Orthopedics Hyperguide Review | Dr Hutaif General Ortho -...
14 Apr 2026
50 min read
61 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedics Hyperguide Review | Dr Hutaif Gen...
00:00
Start Quiz
Question 1High Yield
Which type of thoracolumbar injury typically involves all three columns, is most mechanically unstable, and is most associated with complete spinal cord injury?
Explanation
■
Translation-rotation injuries typically yield fracture dislocations. This injury pattern involves the disruption of skeletal and ligamentous elements of the spine to cause a maximum loss of stability, subsequent deformity in three planes (coronal, axial, and sagittal), and catastrophic neurologic injury.
Compression injuries occur when a force is applied in flexion and injures the anterior column. Compression injuries are usually stable and rarely have neurologic sequelae. Burst fractures occur through axially applied forces, which in turn cause injury to the anterior and middle columns of the vertebrae at minimum. Neurologic injury can occur through direct compression of the neural elements by bone fragments or hematoma or by absorption of the transferred energy. Flexion distraction injuries typically occur as forces are transmitted from anterior to posterior, causing injury to the middle and posterior columns.
Translation-rotation injuries typically yield fracture dislocations. This injury pattern involves the disruption of skeletal and ligamentous elements of the spine to cause a maximum loss of stability, subsequent deformity in three planes (coronal, axial, and sagittal), and catastrophic neurologic injury.
Compression injuries occur when a force is applied in flexion and injures the anterior column. Compression injuries are usually stable and rarely have neurologic sequelae. Burst fractures occur through axially applied forces, which in turn cause injury to the anterior and middle columns of the vertebrae at minimum. Neurologic injury can occur through direct compression of the neural elements by bone fragments or hematoma or by absorption of the transferred energy. Flexion distraction injuries typically occur as forces are transmitted from anterior to posterior, causing injury to the middle and posterior columns.
Question 2High Yield
Which two quadrants of the acetabulum are most at risk for injury by screws during fixation of total hip arthroplasty (THA):
Explanation
The acetabular quadrant system described by Wasielewski and colleagues is useful for determining the location of planned acetabular screw fixation in THA to avoid neurovascular complications. The quadrants are formed by drawing a line from the anterior-superior iliaCspine through the center of the acetabulum and bisecting that line at the center of the acetabulum to form four equal quadrants. The line from the anterior-superior iliaCspine to the center of the acetabulum serves as the dividing line between anterior and posterior, and the bisecting line as the division between superior and inferior.
In cadaver studies, the posterior-superior and posterior-inferior quadrants were shown to have the thickest bone and best potential for obtaining secure fixation with the least risk for injury to vessels. The anterior-superior quadrant (the quadrant of death) and the anterior-inferior quadrant were shown to be the most dangerous quadrants for fixation due to the thin bone and close proximity of the vessels to bone in that region
In cadaver studies, the posterior-superior and posterior-inferior quadrants were shown to have the thickest bone and best potential for obtaining secure fixation with the least risk for injury to vessels. The anterior-superior quadrant (the quadrant of death) and the anterior-inferior quadrant were shown to be the most dangerous quadrants for fixation due to the thin bone and close proximity of the vessels to bone in that region
Question 3High Yield
The clinical photograph of the hand of a 72-year-old woman who sustained a
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
Explanation
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Doyle JR, Blythe WF: Anatomy of the flexor tendon sheath and pulleys of the thumb. J Hand Surg 1977;2:149-151.
#
Question 4High Yield
A 36-year-old woman dislocated her elbow 6 months ago. The elbow was congruently reduced and rehabilitated. She continues to have a sense of painful clunking in her elbow when she pushes up from a chair with forearm supination, but not pronation. What structure did not heal properly?
Explanation
The patient is showing signs of posterolateral rotatory instability after elbow dislocation. The lateral ulnar collateral ligament is responsible for stabilizing the elbow against this type of instability. The posterior and anterior bands of the medial collateral ligament are primarily resistors of valgus load, with the anterior band being the most significant contributor. The radial collateral ligament does not control the posterolateral rotatory instability described.
Question 5High Yield
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of
Explanation
Chronic rotator cuff tears should be nonsurgically managed initially with a strengthening program. A cortisone injection may reduce inflammation. Surgery is reserved for patients who continue to have pain and lose sleep despite the use of physical therapy. Blood tests for infection or inflammation are nonspecific. Arthroscopy may play a role, but surgical replacement is reserved for advanced cases.
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
Question 6High Yield
Which of the following is a significant side effect of biphosphonates (e.g., alendronate):
Explanation
The most significant side effect of biphosphonates is esophagitis and dyspepsia. Biphosphonates must be taken on an empty stomach with no oral intake for 30 minutes. In addition, patients should remain upright
Question 7High Yield
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation?
Explanation
DISCUSSION: Cadaveric studies have demonstrated the important role of the posterior horn of the medial meniscus in stabilizing the anterior cruciate ligament-deficient knee with significantly greater resultant force in the medial meniscus when subjected to anterior tibial loads. The posterior horn of the medial meniscus is thought to limit anterior tibial translation by acting as a buttress by wedging against the posterior aspect of the medial femoral condyle. The other soft tissues mentioned do not play any significant role in prevention of anterior tibial translation in the anterior cruciate ligament-deficient knee.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 200.
Allen CR, Wong EK, Livesay GA, et al: Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res 2000;18:109-115.
Levy IM, Torzilli PA, Warren RF: The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am 1982;64:883-888.
Figure 31
DISCUSSION: Cadaveric studies have demonstrated the important role of the posterior horn of the medial meniscus in stabilizing the anterior cruciate ligament-deficient knee with significantly greater resultant force in the medial meniscus when subjected to anterior tibial loads. The posterior horn of the medial meniscus is thought to limit anterior tibial translation by acting as a buttress by wedging against the posterior aspect of the medial femoral condyle. The other soft tissues mentioned do not play any significant role in prevention of anterior tibial translation in the anterior cruciate ligament-deficient knee.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 200.
Allen CR, Wong EK, Livesay GA, et al: Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res 2000;18:109-115.
Levy IM, Torzilli PA, Warren RF: The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am 1982;64:883-888.
Figure 31
Question 8High Yield
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
Question 9High Yield
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
Explanation
- Anterior shoulder subluxation_
Question 10High Yield
The hereditary pattern for Holt-Oram syndrome is:
Explanation
Holt-Oram syndrome is inherited in an autosomal dominant manner.
Question 11High Yield
A newborn baby has a foot that is dorsiflexed and in valgus. The differential diagnosis includes all of the following conditions except:
Explanation
The foot in a patient with tibial hemimelia does not resemble the other four conditions described; the foot is in equinus and varus.
C alcaneovalgus foot is dorsiflexed and everted through the axis of the ankle joint. A vertical talus has excessive forefoot dorsiflexion and valgus.
A patient with an L5 myelomeningocele may have this appearance due to activity of the dorsiflexors and evertors, with absent power in the plantarflexors and invertors.
Due to the posteromedial bow in the tibia, the foot may appear dorsiflexed and in valgus.
C alcaneovalgus foot is dorsiflexed and everted through the axis of the ankle joint. A vertical talus has excessive forefoot dorsiflexion and valgus.
A patient with an L5 myelomeningocele may have this appearance due to activity of the dorsiflexors and evertors, with absent power in the plantarflexors and invertors.
Due to the posteromedial bow in the tibia, the foot may appear dorsiflexed and in valgus.
Question 12High Yield
Which of the following injuries is most likely associated with the fracture seen in Figure A?



Explanation
Lateral meniscal tears are most commonly associated with Schatzker II tibial plateau fractures (split/depressed).
Soft tissue pathology is common in tibial plateau fractures. In general, fractures that are largely displaced and/or a result of high energy trauma are more likely to have associated soft tissue pathology. A majority of meniscal injuries that occur in the setting of tibial plateau fractures are meniscocapsular detachments. This has important implications for healing (more reliable healing in the vascular zone). Additionally, the meniscus usually remains in close contact with the femoral condyle, while the tibial plateau widens around it. It is generally agreed upon that meniscal tears should be repaired, if possible, at the time of internal fixation to decrease the likelihood of postraumatic arthritis.
Gardner et al. review 62 patients with Schatzker II tibial plateau fractures that had an MRI preoperatively. For displaced fractures, the incidence of lateral meniscal tears was 83%, while the incidence of lateral collateral and posterior cruciate ligament injuries was 30%.
Ringus et al. attempted to determine if the degree of lateral tibial plateau fracture depression on computed tomography (CT) images predicted the presence of lateral meniscus tears. Fractures with > 9mm depression had an eight-fold increase in lateral meniscal tears, and those younger than 48 years-old had a four-fold increase in lateral meniscal tears.
Illustration A shows an MRI of a Schatzker II tibial plateau fracture with a lateral meniscal detachment and a medial meniscal tear. Illustration B shows the Schatzker Classification, I-VI.
Incorrect Answers:
Answers 1, 3, 4, 5: While these soft tissue injuries may occur, lateral meniscal tears are more common for this particular fracture pattern.
Soft tissue pathology is common in tibial plateau fractures. In general, fractures that are largely displaced and/or a result of high energy trauma are more likely to have associated soft tissue pathology. A majority of meniscal injuries that occur in the setting of tibial plateau fractures are meniscocapsular detachments. This has important implications for healing (more reliable healing in the vascular zone). Additionally, the meniscus usually remains in close contact with the femoral condyle, while the tibial plateau widens around it. It is generally agreed upon that meniscal tears should be repaired, if possible, at the time of internal fixation to decrease the likelihood of postraumatic arthritis.
Gardner et al. review 62 patients with Schatzker II tibial plateau fractures that had an MRI preoperatively. For displaced fractures, the incidence of lateral meniscal tears was 83%, while the incidence of lateral collateral and posterior cruciate ligament injuries was 30%.
Ringus et al. attempted to determine if the degree of lateral tibial plateau fracture depression on computed tomography (CT) images predicted the presence of lateral meniscus tears. Fractures with > 9mm depression had an eight-fold increase in lateral meniscal tears, and those younger than 48 years-old had a four-fold increase in lateral meniscal tears.
Illustration A shows an MRI of a Schatzker II tibial plateau fracture with a lateral meniscal detachment and a medial meniscal tear. Illustration B shows the Schatzker Classification, I-VI.
Incorrect Answers:
Answers 1, 3, 4, 5: While these soft tissue injuries may occur, lateral meniscal tears are more common for this particular fracture pattern.
Question 13High Yield
A 25-year-old laborer sustains a transverse fracture of the proximal 25% of the scaphoid. CT reconstructions reveal a 1-mm fracture gap. What is the most appropriate treatment?
Explanation
A higher risk of nonunion and the need for prolonged immobilization is seen after nonsurgical management of proximal pole fractures of the scaphoid. Because of the relatively poor blood supply of the proximal pole, surgical treatment with a compression screw is advocated for fractures of the proximal third of the scaphoid.
REFERENCES: Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Ring D, Jupiter JB, Herndon JH: Acute fractures of the scaphoid. J Am Acad Orthop Surg 2000;8:225-231.
REFERENCES: Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Ring D, Jupiter JB, Herndon JH: Acute fractures of the scaphoid. J Am Acad Orthop Surg 2000;8:225-231.
Question 14High Yield
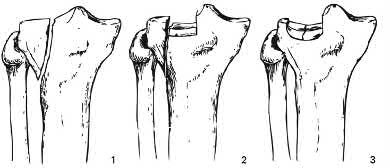
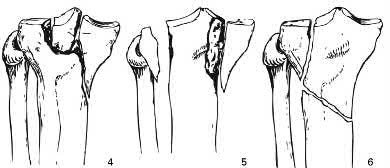
Figure 1 is the radiograph of a 48-year-old man. He is of normal height and weight, medically healthy,and in good physical condition. What is the best treatment option?
Explanation
Immediate open reduction and internal fixation of this fracture is required to prevent necrosis of the overlying soft tissue. Because of the power and proximal pull of the triceps surae,nonsurgical management is not indicated with avulsion fractures of the calcaneus. It leaves a large void that will not fill in with bone, leaves the Achilles tendon weak, and has a high complication rate, especially skin breakdown. The Achilles tendon is securely attached to the fractured tuberosity. Bone-to-bone healing is more reliable than detaching the Achilles tendon from the tuberosity and reattaching it to the remainder of the calcaneus. Because of the size of the avulsed fragment, it will be difficult to correctly tension the tendon if the fractured piece is excised. Percutaneous Kirschner wire fixation is not strong enough to provide a stable fixation of the tuberosity, especially in view of the power of the Achilles tendon contracture.
Question 15High Yield
The clinical variable found to be associated with a higher risk of complications following open reduction and internal fixation of unstable ankle fractures in diabetic patients was:
Explanation
A retrospective Level IV study followed 84 patients with diabetes who underwent open reduction internal fixation of unstable ankle fractures. After analyzing multiple patient factors including sex, fracture pattern, open or closed injury, nephropathy, hypertension, vasculopathy, peripheral neuropathy, and diabetic control (insulin-dependent compared with non-insulin- dependent), the only factors that predicted a higher rate of complications were vasculopathy and peripheral neuropathy. There was a 12% rate of postoperative infection and an overall 14% rate of complications.
Question 16High Yield
The primary function of structure “A” in Figure 29 is to limit
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur.
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 17High Yield
Regarding the management of web space abscess, which of the following statements is not true:
Explanation
Transverse incisions can lead to contractures that limit finger abduction. Leaving wounds open allow for continued drainage. If preferred, closed suction drains can be used after closure of the wound. All devitalized tissue must be debrided and all signs of infection removed and irrigated copiously. Early motion is encouraged to prevent stiffness.
Question 18High Yield
Alumina = 340
Illustration A shows a stress vs. strain curve. Young Modulus of Elasticity is defined is defined as the slope of the line in the elastic zone
A prospective cohort study is performed looking at the relationship between blood transfusions and the risk of developing hepatitis C. In the transfused group (study group) of 595 patients, 75 patients develop hepatitis C. In the non- transfused group (control group) of 712 people, 16 people contract hepatitis C. What is the relative risk of developing hepatitis C with a transfusion.
Illustration A shows a stress vs. strain curve. Young Modulus of Elasticity is defined is defined as the slope of the line in the elastic zone
A prospective cohort study is performed looking at the relationship between blood transfusions and the risk of developing hepatitis C. In the transfused group (study group) of 595 patients, 75 patients develop hepatitis C. In the non- transfused group (control group) of 712 people, 16 people contract hepatitis C. What is the relative risk of developing hepatitis C with a transfusion.






Explanation
Vitronectin, integrin avß3, assists osteoclasts to attach to bone.
Osteoclasts attach to bone surfaces by means of integrins and then seal the space below. A ruffled border is then created and bone matrix is removed by proteolytic digestion through the lysosomal enzyme cathepsin K.
Incorrect Answers:
: RANK is a receptor on osteoclasts that when activated by RANKL stimulates osteoclasts. RANKL is found on osteoblasts.
Answer 3: Osteoprotegerin (OPG) decreases osteoclast differentiation by it’s interaction with RANKL (receptor activator of NF-kappaB ligand). OPG is made by osteoblasts and binds to RANKL (RANK Ligand) to competitively inhibit RANK binding.
Answer 4: PDGF (Platelet Derived Growth Factor) is involved in fracture healing. It is chemotactic and attracts inflammatory cells to the fracture site and is important in early fracture healing, especially the hematoma formation. Answer 5: TGF-B (transforming growth factor Beta) induces mesenchymal cells
to produce type II collagen & proteoglycans. It is important in the early stages of fracture callus formation.
Which of the following is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation?
1) Genetic drift
2) Expansion
3) Mendelian inheritance
4) Anticipation
5) Phenotypic plasticity
Anticipation is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation. In most cases, an increase of severity of symptoms is also noted. Anticipation is common in trinucleotide repeat disorders such as Huntington's disease, myotonic dystrophy, Friedreich ataxia, and Fragile X syndrome. Illustration A shows the genetics of the trinucleotide repeat disorders.
A 58-year-old female complains of continued pain and swelling 6 months following total knee arthroplasty. She describes a burning pain that radiates from the knee down the anterior compartment of the leg. The pain arises sporadically and is associated with swelling,
**sweating, and a purplish hue of the leg. Knee radiographs are**
provided in Figures A and B. Aspiration is negative for infection. Which of the following is the best management?
1) Lumbar spine MRI to evaluate for radiculopathy of the L3 nerve root
2) Alpha-adrenergic blockers, physical therapy, tactile discrimination training, and graded motor imagery
3) Surgical exploration of the knee
4) Surgical debridement, pulsatile irrigation, tissue sampling for culture/biopsy, and polyethylene exchange
5) Magnetic resonance arthrogram (MRA) with intra-articular contrast and diagnostic steroid injection
The clinical scenario and radiographs are consistent with a patient who is experiencing complex regional pain syndrome following total knee arthroplasty (TKA).
Complex regional pain syndrome, which was previously known as reflex sympathetic dystrophy, is characterized by intense burning pain, stiffness, swelling, and discoloration of the legs, feet, arms and hand (most common). Current treatment modalities are multi- modal and include GABA agonists, alpha-blockers, beta-blockers, physical therapy, occupational therapy, graded motor imagery, tactile discrimination treatments, sympathectomy, local anesthetics, and even spinal cord stimulators.
Mont et al. reported limited success in 27 patients who had surgical exploration of radiographically normal knees following TKA with unexplained pain. Outcomes were especially poor in patients who had achieved adequate range of motion and continued to have pain prior to surgical exploration. Patients with decreased range of motion who achieved improvement in motion postoperatively also demonstrated great relief of pain.
Figure A and B are AP and lateral radiographs of a well-fixed total knee
arthroplasty.
Incorrect Answers:
Answer 1: An MRI of the lumbar spine is not indicated in this patient as their symptoms are suggestive of complex regional pain syndrome, not an L3 radiculopathy.
Answer 3: Surgical exploration of radiographically normal knees following TKA for patients with unexplained pain has been found to have limited success. Answer 4: Surgical irrigation and debridement is not indicated in this setting as the patient is not presenting with symptoms suggestive of infection.
Answer 5: An MRA with intra-articular contrast and diagnostic steroid is not indicated in the setting of complex regional pain syndrome.
Which system of lacunar networks is used among osteocytes to communicate?
1) Volkmann canals
2) Cement lines
3) Secondary messenger systems
4) Canaliculi
5) Haversian canals
Canaliculi are a system within the lacunar network used by osteocytes to communicate with each other.
Osteocytes have numerous cell processes (filopodia) that project through the canaliculi and connect to each other via gap junctions (see Illustrations B and C). Through this network osteocytes establish contact and communication with adjacent osteocytes for exchange of nutrients and metabolic waste. They are oriented in a radial fashion around the central Haversian canal.
Knothe Tate et al described the changes occuring in different pathologies. In normal bone, osteocyte connectivity is high and processes are oriented in the direction of blood supply. In osteoporotic bone, there is decreased osteocyte connectivity and orientation and tortuous cell processes. In osteoarthritic bone, there is decreased osteocyte viability and connectivity, but preserved
orientation. In osteomalacic bone, there is preserved viability and connectivity, but tortuous and chaotic cell processes.
Illustration A shows the structure of compact and spongy bone. Illustration B shows gap junctions between cells. Illustration C shows secondary messengers crossing gap junctions.
Incorrect Answers
Vitronectin, integrin avß3, assists osteoclasts to attach to bone.
Osteoclasts attach to bone surfaces by means of integrins and then seal the space below. A ruffled border is then created and bone matrix is removed by proteolytic digestion through the lysosomal enzyme cathepsin K.
Incorrect Answers:
: RANK is a receptor on osteoclasts that when activated by RANKL stimulates osteoclasts. RANKL is found on osteoblasts.
Answer 3: Osteoprotegerin (OPG) decreases osteoclast differentiation by it’s interaction with RANKL (receptor activator of NF-kappaB ligand). OPG is made by osteoblasts and binds to RANKL (RANK Ligand) to competitively inhibit RANK binding.
Answer 4: PDGF (Platelet Derived Growth Factor) is involved in fracture healing. It is chemotactic and attracts inflammatory cells to the fracture site and is important in early fracture healing, especially the hematoma formation. Answer 5: TGF-B (transforming growth factor Beta) induces mesenchymal cells
to produce type II collagen & proteoglycans. It is important in the early stages of fracture callus formation.
Which of the following is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation?
1) Genetic drift
2) Expansion
3) Mendelian inheritance
4) Anticipation
5) Phenotypic plasticity
Anticipation is a phenomenon whereby the symptoms of a genetic disorder become apparent at an earlier age as it is passed on to the next generation. In most cases, an increase of severity of symptoms is also noted. Anticipation is common in trinucleotide repeat disorders such as Huntington's disease, myotonic dystrophy, Friedreich ataxia, and Fragile X syndrome. Illustration A shows the genetics of the trinucleotide repeat disorders.
A 58-year-old female complains of continued pain and swelling 6 months following total knee arthroplasty. She describes a burning pain that radiates from the knee down the anterior compartment of the leg. The pain arises sporadically and is associated with swelling,
**sweating, and a purplish hue of the leg. Knee radiographs are**
provided in Figures A and B. Aspiration is negative for infection. Which of the following is the best management?
1) Lumbar spine MRI to evaluate for radiculopathy of the L3 nerve root
2) Alpha-adrenergic blockers, physical therapy, tactile discrimination training, and graded motor imagery
3) Surgical exploration of the knee
4) Surgical debridement, pulsatile irrigation, tissue sampling for culture/biopsy, and polyethylene exchange
5) Magnetic resonance arthrogram (MRA) with intra-articular contrast and diagnostic steroid injection
The clinical scenario and radiographs are consistent with a patient who is experiencing complex regional pain syndrome following total knee arthroplasty (TKA).
Complex regional pain syndrome, which was previously known as reflex sympathetic dystrophy, is characterized by intense burning pain, stiffness, swelling, and discoloration of the legs, feet, arms and hand (most common). Current treatment modalities are multi- modal and include GABA agonists, alpha-blockers, beta-blockers, physical therapy, occupational therapy, graded motor imagery, tactile discrimination treatments, sympathectomy, local anesthetics, and even spinal cord stimulators.
Mont et al. reported limited success in 27 patients who had surgical exploration of radiographically normal knees following TKA with unexplained pain. Outcomes were especially poor in patients who had achieved adequate range of motion and continued to have pain prior to surgical exploration. Patients with decreased range of motion who achieved improvement in motion postoperatively also demonstrated great relief of pain.
Figure A and B are AP and lateral radiographs of a well-fixed total knee
arthroplasty.
Incorrect Answers:
Answer 1: An MRI of the lumbar spine is not indicated in this patient as their symptoms are suggestive of complex regional pain syndrome, not an L3 radiculopathy.
Answer 3: Surgical exploration of radiographically normal knees following TKA for patients with unexplained pain has been found to have limited success. Answer 4: Surgical irrigation and debridement is not indicated in this setting as the patient is not presenting with symptoms suggestive of infection.
Answer 5: An MRA with intra-articular contrast and diagnostic steroid is not indicated in the setting of complex regional pain syndrome.
Which system of lacunar networks is used among osteocytes to communicate?
1) Volkmann canals
2) Cement lines
3) Secondary messenger systems
4) Canaliculi
5) Haversian canals
Canaliculi are a system within the lacunar network used by osteocytes to communicate with each other.
Osteocytes have numerous cell processes (filopodia) that project through the canaliculi and connect to each other via gap junctions (see Illustrations B and C). Through this network osteocytes establish contact and communication with adjacent osteocytes for exchange of nutrients and metabolic waste. They are oriented in a radial fashion around the central Haversian canal.
Knothe Tate et al described the changes occuring in different pathologies. In normal bone, osteocyte connectivity is high and processes are oriented in the direction of blood supply. In osteoporotic bone, there is decreased osteocyte connectivity and orientation and tortuous cell processes. In osteoarthritic bone, there is decreased osteocyte viability and connectivity, but preserved
orientation. In osteomalacic bone, there is preserved viability and connectivity, but tortuous and chaotic cell processes.
Illustration A shows the structure of compact and spongy bone. Illustration B shows gap junctions between cells. Illustration C shows secondary messengers crossing gap junctions.
Incorrect Answers
Question 19High Yield
-A 63-year-old woman with osteopenia is struck by a motor vehicle and sustains a Schatzker 2 (AO/OTA Type B) fracture of the lateral tibial plateau. She has
1.5 cm of joint depression and 7 mm of condylar widening. What is the most appropriate surgical fixation for this injury?
1.5 cm of joint depression and 7 mm of condylar widening. What is the most appropriate surgical fixation for this injury?
Explanation
_**RESPONSES FOR QUESTIONS 101 THROUGH 104**_
1. Open reduction and internal fixation with absolute stability
2. Open reduction and internal fixation with relative stability
3. Closed reduction with casting
4. Reamed locked intramedullary nailing
5. External fixation
_For each of the following fractures choose the best method for definitive fixation._
1. Open reduction and internal fixation with absolute stability
2. Open reduction and internal fixation with relative stability
3. Closed reduction with casting
4. Reamed locked intramedullary nailing
5. External fixation
_For each of the following fractures choose the best method for definitive fixation._
Question 20High Yield
The nerve most commonly injured during total hip arthroplasty (THA) is the:
Explanation
The primary nerves of the region are the sciatic, femoral, inferior and superior gluteal, and obturator. The most common nerve injury during THA is to the peroneal division of the sciatiCnerve, followed by superior gluteal, obturator, and femoral nerves. Injury to these structures can lead to loss of function and poor outcomes
Question 21High Yield
This finding has been shown to be variably present in asymptomatic patients, and its incidence increases with age.
Explanation
- Figure 72a Figure 72b
Question 22High Yield
A 15-year-old girl who plays high school basketball has had worsening forefoot pain and swelling that is aggravated by activity for the past 5 weeks. She denies any history of an injury. Examination reveals no deformities. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Freiberg’s infraction is believed to be an osteochondrosis of the second metatarsal head. It is the only osteochondrosis that has a predilection for females. The typical patient is an athletically active adolescent female. The radiograph shows stage II disease wherein reossification is occurring; it is at this time that the second metatarsal head is most susceptible to deformation. Therefore, initial management should consist of a short leg
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
walking cast.
REFERENCE: Mann RA, Coughlin MJ: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 413-415.
Question 23High Yield
During controlled perforation for removal of stem and prosthesis, when making 9-mm holes in the femoral diaphysis:
Explanation
The size of the hole must not exceed 30% of the diameter of the shaft. Holes should not be placed any closer than two hole diameters apart, and they should be located in the anterolateral surface of the femur to decrease the stress riser
Question 24High Yield
A 14-year-old male high school wrestler presents to the training room with the lesions seen in Figures 1 and
Explanation
38
The images are consistent with herpes gladiatorum. This condition is caused by herpes simplex type 1 and occurs in 2% to 7% of wrestlers. It is spread via direct skin contact and is generally seen on the head, neck and shoulders. The lesions are characterized by fluid-filled blisters on an erythematous base. Return to play is permitted after the patient has been treated for 5 days with anti-viral medications, no new lesions are seen within 72 hours and previous active lesions have scabbed over.
The images are consistent with herpes gladiatorum. This condition is caused by herpes simplex type 1 and occurs in 2% to 7% of wrestlers. It is spread via direct skin contact and is generally seen on the head, neck and shoulders. The lesions are characterized by fluid-filled blisters on an erythematous base. Return to play is permitted after the patient has been treated for 5 days with anti-viral medications, no new lesions are seen within 72 hours and previous active lesions have scabbed over.
Question 25High Yield
-Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation?
Explanation
No detailed explanation provided for this question.
Question 26High Yield
A 13-year-old girl with idiopathic adolescent scoliosis has a 32° right thoracolumbar curve. Her Risser sign is 1. Her curve measured 29° 4 months ago. You recommend:
Explanation
Idiopathic scoliosis in skeletally immature patients should be braced if it is greater than 30° and significant growth remains (estimated by a Risser sign of 0, 1, or 2). Studies have shown that patients with idiopathic scoliosis without atypical findings do not need magnetic resonance imaging. Physical therapy and electrical stimulation have been shown not to have any effect on the progression of idiopathic scoliosis.
Question 27High Yield
A pantalar arthrodesis is described as a:
Explanation
A pantalar arthrodesis is the combination of an ankle and triple arthrodesis. It should not be confused with an ankle and subtalar arthrodesis (tibiotalocalcaneal).
Question 28High Yield
A 28-year-old male runner presents for treatment of a painful lesion under the first metatarsal head (located more toward the medial aspect of the metatarsophalangeal joint). The lesion is associated with painful callosity to palpation, normal hallux function, and a normal position of the first metatarsal. Attempts to relieve the pressure with orthoses and shoe modifications have not been successful. The ideal treatment is:
Explanation
Planing or shaving of the sesamoid is a reliable procedure for treatment of a specific focal keratosis beneath the tibial sesamoid. Resection of the tibial sesamoid is a reasonable alternative, although it should be used only for pathology of the sesamoid itself. In this individual, the position of the first metatarsal is normal. Since no plantarflexion is present, an osteotomy is not indicated.
Question 29High Yield
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment?
Explanation
DISCUSSION: The examination reveals that the patient has posterior capsular tightness. Surgery should not be considered until the patient has failed to respond to nonsurgical management. The internal rotation contracture (GIRD - glenohumeral internal rotation deficit) should be addressed with appropriate posterior capsular stretching. This should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient’s symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
REFERENCES: Meister K: Injuries to the shoulder in the throwing athlete. Part two: evaluation/ treatment. Am J Sports Med 2000;28:587-601.
Liu SH, Boynton E: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Tyler TF, Nicholas SJ, Roy T, et al: Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med 2000;28:668-673.
2010 Sports Medicine Examination Answer Book • 21
DISCUSSION: The examination reveals that the patient has posterior capsular tightness. Surgery should not be considered until the patient has failed to respond to nonsurgical management. The internal rotation contracture (GIRD - glenohumeral internal rotation deficit) should be addressed with appropriate posterior capsular stretching. This should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient’s symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
REFERENCES: Meister K: Injuries to the shoulder in the throwing athlete. Part two: evaluation/ treatment. Am J Sports Med 2000;28:587-601.
Liu SH, Boynton E: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Tyler TF, Nicholas SJ, Roy T, et al: Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med 2000;28:668-673.
2010 Sports Medicine Examination Answer Book • 21
Question 30High Yield
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy.
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 31High Yield
Figure 1 is the right hand of a 65-year-old man with a history of hypertension and rheumatoid arthritis. He is taking immunosuppressive disease-modifying antirheumatic drugs (DMARDs) and is seen in the emergency department with rapid progression of erythema from his right thumb to his right arm during the last 12 hours. He is confused, lethargic, and has these vital signs: blood pressure 92/40, respiratory rate 45, temperature 39.7°C, pulse 135, and oxygen saturation 90% on 4 liters of oxygen by face mask. An examination of his right upper extremity reveals black bulla extending from the metacarpophalangeal down to the tip and no capillary refill at the pulp. Immediate treatment should consist of
---
---

Explanation
This patient has multiple criteria for necrotizing soft-tissue infection (NSTI, also known as necrotizing fasciitis) including rapidly progressive infection, black bulla, hypotension and hypoxia, and a history of immune compromise. Aggressive emergent debridement including the removal of all necrotic tissue and IV antibiotics can decrease morbidity and mortality. Not all patients will have such obvious NSTI findings. In less clear cases, a scoring system using laboratory values (the Laboratory Risk Indicator for Necrotizing Fasciitis) can help clarify the diagnosis. IV antibiotics are key to treatment as well, but any delay in surgical treatment can increase morbidity and mortality. The black bulla and necrotic-appearing thumb indicate that this infection is not confined to the flexor sheath, therefore irrigation of the tendon sheath alone would be insufficient treatment. Although the thumb is dysvascular, this is because of an _infection, and revascularization is not indicated._
Question 32High Yield
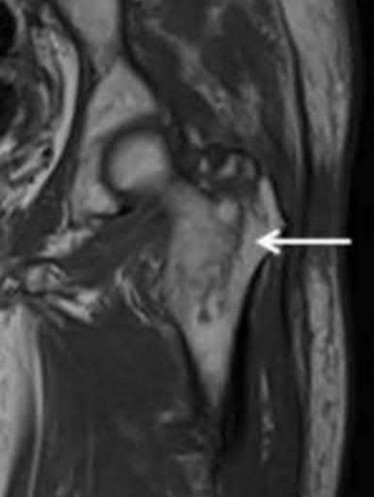
An 80-year-old female sustained a twist and fall earlier at her home. She currently complains of left hip pain. On physical examination, she has hip pain with motion and is tender to palpation over her greater trochanter. Her injury radiographs are shown in Figure A. Which of the following should be performed next in this patient's care?


Explanation
This patient sustained a greater trochanteric (GT) fracture. Evaluation with MRI is the next best step in treatment to evaluate for intertrochanteric (IT) extension.
Isolated fractures of the GT are uncommon. They may be diagnosed on radiography, but the extent of this injury is difficult to ascertain based on radiography alone. MRI has found a role in defining the extent of the fracture line. Though isolated GT fractures are often treated conservatively when they occur in isolation, operative fixation is necessary if there is IT extension. If the extent of the injury is not identified, it may lead to delayed rehabilitation and decreased long-term survival rates.
Kim et al. performed a systematic review to determine what proportion of GT fractures had IT extension and what are the treatment options of GT with occult IT extension. Patients included had an isolated GT fracture on radiographs and underwent MRI scans to determine IT extension. In 99/110 patients (90%), MRI revealed IT extension and surgical fixation followed in 61 patients. They conclude that MRI should be performed in patients presenting with an isolated GT fracture on plain radiograph.
Lee et al. examined the pattern and extent of an injury shown by MRI and radionuclide bone scan (RBS) in patients whose radiographs revealed fractures
limited to the GT. 25 patients were found sustaining a low-energy injury. They found that 3 patients had ITC extension that was not visualized with radiographs or RBS. 8 patients had fractures with MRI evidence of complete extension across the ITC region and 12 had incomplete extension. 11/12 patients with incomplete extension had extension more than 50% to the medial cortex. They recommend that all patients presenting with an isolated GT fracture on the plain radiographs should undergo MRI examination.
Collin et al. performed a study to evaluate the efficacy of CT in diagnosing occult hip fractures compared to MRI. They evaluated 44 consecutive elderly patients with trauma to the hip. All patients had negative CT scans while MRI changed the diagnoses in 27 cases. They conclude that MRI is a more reliable modality for hip fracture diagnosis in comparison to CT and negative CT finding cannot rule out a hip fracture in patients with a clinical suspicion for a hip fracture.
Figure A is an AP pelvis radiograph demonstrating a fracture of the left greater trochanter. Illustration A is a radiograph demonstrating a GT fracture and Illustration B is a T1-weighted MRI of the same patient demonstrating IT extension.
Incorrect Answers:
Answers 1 and 2: Treatment should not be performed until more information with an MRI is obtained.
Answer 3: Traction, internal rotation views are obtained in displaced intertrochanteric fractures to visualize the fracture fragments more accurately and to assess the efficacy of a closed-reduction maneuver.
Answer 4: CT scan of the proximal femur is not the best study to rule out IT extension of this fracture.
Isolated fractures of the GT are uncommon. They may be diagnosed on radiography, but the extent of this injury is difficult to ascertain based on radiography alone. MRI has found a role in defining the extent of the fracture line. Though isolated GT fractures are often treated conservatively when they occur in isolation, operative fixation is necessary if there is IT extension. If the extent of the injury is not identified, it may lead to delayed rehabilitation and decreased long-term survival rates.
Kim et al. performed a systematic review to determine what proportion of GT fractures had IT extension and what are the treatment options of GT with occult IT extension. Patients included had an isolated GT fracture on radiographs and underwent MRI scans to determine IT extension. In 99/110 patients (90%), MRI revealed IT extension and surgical fixation followed in 61 patients. They conclude that MRI should be performed in patients presenting with an isolated GT fracture on plain radiograph.
Lee et al. examined the pattern and extent of an injury shown by MRI and radionuclide bone scan (RBS) in patients whose radiographs revealed fractures
limited to the GT. 25 patients were found sustaining a low-energy injury. They found that 3 patients had ITC extension that was not visualized with radiographs or RBS. 8 patients had fractures with MRI evidence of complete extension across the ITC region and 12 had incomplete extension. 11/12 patients with incomplete extension had extension more than 50% to the medial cortex. They recommend that all patients presenting with an isolated GT fracture on the plain radiographs should undergo MRI examination.
Collin et al. performed a study to evaluate the efficacy of CT in diagnosing occult hip fractures compared to MRI. They evaluated 44 consecutive elderly patients with trauma to the hip. All patients had negative CT scans while MRI changed the diagnoses in 27 cases. They conclude that MRI is a more reliable modality for hip fracture diagnosis in comparison to CT and negative CT finding cannot rule out a hip fracture in patients with a clinical suspicion for a hip fracture.
Figure A is an AP pelvis radiograph demonstrating a fracture of the left greater trochanter. Illustration A is a radiograph demonstrating a GT fracture and Illustration B is a T1-weighted MRI of the same patient demonstrating IT extension.
Incorrect Answers:
Answers 1 and 2: Treatment should not be performed until more information with an MRI is obtained.
Answer 3: Traction, internal rotation views are obtained in displaced intertrochanteric fractures to visualize the fracture fragments more accurately and to assess the efficacy of a closed-reduction maneuver.
Answer 4: CT scan of the proximal femur is not the best study to rule out IT extension of this fracture.
Question 33High Yield
Currently, what is the most common clinical study type in the orthopaedic literature?
Explanation
**
Although a recent push for prospective, randomized trials has been advocated by multiple orthopaedic journals, many studies published continue to be of Level 4 evidence (retrospective case series). Case series represented 64% of all studies reviewed by Freedman and associates in 2001 from the British and American volumes of Journal of Bone and Joint Surgery and from Clinical Orthopaedics and Related Research.
Obremskey and associates published that
58.1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the
current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
Although a recent push for prospective, randomized trials has been advocated by multiple orthopaedic journals, many studies published continue to be of Level 4 evidence (retrospective case series). Case series represented 64% of all studies reviewed by Freedman and associates in 2001 from the British and American volumes of Journal of Bone and Joint Surgery and from Clinical Orthopaedics and Related Research.
Obremskey and associates published that
58.1% of all studies from nine orthopaedic journals were Level 4 evidence. Further investigation of more current trends is likely warranted with the
current emphasis on publishing higher level-of-evidence studies in orthopaedic journals.
Question 34High Yield
Place the following strategies for treating deep infection in total hip replacement in order of their effectiveness from 1 to 4, with
1 being the most effective. 1. No antibiotics 2. SystemiCantibiotics alone 3. AntibiotiCbone cement alone 4. AntibiotiCbone cement plus systemiCantibiotics
1 being the most effective. 1. No antibiotics 2. SystemiCantibiotics alone 3. AntibiotiCbone cement alone 4. AntibiotiCbone cement plus systemiCantibiotics
Explanation
According to Espehaug and colleagues in their assessment of 10,905 primary cemented total knee replacements, the most effective strategy is antibiotic-bone cement plus systemiCantibiotics followed by systemiCantibiotics alone, antibiotic-bone cement alone, and no antibiotics
Question 35High Yield
A 24-year-old female soccer player has recurrent instability following noncontact injury to the right knee 2 years after anterior cruciate reconstruction using hamstring autograft. Physical examination reveals positive Lachman and pivot shift. Radiographs reveal well-preserved joint spaces with 13° of posterior tibial slope. MRI scan reveals failure of graft with small tear of the lateral meniscus. What is the most appropriate treatment?
Explanation
Increased tibial slope (>12°) may be a risk factor for noncontact ACL injury and subsequent failure of repair, and corrective proximal tibial osteotomy may be indicated combined with primary or revision ACL reconstruction. The indications for proximal tibial valgus osteotomy are generally isolated medial compartment degeneration in a knee with varus malalignment in a young, active individual. Factors associated with early failure include increased age (>55 years), increased BMI (10% greater than normal), preoperative flexion
<120° and under- or overcorrection. Inflammatory arthritis, including gout, would be a relative contraindication.
<120° and under- or overcorrection. Inflammatory arthritis, including gout, would be a relative contraindication.
Question 36High Yield
When performing total knee replacement surgery, the following statement is true:
Explanation
These are important concepts when balancing the knee following total knee replacement.
The distal femoral cut only effects the extension gap.
The proximal tibia cut effects the flexion and extension gaps. The posterior femoral condyle cut effects the flexion only.
Attention to these principles is very important to prevent both contractures and flexion instability. Correct Answer: The distal femoral cut only effects the extension gap.
The distal femoral cut only effects the extension gap.
The proximal tibia cut effects the flexion and extension gaps. The posterior femoral condyle cut effects the flexion only.
Attention to these principles is very important to prevent both contractures and flexion instability. Correct Answer: The distal femoral cut only effects the extension gap.
Question 37High Yield
Figures 1 through 3 represent the radiographs obtained from a 37-year- old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?
15
15
Explanation
This patient has severe, uncorrectable varus deformity and pain from end- stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
16
16
Question 38High Yield
Figures 1 through 3 show the radiographs obtained from an 86-year-old- woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
73
73
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 39High Yield
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
The most common complication of dorsal plating is extensor tenosynovitis, which often causes pain and is a frequent reason for hardware removal. Other less frequent complications include loss of reduction and extensor tendon ruptures, with flexor tendon ruptures occuring to an even lesser degree.
REFERENCES: Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
REFERENCES: Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
Question 40High Yield
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
Question 41High Yield
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
The risk of intraoperative fracture in osteoporotic bone in patients with rheumatoid arthritis is significant. Fractures most often occur during humeral head dislocation and positioning for canal reaming. If the fracture occurs at the greater tuberosity, cerclage suture fixation of the tuberosity fracture with autogenous cancellous bone graft from the resected humeral head is the treatment of choice.
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
Question 42High Yield
A 38-year-old marathon runner has had Achilles tendon pain for the past 2 months. Examination reveals that the tendon is thickened and tender proximal to the calcaneal insertion. The tendon sheath is not thickened or tender. The pathophysiology of the tendon is best described as
Explanation
Atraumatic Achilles tendon disease can be differentiated into Achilles tendinosis and peritendinitis. Thickening and tenderness of the Achilles tendon are present in both, but thickening and tenderness of the tendon sheath indicates peritendinitis. Histologic examination of Achilles tendinosis reveals an absence of acute and chronic inflammatory cells. Radiologists often diagnose partial tendon rupture by MRI and there may be microscopic longitudinal tears present, but there is no mechanical compromise as would be implied by a partial rupture. The thickening typically occurs in the portion of the tendon with the poorest blood supply, and biochemical analysis detects high levels of lactate and other products of anaerobic glycolysis.
REFERENCES: Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164.
Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
Alfredson H, Bjur D, Thorsen K, et al: High intratendinous lactate levels in painful chronic Achilles tendinosis: An investigation using microdialysis technique. J Orthop Res
2002;20:934-938.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
REFERENCES: Astrom M, Rausing A: Chronic Achilles tendinopathy: A survey of surgical and histopathologic findings. Clin Orthop 1995;316:151-164.
Ohberg L, Lorentzon R, Alfredson H: Neovascularisation in Achilles tendons with painful tendinosis but not in normal tendons: An ultrasonographic investigation. Knee Surg Sports Traumatol Arthrosc 2001;9:233-238.
Alfredson H, Bjur D, Thorsen K, et al: High intratendinous lactate levels in painful chronic Achilles tendinosis: An investigation using microdialysis technique. J Orthop Res
2002;20:934-938.
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 43High Yield
What is the most appropriate next step?
Explanation
- Nonsteroidal anti-inflammatory drugs and physical therapy_
Question 44High Yield
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?

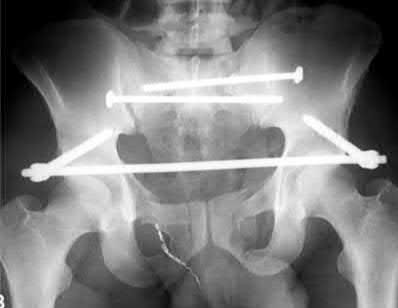
Explanation
This patient was treated with posterior stabilization, and an anterior subcutaneous internal fixator (ASIF). The most common neurologic injury seen following placement of the ASIF construct is irritation of the lateral femoral cutaneous nerve (LFCN), causing numbness and/or pain of the lateral thigh.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Answer 1: Weakness of hip flexion would be due to injury to the femoral nerve, which is not commonly associated with this construct.
Answer 2: Weakness of ankle dorsiflexion would be due to injury to the L5 nerve root, which does not occur due to ASIF placement.
Answer 3: Numbness of the medial thigh is due to injury to the obturator nerve, which is not commonly associated with this construct.
Answer 5: Numbness of the perineum is due to injury to the sacral nerve roots, which is not commonly associated with this construct.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Answer 1: Weakness of hip flexion would be due to injury to the femoral nerve, which is not commonly associated with this construct.
Answer 2: Weakness of ankle dorsiflexion would be due to injury to the L5 nerve root, which does not occur due to ASIF placement.
Answer 3: Numbness of the medial thigh is due to injury to the obturator nerve, which is not commonly associated with this construct.
Answer 5: Numbness of the perineum is due to injury to the sacral nerve roots, which is not commonly associated with this construct.
Question 45High Yield
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
When load is applied to the wrist, most of the stress is absorbed by the radius. As the load is transferred through the forearm, the interosseous membrane transfers some of the load from the radius to the ulna. The load at the elbow is distributed with 40% at the ulnohumeral articulation and 60% at the radiohumeral articulation.
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
Question 46High Yield
Figures 1 through 3 depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the
Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two- stage revision total knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
87
87
Question 47High Yield
Figure 1
A 31-year-old recreational soccer player presents for evaluation of chronic ankle pain during physical activity. He reports a severe inversion ankle sprain that occurred 1 year ago and notes that he was treated with cast immobilization. Upon examination, he does not demonstrate laxity of the ankle ligaments and pain is present along the anterior medial ankle. A radiograph is presented. The recommended treatment is:
A 31-year-old recreational soccer player presents for evaluation of chronic ankle pain during physical activity. He reports a severe inversion ankle sprain that occurred 1 year ago and notes that he was treated with cast immobilization. Upon examination, he does not demonstrate laxity of the ankle ligaments and pain is present along the anterior medial ankle. A radiograph is presented. The recommended treatment is:
Explanation
This patient has an osteochondral defect of the talus. According to most classification systems, the grade of the defect is not severe. Retrograde drilling of the defect through the sinus tarsi is possible for a posteromedial lesion of the talus for which the cartilage surface is intact. An autogenous osteochondral bone graft is indicated for a severe lesion with bone loss or following failure of previous attempts at arthroscopic drilling. The ideal procedure is arthroscopic debridement and drilling of the subchondral bone.
Question 48High Yield
Which of the following statements most accurately describes the risk of ileus following total joint arthroplasty?
Explanation
DISCUSSION: The risk of postoperative ileus is noted to be higher in patients undergoing THA than patients undergoing TKA. Older age, male gender, and a history of abdominal surgery have been identified as risk factors.
REFERENCE: Parvizi J, Han SB, Tarity TD, et al: Postoperative ileus after total joint arthroplasty. J Arthroplasty 2008;23:360-365.
DISCUSSION: The risk of postoperative ileus is noted to be higher in patients undergoing THA than patients undergoing TKA. Older age, male gender, and a history of abdominal surgery have been identified as risk factors.
REFERENCE: Parvizi J, Han SB, Tarity TD, et al: Postoperative ileus after total joint arthroplasty. J Arthroplasty 2008;23:360-365.
Question 49High Yield
Which of the following is an action of 1,25 dihydroxy vitamin D:
Explanation
Vitamin D acts on the intestinal to increase calcium absorption. C alcium binding protein synthesis is increased. Vitamin D is an intracellular messenger, acting through the nucleus.
Vitamin D actions:
Increase the efficiency of calcium absorption in the intestine (primarily duodenum) Increases synthesis of calcium binding protein (and others)
Increases passage of calcium through the cell membrane
Moves calcium through the cell cytoplasm and into the circulation
Increases bone resorption by telling the osteoblasts to release receptor activator of nuclear factor -kB ligand
Osteoblasts have vitamin D receptors
Vitamin D receptors exert a negative feedback on 1,25 dihydroxy vitamin D production
Decreases PTH production
Vitamin D actions:
Increase the efficiency of calcium absorption in the intestine (primarily duodenum) Increases synthesis of calcium binding protein (and others)
Increases passage of calcium through the cell membrane
Moves calcium through the cell cytoplasm and into the circulation
Increases bone resorption by telling the osteoblasts to release receptor activator of nuclear factor -kB ligand
Osteoblasts have vitamin D receptors
Vitamin D receptors exert a negative feedback on 1,25 dihydroxy vitamin D production
Decreases PTH production
Question 50High Yield
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?

Explanation
DISCUSSION: The development of heterotopic bone occurs early after hip arthroplasty. The process begins within days after surgery; therefore, prophylactic treatment must be in the early postoperative period (preoperative radiation given within 24 hours of surgery, or postoperative radiation given within 72 hours of surgery, or nonsteroidal anti- inflammatory drugs (NSAIDs) given postoperatively for 7 to 21 days - longer duration has not been shown to be of any additional benefit). At 6 weeks, prophylactic treatment with NSAIDs or radiation is no longer effective. Surgery at 10 weeks would be premature because the patient is currently asymptomatic with regards to the heterotopic bone, and surgery prior to full maturation of the bone may increase the risk for more abundant recurrence of bone.
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory
drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Figure 64
DISCUSSION: The development of heterotopic bone occurs early after hip arthroplasty. The process begins within days after surgery; therefore, prophylactic treatment must be in the early postoperative period (preoperative radiation given within 24 hours of surgery, or postoperative radiation given within 72 hours of surgery, or nonsteroidal anti- inflammatory drugs (NSAIDs) given postoperatively for 7 to 21 days - longer duration has not been shown to be of any additional benefit). At 6 weeks, prophylactic treatment with NSAIDs or radiation is no longer effective. Surgery at 10 weeks would be premature because the patient is currently asymptomatic with regards to the heterotopic bone, and surgery prior to full maturation of the bone may increase the risk for more abundant recurrence of bone.
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory
drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Figure 64
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon