Orthopedics Hyperguide Review | Dr Hutaif General Ortho -...
14 Apr 2026
109 min read
90 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedics Hyperguide Review | Dr Hutaif Gen...
00:00
Start Quiz
Question 1High Yield
Which of the following proteins or genes is necessary for bone formation and induces osteocalcin:
Explanation
C ore binding factor alpha 1 (C bfa1) and its gene (Cbfa1) have been described as anabolic regulators of bone. C bfa1 is a transcription factor and is responsible for the differentiation of precursor cells into osteoblasts. It also enhances differentiation of chondrocytes during enchondral bone formation. When there is deficiency of C bfa1, there can be abnormal bone development as in cleidocranial dysplasia.
Question 2High Yield
A 25-year-old male is involved in an high-speed motor vehicle collision and sustains a closed femoral shaft fracture. During further evaluation, a CT scan of the chest/abdomen/pelvis reveals a nondisplaced ipsilateral femoral neck fracture. Which of the following treatment options will most likely achieve anatomic healing of the femoral neck and minimize the risk of complications?
Explanation
An ipsilateral femoral neck fracture occurs in approximately 6% to 9% of all femoral shaft fractures. A comminuted midshaft femoral fracture secondary to axial loading should alert the treating physician to the possibility of an associated femoral neck fracture. As a result, trauma CT scans should be reviewed for non to minimally displaced femoral neck fractures during the
initial work up.
Watson et al did a retrospective review of 13 patients who had healing complications develop after their index surgical procedure for ipsilateral femoral shaft and neck fractures. Six of the eight (75%) femoral neck nonunions occurred after the use of a second generation, reconstruction-type intramedullary nail. Factors contributing to nonunion of the femoral shaft were the presence of an open fracture, use of an unreamed, small diameter intramedullary nail, and prolonged delay to weightbearing. Lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications.
Peljovich et al discuss that several treatment options are described in the literature, but no clear consensus exists regarding the optimal treatment of neck/shaft fractures. Due to the the potentially devastating complications of the femoral neck fracture in young patients (avascular necrosis, nonunion, and malunion), the neck fracture should be treated first followed by the shaft.
Current recommendations involve treating the neck with a sliding hip screw versus cannulated screws followed by intramedullary nailing of the femoral shaft.
initial work up.
Watson et al did a retrospective review of 13 patients who had healing complications develop after their index surgical procedure for ipsilateral femoral shaft and neck fractures. Six of the eight (75%) femoral neck nonunions occurred after the use of a second generation, reconstruction-type intramedullary nail. Factors contributing to nonunion of the femoral shaft were the presence of an open fracture, use of an unreamed, small diameter intramedullary nail, and prolonged delay to weightbearing. Lag screw fixation of the femoral neck fracture and reamed intramedullary nailing for shaft fracture stabilization were associated with the fewest complications.
Peljovich et al discuss that several treatment options are described in the literature, but no clear consensus exists regarding the optimal treatment of neck/shaft fractures. Due to the the potentially devastating complications of the femoral neck fracture in young patients (avascular necrosis, nonunion, and malunion), the neck fracture should be treated first followed by the shaft.
Current recommendations involve treating the neck with a sliding hip screw versus cannulated screws followed by intramedullary nailing of the femoral shaft.
Question 3High Yield
A 21-year-old female cross-country runner is brought to the medical tent after completing her run. The race took place during an unseasonably warm day in August. The patient is disoriented upon her arrival to the tent and cannot state the exact date. What is the next most appropriate course of action?
37
37
Explanation
The patient is suffering from heat stroke due to the neurologic changes noted by confusion (can not state the date). This is a medical emergency and should be treated with immediate cold-water ice bath immersion and temperature monitoring with a rectal thermometer. Administration of IV fluids is controversial and is not first-line treatment for heat stroke. Transport to a hospital should be delayed until immediate cooling has been achieved and rectal temperature begins to decrease.
Question 4High Yield
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more
than the extension space?
than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 5High Yield
Figures 1 through 3 show the CT and radiographs of a 45-year-old woman who has low back pain and severe left leg pain in the L5 distribution that is not responsive to nonoperative management (physical therapy, epidural injections, pain medications) for 9 months. What is an appropriate treatment option for this patient?

Explanation
■
The figures show a grade 1 spondylolisthesis at L4-L5 along with a left sided facet cyst in a patient with ongoing symptoms despite nonoperative management. A lumbar decompression with a fusion would be an appropriate treatment option in this patient. There is no evidence in the literature for a lateral lumbar interbody fusion without directly decompressing the spinal canal for treatment of spondylolisthesis in the presence of a large facet cyst. Such procedures have been shown to be successful for treatment in the presence of spinal stenosis from ligament hypertrophy, disk bulge, foraminal stenosis. However, there is no evidence for their effectiveness in the presence of a large facet cyst. Similarly facet cyst aspiration has no evidence for treatment of this pathology. A facetectomy and cyst removal may adequately decompress the L4-L5 level. However, this is likely to create further instability in the presence of a spondylolisthesis.
The figures show a grade 1 spondylolisthesis at L4-L5 along with a left sided facet cyst in a patient with ongoing symptoms despite nonoperative management. A lumbar decompression with a fusion would be an appropriate treatment option in this patient. There is no evidence in the literature for a lateral lumbar interbody fusion without directly decompressing the spinal canal for treatment of spondylolisthesis in the presence of a large facet cyst. Such procedures have been shown to be successful for treatment in the presence of spinal stenosis from ligament hypertrophy, disk bulge, foraminal stenosis. However, there is no evidence for their effectiveness in the presence of a large facet cyst. Similarly facet cyst aspiration has no evidence for treatment of this pathology. A facetectomy and cyst removal may adequately decompress the L4-L5 level. However, this is likely to create further instability in the presence of a spondylolisthesis.
Question 6High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic.
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
76. A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm3 (normal 3,500 to 10,500/ mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
1- Subacromial corticosteroid injection
2- Aspiration of the subacromial and glenohumeral joint spaces
3- Nonsteroidal anti-inflammatory drugs
4- Extensive surgical debridement
5- Diagnostic arthroscopy
PREFERRED RESPONSE: 2
DISCUSSION: Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection.
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
76. A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm3 (normal 3,500 to 10,500/ mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
1- Subacromial corticosteroid injection
2- Aspiration of the subacromial and glenohumeral joint spaces
3- Nonsteroidal anti-inflammatory drugs
4- Extensive surgical debridement
5- Diagnostic arthroscopy
PREFERRED RESPONSE: 2
DISCUSSION: Deep sepsis of the shoulder following rotator cuff repair is an uncommon problem. Patients with infections of this type typically report persistent pain and are not systemically ill. They may have signs of local wound problems such as erythema, drainage, and dehiscence. Laboratory studies can be helpful in making an accurate diagnosis. Most patients will not show a significant elevation of the WBC count; however, an elevated erythrocyte sedimentation rate is nearly always present and should alert the clinician to the presence of infection. Aspiration of both subacromial and glenohumeral joint spaces is necessary to confirm the diagnosis. The most effective treatment for deep shoulder sepsis following rotator cuff repair involves extensive surgical debridement, removing all suspicious soft tissue as well as implants. Administration of appropriate antibiotic therapy is needed for complete control of the infection.
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 7High Yield
Figures 1 and 2 are the radiographs of an 8-year-old boy who was brought to the emergency department after falling from monkey bars. The clinical finding in Firgure 3 is caused by impingement of the proximal bone fragment on which structure?

Explanation
■
The clinical findings of anterior skin puckering with ecchymosis is caused by impingement of the brachialis fascia by the proximal bone fragment. Impingement of the bone on the other structures listed does not result in the skin puckering seen in the clinical photo.
■
The clinical findings of anterior skin puckering with ecchymosis is caused by impingement of the brachialis fascia by the proximal bone fragment. Impingement of the bone on the other structures listed does not result in the skin puckering seen in the clinical photo.
Question 8High Yield
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture. Active older patients who present with a displaced femoral neck fracture should
be treated with total hip arthroplasty (THA).
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture. Incorrect Answers:
Answer 2: Parkinsons dementia presents an increased risk for dislocation and
would make a hemiarthroplasty a more suitable choice.
Answer 3: According to AAOS guidelines, age greater than 80 and low demand status is an indication for hemiarthroplasty
Answer 4: Hepatic encephalopathy would raise concern for the ability to follow hip precautions and presents an increased risk for dislocation. Thus a hemiarthroplasty would be a better choice.
Answer 5: For a young male laborer a closed vs open reduction and internal fixation should be attempted rather than an arthroplasty.
be treated with total hip arthroplasty (THA).
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture. Incorrect Answers:
Answer 2: Parkinsons dementia presents an increased risk for dislocation and
would make a hemiarthroplasty a more suitable choice.
Answer 3: According to AAOS guidelines, age greater than 80 and low demand status is an indication for hemiarthroplasty
Answer 4: Hepatic encephalopathy would raise concern for the ability to follow hip precautions and presents an increased risk for dislocation. Thus a hemiarthroplasty would be a better choice.
Answer 5: For a young male laborer a closed vs open reduction and internal fixation should be attempted rather than an arthroplasty.
Question 9High Yield
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment?
---
---

Explanation
OCD is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help identify the lesion and establish the status of the physes. An MRI scan is useful for assessing the potential for the lesion to heal with nonsurgical treatment. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary for unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular _surface restored whenever possible._
Question 10High Yield
Figure 83 is the CT scan of a 36-year-old man who fell from a roof. Eight hours later at the emergency department he describes low-back pain with numbness and weakness in his bilateral lower extremity. A neurologic examination reveals 2/5 strength in his quadriceps and iliopsoas bilaterally, 2/5 strength in his right anterior tibialis and gastrocsoleus, and 1/5 strength in his left anterior tibialis and gastrocsoleus. Two hours later, strength in his lower extremities has diminished markedly. What is the best next step?

Explanation
Any progressive neurologic deficit requires emergent surgical intervention. Lumbar injuries cannot be reliably reduced with traction. Although IV steroids and management of mean arterial blood pressure are appropriate interventions for injuries in the region of the conus medullaris, steroids are only indicated when given within 8 hours of injury and are not appropriate as a sole means of management for progressive neurologic deficit.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
[Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[View](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15615508)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15615508)
Question 11High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature.
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 12High Yield
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically.
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
Question 13High Yield
A 14-year-old boy suffers a hip dislocation in a motor vehicle accident. It is reduced by closed means. The risk of avascular necrosis is:
Explanation
Avascular necrosis is a risk of traumatic hip dislocation. The risk is closest to 10%.
Question 14High Yield
ORTHOPEDIC MCQS OB 20 BASIC 4
A 64-year-old female with rheumatoid arthritis has decreased functional use of the left hand for activities of daily living. On physical examination she has fixed deformities of the metacarpophalangeal (MCP) joints as demonstrated in Figure A. A radiograph is shown in Figure B. Which of the following management options for the finger MCP joints most likely lead to the least amount of extensor lag and improvement of the ulnar drift at 1-year followup?
A 64-year-old female with rheumatoid arthritis has decreased functional use of the left hand for activities of daily living. On physical examination she has fixed deformities of the metacarpophalangeal (MCP) joints as demonstrated in Figure A. A radiograph is shown in Figure B. Which of the following management options for the finger MCP joints most likely lead to the least amount of extensor lag and improvement of the ulnar drift at 1-year followup?

















Explanation
A Bonferroni correction is a post-hoc statistical correction made to P values when several dependent or independent statistical tests are being performed simultaneously on a single data set.
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect Answers:
: This describes Bayesian analysis. Answer 2: This describes Hawthorne effect. Answer 3: This describes Pearson correlation. Answer 5: This describes Study power.
A 10-year-old child falls from a standing height and sustains the injury shown in Figure A. Her medical history includes hearing defects and the facial appearance shown in Figure B. In addition to operative fixation of her fracture she is scheduled to receive cyclical intravenous**
**pamidronate administration as a treatment after the fracture is healed. Which of the following is associated with this form of treatment?
1) No change in bone pain
2) No change in future fracture incidence
3) An increase in osteoblast density
4) An increased risk of secondary osteosarcoma
5) An increase in bone density
The history and images are consistent with osteogenesis imperfecta (OI). Olecranon avulsion fractures are often seen in patients with OI and children presenting with these should be evaluated for OI. The clinical image of blue sclera can also be a characteristic finding in patients with OI. The Bisphosphonates have been shown to decrease fracture incidence and bone pain while improving bone density and overall function in OI patients.
Zeitlin et al performed a Level 5 review of OI. They state that Sillence Types I through IV are a mutation in the COL1A1 and COL1A2 genes that encode type I collagen. They report that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence, and increases bone density and
level of ambulation.
Burnei et al also performed a Level 5 review of OI. They report that the use of bone marrow transplantation to increase osteoblast density in OI patients is currently being
researched as a potential treatment of OI.
A 35-year-old male presents with pain and limited range of motion 3 months after arthroscopic Bankart repair of his right shoulder. His postoperative course included a continuous intra- articular infusion pump for 3 days, use of a sling for 4 weeks, and initiation of passive range of motion below the level of the shoulder. At 4 weeks postoperatively he started active range of motion exercises, and started an isotonic strengthening program at the 9 week interval. Which of the following options is the MOST appropriate step in his management?
1) Reassurance and appropriate followup
2) Focused physical therapy on aggressive ROM exercises and modalities
3) Intra-articular injection of corticosteroids to decrease post-operative inflammation
4) Shoulder radiograph series to assess for chondrolysis
5) Arthroscopic vs open Bankart revision surgery for failed repair
The above patient was issued an intra-articular infusion of lidocaine for pain control after his surgery and may have developed shoulder chondrolysis. This complication after the use of intra-articular pumps has recently become more well known. The U.S. Federal drug and Administration (FDA) has issued a warning on the adminstration of continuous intra-articular infusion of local anesthestics for pain control.
The FDA has reviewed 35 cases of patients developing chondrolysis after intra- articular infusions, some being as early as 2 months after their surgery. The average time of diagnosis in these cases with chondrolysis were at an average of 8.5 months after the infusion. The majority of the reported cases occurred following shoulder surgeries. Joint pain, stiffness, and loss of motion were the most common physical complaints. As a result of their findings, the FDA issued
a warning for surgeons to be aware and monitor for signs and symptoms of chondrolysis.
Illustration A shows a radiograph consistent with chondrolysis in a patient status post arthroscopic Bankart repair. This image shows the loss of joint height in the glenohumeral joint due to chondrolysis. Also, 2 suture anchors are visible as well in the glenoid from the Bankart repair. Illustration B shows an arthroscopic image of chondrolysis and Illustrations C and D demonstrate chondrolyis viewed from an open approach.
Regarding bone densitometry, a T-score of -3.5 is defined as which of the following?
1) Normal bone
2) Osteopenia
3) Age appropriate bone loss
4) Osteoporosis
5) None. One cannot make this diagnosis without further information.
A T-score of -3.5 is defined as osteoporosis, regardless of the other clinical factors.
As described in the review by Kanis et al., the World Health Organization (WHO) has defined the following categories based on bone density in white women:
Normal bone: T-score greater than -1 Osteopenia: T-score between -1 and -2.5 Osteoporosis: T-score less than -2.5
The WHO committee did not have enough data to create definitions for men or other ethnic groups. T-score is a comparison of a patient's BMD to that of a healthy thirty-year- old of the same sex and ethnicity. Z-score is the number of standard deviations a patient's BMD differs from the average BMD of their age, sex, and ethnicity.
A 67-year-old female presented 2 months ago to her primary care physician with left sided thigh pain. A radiograph was taken at that time and is shown in Figure A. She was diagnosed at that time with a quadriceps strain and given a prescription for ibuprofen and physical therapy. She is now in the emergency room with severe left thigh pain and inability to bear weight on the left lower extremity after bending down to tie her shoes. She denies any constitutional symptoms. A current radiograph from the emergency room is shown in Figure B. Which of the following most likely explains this patient's fracture?
1) Long-term corticosteroid use
2) Secondary malignancy arising from Paget disease
3) Long-term alendronate use
4) Long-term ergocalciferol use
5) Short-term teraparatide use
Subtrochanteric stress reaction (Figure A) and low-energy transverse fracture (Figure B) is a complication of long-term bisphosphonate use documented in the literature. Of note, a healed right sided subtrochanteric femur fracture is also visualized in Figure A.
Neviaser et al conducted a Level 4 study of 70 patients with low energy femur fractures. They found that a simple, transverse pattern and hypertrophy of the diaphyseal cortex are associated with alendronate use with 98% specificity. They report that the average alendronate usage time was 6.9 years in patients exhibiting this pattern of fracture.
Capeci et al performed a Level 4 review of alendronate therapy and its association with unilateral low-energy subtrochanteric and diaphyseal femur fractures. They recommended consideration of discontinuing alendronate with the consultation of an endocrinologist if a fracture occurs. They also recommend routine contralateral leg surveillance after to rule out contralateral stress fracture. If contralateral stress fracture is found, it it is recommended that it is treated with prophylactic intramedullary fixation.
Imaging typically shows lateral cortical thickening in the subtrochanteric femur as demonstrating on the coronal and axial CT scans shown in Illustration A and B, respectively.
In the study by Moseley et al published in the New England Journal of Medicine, 180 patients with knee osteoarthritis were randomly assigned via sealed envelope to receive arthroscopic débridement, arthroscopic lavage, or placebo surgery. Outcomes were assessed by blinded evaluators at several points over a 2 year period**
**with the use of five self-reported pain and function scores. There was a greater than 90% follow-up in the study. This study is best described as having which level of evidence?
1) Therapeutic study, evidence level I
2) Therapeutic study, evidence level II
3) Diagnostic study, evidence level I
4) Diagnostic study, evidence level II
5) Prognostic study, evidence level I
Therapeutic studies investigate the results of treatment. Level 1 evidence includes randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence interval.
A level II therapeutic study would include a lesser-quality randomized controlled trial (eg,
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
1) Per-protocol
2) Crossover analysis
3) Intent-to-treat
4) Bayesian analysis
5) Effect size
The following is an example of intent-to-treat analysis.
The intent-to-treat approach aims to keep similar groups similar by not
allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per- protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
Answer 1: Per-protocol- excludes patients who were not compliant with the protocol
guidelines
Answer 2: Crossover studies involve switching patients between different arms of the study.
Answer 4: Bayesian analysis— An analysis that starts with a particular probability of an event (the prior probability) and incorporates new information to generate a revised probability (a posterior probability).
Answer 5: Effect size— The difference in outcome between the intervention group and the control group divided by some measure of the variability, typically the standard deviation.
A 32-year-old male is being seen in your office for evaluation of a possible rotator cuff tear. He has been seen in your office by one of**
**your partners previously after surgical treatment of a femoral shaft fracture. How much time has to pass since last evaluation or treatment in your group for this patient to revert to a new patient under CPT guidelines?
1) 6 months
2) 1 year
3) 18 months
4) 2 years
5) 3 years
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.” By contrast, an established patient has received professional services from the physician or another physician in the same group and the same specialty within the prior three years.
The referenced study by Shalowitz reviewed 500 Medicare claims and found an overall coding error rate of 32.4%, with high levels of consultation coding errors. He reports that changing ambulatory consultation codes to those for new patient visits would save Medicare $534.5 million per year.
As a result of this study, as well as others, Medicare does not recognize consultation codes.
A 55-year-old healthy female presents for a routine physical exam. When discussing bone health and osteoporosis prevention, what dose of calcium and vitamin D should be recommended for daily consumption?
1) 1,500mg of calcium and 1,000 IUs of vitamin D
2) 2,200mg of calcium and 1,000 IUs of vitamin D
3) 750mg of calcium and 5,000 IUs of vitamin D
4) 750mg of calcium and 10,000 IUs of vitamin D
5) 2,200mg of calcium and 5,000 IUs of vitamin D
The National Osteoporosis Foundation recommends a daily intake of 1,200- 1500mg of calcium 800-1,000 IUs of vitamin D for adults over the age of 50.
The review article by Gehrig et al discusses the factors surrounding osteoporosis that can be modified to optimize fracture risk reduction. They report that non-prescription interventions such as calcium and vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs are treatment options.
What is the function of the core binding factor alpha-1 (Cbfa1/Runx2)?
1) Phosphorylation and intracellular activation of signal transducers and activators of transcription (STATs)
2) Chemotaxis of mesenchymal stem cells to sites of skeletal fractures
3) Tumor-induced osteolysis
4) Osteoclastic apoptosis
5) Osteoblastic differentiation
As described by Ducy et al., Cbfa1/Runx2 is a key transcription factor associated with osteoblast differentiation, skeletal morphogenesis, and acts as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression. A stop codon mutation in the Cbfa 1 gene causes cleidocranial dysplasia. Stem cell chemotaxis (moving to various sites in the body) is accomplished through a variety of cytokines, one of which is platelet derived growth factor. Tumor-induced osteolysis occurs secondary to tumor-produced cytokine activation of osteoclasts. Osteoclastic apoptosis occurs secondary to bisphosphonates.
Ballock and O'Keefe review the development, growth, and complex cytokine interaction required for normal growth plate function.
A 20-year-old male is involved in motor vehicle collision and sustains a depressed tibial plateau fracture. When performing surgery, if calcium sulfate is used as the primary bone substitute void filler, an increase in which of the following outcomes may be expected as compared to autograft?
1) Increased complications due to serous drainage
2) Improved clinical outcomes as shown by more rapid time to healing
3) Improved clinical outcomes as shown by SF-36 scores
4) Increased complications due to autoimmune reactions and graft rejection
5) Equivalent complication rates and clinical outcomes
Calcium sulfate bone graft substitute has demonstrated an increased rate of serous drainage at the surgical site. Evidence examining the use of calcium sulfate in the treatment of bone nonunions revealed a significant failure rate, suggesting that this material, used in isolation, is not optimal to promote union in that setting.
Beuerlein and Mckee reviewed the literature, showing that calcium sulfate is
an effective void filler in metaphyseal defects after impacted fracture reduction (calcaneus, tibial plateau) or simple bone cysts. However, they report that calcium sulfate is associated with serous wound drainage especially when used at subcutaneous sites and in amounts greater than 20ml.
Ziran et al present a series of 41 patients undergoing bone grafting for atrophic/avascular nonunions with adjunctive calcium sulfate-demineralized bone matrix (Allomatrix). Of the 41 patients, 13 (32%) had drainage that necessitated surgical procedures and 14 (34%) developed a deep infection.
A 46-year-old female begins to have personality changes, cognitive decline, and chorea. Her father began having similar but less severe symptoms at age 55 before passing away 6 years later. One of her 2 older siblings has also begun to show deterioration. Which of the following describes the hereditary pattern of this disease?
1) Autosomal dominant with variable penetrance
2) Autosomal recessive with variable penetrance
3) X-linked recessive
4) Autosomal dominant with anticipation
5) Autosomal dominant with imprinting
This clinical vignette describes a patient with Huntington's disease. Huntington's disease has an autosomal dominant hereditary pattern with anticipation.
Anticipation is a term used to describe trinucleotide repeat
disorders that if passed on, will present earlier and more severely in affected subjects than in their affected parent. In Huntington's disease, it is due to a "CAG" trinucleotide repeat on chromosome 4. Subjects with an affected parent have a 50% chance of inheriting the disease from them, and if present will have more severe disease.
Deighton et al provide a review on the genetics of musculoskeletal disease including the hereditary pattern of anticipation.
All of the following are indications for locked plating technology EXCEPT:
1) Periarticular fracture with metaphyseal comminution
2) Fracture in osteoporotic bone
3) Bridge plating for severely comminuted fractures
4) Compression plating of transverse fracture
5) Plating of fractures where anatomical constraints prevent plating on the tension side of the bone
Locked plates are indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone.
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Approaches to internal fixation have become more biologic. Greater emphasis is placed on vascularity and soft tissue integrity. Locked plates, analogous to rigid internal fixators, can provide relative stability favorable to secondary fracture healing. If applied appropriately, they can
avoid soft tissue compromise. The key to this new generation of plates is the locking mechanism of the screw to the plate, which provides angular stability and avoids compression of the plate to the periosteum. Favorable biomechanical and clinical results continue to expand the number of appropriate indications for use of locked plating devices, although exact indications for their use have yet to be precisely defined.
The referenced articles by Haidukewych and Egol et al are reviews of the biomechanical characteristics of locked plating technology.
Which of the following lists these materials in order of increasing modulus of elasticity?:
1) Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
2) Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
3) Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
4) Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
5) Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Answers 1, 2, 4, 5: Cortical bone is the least stiff of the materials listed. Ceramic is the stiffest. The intermediate materials listed are in the relative order listed in answer 3.
Which of the following substances increases the chondrogenic phenotype of intervertebral disk cells and matrix synthesis?
1) Osteoprotegrin
2) Osteonectin
3) Hyperosmotic saline
4) Corticosteroids
5) Bone morphogenic proteins
Bone morphogenic proteins have been shown to increase chondrogenic phenotype expression and increase matrix synthesis of the intervertebral disc in animal studies.
Bone morphogenetic protein-2, bone morphogenetic protein-7, and
transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of the disk matrix. Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
Miyamoto et al. evaluated rabbits that underwent annulus fibrosus (AF) injury where they either injected a control or BMP into the nucleus pulposus. The BMP injection significantly restored disc height and improved the modulus as compared to control injections. They concluded the biochemical data suggested that the OP-1-induced restoration of the disc space was a consequence of the increased activity of anabolic pathways that resulted in biochemical changes in the IVD.
Kim et al. evaluated mRNA levels of BMP-2, BMP-7, and TGF-beta in a rabbit model of intervertebral discs. Compared to young rabbits, old rabbits generally had higher levels of mRNA expression of these three cytokines in both the annulus fibrosus and nucleus pulposus. The similar patterns of up-regulation in gene expression with age shown by these 3 anabolic cytokines suggest a common pathway in terms of regulation and transcription in the early stage of disc degeneration.
Incorrect Answers:
Answer 1: Osteoprotegrin function to limit the activity of RANKL, thus promoting net osteoblast activity and increased bone formation.
Answer 2: Osteonectin is secreted by platelets and osteoblasts and functions to regulate calcium and organizing mineral in the bone matrix.
Answer 3: Hyperosmotic saline has not demonstrated to have an effect on gene expression in intervertebral discs.
Answer 4: Corticosteroids have not been found to promote gene expression of BMP cytokines and promote matrix synthesis in intervertebral discs. Generally, corticosteroids are catabolic hormones that would likely have an inverse reaction on biochemical activities of the intervertebral disc than BMP.
A colleague is struggling to obtain a perfect lateral radiograph for distal locking screw placement. Other than good technique, how might the surgeon best reduce the amount of radiation exposure to the patient and personnel when using fluoroscopy?
1) The use of continuous fluoroscopy while manipulating the leg
2) Standing directly behind the cathode ray tube
3) Advising the technician to position the fluoroscopy beam on command
4) Placement of the image intensifier receptor as close to the patient as possible
5) Placement of the cathode ray tube as close to the patient as possible
**
Placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Numerous steps have been described to decrease radiation in the operating room. They include:
A Bonferroni correction is a post-hoc statistical correction made to P values when several dependent or independent statistical tests are being performed simultaneously on a single data set.
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect Answers:
: This describes Bayesian analysis. Answer 2: This describes Hawthorne effect. Answer 3: This describes Pearson correlation. Answer 5: This describes Study power.
A 10-year-old child falls from a standing height and sustains the injury shown in Figure A. Her medical history includes hearing defects and the facial appearance shown in Figure B. In addition to operative fixation of her fracture she is scheduled to receive cyclical intravenous**
**pamidronate administration as a treatment after the fracture is healed. Which of the following is associated with this form of treatment?
1) No change in bone pain
2) No change in future fracture incidence
3) An increase in osteoblast density
4) An increased risk of secondary osteosarcoma
5) An increase in bone density
The history and images are consistent with osteogenesis imperfecta (OI). Olecranon avulsion fractures are often seen in patients with OI and children presenting with these should be evaluated for OI. The clinical image of blue sclera can also be a characteristic finding in patients with OI. The Bisphosphonates have been shown to decrease fracture incidence and bone pain while improving bone density and overall function in OI patients.
Zeitlin et al performed a Level 5 review of OI. They state that Sillence Types I through IV are a mutation in the COL1A1 and COL1A2 genes that encode type I collagen. They report that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence, and increases bone density and
level of ambulation.
Burnei et al also performed a Level 5 review of OI. They report that the use of bone marrow transplantation to increase osteoblast density in OI patients is currently being
researched as a potential treatment of OI.
A 35-year-old male presents with pain and limited range of motion 3 months after arthroscopic Bankart repair of his right shoulder. His postoperative course included a continuous intra- articular infusion pump for 3 days, use of a sling for 4 weeks, and initiation of passive range of motion below the level of the shoulder. At 4 weeks postoperatively he started active range of motion exercises, and started an isotonic strengthening program at the 9 week interval. Which of the following options is the MOST appropriate step in his management?
1) Reassurance and appropriate followup
2) Focused physical therapy on aggressive ROM exercises and modalities
3) Intra-articular injection of corticosteroids to decrease post-operative inflammation
4) Shoulder radiograph series to assess for chondrolysis
5) Arthroscopic vs open Bankart revision surgery for failed repair
The above patient was issued an intra-articular infusion of lidocaine for pain control after his surgery and may have developed shoulder chondrolysis. This complication after the use of intra-articular pumps has recently become more well known. The U.S. Federal drug and Administration (FDA) has issued a warning on the adminstration of continuous intra-articular infusion of local anesthestics for pain control.
The FDA has reviewed 35 cases of patients developing chondrolysis after intra- articular infusions, some being as early as 2 months after their surgery. The average time of diagnosis in these cases with chondrolysis were at an average of 8.5 months after the infusion. The majority of the reported cases occurred following shoulder surgeries. Joint pain, stiffness, and loss of motion were the most common physical complaints. As a result of their findings, the FDA issued
a warning for surgeons to be aware and monitor for signs and symptoms of chondrolysis.
Illustration A shows a radiograph consistent with chondrolysis in a patient status post arthroscopic Bankart repair. This image shows the loss of joint height in the glenohumeral joint due to chondrolysis. Also, 2 suture anchors are visible as well in the glenoid from the Bankart repair. Illustration B shows an arthroscopic image of chondrolysis and Illustrations C and D demonstrate chondrolyis viewed from an open approach.
Regarding bone densitometry, a T-score of -3.5 is defined as which of the following?
1) Normal bone
2) Osteopenia
3) Age appropriate bone loss
4) Osteoporosis
5) None. One cannot make this diagnosis without further information.
A T-score of -3.5 is defined as osteoporosis, regardless of the other clinical factors.
As described in the review by Kanis et al., the World Health Organization (WHO) has defined the following categories based on bone density in white women:
Normal bone: T-score greater than -1 Osteopenia: T-score between -1 and -2.5 Osteoporosis: T-score less than -2.5
The WHO committee did not have enough data to create definitions for men or other ethnic groups. T-score is a comparison of a patient's BMD to that of a healthy thirty-year- old of the same sex and ethnicity. Z-score is the number of standard deviations a patient's BMD differs from the average BMD of their age, sex, and ethnicity.
A 67-year-old female presented 2 months ago to her primary care physician with left sided thigh pain. A radiograph was taken at that time and is shown in Figure A. She was diagnosed at that time with a quadriceps strain and given a prescription for ibuprofen and physical therapy. She is now in the emergency room with severe left thigh pain and inability to bear weight on the left lower extremity after bending down to tie her shoes. She denies any constitutional symptoms. A current radiograph from the emergency room is shown in Figure B. Which of the following most likely explains this patient's fracture?
1) Long-term corticosteroid use
2) Secondary malignancy arising from Paget disease
3) Long-term alendronate use
4) Long-term ergocalciferol use
5) Short-term teraparatide use
Subtrochanteric stress reaction (Figure A) and low-energy transverse fracture (Figure B) is a complication of long-term bisphosphonate use documented in the literature. Of note, a healed right sided subtrochanteric femur fracture is also visualized in Figure A.
Neviaser et al conducted a Level 4 study of 70 patients with low energy femur fractures. They found that a simple, transverse pattern and hypertrophy of the diaphyseal cortex are associated with alendronate use with 98% specificity. They report that the average alendronate usage time was 6.9 years in patients exhibiting this pattern of fracture.
Capeci et al performed a Level 4 review of alendronate therapy and its association with unilateral low-energy subtrochanteric and diaphyseal femur fractures. They recommended consideration of discontinuing alendronate with the consultation of an endocrinologist if a fracture occurs. They also recommend routine contralateral leg surveillance after to rule out contralateral stress fracture. If contralateral stress fracture is found, it it is recommended that it is treated with prophylactic intramedullary fixation.
Imaging typically shows lateral cortical thickening in the subtrochanteric femur as demonstrating on the coronal and axial CT scans shown in Illustration A and B, respectively.
In the study by Moseley et al published in the New England Journal of Medicine, 180 patients with knee osteoarthritis were randomly assigned via sealed envelope to receive arthroscopic débridement, arthroscopic lavage, or placebo surgery. Outcomes were assessed by blinded evaluators at several points over a 2 year period**
**with the use of five self-reported pain and function scores. There was a greater than 90% follow-up in the study. This study is best described as having which level of evidence?
1) Therapeutic study, evidence level I
2) Therapeutic study, evidence level II
3) Diagnostic study, evidence level I
4) Diagnostic study, evidence level II
5) Prognostic study, evidence level I
Therapeutic studies investigate the results of treatment. Level 1 evidence includes randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence interval.
A level II therapeutic study would include a lesser-quality randomized controlled trial (eg,
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
1) Per-protocol
2) Crossover analysis
3) Intent-to-treat
4) Bayesian analysis
5) Effect size
The following is an example of intent-to-treat analysis.
The intent-to-treat approach aims to keep similar groups similar by not
allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per- protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
Answer 1: Per-protocol- excludes patients who were not compliant with the protocol
guidelines
Answer 2: Crossover studies involve switching patients between different arms of the study.
Answer 4: Bayesian analysis— An analysis that starts with a particular probability of an event (the prior probability) and incorporates new information to generate a revised probability (a posterior probability).
Answer 5: Effect size— The difference in outcome between the intervention group and the control group divided by some measure of the variability, typically the standard deviation.
A 32-year-old male is being seen in your office for evaluation of a possible rotator cuff tear. He has been seen in your office by one of**
**your partners previously after surgical treatment of a femoral shaft fracture. How much time has to pass since last evaluation or treatment in your group for this patient to revert to a new patient under CPT guidelines?
1) 6 months
2) 1 year
3) 18 months
4) 2 years
5) 3 years
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.” By contrast, an established patient has received professional services from the physician or another physician in the same group and the same specialty within the prior three years.
The referenced study by Shalowitz reviewed 500 Medicare claims and found an overall coding error rate of 32.4%, with high levels of consultation coding errors. He reports that changing ambulatory consultation codes to those for new patient visits would save Medicare $534.5 million per year.
As a result of this study, as well as others, Medicare does not recognize consultation codes.
A 55-year-old healthy female presents for a routine physical exam. When discussing bone health and osteoporosis prevention, what dose of calcium and vitamin D should be recommended for daily consumption?
1) 1,500mg of calcium and 1,000 IUs of vitamin D
2) 2,200mg of calcium and 1,000 IUs of vitamin D
3) 750mg of calcium and 5,000 IUs of vitamin D
4) 750mg of calcium and 10,000 IUs of vitamin D
5) 2,200mg of calcium and 5,000 IUs of vitamin D
The National Osteoporosis Foundation recommends a daily intake of 1,200- 1500mg of calcium 800-1,000 IUs of vitamin D for adults over the age of 50.
The review article by Gehrig et al discusses the factors surrounding osteoporosis that can be modified to optimize fracture risk reduction. They report that non-prescription interventions such as calcium and vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs are treatment options.
What is the function of the core binding factor alpha-1 (Cbfa1/Runx2)?
1) Phosphorylation and intracellular activation of signal transducers and activators of transcription (STATs)
2) Chemotaxis of mesenchymal stem cells to sites of skeletal fractures
3) Tumor-induced osteolysis
4) Osteoclastic apoptosis
5) Osteoblastic differentiation
As described by Ducy et al., Cbfa1/Runx2 is a key transcription factor associated with osteoblast differentiation, skeletal morphogenesis, and acts as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression. A stop codon mutation in the Cbfa 1 gene causes cleidocranial dysplasia. Stem cell chemotaxis (moving to various sites in the body) is accomplished through a variety of cytokines, one of which is platelet derived growth factor. Tumor-induced osteolysis occurs secondary to tumor-produced cytokine activation of osteoclasts. Osteoclastic apoptosis occurs secondary to bisphosphonates.
Ballock and O'Keefe review the development, growth, and complex cytokine interaction required for normal growth plate function.
A 20-year-old male is involved in motor vehicle collision and sustains a depressed tibial plateau fracture. When performing surgery, if calcium sulfate is used as the primary bone substitute void filler, an increase in which of the following outcomes may be expected as compared to autograft?
1) Increased complications due to serous drainage
2) Improved clinical outcomes as shown by more rapid time to healing
3) Improved clinical outcomes as shown by SF-36 scores
4) Increased complications due to autoimmune reactions and graft rejection
5) Equivalent complication rates and clinical outcomes
Calcium sulfate bone graft substitute has demonstrated an increased rate of serous drainage at the surgical site. Evidence examining the use of calcium sulfate in the treatment of bone nonunions revealed a significant failure rate, suggesting that this material, used in isolation, is not optimal to promote union in that setting.
Beuerlein and Mckee reviewed the literature, showing that calcium sulfate is
an effective void filler in metaphyseal defects after impacted fracture reduction (calcaneus, tibial plateau) or simple bone cysts. However, they report that calcium sulfate is associated with serous wound drainage especially when used at subcutaneous sites and in amounts greater than 20ml.
Ziran et al present a series of 41 patients undergoing bone grafting for atrophic/avascular nonunions with adjunctive calcium sulfate-demineralized bone matrix (Allomatrix). Of the 41 patients, 13 (32%) had drainage that necessitated surgical procedures and 14 (34%) developed a deep infection.
A 46-year-old female begins to have personality changes, cognitive decline, and chorea. Her father began having similar but less severe symptoms at age 55 before passing away 6 years later. One of her 2 older siblings has also begun to show deterioration. Which of the following describes the hereditary pattern of this disease?
1) Autosomal dominant with variable penetrance
2) Autosomal recessive with variable penetrance
3) X-linked recessive
4) Autosomal dominant with anticipation
5) Autosomal dominant with imprinting
This clinical vignette describes a patient with Huntington's disease. Huntington's disease has an autosomal dominant hereditary pattern with anticipation.
Anticipation is a term used to describe trinucleotide repeat
disorders that if passed on, will present earlier and more severely in affected subjects than in their affected parent. In Huntington's disease, it is due to a "CAG" trinucleotide repeat on chromosome 4. Subjects with an affected parent have a 50% chance of inheriting the disease from them, and if present will have more severe disease.
Deighton et al provide a review on the genetics of musculoskeletal disease including the hereditary pattern of anticipation.
All of the following are indications for locked plating technology EXCEPT:
1) Periarticular fracture with metaphyseal comminution
2) Fracture in osteoporotic bone
3) Bridge plating for severely comminuted fractures
4) Compression plating of transverse fracture
5) Plating of fractures where anatomical constraints prevent plating on the tension side of the bone
Locked plates are indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone.
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Approaches to internal fixation have become more biologic. Greater emphasis is placed on vascularity and soft tissue integrity. Locked plates, analogous to rigid internal fixators, can provide relative stability favorable to secondary fracture healing. If applied appropriately, they can
avoid soft tissue compromise. The key to this new generation of plates is the locking mechanism of the screw to the plate, which provides angular stability and avoids compression of the plate to the periosteum. Favorable biomechanical and clinical results continue to expand the number of appropriate indications for use of locked plating devices, although exact indications for their use have yet to be precisely defined.
The referenced articles by Haidukewych and Egol et al are reviews of the biomechanical characteristics of locked plating technology.
Which of the following lists these materials in order of increasing modulus of elasticity?:
1) Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
2) Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
3) Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
4) Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
5) Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Answers 1, 2, 4, 5: Cortical bone is the least stiff of the materials listed. Ceramic is the stiffest. The intermediate materials listed are in the relative order listed in answer 3.
Which of the following substances increases the chondrogenic phenotype of intervertebral disk cells and matrix synthesis?
1) Osteoprotegrin
2) Osteonectin
3) Hyperosmotic saline
4) Corticosteroids
5) Bone morphogenic proteins
Bone morphogenic proteins have been shown to increase chondrogenic phenotype expression and increase matrix synthesis of the intervertebral disc in animal studies.
Bone morphogenetic protein-2, bone morphogenetic protein-7, and
transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of the disk matrix. Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
Miyamoto et al. evaluated rabbits that underwent annulus fibrosus (AF) injury where they either injected a control or BMP into the nucleus pulposus. The BMP injection significantly restored disc height and improved the modulus as compared to control injections. They concluded the biochemical data suggested that the OP-1-induced restoration of the disc space was a consequence of the increased activity of anabolic pathways that resulted in biochemical changes in the IVD.
Kim et al. evaluated mRNA levels of BMP-2, BMP-7, and TGF-beta in a rabbit model of intervertebral discs. Compared to young rabbits, old rabbits generally had higher levels of mRNA expression of these three cytokines in both the annulus fibrosus and nucleus pulposus. The similar patterns of up-regulation in gene expression with age shown by these 3 anabolic cytokines suggest a common pathway in terms of regulation and transcription in the early stage of disc degeneration.
Incorrect Answers:
Answer 1: Osteoprotegrin function to limit the activity of RANKL, thus promoting net osteoblast activity and increased bone formation.
Answer 2: Osteonectin is secreted by platelets and osteoblasts and functions to regulate calcium and organizing mineral in the bone matrix.
Answer 3: Hyperosmotic saline has not demonstrated to have an effect on gene expression in intervertebral discs.
Answer 4: Corticosteroids have not been found to promote gene expression of BMP cytokines and promote matrix synthesis in intervertebral discs. Generally, corticosteroids are catabolic hormones that would likely have an inverse reaction on biochemical activities of the intervertebral disc than BMP.
A colleague is struggling to obtain a perfect lateral radiograph for distal locking screw placement. Other than good technique, how might the surgeon best reduce the amount of radiation exposure to the patient and personnel when using fluoroscopy?
1) The use of continuous fluoroscopy while manipulating the leg
2) Standing directly behind the cathode ray tube
3) Advising the technician to position the fluoroscopy beam on command
4) Placement of the image intensifier receptor as close to the patient as possible
5) Placement of the cathode ray tube as close to the patient as possible
**
Placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Numerous steps have been described to decrease radiation in the operating room. They include:
Question 15High Yield
Figures 1 and 2 show the radiograph and CT obtained from a 78-year-old woman who underwent right
total hip replacement in 1995. She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 0.5 mg/L, a serum cobalt level of 0.4 µg/L, and a serum chromium level of 0.6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
total hip replacement in 1995. She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 0.5 mg/L, a serum cobalt level of 0.4 µg/L, and a serum chromium level of 0.6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?

Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 16High Yield
ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D
In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?
In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?








































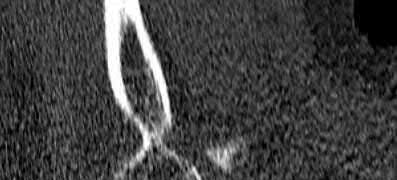
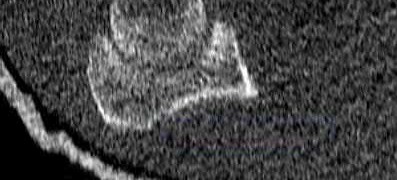
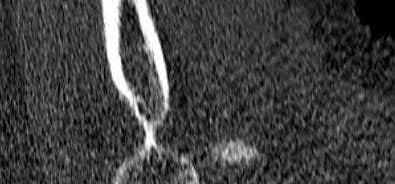
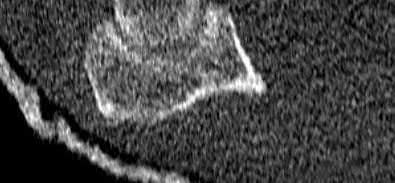
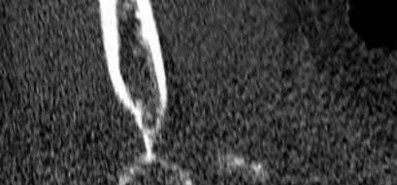
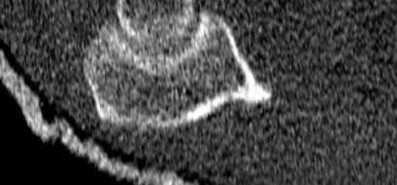
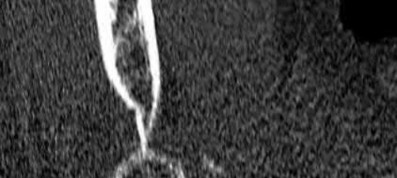
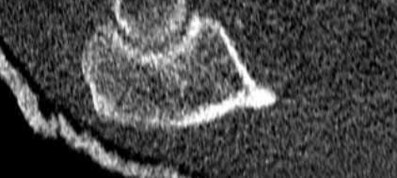







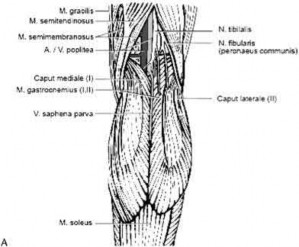
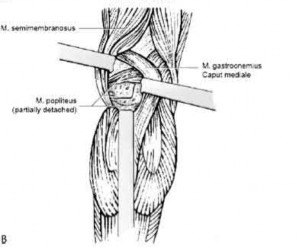


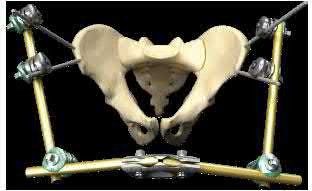




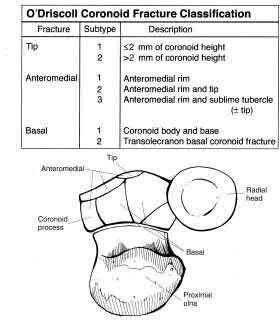
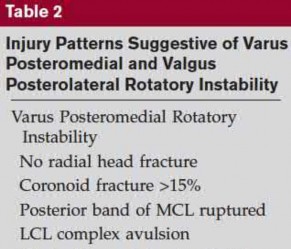





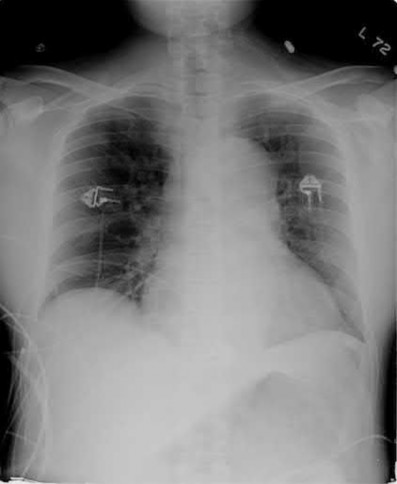





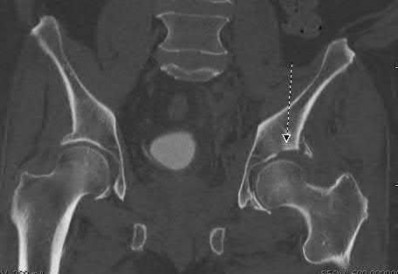

Explanation
Reamed exchange nailing is recommended for the management of aseptic nonunions of noncomminuted tibial shaft fractures. Union rates have been reported between 76-96% in large studies.
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
, 2: Exchange nailing has not produced good results following failures of intramedullary nail fixation of humeral shaft fractures. Union rates have been shown between 30-40%,
Answer 3: There is little evidence to support exchange nailing for distal femoral nonunions. Union rates have been shown at 50-60%.
Answer 4: Nonunions following comminuted fractures do not appear to respond
to exchange nailing. Union rates have been reported as 45-80%.
Figures A to C show radiographs of a 70 year-old male who fell on the ice 5 days ago. He could initially walk after the fall, but he is now unable to weight-bear on the leg due to pain. Physical examination shows diffuse ankle swelling, with no medial sided ankle tenderness. He is neurovascularly intact. The patient does not smoke and has no medical history. A gravity stress radiograph is demonstrated in Figure
D. After closed reduction, there is 2 mm of fracture displacement, no talar shift and the talocrural angle = 83 degrees. What is the most appropriate treatment?
1) Total contact casting, non-weightbearing, for 6-8 weeks.
2) MRI to better evaluate the deep deltoid ligament
3) Open reduction and internal fixation
4) CT scan to better identify the fracture pattern
5) Below knee splint for 2-4 weeks and advance to weight-bearing as tolerated in an immobilizer boot
The patient has a 5 day old Weber B fibula fracture with a well reduced mortise and stress radiograph that demonstrates no instability of the mortise. The appropriate treatment would be a period of immobilization followed by advanced weight-bearing as tolerated.
The patient has an isolated lateral malleolus fracture. These fracture are stable if the deltoid ligament is intact, and unstable if the deltoid ligament is disrupted. The competency of the deltoid ligament can be evaluated with a stress radiograph which is completed by placing the ankle in maximum dorsiflexion and 15° of internal rotation while an external rotation force is applied to the foot. A stress radiograph (manual or gravity assisted) is positive if there is subluxation of the talus during the exam. The presence of tenderness or swelling medially at the ankle has been shown to be a poor indicator of medial-sided injury. The clinical utility of MRI scans in ankle fractures is controversial.
Koval et al. reported on 21 patients with 5-8 mm of clear space widening on stress radiographs after an isolated Weber B lateral malleolus fracture. They performed MRI's of all ankles and found 90% had at least a partially intact deep deltoid. The patients with a partially intact deep deltoid were treated with weight-bearing as tolerated in a removable boot. 14/15 patients that were available for one year follow-up had an AOFAS score of 100.
Egol et al. reported on the treatment of 30 patients with an isolated fibula fracture and a stress XR with over 4mm of clear space widening, but no signs of medial injury such as tenderness, ecchymosis, or swelling around the medial malleolus on physical exam. Twenty patients were treated without surgery, and 10 patients were treated with surgery. The average AOFAS score was similar in both groups at final follow up.
Figure A demonstrates an AP radiograph of a Weber B fibula fracture with minimal medial clear space widening.
Figure B demonstrates a mortise radiograph of a Weber B fibula fracture with a congruent mortise.
Figure C demonstrates a lateral radiograph of a Weber B fibula fracture with a congruent mortise.
Figure D demonstrates a stress radiograph with minimal medial clear space widening.
Incorrect Answers:
Answer 1: Total contact cast (TCC) is an effective treatment in neuropathic, noninfected, and nonischemic foot ulcers. There is no indication for TCC in this
patient.
Answer 2: The clinical utility of MRI scans in ankle fractures is controversial. Answer 3: The patient has a stable ankle fracture. The post-reduction parameters are within normal limits - intact mortise, no talar shift,
A 44-year-old male presents after being struck by a car. He is hypotensive, and has an obvious open tibia and a closed femoral shaft fracture. A pelvic radiograph is obtained and shown in Figure A. A representative CT scan image in shown in Figure B. The patient is placed in a pelvic binder, and his blood pressure normalizes with crystalloid and a blood transfusion. He then undergoes pelvic angiography, and his internal iliac artery is embolized. Which of the following definitive treatment options is most appropriate in this case?
1) Anterior pelvic external fixation with pins placed in the AIIS and a posterior sacroiliac screw
2) Open reduction and internal fixation of the pubic symphysis with a two hole plate and posterior fixation with a iliosacral screw
3) Open reduction and internal fixation of the pubic symphysis with a nonlocking multi-hole plate and posterior fixation with a iliosacral screw
4) Anterior pelvic external fixation and posterior triangular osteosynthesis
5) Open reduction and internal fixation of the pubic symphysis with a locked multi-hole plate and posterior sacral plate fixation
The radiographs and CT scan show a fracture pattern consistent with an APC-III injury. This is most appropriately treated with pubic symphysis ORIF with a multi-hole plate and posterior iliosacral screw fixation.
APC-III pelvic ring injuries are associated with with disruption of the anterior and posterior SI ligaments (SI dislocation) as well as disruption of
sacrospinous and sacrotuberous ligaments. They are commonly associated with vascular injury and retroperitoneal bleeding.
Sagi et al studied the radiographic and clinical outcome of symphyseal plating techniques, specifically comparing two hole (THP) vs multi-hole plating (MHP). Retrospective review of charts and radiographs immediately after the index procedure to latest follow-up was performed. When comparing the 2 different methods of anterior fixation, they found that the rate of fixation failure was greater in group THP (33%) than group MHP (12%). When evaluating the presence of a malunion as a result of these 2 treatment methods, there were more present in the THP group (57%) than in the MHP group (15%). On the basis of these findings, the authors recommended multi-hole plating of unstable pubic symphyseal disruptions.
Grimshaw et al performed a biomechanical study to determine the failure risk and potential benefit to use of locked fixation constructs in simulated pelvic ring injuries. The authors used a six-hole 3.5-mm plate specifically designed for the symphysis pubis with the capability of fixation in locked or unlocked mode, six pelves were fixed with locked screws and six pelves were fixed standard unlocked bicortical screws. Biomechanical testing was performed, and no abrupt failures were noted. However, locked plating of the pubic symphysis did not appear to offer any advantage over the standard unlocked technique
Illustrations A, B, and C show the AP, outlet, and inlet postoperative radiographs.
Incorrect Answers:
1,4-Anterior pelvic fixation is typically not used as definitive treatment of these injuries unless performed in a damage-control setting. The patient in this case is stable.
2-Multi-hole plate fixation of the pubic symphysis is preferred over 2-hole plate fixation.
5-Posterior sacral plating is not indicated in this fracture pattern, as there is no significant sacral comminution of vertical shear component. Furthermore, no distinct advantage has been found with locked symphyseal plating.
Figure A is a radiograph of an 80-year-old woman who sustained a closed injury to her left arm 10 months ago. She presents to office today complaining of persistent pain in her arm. What is the most likely metabolic or endocrine abnormality contributing to this patients presentation?
1) Vitamin D deficiency
2) Central hypogonadism
3) Thyroid disorder
4) Parathyroid hormone disorder
5) Calcium deficiency
Figure A is a radiograph showing oligotrophic nonunion of a proximal third humeral shaft fracture. The most likely underlying metabolic or endocrine abnormality with this presentation is vitamin D deficiency.
The etiology of fracture nonunion is multifactorial. Predisposing factors include: mechanical instability, poor bone-to-bone contact, infection and biological/biochemical factors. A variety of other contributing factors, such as cigarette smoking and malnutrition, have also been described. Correctable metabolic or endocrine abnormalities are common in elderly patients and are considered contributory in the etiology of fracture non-union. Correction of these abnormalities should be considered prior to surgical fixation.
Brinker et al. studied 37 patients with fracture nonunions with identifiable metabolic or endocrine abnormalities. The distribution of nonunion types at the 46 sites were: oligotrophic (23), atrophic (12), infected (7), and hypertrophic
(4). They showed that 85% of patients had a previously undiagnosed metabolic or endocrine abnormality. The most common newly diagnosed abnormality was vitamin D deficiency in 25 of the 37 patients (68%).
Kuo et al. studied 155 consecutive minimal-trauma fracture subjects for metabolic abnormalities with bone mineral density and laboratory testing. At baseline, only 26% had had proper workup for metabolic abnormalities. After diagnostic work-up, 44% of patients were recommended for anti-resorptive therapy and 56% were recommended calcium/vitamin D medication.
Illustrations A and B show open reduction internal fixation of Figure A with a proximal humeral plate.
Incorrect Answers:
Answer 2: Studies show 15% of fracture nonunions can be attributed to undiagnosed central hypogonadism.
Answer 3: Studies show 24% of fracture nonunions can be attributed to previously established or undiagnosed thyroid disorders
Answer 4: Studies show 11% of fracture nonunions can be attributed to previously established or undiagnosed parathyroid disorders
Answer 5: Studies show 35% of fracture nonunions can be attributed to lack of calcium.
Which of the following fracture patterns is classically associated with varus malunion if treated with closed reduction and casting?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure B shows a midshaft tibia fracture with an intact fibula, which places the fracture at increased risk of varus malalignment during healing.
Nonsurgically treated tibial shaft fractures with an intact fibula have an increased risk of varus malunion when treated nonsurgically. The fibula acts as a strut, preventing valgus collapse, but predisposing to varus angulation. Limb-length discrepancies can also occur.
Teitz et al. found that 26 percent of patients over the ago of 20 years old with isolated tibial shaft fractures treated nonsurgically went on to varus malunion. They also found that when the fibula remains intact, a tibiofibular length discrepancy can develop and cause altered strain patterns in the tibia and fibula leading to later ipsilateral joint sequeale.
Bonnevialle et al performed a retrospective study to assess the outcome after reamed nailing of tibial fractures with an intact fibula. Thirty-eight fractures were evaluated at a minimum of one year from surgery. Healing was achieved after the first intention treatment in 30 patients, after dynamization in 6. A non-union in 2 patients was also successfully managed with new nailing and dynamization. The authors concluded that nailing is a reliable technique for the treatment of tibial fractures with an intact fibula.
Sarmiento et al reviewed 1,000 consecutive closed diaphyseal tibial fractures, treated with prefabricated functional below-knee braces, to determine factors predictive of final fracture outcome. They found that final angulatory deformity in any plane was
A 55-year-old female presents to the emergency room after falling off her balcony. She sustained the isolated, closed injury shown in Figures A and B. She is otherwise healthy, but routinely smokes 30 cigarettes per day. What would be the most appropriate sequence of treatment steps for definitive management of this injury?
1) Closed reduction and splinting followed by delayed casting
2) Immediate open reduction internal fixation
3) Closed reduction and splinting, CT scan, and immediate open reduction internal fixation
4) Closed reduction and splinting, CT scan, external fixation, delayed open reduction internal fixation
5) Closed reduction and splinting, external fixation, CT scan, delayed open reduction internal fixation
Figures A and B show radiographs of a comminuted AO/OTA C3 fracture of the distal tibia. The most appropriate steps in the management of this patients injury would include: Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation in this sequence.
Infection and wound healing problems are common with comminuted distal tibia fractures due to an increased incidence of soft-tissue complications associated with the operative management. Patients with a history of diabetes and smoking are at further risk. To decrease the risk of complications in this patient, a two-staged, delayed open reduction internal fixation technique is the best option for the treatment of severe pilon fractures.
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Re-evaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 82 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
Illustration A shows open reduction internal fixation of the above injury. Incorrect Answers:
Answer 1: Universally, nonoperative treatment of OTA/AO C3 fractures has led
to poor outcomes.
Answer 2,3: Although Ruedi and Allgower (1969) were the first to report successful results with primary open reduction and internal fixation of low-energy fracture patterns, few studies have achieved good results with low soft-tissue complications.
Answer 4: CT scan is most appropriate after frame application. This will allow for distraction and indirect reduction of the fragments to better characterize the fracture pattern for pre-operative planning.
When using a trochanteric femoral nail, placing your start point in which area will result in varus deformity?
1) A
2) B
3) C
4) A and B
5) B and C
Placing your start point lateral to the tip of the greater trochanter (location A) will cause varus deformity.
When using a trochanteric entry femoral nail, the ideal starting point is just medial to the tip of the greater trochanter. Placement lateral to the tip of the trochanter will cause varus malalignment.
Ostrum et al. in a cadaveric study, reported on deformities following medial, standard, and lateral starting points for trochanteric entry femoral nails. Nails inserted too medially yielded excessive valgus, while nails inserted too laterally yielded varus malalignment. Those started at the tip yielded the most neutral alignment, but still with slight varus. The authors recommended a start point just medial to the tip of the greater trochanter.
Figure A exhibits ideal starting point for a trochanteric entry nail (B), for a piriformis start nail (C) and a start point that is too lateral, causing varus (A). Illustration A depicts 4 different types of trochanteric entry nails that started at the tip of the greater trochanter and although mostly neutral, still exhibit slight varus.
Incorrect answers:
Answer 2. Ideal starting point for a trochanteric entry nail resulting in neutral alignment.
Answer 3. Ideal starting point for a piriformis entry nail or valgus in a trochanteric entry nail.
Answer 4. All of the choices will yield different results. Answer 5. The appropriate answer choice is A.
A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and
B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?
1) Absent plantar sensation at presentation
2) Depression at 3 months post-injury
3) Use of an intramedullary nail
4) Free tissue transfer instead of rotational flap
5) Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
Answer 1: Absent plantar sensation does not predict worse outcomes and patients may have significant return of sensation at 2-year follow up.
Answer 3: No difference has been demonstrated with methods of internal fixation for type IIIB tibia shaft fractures.
Answer 4: No difference has been shown with the use of free tissue versus rotational tissue for type IIIB tibia fractures.
Answer 5: The number of debridements has not been shown to influence outcome.
A 45-year-old male is involved in a motorcycle crash. Work-up reveals a closed, right femoral shaft fracture, an open, right tibial shaft fracture, a closed left mid-shaft radius and ulna fractures, and a closed left femoral shaft fracture. His heart rate is 115bpm with a systolic blood pressure of 105mmHg. Initial hematocrit values are reported at
31.5 g/dL and his base deficit is 10mEq/L. What is the most appropriate next step in management?
1) Reamed intramedullary nailing bilateral femur fractures, irrigation and debridement followed by reamed intramedullary nailing right tibia, open reduction internal fixation left forearm
2) Reamed intramedullary nailing bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, splinting left forearm
3) External fixation bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, open reduction internal fixation left
forearm
4) External fixation bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, splinting left forearm
5) External fixation right femur and right tibia following irrigation and debridement, reamed intramedullary nailing left femur, splinting left forearm
With a base deficit of 10mEq/L, the patient is under-resuscitated and unstable. Thus, damage control orthopedics via external fixation of the long bone injuries with irrigation and debridement of the open tibia is the appropriate next step in management.
Of all of the reported values, the most important predictor of morbidity and mortality is the base deficit (normal range -2 to +2mEq/L), which represents overall resuscitation status. Another representative parameter of resuscitation status is lactate (normal
A 26-year-old male sustains an elbow injury after a fall from a skateboard resulting in valgus and supination forces across the left elbow. A CT scan of the left elbow is shown in Figures A through D. This fracture pattern is most commonly associated with what other traumatic elbow pathology?
1) Posteromedial rotatory instability
2) Capitellum fracture
3) Radial head fracture and posterolateral ulnohumeral dislocation
4) Trans-olecranon fracture dislocation
5) Medial (ulnar) collateral ligament rupture
The clinical presentation is consistent with a coronoid tip fracture. This fracture pattern is associated with a radial head fracture and posterolateral ulnohumeral dislocation - together making up the terrible triad injury.
A terrible triad injury is the result of a valgus and supination injury and involves posterolateral elbow dislocation or lateral collateral ligament injury, radial head fracture, and fracture of the coronoid process. The elbow may dislocate postero-laterally with the anterior bundle of the MCL intact, but if the MCL is injured it is typically the last structure to fail. The coronoid fracture is typically a small fragment isolated to the tip. This is a result of a posteriorly directed force driving the coronoid into the trochlea prior to posterior elbow dislocation. CT scan is a useful modality when small or comminuted fragments are difficult to visualize on plain radiographs.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figures A through D show consecutive 2.00 mm sagittal CT reformats demonstrating a small coronoid fracture fragment which was addressed with suture fixation.
Incorrect Answers:
Answer 1. Coronoid anteromedial facet fracture (not tip) in conjunction with LCL disruption can cause posteromedial rotatory instability. Coronoid tip fractures may be associated with posteroLATERAL rotatory instability Answer 2. Capitellum fractures are not associated with coronoid fractures Answer 4. Trans-olecranon fracture dislocations are associated with larger coronoid fracture fragments.
Answer 5. MCL injury is associated with valgus instability but not coronoid fracture
A 62-year-old right-hand-dominant school teacher sustains a mechanical fall at home and presents with right shoulder pain. Plain
radiographs of the right shoulder are pictured in Figures A and B. The patient asks you what she can expect in terms of recovery following this injury. Which of the following is the most appropriate statement?
1) At 1-year post-injury, the right shoulder range of motion will most likely be equal to the contralateral extremity.
2) At 1-year post-injury, you will most likely have returned to your baseline functional status.
3) Early range of motion exercises risk fracture displacement and should be avoided until at least 4 weeks post-injury.
4) Most patients do not return to work following this injury.
5) One in 5 patients with this fracture go on to nonunion and you may benefit from surgery in the future to address this.
This patient has a minimally displaced (1-part) proximal humerus fracture involving the humeral neck and greater tuberosity. This injury pattern is most commonly managed nonoperatively with the majority of patients returning to their baseline functional status by 1 year.
Proximal humerus fractures (PHF) can be classified by number of parts (Neer classification), with a part defined as a fracture fragment displaced > 1cm (> 5mm for greater tuberosity) or angulated > 45°. One-part PHF comprise ~80% of all PHF and are treated nonoperatively with a sling and early range of motion (ROM).
Tejwani et al performed a prospective study of 67 patients with 1-part PHF. At 1-year follow up the ASES score and functional status was similar to pre-injury status. However, ROM of the affected shoulder was diminished in both external and internal rotation. Forward flexion was preserved.
Hanson et al prospectively analyzed 160 patients with PHF of all types (1-4 parts and head-splitting) managed nonoperatively. At 1-year follow up, 93% showed solid union. Constant and DASH scores improved steadily over time but were still lower compared to the contralateral extremity. Of employed patients, 97.6% returned to work with a median time off of 10 weeks and no difference between manual and nonmanual workers.
Figures A and B are the AP and axillary radiographs of the right shoulder, respectively, demonstrating a 1-part PHF involving the humeral neck and greater tuberosity.
Incorrect Responses:
Answer 1: At 1-year follow up, most patients have restored forward flexion but lack both internal and external rotation compared to the contralateral extremity.
Answer 3: Early ROM exercises starting at 2 weeks post-injury have not been shown to result in fracture displacement. Patients managed with early rehabilitation exhibit high union rates and largely return to baseline functional status.
Answer 4: The vast majority of patients with PHF of all types return to work post-injury.
Answer 5: One-part PHF have an excellent union rate (>90%) and rarely require surgery.
A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?
1) Pulmonary embolus
2) Periprosthetic fracture
3) Contralateral hip fracture
4) Osteonecrosis
5) Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels III hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
Answer 1: The incidence of pulmonary embolus after hip fracture is
A 58-year-old male is involved in a motor vehicle collision and sustains the injury shown in Figure A in addition to right 5th and 6th rib fractures. Upon evaluation in the emergency department, he is noted to have a 2 centimeter laceration over the anterior aspect of his left leg with visible bone. Vitals and labs are normal. Which of the following statements is most accurate regarding surgical management for this patient?
1) Reamed intramedullary nailing is favored due to increased rates of union
2) Unreamed intramedullary nailing is favored due to presence of concomitant rib fractures
3) Reamed intramedullary nailing is favored due to decreased rates of infection
4) Unreamed intramedullary nailing is favored due to less local trauma
5) Both unreamed and reamed intramedullary nailing are equivalent
Both unreamed and reamed intramedullary nailing are equivalent treatments in patients with open tibia fractures. Intramedullary nailing is the treatment of choice for stable patients with tibial shaft fractures.
Tibial shaft fractures can be the result of low energy twisting injuries or higher energy axial loads. Closed fractures with acceptable alignment can be often be treated with closed reduction and casting. Intramedullary nailing, unreamed or reamed, is the treatment of choice for open fractures except in the setting of damage control orthopaedics when an external fixator may be more appropriate.
Bhandari et al. investigated reamed and unreamed intramedullary nailing for tibial shaft fractures in a randomized trial ("SPRINT" Trial - Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators). They concluded that reamed nailing was more beneficial (decreased rate of primary outcome event: need for bone grafting, implant exchange or removal for infection, debridement for infection) for closed fractures, but had no benefit in open fractures.
Finkemeier et al. evaluated consecutive patients treated with unreamed and reamed intramedullary nailing and found similar rates of union in both open and closed tibial shaft fractures at six and twelve months.
Figures A shows AP and lateral xrays of the left tibia showing a tibial shaft fracture.
Incorrect Answers:
Answer 1-4: Unreamed and reamed intramedullary nailing for open tibia fractures are similar in terms of union rates, infection rates, and rates of reoperation. There is a theoretical risk of pulmonary complications with reaming but it has not been proven.
A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
1) Popliteus and pes anserine
2) Lateral head of the gastrocnemius and pes anserine
3) Politeus and lateral head of the gastrocnemius
4) Iliotibial band and medial head of the gastrocnemius
5) Pes anserine and medial head of the gastrocnemius
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
Answers 1-4. These intervals are not the correct intervals utilized in a posteromedial approach to the tibial plateau.
A 25-year-old male presents to the emergency department with the injury seen in Figure A after a motorcycle collision. The patient has a blood pressure of 70 systolic, elevated lactate and a tense abdomen with positive FAST examination. Trauma surgery will be performing an emergent laparotomy. Orthopaedic surgery is consulted and places a pelvic external fixator intraoperatvely to assist with resuscitation. What is an advantage of supra-acetabular external fixator pins as compared with iliac crest pins?
1) Less interference with pelvic surgical incisions
2) Less risk of pin tract infection
3) Less risk of malreduction
4) Less control of posterior pelvic ring
5) No interference with laparotomy
One advantage of supra-acetabular external fixator pins is that they do not interfere or contaminate future approaches to the pelvis or acetabulum involving the lateral window.
In multiply injured patients with pelvic trauma external fixation of the pelvic ring is a valuable tool to assist with resuscitation. Pelvic external fixation should be applied rapidly and allow full access to the abdomen for general surgery intervention. Regardless of the technique used, a pelvic external fixator should form a stable construct that minimizes motion of fracture surfaces and allows for clot formation.
Haidukewych et al evaluated the safety of supra-acetabular pin placement in a cadaveric study. The authors found that the lateral femoral cutaneous nerve (LFCN) was most at risk during pin placement.
Figure A demonstrates a widely displaced symphyseal dislocation with associated bilateral sacroiliac (SI) dislocations (APC 3). Illustration A demonstrates an outlet radiograph of a supra-acetabular external fixtator in conjunction with posterior pelvic ring fixation for an LC3 pelvic ring injury.
Illustration B is an illustration of iliac crest external fixation. The video demonstrates techniques for application of both supra-acetabular and iliac
crest external fixation pins.
Incorrect Answers:
Answer 2: There has not been a difference demonstrated with pin tract infection between supra-acetabular and iliac crest pins
Answer 3: Both techniques have a risk of malreduction
Answer 4: Theoretically supra-acetabular pins may better control the posterior ring as they may be advanced to the posterior ilium (PSIS) if placed appropriately
Answer 5: Neither type of pin placement or frame should interfere with laparotomy
What physical exam finding is most likely to be found in association with the injury shown in Figures A and B?
1) Numbness in the small finger and ulnar side of the ring finger
2) No elbow instability
3) Varus posteromedial rotatory instability
4) Valgus posterolateral rotatory instability
5) An anterior open wound
The x-ray shows a fracture of the anteromedial facet of the coronoid with an intact radial head. Large anteromedial facet fractures are associated with varus posteromedial rotatory instability.
The anteromedial facet of the coronoid provides support to the medial elbow against varus stress. Varus and posteromedial force applied to the elbow results in disruption of the lateral collateral ligament (LCL) from its proximal origin. The coronoid is fractured as it is forced against the medial trochlea.
Coronoid fractures of significant size involving the sublime tubercle (insertion of medial collateral ligament) result in varus instability.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques. He states that when a coronoid fracture is associated with a pattern of varus instability, it requires fixation with either suture, buttress plating or screw fixation. Concomitant LCL repair or reconstruction will also be necessary.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong
associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figure A is an AP view of an elbow with an anteromedial facet of the coronoid fractured. The lateral joint space is widened due to injury to the LCL. The medial joint space is narrowed and collapsed. A lateral view is shown in Figure
B. Illustrations A and B show AP and lateral views of a coronoid fracture fixed with buttress plating. The LCL origin was fixed with a suture anchor. Illustration C shows the O'Driscoll classification of coronoid fractures. Illustration D lists injury patterns that suggest posteromedial versus posterolateral rotatory instability.
Incorrect Answers:
Answer 1. Although possible, ulnar nerve symptoms are not characteristic of this injury and would not be as likely as elbow instability in the non-dislocated elbow shown in the radiograph
Answer 2. Although not dislocated, the AP radiograph shows signs of subluxation and instability (lateral joint space widening, medial joint space collapse and large coronoid fragment).
Answer 4. Valgus posterolateral instability is associated with very small coronoid fragments
Answer 5. If open, the wound associated with these fractures is usually posterior
A 35-year-old man presents to the ED as the restrained driver of a high speed motor vehicle collision complaining of hip, chest, and abdominal pain. He becomes diaphoretic, tachycardic, and hypotensive in the trauma bay and is noted to have diminished lower extremity pulses. He is found on ATLS workup to have mediastinal widening.
Which of the following injuries is most associated with thoracic aortic injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Thoracic aortic rupture is associated with posterior hip dislocation in deceleration trauma mechanism of injuries.
Posterior hip dislocations are infrequently associated with local vascular injuries. With bilateral perfusion deficits, more proximal large vessel trauma should be considered, and in this situation, thoracic surgery should be involved emergently. Screening chest x-ray in the trauma bay should be reviewed for widened mediastinum, suggestive of aortic injury, as shown in illustration A. Given the high energy mechanism associated with these injuries, a full ATLS trauma survey must be done for every patient.
Marymont et al. studies the association between posterior hip dislocation and thoracic aortic injury. They performed a retrospective chart review of 89 posterior hip dislocations and found 8% had an aortic injury. Although not statistically significant, they note the importance of evaluation for aortic injury in patients with posterior hip dislocations given its emergent life-threatening nature.
In addition to associated chest injuries, Schmidt et al. highlight the importance of evaluating the ipsilateral knee after high-energy traumatic hip dislocation. In a prospective study, they identified a 93% rate of ipsilateral knee injury on MRI including effusion (37%), bone bruising (33%), and meniscal tear (30%) as the most common. They recommend a thorough exam but also expanded use of knee MRI after hip dislocation.
Illustration A shows an example of chest x-ray with a widened mediastinum, suggestive of thoracic aortic injury.
Answer choices A,B,D,E show other injury patterns: Answer A - Right femoral neck fracture
Answer B - Right intertrochanteric hip fracture Answer D - Right subtrochanteric hip fracture
Answer E - Right superior and inferior pubic rami fractures
A 31-year-old female smoker was involved in a skiing accident approximately 9 months ago and underwent open reduction internal fixation of the radius and ulna at the time of injury. She now returns to the clinic complaining of increasing pain with range of motion and activity. Radiographs from her most recent follow-up can be seen in Figure A. Laboratory tests show ESR, CRP and WBC count to be within normal limits. Which of the following options is the most appropriate next step in management?
1) Bone scan
2) Above elbow cast
3) Removable splint
4) Reamed intramedullary nail
5) Iliac crest bone grafting + compression plating
This patient is presenting with an atrophic non-union of the ulna after open reduction internal fixation for a both bone forearm fracture 9 months ago. The most appropriate next step in management would be iliac crest bone grafting and compression plating of the ulna.
The primary issue with an atrophic nonunion is biological. The blood supply is poor and therefore incapable of purposeful fracture healing. Smokers, as in this vignette, are at high risk for nonunion. The treatment of an atrophic nonunion involves improving biology at the fracture site through use of autologous bone graft (e.g. iliac crest) and providing mechanical stability by means of compression plating (e.g. 3.5 mm LC-DCP).
dos Reis et al. reports excellent results of 31 cases of diaphyseal forearm fracture non-unions treated with autologous bone grafting and compression
plating. Thirty of thirty-one patients went on to bony union within 3.5 months of revision surgery.
Nadkarni et al. presented a case series of 11 patients with non-unions of various long bones initially managed with intradmedullary (IM) nail fixation. The authors successfully used locking compression plates while retaining the IM nails in the treatment of the nonunion in all cases.
Figure A shows an AP radiograph of a both bone forearm fracture. Figure B shows an AP and lateral radiograph of an atrophic non-union of the ulnar shaft. Illustration A shows a lateral x-ray of a fully healed radius and ulna after hardware removal 1 year after revision surgery.
Incorrect Answers:
Answer 1: With normal WBC, ESR and CRP levels, there is little reason to suspect an infectious non-union, thus, there is no indication for a bone scan at this time.
Answer 2 & 3: Immobilization will not treat the underlying issue of biology. Autologous bone grafting is necessary in the treatment of atrophic non-unions. Answer 4: A reamed IM nail does not provide adequate mechanical stability and is not used in the treatment of radius or ulna non-unions.
A 27 year-old patient sustains a fracture-dislocation of the acetabulum. Pelvic radiographs (Figures A and B) are taken at initial presentation and a CT scan (Figures C and D) is performed after reduction of the hip in the emergency room. What is the importance of the finding highlighted in the CT scan cuts?
1) Comminution indicates a better result with non-operative management
2) Significant marginal impaction could compromise the results of the surgical reduction if the joint surface is not properly restored
3) The impacted fracture segment will heal without fixation because it is not gapped or translated
4) The CT scan finding highlighted indicates osteochondral defects to the femoral head, which can be addressed arthroscopically
5) Intraarticular fracture fragments should be discarded from the surgical field, as incorporation of the fragments into the fixation construct leads to a high rate of avascular necrosis
The CT images shown in Figures C and D display significant marginal impaction of the joint surface.
Marginal impaction is common in posterior wall fractures and fracture-dislocations. Critical review of CT imaging of posterior wall fractures can help with preoperative planning for identifying impaction of the articular surface of the acetabulum. Restoration of the sphericity of the acetabulum to match that of the femoral head is important for successful outcome following ORIF of posterior wall fractures. A common surgical technique to accomplish joint surface restoration includes freeing the impacted articular segments, bone grafting of the void created to support the articular segments, and buttress plating of the posterior wall fracture fragments.
Patel et al. discuss the challenge of interpreting imaging of the acetabulum for assessing fracture characteristics that may significantly impact success or surgical intervention. These characteristics include: articular displacement, marginal impaction, incongruity of the joint surface, intra-articular fragments, and osteochondral injury to the femoral head. Based on expert review of images, determination of significant marginal impaction had a poor intraobserver reliability, as did each of the other modifiers listed.
Figures A and B are radiographs of the posterior wall fracture and hip dislocation. They do not show the large amount of marginal impaction of the acetabular surface. Figure C (coronal reconstruction) and Figure D (sagittal reconstruction) point out a large a amount of marginal impaction of the acetabular. Note the disruption of the joint surface on the intact portion of the acetabulum.
Incorrect answers:
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
, 2: Exchange nailing has not produced good results following failures of intramedullary nail fixation of humeral shaft fractures. Union rates have been shown between 30-40%,
Answer 3: There is little evidence to support exchange nailing for distal femoral nonunions. Union rates have been shown at 50-60%.
Answer 4: Nonunions following comminuted fractures do not appear to respond
to exchange nailing. Union rates have been reported as 45-80%.
Figures A to C show radiographs of a 70 year-old male who fell on the ice 5 days ago. He could initially walk after the fall, but he is now unable to weight-bear on the leg due to pain. Physical examination shows diffuse ankle swelling, with no medial sided ankle tenderness. He is neurovascularly intact. The patient does not smoke and has no medical history. A gravity stress radiograph is demonstrated in Figure
D. After closed reduction, there is 2 mm of fracture displacement, no talar shift and the talocrural angle = 83 degrees. What is the most appropriate treatment?
1) Total contact casting, non-weightbearing, for 6-8 weeks.
2) MRI to better evaluate the deep deltoid ligament
3) Open reduction and internal fixation
4) CT scan to better identify the fracture pattern
5) Below knee splint for 2-4 weeks and advance to weight-bearing as tolerated in an immobilizer boot
The patient has a 5 day old Weber B fibula fracture with a well reduced mortise and stress radiograph that demonstrates no instability of the mortise. The appropriate treatment would be a period of immobilization followed by advanced weight-bearing as tolerated.
The patient has an isolated lateral malleolus fracture. These fracture are stable if the deltoid ligament is intact, and unstable if the deltoid ligament is disrupted. The competency of the deltoid ligament can be evaluated with a stress radiograph which is completed by placing the ankle in maximum dorsiflexion and 15° of internal rotation while an external rotation force is applied to the foot. A stress radiograph (manual or gravity assisted) is positive if there is subluxation of the talus during the exam. The presence of tenderness or swelling medially at the ankle has been shown to be a poor indicator of medial-sided injury. The clinical utility of MRI scans in ankle fractures is controversial.
Koval et al. reported on 21 patients with 5-8 mm of clear space widening on stress radiographs after an isolated Weber B lateral malleolus fracture. They performed MRI's of all ankles and found 90% had at least a partially intact deep deltoid. The patients with a partially intact deep deltoid were treated with weight-bearing as tolerated in a removable boot. 14/15 patients that were available for one year follow-up had an AOFAS score of 100.
Egol et al. reported on the treatment of 30 patients with an isolated fibula fracture and a stress XR with over 4mm of clear space widening, but no signs of medial injury such as tenderness, ecchymosis, or swelling around the medial malleolus on physical exam. Twenty patients were treated without surgery, and 10 patients were treated with surgery. The average AOFAS score was similar in both groups at final follow up.
Figure A demonstrates an AP radiograph of a Weber B fibula fracture with minimal medial clear space widening.
Figure B demonstrates a mortise radiograph of a Weber B fibula fracture with a congruent mortise.
Figure C demonstrates a lateral radiograph of a Weber B fibula fracture with a congruent mortise.
Figure D demonstrates a stress radiograph with minimal medial clear space widening.
Incorrect Answers:
Answer 1: Total contact cast (TCC) is an effective treatment in neuropathic, noninfected, and nonischemic foot ulcers. There is no indication for TCC in this
patient.
Answer 2: The clinical utility of MRI scans in ankle fractures is controversial. Answer 3: The patient has a stable ankle fracture. The post-reduction parameters are within normal limits - intact mortise, no talar shift,
A 44-year-old male presents after being struck by a car. He is hypotensive, and has an obvious open tibia and a closed femoral shaft fracture. A pelvic radiograph is obtained and shown in Figure A. A representative CT scan image in shown in Figure B. The patient is placed in a pelvic binder, and his blood pressure normalizes with crystalloid and a blood transfusion. He then undergoes pelvic angiography, and his internal iliac artery is embolized. Which of the following definitive treatment options is most appropriate in this case?
1) Anterior pelvic external fixation with pins placed in the AIIS and a posterior sacroiliac screw
2) Open reduction and internal fixation of the pubic symphysis with a two hole plate and posterior fixation with a iliosacral screw
3) Open reduction and internal fixation of the pubic symphysis with a nonlocking multi-hole plate and posterior fixation with a iliosacral screw
4) Anterior pelvic external fixation and posterior triangular osteosynthesis
5) Open reduction and internal fixation of the pubic symphysis with a locked multi-hole plate and posterior sacral plate fixation
The radiographs and CT scan show a fracture pattern consistent with an APC-III injury. This is most appropriately treated with pubic symphysis ORIF with a multi-hole plate and posterior iliosacral screw fixation.
APC-III pelvic ring injuries are associated with with disruption of the anterior and posterior SI ligaments (SI dislocation) as well as disruption of
sacrospinous and sacrotuberous ligaments. They are commonly associated with vascular injury and retroperitoneal bleeding.
Sagi et al studied the radiographic and clinical outcome of symphyseal plating techniques, specifically comparing two hole (THP) vs multi-hole plating (MHP). Retrospective review of charts and radiographs immediately after the index procedure to latest follow-up was performed. When comparing the 2 different methods of anterior fixation, they found that the rate of fixation failure was greater in group THP (33%) than group MHP (12%). When evaluating the presence of a malunion as a result of these 2 treatment methods, there were more present in the THP group (57%) than in the MHP group (15%). On the basis of these findings, the authors recommended multi-hole plating of unstable pubic symphyseal disruptions.
Grimshaw et al performed a biomechanical study to determine the failure risk and potential benefit to use of locked fixation constructs in simulated pelvic ring injuries. The authors used a six-hole 3.5-mm plate specifically designed for the symphysis pubis with the capability of fixation in locked or unlocked mode, six pelves were fixed with locked screws and six pelves were fixed standard unlocked bicortical screws. Biomechanical testing was performed, and no abrupt failures were noted. However, locked plating of the pubic symphysis did not appear to offer any advantage over the standard unlocked technique
Illustrations A, B, and C show the AP, outlet, and inlet postoperative radiographs.
Incorrect Answers:
1,4-Anterior pelvic fixation is typically not used as definitive treatment of these injuries unless performed in a damage-control setting. The patient in this case is stable.
2-Multi-hole plate fixation of the pubic symphysis is preferred over 2-hole plate fixation.
5-Posterior sacral plating is not indicated in this fracture pattern, as there is no significant sacral comminution of vertical shear component. Furthermore, no distinct advantage has been found with locked symphyseal plating.
Figure A is a radiograph of an 80-year-old woman who sustained a closed injury to her left arm 10 months ago. She presents to office today complaining of persistent pain in her arm. What is the most likely metabolic or endocrine abnormality contributing to this patients presentation?
1) Vitamin D deficiency
2) Central hypogonadism
3) Thyroid disorder
4) Parathyroid hormone disorder
5) Calcium deficiency
Figure A is a radiograph showing oligotrophic nonunion of a proximal third humeral shaft fracture. The most likely underlying metabolic or endocrine abnormality with this presentation is vitamin D deficiency.
The etiology of fracture nonunion is multifactorial. Predisposing factors include: mechanical instability, poor bone-to-bone contact, infection and biological/biochemical factors. A variety of other contributing factors, such as cigarette smoking and malnutrition, have also been described. Correctable metabolic or endocrine abnormalities are common in elderly patients and are considered contributory in the etiology of fracture non-union. Correction of these abnormalities should be considered prior to surgical fixation.
Brinker et al. studied 37 patients with fracture nonunions with identifiable metabolic or endocrine abnormalities. The distribution of nonunion types at the 46 sites were: oligotrophic (23), atrophic (12), infected (7), and hypertrophic
(4). They showed that 85% of patients had a previously undiagnosed metabolic or endocrine abnormality. The most common newly diagnosed abnormality was vitamin D deficiency in 25 of the 37 patients (68%).
Kuo et al. studied 155 consecutive minimal-trauma fracture subjects for metabolic abnormalities with bone mineral density and laboratory testing. At baseline, only 26% had had proper workup for metabolic abnormalities. After diagnostic work-up, 44% of patients were recommended for anti-resorptive therapy and 56% were recommended calcium/vitamin D medication.
Illustrations A and B show open reduction internal fixation of Figure A with a proximal humeral plate.
Incorrect Answers:
Answer 2: Studies show 15% of fracture nonunions can be attributed to undiagnosed central hypogonadism.
Answer 3: Studies show 24% of fracture nonunions can be attributed to previously established or undiagnosed thyroid disorders
Answer 4: Studies show 11% of fracture nonunions can be attributed to previously established or undiagnosed parathyroid disorders
Answer 5: Studies show 35% of fracture nonunions can be attributed to lack of calcium.
Which of the following fracture patterns is classically associated with varus malunion if treated with closed reduction and casting?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure B shows a midshaft tibia fracture with an intact fibula, which places the fracture at increased risk of varus malalignment during healing.
Nonsurgically treated tibial shaft fractures with an intact fibula have an increased risk of varus malunion when treated nonsurgically. The fibula acts as a strut, preventing valgus collapse, but predisposing to varus angulation. Limb-length discrepancies can also occur.
Teitz et al. found that 26 percent of patients over the ago of 20 years old with isolated tibial shaft fractures treated nonsurgically went on to varus malunion. They also found that when the fibula remains intact, a tibiofibular length discrepancy can develop and cause altered strain patterns in the tibia and fibula leading to later ipsilateral joint sequeale.
Bonnevialle et al performed a retrospective study to assess the outcome after reamed nailing of tibial fractures with an intact fibula. Thirty-eight fractures were evaluated at a minimum of one year from surgery. Healing was achieved after the first intention treatment in 30 patients, after dynamization in 6. A non-union in 2 patients was also successfully managed with new nailing and dynamization. The authors concluded that nailing is a reliable technique for the treatment of tibial fractures with an intact fibula.
Sarmiento et al reviewed 1,000 consecutive closed diaphyseal tibial fractures, treated with prefabricated functional below-knee braces, to determine factors predictive of final fracture outcome. They found that final angulatory deformity in any plane was
A 55-year-old female presents to the emergency room after falling off her balcony. She sustained the isolated, closed injury shown in Figures A and B. She is otherwise healthy, but routinely smokes 30 cigarettes per day. What would be the most appropriate sequence of treatment steps for definitive management of this injury?
1) Closed reduction and splinting followed by delayed casting
2) Immediate open reduction internal fixation
3) Closed reduction and splinting, CT scan, and immediate open reduction internal fixation
4) Closed reduction and splinting, CT scan, external fixation, delayed open reduction internal fixation
5) Closed reduction and splinting, external fixation, CT scan, delayed open reduction internal fixation
Figures A and B show radiographs of a comminuted AO/OTA C3 fracture of the distal tibia. The most appropriate steps in the management of this patients injury would include: Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation in this sequence.
Infection and wound healing problems are common with comminuted distal tibia fractures due to an increased incidence of soft-tissue complications associated with the operative management. Patients with a history of diabetes and smoking are at further risk. To decrease the risk of complications in this patient, a two-staged, delayed open reduction internal fixation technique is the best option for the treatment of severe pilon fractures.
Patterson et al. reviewed 23 consecutive patients with comminuted distal tibia fractures. They showed 0% infections or wound-healing problems in their patient population treated with a two-staged protocol. Their protocol involved fibula fixation with an intramedullary implant and application of a medial external fixator to to regain length and restore anatomic alignment. Re-evaluation of the limb occurred ten to fourteen days later for definitive fixation.
Sirkin et al. retrospectively reviewed 40 closed and 82 open pilon fractures (AO types 43A-C) that were treated with staged surgical management (avg. time from ext. fix. to formal reconstruction was 14 days (range 4 to 31) They reported 17% post-operative wound complication in the closed group and 11% post-operative wound complication in the open group (Gustilo Type I-III). They suggest the technique was successful in both closed and open pilon fractures.
Illustration A shows open reduction internal fixation of the above injury. Incorrect Answers:
Answer 1: Universally, nonoperative treatment of OTA/AO C3 fractures has led
to poor outcomes.
Answer 2,3: Although Ruedi and Allgower (1969) were the first to report successful results with primary open reduction and internal fixation of low-energy fracture patterns, few studies have achieved good results with low soft-tissue complications.
Answer 4: CT scan is most appropriate after frame application. This will allow for distraction and indirect reduction of the fragments to better characterize the fracture pattern for pre-operative planning.
When using a trochanteric femoral nail, placing your start point in which area will result in varus deformity?
1) A
2) B
3) C
4) A and B
5) B and C
Placing your start point lateral to the tip of the greater trochanter (location A) will cause varus deformity.
When using a trochanteric entry femoral nail, the ideal starting point is just medial to the tip of the greater trochanter. Placement lateral to the tip of the trochanter will cause varus malalignment.
Ostrum et al. in a cadaveric study, reported on deformities following medial, standard, and lateral starting points for trochanteric entry femoral nails. Nails inserted too medially yielded excessive valgus, while nails inserted too laterally yielded varus malalignment. Those started at the tip yielded the most neutral alignment, but still with slight varus. The authors recommended a start point just medial to the tip of the greater trochanter.
Figure A exhibits ideal starting point for a trochanteric entry nail (B), for a piriformis start nail (C) and a start point that is too lateral, causing varus (A). Illustration A depicts 4 different types of trochanteric entry nails that started at the tip of the greater trochanter and although mostly neutral, still exhibit slight varus.
Incorrect answers:
Answer 2. Ideal starting point for a trochanteric entry nail resulting in neutral alignment.
Answer 3. Ideal starting point for a piriformis entry nail or valgus in a trochanteric entry nail.
Answer 4. All of the choices will yield different results. Answer 5. The appropriate answer choice is A.
A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and
B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?
1) Absent plantar sensation at presentation
2) Depression at 3 months post-injury
3) Use of an intramedullary nail
4) Free tissue transfer instead of rotational flap
5) Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
Answer 1: Absent plantar sensation does not predict worse outcomes and patients may have significant return of sensation at 2-year follow up.
Answer 3: No difference has been demonstrated with methods of internal fixation for type IIIB tibia shaft fractures.
Answer 4: No difference has been shown with the use of free tissue versus rotational tissue for type IIIB tibia fractures.
Answer 5: The number of debridements has not been shown to influence outcome.
A 45-year-old male is involved in a motorcycle crash. Work-up reveals a closed, right femoral shaft fracture, an open, right tibial shaft fracture, a closed left mid-shaft radius and ulna fractures, and a closed left femoral shaft fracture. His heart rate is 115bpm with a systolic blood pressure of 105mmHg. Initial hematocrit values are reported at
31.5 g/dL and his base deficit is 10mEq/L. What is the most appropriate next step in management?
1) Reamed intramedullary nailing bilateral femur fractures, irrigation and debridement followed by reamed intramedullary nailing right tibia, open reduction internal fixation left forearm
2) Reamed intramedullary nailing bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, splinting left forearm
3) External fixation bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, open reduction internal fixation left
forearm
4) External fixation bilateral femur fractures, irrigation and debridement followed by external fixation right tibia, splinting left forearm
5) External fixation right femur and right tibia following irrigation and debridement, reamed intramedullary nailing left femur, splinting left forearm
With a base deficit of 10mEq/L, the patient is under-resuscitated and unstable. Thus, damage control orthopedics via external fixation of the long bone injuries with irrigation and debridement of the open tibia is the appropriate next step in management.
Of all of the reported values, the most important predictor of morbidity and mortality is the base deficit (normal range -2 to +2mEq/L), which represents overall resuscitation status. Another representative parameter of resuscitation status is lactate (normal
A 26-year-old male sustains an elbow injury after a fall from a skateboard resulting in valgus and supination forces across the left elbow. A CT scan of the left elbow is shown in Figures A through D. This fracture pattern is most commonly associated with what other traumatic elbow pathology?
1) Posteromedial rotatory instability
2) Capitellum fracture
3) Radial head fracture and posterolateral ulnohumeral dislocation
4) Trans-olecranon fracture dislocation
5) Medial (ulnar) collateral ligament rupture
The clinical presentation is consistent with a coronoid tip fracture. This fracture pattern is associated with a radial head fracture and posterolateral ulnohumeral dislocation - together making up the terrible triad injury.
A terrible triad injury is the result of a valgus and supination injury and involves posterolateral elbow dislocation or lateral collateral ligament injury, radial head fracture, and fracture of the coronoid process. The elbow may dislocate postero-laterally with the anterior bundle of the MCL intact, but if the MCL is injured it is typically the last structure to fail. The coronoid fracture is typically a small fragment isolated to the tip. This is a result of a posteriorly directed force driving the coronoid into the trochlea prior to posterior elbow dislocation. CT scan is a useful modality when small or comminuted fragments are difficult to visualize on plain radiographs.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figures A through D show consecutive 2.00 mm sagittal CT reformats demonstrating a small coronoid fracture fragment which was addressed with suture fixation.
Incorrect Answers:
Answer 1. Coronoid anteromedial facet fracture (not tip) in conjunction with LCL disruption can cause posteromedial rotatory instability. Coronoid tip fractures may be associated with posteroLATERAL rotatory instability Answer 2. Capitellum fractures are not associated with coronoid fractures Answer 4. Trans-olecranon fracture dislocations are associated with larger coronoid fracture fragments.
Answer 5. MCL injury is associated with valgus instability but not coronoid fracture
A 62-year-old right-hand-dominant school teacher sustains a mechanical fall at home and presents with right shoulder pain. Plain
radiographs of the right shoulder are pictured in Figures A and B. The patient asks you what she can expect in terms of recovery following this injury. Which of the following is the most appropriate statement?
1) At 1-year post-injury, the right shoulder range of motion will most likely be equal to the contralateral extremity.
2) At 1-year post-injury, you will most likely have returned to your baseline functional status.
3) Early range of motion exercises risk fracture displacement and should be avoided until at least 4 weeks post-injury.
4) Most patients do not return to work following this injury.
5) One in 5 patients with this fracture go on to nonunion and you may benefit from surgery in the future to address this.
This patient has a minimally displaced (1-part) proximal humerus fracture involving the humeral neck and greater tuberosity. This injury pattern is most commonly managed nonoperatively with the majority of patients returning to their baseline functional status by 1 year.
Proximal humerus fractures (PHF) can be classified by number of parts (Neer classification), with a part defined as a fracture fragment displaced > 1cm (> 5mm for greater tuberosity) or angulated > 45°. One-part PHF comprise ~80% of all PHF and are treated nonoperatively with a sling and early range of motion (ROM).
Tejwani et al performed a prospective study of 67 patients with 1-part PHF. At 1-year follow up the ASES score and functional status was similar to pre-injury status. However, ROM of the affected shoulder was diminished in both external and internal rotation. Forward flexion was preserved.
Hanson et al prospectively analyzed 160 patients with PHF of all types (1-4 parts and head-splitting) managed nonoperatively. At 1-year follow up, 93% showed solid union. Constant and DASH scores improved steadily over time but were still lower compared to the contralateral extremity. Of employed patients, 97.6% returned to work with a median time off of 10 weeks and no difference between manual and nonmanual workers.
Figures A and B are the AP and axillary radiographs of the right shoulder, respectively, demonstrating a 1-part PHF involving the humeral neck and greater tuberosity.
Incorrect Responses:
Answer 1: At 1-year follow up, most patients have restored forward flexion but lack both internal and external rotation compared to the contralateral extremity.
Answer 3: Early ROM exercises starting at 2 weeks post-injury have not been shown to result in fracture displacement. Patients managed with early rehabilitation exhibit high union rates and largely return to baseline functional status.
Answer 4: The vast majority of patients with PHF of all types return to work post-injury.
Answer 5: One-part PHF have an excellent union rate (>90%) and rarely require surgery.
A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?
1) Pulmonary embolus
2) Periprosthetic fracture
3) Contralateral hip fracture
4) Osteonecrosis
5) Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels III hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
Answer 1: The incidence of pulmonary embolus after hip fracture is
A 58-year-old male is involved in a motor vehicle collision and sustains the injury shown in Figure A in addition to right 5th and 6th rib fractures. Upon evaluation in the emergency department, he is noted to have a 2 centimeter laceration over the anterior aspect of his left leg with visible bone. Vitals and labs are normal. Which of the following statements is most accurate regarding surgical management for this patient?
1) Reamed intramedullary nailing is favored due to increased rates of union
2) Unreamed intramedullary nailing is favored due to presence of concomitant rib fractures
3) Reamed intramedullary nailing is favored due to decreased rates of infection
4) Unreamed intramedullary nailing is favored due to less local trauma
5) Both unreamed and reamed intramedullary nailing are equivalent
Both unreamed and reamed intramedullary nailing are equivalent treatments in patients with open tibia fractures. Intramedullary nailing is the treatment of choice for stable patients with tibial shaft fractures.
Tibial shaft fractures can be the result of low energy twisting injuries or higher energy axial loads. Closed fractures with acceptable alignment can be often be treated with closed reduction and casting. Intramedullary nailing, unreamed or reamed, is the treatment of choice for open fractures except in the setting of damage control orthopaedics when an external fixator may be more appropriate.
Bhandari et al. investigated reamed and unreamed intramedullary nailing for tibial shaft fractures in a randomized trial ("SPRINT" Trial - Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators). They concluded that reamed nailing was more beneficial (decreased rate of primary outcome event: need for bone grafting, implant exchange or removal for infection, debridement for infection) for closed fractures, but had no benefit in open fractures.
Finkemeier et al. evaluated consecutive patients treated with unreamed and reamed intramedullary nailing and found similar rates of union in both open and closed tibial shaft fractures at six and twelve months.
Figures A shows AP and lateral xrays of the left tibia showing a tibial shaft fracture.
Incorrect Answers:
Answer 1-4: Unreamed and reamed intramedullary nailing for open tibia fractures are similar in terms of union rates, infection rates, and rates of reoperation. There is a theoretical risk of pulmonary complications with reaming but it has not been proven.
A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
1) Popliteus and pes anserine
2) Lateral head of the gastrocnemius and pes anserine
3) Politeus and lateral head of the gastrocnemius
4) Iliotibial band and medial head of the gastrocnemius
5) Pes anserine and medial head of the gastrocnemius
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
Answers 1-4. These intervals are not the correct intervals utilized in a posteromedial approach to the tibial plateau.
A 25-year-old male presents to the emergency department with the injury seen in Figure A after a motorcycle collision. The patient has a blood pressure of 70 systolic, elevated lactate and a tense abdomen with positive FAST examination. Trauma surgery will be performing an emergent laparotomy. Orthopaedic surgery is consulted and places a pelvic external fixator intraoperatvely to assist with resuscitation. What is an advantage of supra-acetabular external fixator pins as compared with iliac crest pins?
1) Less interference with pelvic surgical incisions
2) Less risk of pin tract infection
3) Less risk of malreduction
4) Less control of posterior pelvic ring
5) No interference with laparotomy
One advantage of supra-acetabular external fixator pins is that they do not interfere or contaminate future approaches to the pelvis or acetabulum involving the lateral window.
In multiply injured patients with pelvic trauma external fixation of the pelvic ring is a valuable tool to assist with resuscitation. Pelvic external fixation should be applied rapidly and allow full access to the abdomen for general surgery intervention. Regardless of the technique used, a pelvic external fixator should form a stable construct that minimizes motion of fracture surfaces and allows for clot formation.
Haidukewych et al evaluated the safety of supra-acetabular pin placement in a cadaveric study. The authors found that the lateral femoral cutaneous nerve (LFCN) was most at risk during pin placement.
Figure A demonstrates a widely displaced symphyseal dislocation with associated bilateral sacroiliac (SI) dislocations (APC 3). Illustration A demonstrates an outlet radiograph of a supra-acetabular external fixtator in conjunction with posterior pelvic ring fixation for an LC3 pelvic ring injury.
Illustration B is an illustration of iliac crest external fixation. The video demonstrates techniques for application of both supra-acetabular and iliac
crest external fixation pins.
Incorrect Answers:
Answer 2: There has not been a difference demonstrated with pin tract infection between supra-acetabular and iliac crest pins
Answer 3: Both techniques have a risk of malreduction
Answer 4: Theoretically supra-acetabular pins may better control the posterior ring as they may be advanced to the posterior ilium (PSIS) if placed appropriately
Answer 5: Neither type of pin placement or frame should interfere with laparotomy
What physical exam finding is most likely to be found in association with the injury shown in Figures A and B?
1) Numbness in the small finger and ulnar side of the ring finger
2) No elbow instability
3) Varus posteromedial rotatory instability
4) Valgus posterolateral rotatory instability
5) An anterior open wound
The x-ray shows a fracture of the anteromedial facet of the coronoid with an intact radial head. Large anteromedial facet fractures are associated with varus posteromedial rotatory instability.
The anteromedial facet of the coronoid provides support to the medial elbow against varus stress. Varus and posteromedial force applied to the elbow results in disruption of the lateral collateral ligament (LCL) from its proximal origin. The coronoid is fractured as it is forced against the medial trochlea.
Coronoid fractures of significant size involving the sublime tubercle (insertion of medial collateral ligament) result in varus instability.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques. He states that when a coronoid fracture is associated with a pattern of varus instability, it requires fixation with either suture, buttress plating or screw fixation. Concomitant LCL repair or reconstruction will also be necessary.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong
associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figure A is an AP view of an elbow with an anteromedial facet of the coronoid fractured. The lateral joint space is widened due to injury to the LCL. The medial joint space is narrowed and collapsed. A lateral view is shown in Figure
B. Illustrations A and B show AP and lateral views of a coronoid fracture fixed with buttress plating. The LCL origin was fixed with a suture anchor. Illustration C shows the O'Driscoll classification of coronoid fractures. Illustration D lists injury patterns that suggest posteromedial versus posterolateral rotatory instability.
Incorrect Answers:
Answer 1. Although possible, ulnar nerve symptoms are not characteristic of this injury and would not be as likely as elbow instability in the non-dislocated elbow shown in the radiograph
Answer 2. Although not dislocated, the AP radiograph shows signs of subluxation and instability (lateral joint space widening, medial joint space collapse and large coronoid fragment).
Answer 4. Valgus posterolateral instability is associated with very small coronoid fragments
Answer 5. If open, the wound associated with these fractures is usually posterior
A 35-year-old man presents to the ED as the restrained driver of a high speed motor vehicle collision complaining of hip, chest, and abdominal pain. He becomes diaphoretic, tachycardic, and hypotensive in the trauma bay and is noted to have diminished lower extremity pulses. He is found on ATLS workup to have mediastinal widening.
Which of the following injuries is most associated with thoracic aortic injury?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Thoracic aortic rupture is associated with posterior hip dislocation in deceleration trauma mechanism of injuries.
Posterior hip dislocations are infrequently associated with local vascular injuries. With bilateral perfusion deficits, more proximal large vessel trauma should be considered, and in this situation, thoracic surgery should be involved emergently. Screening chest x-ray in the trauma bay should be reviewed for widened mediastinum, suggestive of aortic injury, as shown in illustration A. Given the high energy mechanism associated with these injuries, a full ATLS trauma survey must be done for every patient.
Marymont et al. studies the association between posterior hip dislocation and thoracic aortic injury. They performed a retrospective chart review of 89 posterior hip dislocations and found 8% had an aortic injury. Although not statistically significant, they note the importance of evaluation for aortic injury in patients with posterior hip dislocations given its emergent life-threatening nature.
In addition to associated chest injuries, Schmidt et al. highlight the importance of evaluating the ipsilateral knee after high-energy traumatic hip dislocation. In a prospective study, they identified a 93% rate of ipsilateral knee injury on MRI including effusion (37%), bone bruising (33%), and meniscal tear (30%) as the most common. They recommend a thorough exam but also expanded use of knee MRI after hip dislocation.
Illustration A shows an example of chest x-ray with a widened mediastinum, suggestive of thoracic aortic injury.
Answer choices A,B,D,E show other injury patterns: Answer A - Right femoral neck fracture
Answer B - Right intertrochanteric hip fracture Answer D - Right subtrochanteric hip fracture
Answer E - Right superior and inferior pubic rami fractures
A 31-year-old female smoker was involved in a skiing accident approximately 9 months ago and underwent open reduction internal fixation of the radius and ulna at the time of injury. She now returns to the clinic complaining of increasing pain with range of motion and activity. Radiographs from her most recent follow-up can be seen in Figure A. Laboratory tests show ESR, CRP and WBC count to be within normal limits. Which of the following options is the most appropriate next step in management?
1) Bone scan
2) Above elbow cast
3) Removable splint
4) Reamed intramedullary nail
5) Iliac crest bone grafting + compression plating
This patient is presenting with an atrophic non-union of the ulna after open reduction internal fixation for a both bone forearm fracture 9 months ago. The most appropriate next step in management would be iliac crest bone grafting and compression plating of the ulna.
The primary issue with an atrophic nonunion is biological. The blood supply is poor and therefore incapable of purposeful fracture healing. Smokers, as in this vignette, are at high risk for nonunion. The treatment of an atrophic nonunion involves improving biology at the fracture site through use of autologous bone graft (e.g. iliac crest) and providing mechanical stability by means of compression plating (e.g. 3.5 mm LC-DCP).
dos Reis et al. reports excellent results of 31 cases of diaphyseal forearm fracture non-unions treated with autologous bone grafting and compression
plating. Thirty of thirty-one patients went on to bony union within 3.5 months of revision surgery.
Nadkarni et al. presented a case series of 11 patients with non-unions of various long bones initially managed with intradmedullary (IM) nail fixation. The authors successfully used locking compression plates while retaining the IM nails in the treatment of the nonunion in all cases.
Figure A shows an AP radiograph of a both bone forearm fracture. Figure B shows an AP and lateral radiograph of an atrophic non-union of the ulnar shaft. Illustration A shows a lateral x-ray of a fully healed radius and ulna after hardware removal 1 year after revision surgery.
Incorrect Answers:
Answer 1: With normal WBC, ESR and CRP levels, there is little reason to suspect an infectious non-union, thus, there is no indication for a bone scan at this time.
Answer 2 & 3: Immobilization will not treat the underlying issue of biology. Autologous bone grafting is necessary in the treatment of atrophic non-unions. Answer 4: A reamed IM nail does not provide adequate mechanical stability and is not used in the treatment of radius or ulna non-unions.
A 27 year-old patient sustains a fracture-dislocation of the acetabulum. Pelvic radiographs (Figures A and B) are taken at initial presentation and a CT scan (Figures C and D) is performed after reduction of the hip in the emergency room. What is the importance of the finding highlighted in the CT scan cuts?
1) Comminution indicates a better result with non-operative management
2) Significant marginal impaction could compromise the results of the surgical reduction if the joint surface is not properly restored
3) The impacted fracture segment will heal without fixation because it is not gapped or translated
4) The CT scan finding highlighted indicates osteochondral defects to the femoral head, which can be addressed arthroscopically
5) Intraarticular fracture fragments should be discarded from the surgical field, as incorporation of the fragments into the fixation construct leads to a high rate of avascular necrosis
The CT images shown in Figures C and D display significant marginal impaction of the joint surface.
Marginal impaction is common in posterior wall fractures and fracture-dislocations. Critical review of CT imaging of posterior wall fractures can help with preoperative planning for identifying impaction of the articular surface of the acetabulum. Restoration of the sphericity of the acetabulum to match that of the femoral head is important for successful outcome following ORIF of posterior wall fractures. A common surgical technique to accomplish joint surface restoration includes freeing the impacted articular segments, bone grafting of the void created to support the articular segments, and buttress plating of the posterior wall fracture fragments.
Patel et al. discuss the challenge of interpreting imaging of the acetabulum for assessing fracture characteristics that may significantly impact success or surgical intervention. These characteristics include: articular displacement, marginal impaction, incongruity of the joint surface, intra-articular fragments, and osteochondral injury to the femoral head. Based on expert review of images, determination of significant marginal impaction had a poor intraobserver reliability, as did each of the other modifiers listed.
Figures A and B are radiographs of the posterior wall fracture and hip dislocation. They do not show the large amount of marginal impaction of the acetabular surface. Figure C (coronal reconstruction) and Figure D (sagittal reconstruction) point out a large a amount of marginal impaction of the acetabular. Note the disruption of the joint surface on the intact portion of the acetabulum.
Incorrect answers:
Question 17High Yield
The primary function of structure “A” in Figure 29 is to limit
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur.
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 18High Yield
All of the following muscles are innervated by the median nerve except:
Explanation
Lumbricals 1 and 2 are innervated by the median nerve, in addition to the opponens pollicis brevis, abductor pollicis brevis, and flexor pollicis brevis.
Question 19High Yield
Arab Board Orthopedic MCQs Online Bank - Improve Your Knowledge and Skills
26/. A 14-year-old boy complains of pain along the medial aspect of the thigh, more severe at night. A bone scan reveals a double density sign with a maximum uptake in the center of a 1cm diameter lesion. The most likely diagnosis would be:
26/. A 14-year-old boy complains of pain along the medial aspect of the thigh, more severe at night. A bone scan reveals a double density sign with a maximum uptake in the center of a 1cm diameter lesion. The most likely diagnosis would be:
Explanation
No detailed explanation provided for this question.
Question 20High Yield
A 45-year-old construction worker sees a surgeon 23 days after sustaining an eccentric injury to his dominant right elbow. An MRI demonstrates a distal biceps tendon rupture with 5 cm of proximal retraction. In the operating room, the surgeon encounters good tissue quality but finds that primary repair can only be performed with the elbow hyperflexed to 70°. What is the best next step?
Explanation
DISCUSSION:
Distal biceps ruptures, although relatively less common in comparison with other upper extremity tendon injuries, still garner considerable attention in the orthopaedic literature. The mechanism of injury typically results from an eccentric extension load to a flexed elbow. A biceps-deficient arm can result in up to 40% loss of supination strength and up to 80% loss of supination endurance. A delay in diagnosis can compromise the ability to reduce the tendon back to its anatomic insertion without having to hyperflex the elbow. Current literature confirms the ability to safely proceed with primary repair even with the elbow flexed up to 100° without fear of developing a flexion contracture. With time, patients can anticipate restoration of full elbow extension. An interposition graft should be used for a poor residual tendon quality stump <4 cm in length and in cases of delay to surgery of >6 weeks. Biceps to brachialis tendon transfer does not restore supination
strength. Isolated debridement of the distal tendon would not be an appropriate treatment.
DISCUSSION:
Distal biceps ruptures, although relatively less common in comparison with other upper extremity tendon injuries, still garner considerable attention in the orthopaedic literature. The mechanism of injury typically results from an eccentric extension load to a flexed elbow. A biceps-deficient arm can result in up to 40% loss of supination strength and up to 80% loss of supination endurance. A delay in diagnosis can compromise the ability to reduce the tendon back to its anatomic insertion without having to hyperflex the elbow. Current literature confirms the ability to safely proceed with primary repair even with the elbow flexed up to 100° without fear of developing a flexion contracture. With time, patients can anticipate restoration of full elbow extension. An interposition graft should be used for a poor residual tendon quality stump <4 cm in length and in cases of delay to surgery of >6 weeks. Biceps to brachialis tendon transfer does not restore supination
strength. Isolated debridement of the distal tendon would not be an appropriate treatment.
Question 21High Yield
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 1 and

Explanation
■
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis. The cord compression is noted to be not only at the disk levels but also at the midvertebral body levels, and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1C2 on flexion-extension radiographs and subaxial subluxations.
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis. The cord compression is noted to be not only at the disk levels but also at the midvertebral body levels, and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1C2 on flexion-extension radiographs and subaxial subluxations.
Question 22High Yield
A 25-year-old woman has lower leg pain during exercise without numbness, tingling, or weakness. The symptoms resolve within 45 minutes of exercise cessation. Compartment pressure measurements obtained 1 minute after exercise are shown in Figure
Explanation
49
Exertional compartment syndrome involves an increase in compartment pressure caused by exercise or sports activity that restricts blood flow in the compartment, resulting in pain with continued activity. Compartment pressures of at least 15 mm Hg measured at rest, at least 30 mm Hg measured 1 minute after exercise, and at least 20 mm Hg measured 5 minutes after exercise are diagnostic. Surgical fasciotomy for exertional compartment syndrome is successful for the majority of patients, but recurrence rates as high as 20% have been reported. Scar formation within the fascial defect can result in recurrent symptoms and/or nerve entrapment, and recurrence is typically observed after an initial symptom-free period. In a series of 18 patients, recurrent symptoms occurred at a mean of 23.5 months after the index procedure. Other potential causes of recurrence include inadequate fascial release, failure to recognize involvement of other compartments, nerve compression, and misdiagnosis. Surgical complications after fasciotomy include hemorrhage leading to excessive fibrosis, neurovascular injury, and hematoma or seroma formation.
Exertional compartment syndrome involves an increase in compartment pressure caused by exercise or sports activity that restricts blood flow in the compartment, resulting in pain with continued activity. Compartment pressures of at least 15 mm Hg measured at rest, at least 30 mm Hg measured 1 minute after exercise, and at least 20 mm Hg measured 5 minutes after exercise are diagnostic. Surgical fasciotomy for exertional compartment syndrome is successful for the majority of patients, but recurrence rates as high as 20% have been reported. Scar formation within the fascial defect can result in recurrent symptoms and/or nerve entrapment, and recurrence is typically observed after an initial symptom-free period. In a series of 18 patients, recurrent symptoms occurred at a mean of 23.5 months after the index procedure. Other potential causes of recurrence include inadequate fascial release, failure to recognize involvement of other compartments, nerve compression, and misdiagnosis. Surgical complications after fasciotomy include hemorrhage leading to excessive fibrosis, neurovascular injury, and hematoma or seroma formation.
Question 23High Yield
What is the most common turf toe mechanism of injury?
Explanation
Turf toe, or capsuloligamentous injury to the first MTP joint, most commonly is caused by an axial load being applied to a fixed, dorsiflexed great toe with the heel off the ground. The external force causes further dorsiflexion of the great toe, leading to injury to the capsuloligamentous complex. A less common mechanism of turf toe is hyperplantarflexion of the great toe with valgus stress, which is seen in beach volleyball players.
RECOMMENDED READINGS
[Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. ](http://www.ncbi.nlm.nih.gov/pubmed/22049873)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22049873)
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
RECOMMENDED READINGS
[Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873. ](http://www.ncbi.nlm.nih.gov/pubmed/22049873)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22049873)
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
Question 24High Yield
A 30-year-old manual laborer is forced to jump from a collapsing building. He lands on his feet but experiences severe right foot pain. He presents with intact skin, moderate swelling and ecchymosis about the right heel, and global tenderness of the hindfoot. He is otherwise neurovascularly intact. Radiographs of his right foot are shown in Figures A-C. When considering surgery, which of the following is the
only undisputed difference when comparing nonoperative management of this injury to open reduction and internal fixation?
only undisputed difference when comparing nonoperative management of this injury to open reduction and internal fixation?



Explanation
An increased risk of surgical complications and reoperation is the only difference which has been found among patients who have undergone operative versus nonoperative management of displaced intra-articular calcaneal fractures (DIACFs). Differences between all other radiographic, subjective, and standardized functional outcomes remain disputed.
Despite a number of randomized control trials directly comparing operative to nonoperative management of DIACFs, controversy still surrounds the surgical indications. This is thought to be largely due to patient heterogeneity and the impact of age, gender, and other potentially confounding variables such as vocation and socioeconomic status. Furthermore, variability in surgical technique and functional outcome measures used preclude direct comparisons between studies as well as implementation of effective meta-analyses.
Functional outcomes following operative management have been shown to be worse in the older, obese, smoking, manual laborer, and worker’s compensation demographics, albeit only on subgroup analysis and not in direct comparison to a nonoperatively managed matched cohort. Some studies have suggested an improved ability to return to work and decreased risk of subtalar arthritis in operatively-managed DIACFs. However long-term investigations have shown conflicting findings on maintenance of radiographic indices including calcaneal height, width, and Bohler’s angle, regardless of management strategy.
Buckley et al. compared nonoperative management to open reduction and internal fixation of DIACFs. The authors found no significant difference in functional outcomes at a minimum of 2-year follow-up. However, after eliminating the worker’s compensation patients from the analysis, SF-36 and VAS scores were significantly better in the surgical cohort. They supported that the outcomes following operative management were in general superior.
Griffin et al. performed a randomized controlled trial comparing operative to nonoperative management of acute DIACFs. At a minimum two-year follow-up, the authors found that there was no significant difference in any of the functional outcome measures. However, the risk of complications and all-cause reoperation was perhaps not surprisingly significantly higher in the surgical
cohort.
Ibrahim et al. performed a 15-year follow-up of a randomized control trial evaluating the differences between nonoperative and operative management of DIACFs. The findings were similar to their index study, with no significant differences in any of the functional outcomes scores or radiographic parameters. The authors also found no difference in the rate of development in subtalar arthritis. This study has been criticized for the incomplete follow-up data in nearly two-thirds of the original cohort.
In a recent meta-analysis, Ning et al. evaluated studies comparing outcomes following operative versus nonoperative management of DIACFs. The authors found no significant differences in standardized functional outcomes, but they noted that heterogeneity in the outcome measures across studies may contribute to ambiguity in interpreting this finding. Conversely, operatively managed patients were more likely to return to work, but were also more likely to experience complications. The authors concluded that operative management for DIACFs was superior when displacement was outside of acceptable tolerances.
Figures:
Figure A is an AP radiographic of the right foot demonstrating a comminuted DIACF with subluxation of the calcaneocuboid joint.
Figure B is an oblique view of the right foot confirming a depressed posterior facet.
Figure C is a lateral view of the foot showing significant loss of calcaneal height and articular incongruity.
Incorrect Answers:
Answer 1: Previous studies have shown either a comparable or increased risk of development of subtalar arthritis in nonoperatively managed DIACFs.
Answer 3: Most comparative studies have found no significant difference in long-term subjective and functional outcomes between operatively and nonoperatively managed DIACFs. Subgroup analysis supports improved outcomes in select patient demographics with certain injury characteristics, but this remains disputed.
Answer 4: Nonoperatively managed DIACFs have been shown to have greater difficulty with shoe wear but generally a decreased likelihood of returning to work post-operatively.
Answer 5: Studies are conflicting and inconclusive regarding maintenance of radiographic indices such as Bohler’s angle, calcaneal height and width at longterm follow-up regardless of treatment method.
Despite a number of randomized control trials directly comparing operative to nonoperative management of DIACFs, controversy still surrounds the surgical indications. This is thought to be largely due to patient heterogeneity and the impact of age, gender, and other potentially confounding variables such as vocation and socioeconomic status. Furthermore, variability in surgical technique and functional outcome measures used preclude direct comparisons between studies as well as implementation of effective meta-analyses.
Functional outcomes following operative management have been shown to be worse in the older, obese, smoking, manual laborer, and worker’s compensation demographics, albeit only on subgroup analysis and not in direct comparison to a nonoperatively managed matched cohort. Some studies have suggested an improved ability to return to work and decreased risk of subtalar arthritis in operatively-managed DIACFs. However long-term investigations have shown conflicting findings on maintenance of radiographic indices including calcaneal height, width, and Bohler’s angle, regardless of management strategy.
Buckley et al. compared nonoperative management to open reduction and internal fixation of DIACFs. The authors found no significant difference in functional outcomes at a minimum of 2-year follow-up. However, after eliminating the worker’s compensation patients from the analysis, SF-36 and VAS scores were significantly better in the surgical cohort. They supported that the outcomes following operative management were in general superior.
Griffin et al. performed a randomized controlled trial comparing operative to nonoperative management of acute DIACFs. At a minimum two-year follow-up, the authors found that there was no significant difference in any of the functional outcome measures. However, the risk of complications and all-cause reoperation was perhaps not surprisingly significantly higher in the surgical
cohort.
Ibrahim et al. performed a 15-year follow-up of a randomized control trial evaluating the differences between nonoperative and operative management of DIACFs. The findings were similar to their index study, with no significant differences in any of the functional outcomes scores or radiographic parameters. The authors also found no difference in the rate of development in subtalar arthritis. This study has been criticized for the incomplete follow-up data in nearly two-thirds of the original cohort.
In a recent meta-analysis, Ning et al. evaluated studies comparing outcomes following operative versus nonoperative management of DIACFs. The authors found no significant differences in standardized functional outcomes, but they noted that heterogeneity in the outcome measures across studies may contribute to ambiguity in interpreting this finding. Conversely, operatively managed patients were more likely to return to work, but were also more likely to experience complications. The authors concluded that operative management for DIACFs was superior when displacement was outside of acceptable tolerances.
Figures:
Figure A is an AP radiographic of the right foot demonstrating a comminuted DIACF with subluxation of the calcaneocuboid joint.
Figure B is an oblique view of the right foot confirming a depressed posterior facet.
Figure C is a lateral view of the foot showing significant loss of calcaneal height and articular incongruity.
Incorrect Answers:
Answer 1: Previous studies have shown either a comparable or increased risk of development of subtalar arthritis in nonoperatively managed DIACFs.
Answer 3: Most comparative studies have found no significant difference in long-term subjective and functional outcomes between operatively and nonoperatively managed DIACFs. Subgroup analysis supports improved outcomes in select patient demographics with certain injury characteristics, but this remains disputed.
Answer 4: Nonoperatively managed DIACFs have been shown to have greater difficulty with shoe wear but generally a decreased likelihood of returning to work post-operatively.
Answer 5: Studies are conflicting and inconclusive regarding maintenance of radiographic indices such as Bohler’s angle, calcaneal height and width at longterm follow-up regardless of treatment method.
Question 25High Yield
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension.
REFERENCES: Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS: Two-bundle posterior cruciate ligament reconstruction: An in vitro analysis of graft placement and tension. Am J Sports Med 2000;28:833-845.
REFERENCES: Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS: Two-bundle posterior cruciate ligament reconstruction: An in vitro analysis of graft placement and tension. Am J Sports Med 2000;28:833-845.
Question 26High Yield
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of
Explanation
The radiograph reveals a reverse obliquely subtrochanteric/intertrochanteric fracture. Open reduction and internal fixation should be accomplished with a 95° fixed angle device. An intramedullary nail with screw fixation into the head is another possible technique. Either method should correct the varus deformity. Exchange of a high-angled screw and plate device to a longer side plate and bone grafting does not afford any improvement in the mechanical stability. Hardware removal and retrograde intramedullary nailing is not indicated for this level of a proximal femoral injury. Placement of an implantable bone stimulator may change local biologic factors but would not enhance mechanical stability. The patient’s femoral head is intact without signs of collapse; therefore, hardware removal, proximal femoral resection, and total hip arthroplasty are not warranted.
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Koval KJ, Zuckerman JD: Intertrochanteric fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1635-1681.
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Koval KJ, Zuckerman JD: Intertrochanteric fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1635-1681.
Question 27High Yield
..A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
- Pushing off an ipsilateral chair armrest to assist in standing up
Question 28High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season.
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
REFERENCES: Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Cantu RC: Criteria for return to competition after closed head injury, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby, 1991.
Question 29High Yield
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion.
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 30High Yield
Three years ago, a patient underwent successful resection of a third web space neuroma. She now presents with identical symptoms in the same location. She requests surgery because all attempts at conservative care have failed. Recommended treatment includes:
Explanation
The recurrence rate of a previously resected neuroma is approximately 15%. The deep transverse metatarsal ligament is involved in the pathogenesis of a primary, but not a recurrent, neuroma. None of the present symptoms suggests tarsal tunnel syndrome, although this may exist concurrently with a neuroma. Phenol has ablative neural properties, but it cannot be injected due to the local effect on tissue necrosis.
Question 31High Yield
Figures 1 through 3 are the MRI scans of a 15-year-old boy who sustained an injury to his shoulder after a fall while playing soccer. Following completion of a month-long rehabilitation program, he is able to tolerate sports-specific drills without symptoms. The patient is eager to return to play, as it is mid-season. How should the patient be counseled?
72
72
Explanation
Controversy exists regarding optimal treatment of an athlete with a shoulder instability event that has occurred during the competitive season. In the absence of large bony Bankart lesion or significant glenoid or humeral bone loss, particularly in athletes who are not involved in contact sports or throwing, return to sport may be attempted following a course of rehabilitation, provided the patient is asymptomatic following sports-specific drills. However, there is a significant risk of recurrence following nonoperative treatment in patients <20 years, and athletes should be counseled appropriately. Although motion-limiting braces may be associated with subjective improvement in stability, no studies have demonstrated a decreased rate of dislocation associated with bracing.
Question 32High Yield
Which of the following is not characteristic of Dupuytrenâs disease:
Explanation
Dupuytrenâs disease is characteristically unpredictable in its clinical progression. It may spontaneously resolve or quickly progress to advanced disease.
Question 33High Yield
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Tibial tubercle avulsion is an injury of the adolescent knee that most often occurs just before the end of growth. The fracture usually occurs with jumping, either at push-off or landing. This patient has a type III injury. In type III injuries, the articular surface is disrupted, and meniscal injury and compartment syndrome can occur. Open reduction is the treatment of choice, and anterior fasciotomy should be considered prophylactically at the time of surgery. Although the fracture heals with an anterior epiphysiodesis of the proximal tibia, little growth remains in this patient and no special handling of the physis is warranted.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 34High Yield
Isolated subtalar fusion:
Explanation
In 48 subtalar fusions followed for 5 years, 36% of patients developed ankle arthritis and 41% of patients developed transverse tarsal joint arthritis.
Question 35High Yield
Which pathology is associated with this condition?
Explanation
- Apophysitis of the tibial tubercle_
Question 36High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 37High Yield
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during
the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
of the knee.
Question 38High Yield
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time?
Explanation
■
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Nonsurgical treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise, without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Nonsurgical treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise, without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
Question 39High Yield
What is the most likely mechanism of injury?
Explanation
- Fall onto an outstretched elbow and hand
Question 40High Yield
A 47-year-old male sustains the closed injury seen in Figures A and B after failing to land a motorcycle jump. A post-reduction radiograph is seen in Figure C. Which of the following is the most appropriate treatment at this time?



Explanation
The clinical presentation and imaging studies are consistent with Hawkins II talar neck fracture, which by definition is a displaced talar neck fracture with subtalar dislocation/subluxation. Despite achieving an adequate reduction initially (shown in Figure C), there is no role for closed treatment of these unstable injuries, and the treatment of choice is open reduction and internal fixation.
The referenced article by Bibbo et al describes these injuries: 32% of subtalar joints are irreducible to closed means (half with soft tissue block, half with bony block to reduction), 88% have co-existing injuries of the ipsilateral foot, 89% have radiographic subtalar arthrosis at 5 years (62% symptomatic).
The referenced article by Bibbo et al describes these injuries: 32% of subtalar joints are irreducible to closed means (half with soft tissue block, half with bony block to reduction), 88% have co-existing injuries of the ipsilateral foot, 89% have radiographic subtalar arthrosis at 5 years (62% symptomatic).
Question 41High Yield
A 27-year-old male is involved in a motor vehicle accident and sustains the injury shown in Figures A through E. The articular surface is depressed 2 mm while there is 3 mm of condylar widening. Valgus instability of the knee is noted. Which of the following is most important to long-term success in surgical treatment of this case?



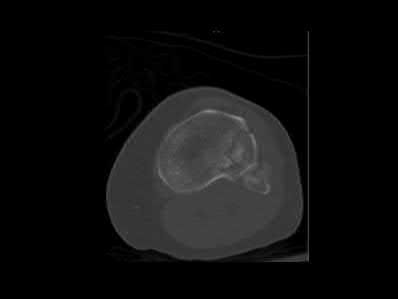




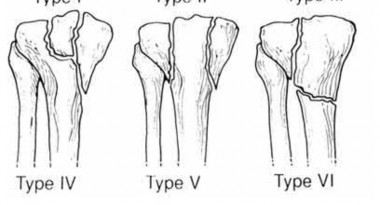
Explanation
The clinical presentation and imaging studies are consistent with a tibial plateau fracture. Restoration of joint stability has been shown to be the strongest predictor of long term outcomes.
Honkonen reviewed 131 tibial condyle fractures and determined that articular stepoff <3mm and tibial widening <5mm did not negatively effect outcomes. In contrast, 70% of knees with moderate to severe malalignment went on to functionally unacceptable outcomes. They suggested operative fixation for all medial uni and bicondylar fractures, any lateral fractures with >5 degrees of
valgus tilt, >3mm of articular depression, >5mm of condylar widening, or >5 degrees of valgus malalignment.
In the Marsh et al JAAOS symposium review, the authors noted that fractures with up to 10mm of articular depression and joint stability obtained acceptable functional outcomes. They also cited a 20 year follow-up which indicated that articular step-off alone was not a predictor of poor long-term results. More importantly, when instability is present with other factors, including step-off and central depression, poor results followed.
Illustrations A and B show the intraoperative films. Illustration C reviews the Schatzker classification system.
Honkonen reviewed 131 tibial condyle fractures and determined that articular stepoff <3mm and tibial widening <5mm did not negatively effect outcomes. In contrast, 70% of knees with moderate to severe malalignment went on to functionally unacceptable outcomes. They suggested operative fixation for all medial uni and bicondylar fractures, any lateral fractures with >5 degrees of
valgus tilt, >3mm of articular depression, >5mm of condylar widening, or >5 degrees of valgus malalignment.
In the Marsh et al JAAOS symposium review, the authors noted that fractures with up to 10mm of articular depression and joint stability obtained acceptable functional outcomes. They also cited a 20 year follow-up which indicated that articular step-off alone was not a predictor of poor long-term results. More importantly, when instability is present with other factors, including step-off and central depression, poor results followed.
Illustrations A and B show the intraoperative films. Illustration C reviews the Schatzker classification system.
Question 42High Yield
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
A complete tear of the distal biceps brachii most often occurs from a large, rapid eccentric elbow extension load. A pop or tearing sensation usually occurs, and a palpable defect in the antecubital fossa is often present on examination. The treatment of choice is a direct primary repair by a two-incision technique. If left unrepaired, the most disabling consequence is the loss of forearm supination strength. It is unlikely that significant elbow or forearm motion will be lost if the rupture is left unrepaired and early motion exercises are initiated. Elbow flexion strength tends to return with time, but the loss of forearm supination strength remains problematic.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 43High Yield
A 26-year-old male sustains a traction injury to his left arm after a motorcycle crash with resulting weakness in this left upper extremity. An electromyography (EMG) done shows normal cervical paraspinal muscle activity. Which of the following statements is true regarding this injury?
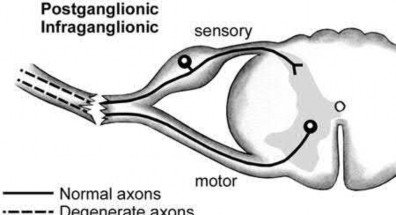
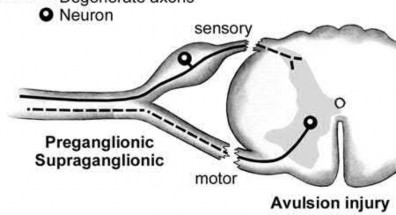
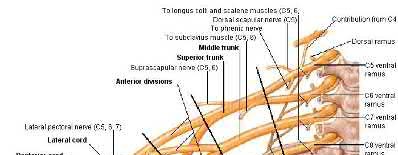
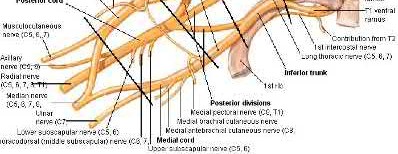
Explanation
Normal cervical paraspinal muscle activity on EMG is characteristic of a postganglionic injury.
Determining whether a brachial plexus injury is pre- or post-ganglionic has important treatment and prognostic implications. Findings that suggest a preganglionic lesion include Horner syndrome (ptosis, miosis, anhidrosis), a medially winged scapula, loss of paraspinal musculature activity on EMG, and a normal histamine test. These injuries tend to have a worse prognosis than post-ganglionic lesions, which show an abnormal histamine test and intact cervical paraspinal activity on EMG.
Moran et al. review brachial plexus injuries. They recommend a baseline EMG for non-operative injuries at 3-4 weeks time after Wallerian degeneration has occurred.
Shin et al. also review brachial plexus injuries. While an MRI can visualize much of the brachial plexus and may be able to demonstrate neuromas, a CT myelogram still remains the primary mode of radiographic evaluation for nerve root avulsion in the acute setting.
Illustration A shows the difference between a pre- and post-ganglionic lesion. Illustration B shows the brachial plexus for reference.
Incorrect Answers:
Answer 1: This is the definition of a pre-ganglionic lesion.
Answer 2: Horner syndrome is typically found in patients with pre-ganglionic lesions.
Answer 4: Neurotization is usually only considered for pre-ganglionic lesions. Answer 5: Post-ganglionic injuries show an abnormal histamine test.
Determining whether a brachial plexus injury is pre- or post-ganglionic has important treatment and prognostic implications. Findings that suggest a preganglionic lesion include Horner syndrome (ptosis, miosis, anhidrosis), a medially winged scapula, loss of paraspinal musculature activity on EMG, and a normal histamine test. These injuries tend to have a worse prognosis than post-ganglionic lesions, which show an abnormal histamine test and intact cervical paraspinal activity on EMG.
Moran et al. review brachial plexus injuries. They recommend a baseline EMG for non-operative injuries at 3-4 weeks time after Wallerian degeneration has occurred.
Shin et al. also review brachial plexus injuries. While an MRI can visualize much of the brachial plexus and may be able to demonstrate neuromas, a CT myelogram still remains the primary mode of radiographic evaluation for nerve root avulsion in the acute setting.
Illustration A shows the difference between a pre- and post-ganglionic lesion. Illustration B shows the brachial plexus for reference.
Incorrect Answers:
Answer 1: This is the definition of a pre-ganglionic lesion.
Answer 2: Horner syndrome is typically found in patients with pre-ganglionic lesions.
Answer 4: Neurotization is usually only considered for pre-ganglionic lesions. Answer 5: Post-ganglionic injuries show an abnormal histamine test.
Question 44High Yield
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular
reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 45High Yield
Slide 1 Slide 2 Slide 3
A 65-year-old man has severe foot pain. His plain radiograph is shown in Slide 1, and a needle biopsy specimen in Slides 2 and
3/. The most appropriate treatment for this patient is:
A 65-year-old man has severe foot pain. His plain radiograph is shown in Slide 1, and a needle biopsy specimen in Slides 2 and
3/. The most appropriate treatment for this patient is:
Explanation
Gout is caused by the deposition of monosodium urate crystals in tissues, typically around joints. Common locations of gout include the great toe, heel, ankle, and knee. In approximately 50% of patients, the first affected location is the great toe. Gout commonly occurs inside a joint for two reasons - synovial fluid is a poorer solvent than plasma and lower temperatures (as in peripheral joints) favor crystallization.
Neutrophils ingest the crystals and release potent lysosomal enzymes. Punched lesions may be seen on radiographs in chroniCcases, and one can often see an overlying lip of cortex at the edge of the lesion.
Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
In this patient, the joint space is preserved on the plain radiographs. The biopsy specimen has the characteristiCfeatures of gout - acellular amorphous material, macrophages, and foreign body giant cells.
The treatment of gout includes nonsteroidal anti-inflammatory drugs and medications such as allopurinol and colchicines, which lower hyperuricemia.
Neutrophils ingest the crystals and release potent lysosomal enzymes. Punched lesions may be seen on radiographs in chroniCcases, and one can often see an overlying lip of cortex at the edge of the lesion.
Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
In this patient, the joint space is preserved on the plain radiographs. The biopsy specimen has the characteristiCfeatures of gout - acellular amorphous material, macrophages, and foreign body giant cells.
The treatment of gout includes nonsteroidal anti-inflammatory drugs and medications such as allopurinol and colchicines, which lower hyperuricemia.
Question 46High Yield
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain.
Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
arthroscopic debridement and lavage).
Question 47High Yield
A 12-year-old boy with a history of Duchenne muscular dystrophy is being evaluated for progressive scoliosis. He now has 35° long thoracolumbar scoliosis, which was 20° only 6 months ago. He has a pelvic obliquity of 20°. He is a full-time wheelchair user. What is the most appropriate next step for this patient's spine deformity care?
Explanation
■
Duchenne muscular dystrophy is a recessive, X-linked, inherited disorder. Most (90%) untreated boys with this disorder develop progressive scoliosis, secondary to muscle weakness, after becoming full-time wheelchair users. Several studies suggest that the long-term use of glucocorticoids has prolonged effects against detrimental aspects of Duchenne muscular dystrophy.
The widespread use of glucocorticoids for patients with Duchenne muscular dystrophy has dramatically decreased the development of scoliosis and need for subsequent surgical intervention. There is still much to be learned about the impact of glucocorticoids on the spine, including the duration of glucocorticoid treatment needed to reduce the risk of a progressive curve and whether this treatment merely delays the onset. In recent studies in which researchers followed young men into their twenties, it was shown that glucocorticoids protect against the development of scoliosis well past skeletal maturity.
Posterior spinal instrumentation and fusion are recommended in those whose spinal curve is >20°, are prepubertal, and are not on glucocorticoids because progression of the curve is expected. Although patients taking glucocorticoids may still develop a scoliosis, it is reasonable to wait until progression is documented. When surgery is done to correct scoliosis, it is recommended that those with a pelvic obliquity of >15° also have stabilization and fusion into the pelvis. This helps patients with seating and positioning. Fusion to the L5 is sufficient for patients who do not have a severe pelvic obliquity. With surgical intervention of the spine, the aim is to reduce the patient’s pain, improve his ability to sit comfortably, and prevent further progression.
Duchenne muscular dystrophy is a recessive, X-linked, inherited disorder. Most (90%) untreated boys with this disorder develop progressive scoliosis, secondary to muscle weakness, after becoming full-time wheelchair users. Several studies suggest that the long-term use of glucocorticoids has prolonged effects against detrimental aspects of Duchenne muscular dystrophy.
The widespread use of glucocorticoids for patients with Duchenne muscular dystrophy has dramatically decreased the development of scoliosis and need for subsequent surgical intervention. There is still much to be learned about the impact of glucocorticoids on the spine, including the duration of glucocorticoid treatment needed to reduce the risk of a progressive curve and whether this treatment merely delays the onset. In recent studies in which researchers followed young men into their twenties, it was shown that glucocorticoids protect against the development of scoliosis well past skeletal maturity.
Posterior spinal instrumentation and fusion are recommended in those whose spinal curve is >20°, are prepubertal, and are not on glucocorticoids because progression of the curve is expected. Although patients taking glucocorticoids may still develop a scoliosis, it is reasonable to wait until progression is documented. When surgery is done to correct scoliosis, it is recommended that those with a pelvic obliquity of >15° also have stabilization and fusion into the pelvis. This helps patients with seating and positioning. Fusion to the L5 is sufficient for patients who do not have a severe pelvic obliquity. With surgical intervention of the spine, the aim is to reduce the patient’s pain, improve his ability to sit comfortably, and prevent further progression.
Question 48High Yield
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph
is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg
length, what is the most appropriate surgical plan?
is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg
length, what is the most appropriate surgical plan?

Explanation
---
DISCUSSION:
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
DISCUSSION:
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 49High Yield
Figure 1
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
Explanation
The prognosis following fracture dislocation of the navicular is not good regardless of treatment. Although one may be tempted to perform an open reduction and immediate primary talonavicular arthrodesis, this is not necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
Question 50High Yield
A 22-year-old male sustains the injury shown in Figure A. When placing an antegrade intramedullary nail with manual traction in a supine position, which of the following is true when compared to placement of a nail using a fracture table?

Explanation
Figure A shows a proximal (supraisthmal) femoral shaft fracture.
The referenced article by Stephen et al is a randomized controlled trial between manual traction and fracture-table traction for the reduction and nailing of femoral shaft fractures in terms of quality of the reduction, operative time, complications, and functional status of the patient in eighty-seven patients. Internal malrotation was significantly more common when the fracture table had been used: twelve (29%) of the forty-two femora were internally rotated by >10° compared with three (7%) of the forty-five treated with manual traction. Mean operative time was also less in the manual traction group.
The referenced study by Wolinsky et al also found that use of a traction table significantly increased the anesthesia time, total operating room time, prep and drape time, and overall surgical time as compared to manual traction.
The referenced article by Stephen et al is a randomized controlled trial between manual traction and fracture-table traction for the reduction and nailing of femoral shaft fractures in terms of quality of the reduction, operative time, complications, and functional status of the patient in eighty-seven patients. Internal malrotation was significantly more common when the fracture table had been used: twelve (29%) of the forty-two femora were internally rotated by >10° compared with three (7%) of the forty-five treated with manual traction. Mean operative time was also less in the manual traction group.
The referenced study by Wolinsky et al also found that use of a traction table significantly increased the anesthesia time, total operating room time, prep and drape time, and overall surgical time as compared to manual traction.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon