and robust approach.
Rationale for options:
A. Microdiscectomy is for disc herniation and nerve root compression, not primarily for multi-level spinal stenosis with spondylolisthesis. It would not address the stenosis or instability.
B. Laminectomy and instrumented fusion from L4 to S1 addresses both the multi-level spinal stenosis (decompression) and the degenerative spondylolisthesis (stabilization), providing a durable solution. This is the correct answer.
C. Unilateral hemilaminectomy and decompression at L4-L5 only is inadequate for multi-level stenosis and would not stabilize the spondylolisthesis.
D. Posterior lumbar interbody fusion (PLIF) at L4-L5 only would address the spondylolisthesis and stenosis at that level, but would not address the L5-S1 stenosis. While a PLIF is a type of instrumented fusion, the choice needs to cover all symptomatic levels.
E. Laminoplasty is a technique primarily used in the cervical spine to decompress the spinal cord while preserving motion; it is not a standard procedure for lumbar spinal stenosis, especially with spondylolisthesis.
Question 97
A 6-year-old male is evaluated for a progressively worsening left upper extremity deformity and functional limitation. He was born with a congenitally short ulna and radial head dislocation. Clinical examination reveals significant forearm bowing, restricted elbow and wrist motion, and instability of the radial head. Radiographs confirm severe ulnar hypoplasia, radial bowing, and a dislocated radial head. Which of the following is the MOST appropriate surgical management strategy for this patient?
Explanation
The management aims to improve forearm alignment and elbow/wrist function. Early radial head excision is generally contraindicated in skeletally immature patients as it can lead to further deformity (progressive ulnar deviation of the wrist) and loss of distal radial support. DRUJ fusion is not indicated here.
For this complex deformity, a multi-stage approach is often required. The primary goals are to restore forearm alignment and length. Ulnar lengthening (often with an external fixator) combined with a radial osteotomy to correct the bowing can improve forearm length and alignment. This may indirectly help in reducing the radial head or improving the conditions for a stable reduction if attempted. Bone grafting may be necessary to augment lengthening.
Rationale for options:
A. Early radial head excision in a growing child is generally contraindicated because it can lead to progressive proximal migration of the radius and severe radial deviation of the wrist, worsening the deformity and function.
B. Ulnar lengthening with bone grafting and radial osteotomy to correct bowing is the most comprehensive and appropriate surgical strategy for this severe congenital forearm deformity. It addresses the fundamental issues of ulnar deficiency and radial bowing, aiming to restore overall forearm length and alignment. This is the correct answer.
C. Forearm osteotomy to correct radial bowing and stabilize radial head may be part of the treatment, but without addressing the ulnar hypoplasia (length discrepancy), the deformity will likely recur or persist. Stabilization of the radial head can be very difficult with severe ulnar hypoplasia.
D. Distal radioulnar joint (DRUJ) fusion is not indicated as the primary issue is the radial head dislocation and overall forearm length/alignment, not an isolated DRUJ problem.
E. Observation is inappropriate for a progressively worsening, severe deformity in a young, growing child, as it will likely lead to irreversible functional loss.
Question 98
A 3-year-old male presents with a painful, swollen left knee. He has a history of hemophilia A and recently experienced a minor fall. Physical examination reveals a warm, swollen knee with limited range of motion and significant tenderness. Radiographs show signs of soft tissue swelling but no acute fracture. Laboratory tests reveal an elevated activated partial thromboplastin time (aPTT). What is the MOST critical immediate management step?
Explanation
The MOST critical immediate management step for suspected hemarthrosis in a hemophiliac is to administer the deficient clotting factor (Factor VIII in hemophilia A) to achieve hemostasis and prevent further bleeding and joint damage. This should be done promptly without delay. Aspiration can be diagnostic and therapeutic but should follow factor replacement to minimize bleeding risk.
Rationale for options:
A. Aspiration of the knee joint is diagnostic and can relieve pressure, but it should be performed after factor replacement to minimize bleeding risk. It is not the first critical step.
B. Administration of factor VIII concentrate is the most critical immediate step to stop the bleeding and prevent further joint damage. This is the correct answer.
C. Application of a knee immobilizer and ice are supportive measures for pain and swelling, but they do not address the underlying bleeding disorder.
D. Initiation of oral pain medication and physical therapy are insufficient and inappropriate as immediate management without addressing the bleeding.
E. Urgent MRI can be helpful for assessing joint damage but is secondary to immediate factor replacement and hemorrhage control.
Question 99
A 55-year-old female presents with severe, progressive right foot pain and deformity for 2 years. She has a history of systemic lupus erythematosus (SLE) and chronic steroid use. Clinical examination reveals a fixed, planovalgus foot deformity with a prominence medially. Radiographs demonstrate collapse of the midfoot arch, marked talonavicular subluxation, and degenerative changes, consistent with a severe pes planovalgus deformity with secondary arthritis. What is the MOST appropriate surgical treatment for this rigid, symptomatic deformity in a patient with SLE and chronic steroid use?
Explanation
Conservative measures (orthotics) are typically ineffective for rigid deformities with established arthritis. Isolated subtalar arthrodesis or medializing calcaneal osteotomy with FDL transfer are reconstructive procedures often used for flexible flatfoot or early stages of rigid flatfoot, but they are unlikely to be sufficient for a severe, rigid deformity with talonavicular subluxation and arthritis.
For severe, rigid pes planovalgus deformity with significant talonavicular subluxation and secondary arthritis, a triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is often the most appropriate and reliable surgical option. It corrects the deformity, provides a stable, pain-free plantigrade foot, and addresses the multi-joint arthritis. The history of SLE and steroid use means attention to wound healing and bone fusion potential is critical, but triple arthrodesis is a proven salvage.
Rationale for options:
A. Isolated subtalar arthrodesis is for flexible flatfoot or less severe rigid flatfoot primarily affecting the subtalar joint. It would not correct the severe midfoot collapse and talonavicular subluxation.
B. Medializing calcaneal osteotomy and FDL transfer are common procedures for flexible flatfoot reconstruction (adult acquired flatfoot deformity) and are insufficient for a rigid deformity with advanced arthritis.
C. Triple arthrodesis (fusion of subtalar, talonavicular, and calcaneocuboid joints) is the definitive treatment for severe, rigid pes planovalgus deformity with secondary arthritis. It provides correction, stability, and pain relief. This is the correct answer.
D. Lateral column lengthening with a calcaneocuboid fusion is a component of some flatfoot reconstructions but is not a comprehensive solution for a severe, rigid, multi-joint arthritic deformity.
E. Custom orthotics and shoe modifications are conservative measures, which have already failed given the chronic and worsening nature of the rigid deformity.
Question 100
A 60-year-old male presents with chronic low back pain, radiculopathy, and progressive neurological deficits in both lower extremities. Imaging reveals a large sacral mass consistent with a chordoma. The tumor involves the S3 and S4 segments of the sacrum, with extension into the soft tissues and rectum. Biopsy confirms chordoma. What is the MOST appropriate surgical approach and margin goal for this tumor?
Explanation
Due to their location (sacrum) and extension, sacral chordomas often require complex surgical approaches, frequently a combined anterior and posterior approach, to achieve wide margins while minimizing damage to vital structures like the rectum, bladder, and nerve roots. The level of sacrectomy dictates functional outcomes (S3 or below preserves most bladder/bowel function). Intralesional or marginal resections are associated with high recurrence rates.
Rationale for options:
A. Intralesional debulking is associated with very high local recurrence rates and is reserved for palliative care or situations where wide resection is impossible and the goal is symptom relief, not oncologic cure.
B. Marginal excision, especially via a posterior approach only for a tumor with anterior extension, is insufficient for a chordoma and would lead to high local recurrence rates.
C. En bloc wide resection with sacrectomy, often requiring a combined anterior and posterior approach to achieve negative margins, is the gold standard for sacral chordomas. This is the correct answer.
D. Radiation therapy is often used as an adjunct to surgery, especially for positive margins or unresectable tumors, but it is not the primary curative treatment for chordomas due to their radioresistance and the need for high doses that can damage adjacent structures.
E. Complete amputation of both lower extremities is an extreme measure not indicated for a sacral chordoma, which is locally invasive but typically does not metastasize widely until late stages.
