Mastering Lateral Epicondylitis: Open & Arthroscopic Debridement
Key Takeaway
Welcome to this masterclass on surgical management of lateral epicondylitis. We'll meticulously cover patient selection, detailed anatomy of the common extensor origin, and precise intraoperative execution for both open and arthroscopic debridement. Expect an immersive, step-by-step guide through the procedure, emphasizing critical pearls, avoiding pitfalls, and ensuring optimal patient outcomes through expert technique and comprehensive postoperative care.
Comprehensive Introduction and Patho-Epidemiology
Lateral epicondylitis, more accurately described in the contemporary orthopedic literature as lateral elbow tendinopathy (LET), represents one of the most frequently encountered overuse syndromes of the upper extremity. While colloquially termed "tennis elbow," the vast majority of patients afflicted with this condition do not actively participate in racquet sports; rather, the etiology is deeply rooted in repetitive, forceful eccentric contractions of the wrist extensor musculature during occupational or daily activities. The epidemiological burden is substantial, affecting approximately 1% to 3% of the general adult population, with a peak incidence occurring in the fourth and fifth decades of life. The dominant arm is disproportionately affected, underscoring the mechanical and functional origins of the disease process. As orthopedic surgeons, we must recognize that this condition is a leading cause of prolonged occupational disability and substantial healthcare expenditure, necessitating a rigorous, evidence-based approach to both non-operative and surgical management.
The fundamental histopathology of lateral elbow tendinopathy was elegantly elucidated by Robert Nirschl, who coined the term "angiofibroblastic tendinosis." This nomenclature is critical because it fundamentally shifts our paradigm away from an acute inflammatory process ("-itis") toward a chronic, degenerative one ("-osis"). Histological analysis of excised tissue consistently demonstrates a profound absence of acute inflammatory cells, such as macrophages or neutrophils. Instead, the architecture is characterized by disorganized, immature collagen formation, mucoid ground substance degeneration, and a chaotic, non-functional neovascularization. This fibrovascular response represents an aborted or incomplete healing cascade in the face of repetitive microtrauma. The extensor carpi radialis brevis (ECRB) is the primary anatomic epicenter of this degeneration, owing to its distinct biomechanical disadvantages and tenuous vascular watershed zones at its origin.
Clinically, patients present with a highly localized, often debilitating pain directly over the lateral epicondyle, which classically radiates distally along the extensor muscle mass of the forearm. The pain is predictably exacerbated by gripping activities, resisted wrist extension, and passive wrist flexion with the elbow extended. From a diagnostic standpoint, the physical examination remains the cornerstone of evaluation. Universal tenderness at the ECRB origin is palpable just anterior and distal to the lateral epicondyle. Provocative maneuvers, including Mill's test (passive stretching of the extensors) and Cozen's or Thompson's tests (resisted wrist and finger extension), reliably reproduce the patient's chief complaint. Furthermore, assessing grip strength with the elbow in full extension often reveals significant weakness secondary to pain inhibition, a metric that serves as a useful objective baseline for tracking clinical progress.
The natural history of lateral elbow tendinopathy is generally favorable, with the condition often proving to be self-limiting over a 12- to 18-month period in up to 80% to 90% of patients. Consequently, the initial management strategy must be strictly non-operative, encompassing activity modification, counterforce bracing, structured physical therapy emphasizing eccentric strengthening, and judicious use of orthobiologics or corticosteroid injections. However, a distinct subset of patients—approximately 5% to 10%—will develop recalcitrant, chronic tendinosis that fails to respond to exhaustive conservative measures. For this specific cohort, surgical intervention becomes a highly effective and definitive solution. The overarching surgical objective, whether executed via an open or arthroscopic approach, is the meticulous excision of the angiofibroblastic tissue, decortication of the lateral epicondyle to stimulate a marrow-mediated healing response, and the careful preservation of the critical posterolateral stabilizing structures of the elbow.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the lateral elbow anatomy is the absolute prerequisite for executing a safe and effective debridement while avoiding catastrophic iatrogenic complications. The osteology of the lateral elbow comprises the lateral epicondyle, the supracondylar ridge, and the capitellum. The lateral epicondyle serves as the osseous footprint for the common extensor origin (CEO) and the lateral collateral ligament (LCL) complex. The CEO is a complex, confluent aponeurotic structure giving rise to four primary musculotendinous units: the extensor carpi radialis brevis (ECRB), the extensor digitorum communis (EDC), the extensor digiti minimi (EDM), and the extensor carpi ulnaris (ECU). The extensor carpi radialis longus (ECRL) originates more proximally on the lateral supracondylar ridge and is structurally distinct from the CEO, a critical anatomic relationship utilized during the surgical approach.
The ECRB is the primary pathological focus in lateral elbow tendinopathy. Its origin is situated deep and anteriorly on the lateral epicondyle, intimately blending with the underlying lateral joint capsule and the annular ligament. Biomechanically, the ECRB is uniquely vulnerable to microtrauma. During elbow flexion and extension, the undersurface of the ECRB tendon glides directly over the prominent capitellum, subjecting it to significant sheer and compressive forces. Furthermore, the ECRB acts as a primary stabilizer of the wrist during gripping activities, enduring massive eccentric loads. The EDC originates superficially and slightly posterior to the ECRB. In chronic, advanced cases of tendinosis, the degenerative process may extend from the ECRB to involve the deep, undersurface fibers of the EDC aponeurosis, necessitating inspection and potential debridement of this structure as well.
The ligamentous anatomy of the lateral elbow is of paramount importance, specifically the lateral collateral ligament (LCL) complex. This complex consists of the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), and the annular ligament. The LUCL is the primary restraint against posterolateral rotatory instability (PLRI). It originates on the lateral epicondyle, intimately blending with the common extensor origin, and inserts on the supinator crest of the ulna. The most critical anatomic axiom for the operating surgeon is that the LUCL lies explicitly posterior to the mid-radiocapitellar joint line. Therefore, all surgical dissection, whether open or arthroscopic, must remain strictly anterior to the equator of the radial head. Violation of the LUCL during aggressive debridement will result in iatrogenic PLRI, a devastating complication that fundamentally alters the kinematics of the elbow and requires complex reconstructive procedures.
The neurovascular topography surrounding the lateral elbow demands meticulous respect. The radial nerve descends through the anterior compartment of the arm and bifurcates into the superficial radial nerve (sensory) and the deep posterior interosseous nerve (PIN) at the level of the radiocapitellar joint. The PIN subsequently dives deep, passing between the two heads of the supinator muscle at the arcade of Frohse. While the PIN is generally safe during a standard, localized ECRB debridement, it becomes highly vulnerable during overly distal dissection, aggressive retraction, or errant placement of arthroscopic portals. The vascular supply to the lateral epicondyle is primarily derived from the radial recurrent artery, which ascends anteriorly to anastomose with the radial collateral artery. The ECRB origin itself has been shown to possess a hypovascular watershed zone, further predisposing it to degenerative changes and poor healing potential following repetitive microtrauma.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for lateral elbow tendinopathy must be predicated on a rigorous, evidence-based algorithm. Surgery is strictly reserved for patients who have demonstrably failed a comprehensive, protracted course of non-operative management. The universally accepted temporal threshold is a minimum of 6 to 12 months of conservative therapy. This non-operative regimen should include, but is not limited to, absolute cessation of the offending activities, dedicated physical therapy focusing on eccentric extensor strengthening and scapular stabilization, non-steroidal anti-inflammatory drugs (NSAIDs), counterforce bracing, and potentially the judicious use of corticosteroid or platelet-rich plasma (PRP) injections. Patients must present with chronic, unrelenting pain that significantly impairs their activities of daily living, occupational duties, or sleep quality, thereby justifying the inherent risks of surgical intervention.
Diagnostic imaging plays a crucial role in confirming the clinical diagnosis and ruling out concomitant pathology prior to surgery. While plain radiographs are often unremarkable, they are necessary to evaluate for intra-articular loose bodies, radiocapitellar osteoarthritis, or calcific tendinosis at the epicondyle. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the structural integrity of the common extensor origin. T2-weighted sequences will reliably demonstrate increased signal intensity and tendon thickening within the ECRB origin, indicative of mucoid degeneration and interstitial tearing. Furthermore, MRI is invaluable for assessing the integrity of the LCL complex, evaluating the articular cartilage of the radiocapitellar joint, and ruling out occult pathology such as osteochondritis dissecans of the capitellum, which would dramatically alter the surgical plan.
Contraindications to surgical debridement must be carefully evaluated to prevent postoperative failures and patient dissatisfaction. Absolute contraindications include active local or systemic infection, complex regional pain syndrome (CRPS), and the presence of severe, untreated psychiatric comorbidities that would preclude adherence to postoperative rehabilitation. Relative contraindications, which require astute clinical differentiation, include alternative sources of lateral elbow pain. Cervical radiculopathy, specifically involving the C6 or C7 nerve roots, can refer pain to the lateral elbow and must be ruled out via a thorough neurological examination and potentially electromyography (EMG). Similarly, radial tunnel syndrome—compression of the PIN within the radial tunnel—often masquerades as lateral epicondylitis. Pain in radial tunnel syndrome is typically localized 3 to 4 centimeters distal to the lateral epicondyle, over the mobile wad, and is exacerbated by resisted middle finger extension. Operating on an unrecognized radial tunnel syndrome under the guise of lateral epicondylitis will uniformly result in surgical failure.
Furthermore, the presence of pre-existing posterolateral rotatory instability (PLRI) is a critical consideration. If a patient demonstrates a positive pivot-shift test or apprehension during the preoperative examination, a simple ECRB debridement is contraindicated. In such scenarios, the surgeon must be prepared to perform a concomitant LUCL reconstruction or repair. Failure to address underlying instability will not only fail to resolve the patient's pain but may exacerbate the mechanical dysfunction of the joint. The choice between open and arthroscopic techniques is largely driven by surgeon preference and experience; however, significant intra-articular pathology (e.g., symptomatic synovial plica, loose bodies, or focal chondral defects) strongly favors an arthroscopic approach to allow for comprehensive joint evaluation and concurrent treatment.
| Category | Specific Conditions | Clinical Implications |
|---|---|---|
| Absolute Indications | Failure of 6-12 months of conservative management | Surgery is the definitive treatment for recalcitrant angiofibroblastic tendinosis. |
| Severe, unrelenting pain impacting ADLs/sleep | Quality of life impairment justifies surgical risk profile. | |
| MRI-confirmed high-grade ECRB tearing/degeneration | Objective structural failure correlating with clinical symptoms. | |
| Relative Indications | Concomitant intra-articular pathology (plica, loose bodies) | Strongly favors an arthroscopic approach for concurrent management. |
| Patient intolerance to prolonged conservative care | Requires careful counseling regarding surgical expectations and rehab. | |
| Absolute Contraindications | Active local or systemic infection | High risk of septic arthritis or deep space infection. |
| Unaddressed Cervical Radiculopathy (C6/C7) | Surgery will fail to resolve referred neurogenic pain. | |
| Unrecognized Radial Tunnel Syndrome | Debridement will not decompress the posterior interosseous nerve. | |
| Relative Contraindications | Pre-existing Posterolateral Rotatory Instability (PLRI) | Requires concurrent LUCL reconstruction; simple debridement will fail. |
| Severe radiocapitellar osteoarthritis | Debridement alone may not alleviate mechanically driven articular pain. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful surgical outcome. The surgeon must comprehensively synthesize the patient's clinical history, physical examination findings, and advanced imaging modalities. The MRI should be scrutinized not only for the extent of ECRB tendinosis but also to precisely map the location of the degenerative tissue. Is the pathology isolated to the deep anterior fibers, or does it extend posteriorly into the EDC aponeurosis? Is there a full-thickness macroscopic tear that will require a more extensive repair following debridement? Furthermore, the integrity of the LUCL must be explicitly verified on the coronal and axial MRI sequences. Any ambiguity regarding ligamentous competency should prompt a high index of suspicion for instability, which must be dynamically assessed under anesthesia prior to making the incision.
Once the patient is brought into the operating theater and general anesthesia or a regional brachial plexus block is administered, a thorough Examination Under Anesthesia (EUA) is mandatory. With the protective muscle guarding eliminated, the elbow is taken through a full range of motion. The surgeon must perform a definitive posterolateral pivot-shift test, assessing for subluxation of the radial head posterior to the capitellum as the elbow is brought from extension to flexion under an axial load and supination moment. The varus and valgus stability of the elbow are also documented. If unexpected PLRI is encountered, the surgical plan must dynamically shift to include a lateral ulnar collateral ligament stabilization procedure. The operative limb is then prepped and draped in standard sterile fashion, ensuring access to the iliac crest or allograft if a ligament reconstruction becomes necessary.
Patient positioning is dictated by the chosen surgical technique. For the Open Lateral Epicondylar Fasciectomy (Nirschl Technique), the patient is placed in the supine position. A sterile tourniquet is applied high on the brachium to ensure a bloodless surgical field, which is critical for identifying the subtle visual distinctions between healthy tendon and angiofibroblastic tissue. The arm is positioned on a well-padded hand table. The shoulder is slightly internally rotated, allowing the lateral aspect of the elbow to present anteriorly, optimizing the surgeon's ergonomic access. The elbow is typically flexed to approximately 60 to 90 degrees during the procedure, which relaxes the neurovascular structures of the anterior compartment and brings the ECRB footprint into clear view. Bony landmarks, including the lateral epicondyle, the radial head, and the olecranon, are carefully palpated and marked with a sterile surgical pen.
For the Arthroscopic Lateral Epicondylar Debridement, positioning requires specialized equipment and a dedicated setup. While some surgeons prefer the prone or supine suspended positions, the lateral decubitus position is highly advantageous. The patient is placed in the lateral decubitus position with the operative arm superior. A specialized limb positioner, such as a Spider Arm Holder, is utilized to securely suspend the arm. The shoulder is abducted to 90 degrees and forward flexed slightly, while the elbow is flexed to 90 degrees. This position utilizes gravity to assist in joint distraction and provides excellent, unimpeded access to the anterior and posterior compartments of the elbow. A non-sterile tourniquet is applied proximally. Precise anatomical marking is even more critical in arthroscopy to ensure safe portal placement. The lateral epicondyle, radial head, olecranon, and the course of the ulnar nerve are demarcated. The joint is then insufflated with 15 to 20 cc of sterile normal saline via a direct lateral approach through the anconeus soft spot to distend the capsule and displace the neurovascular structures anteriorly, thereby increasing the margin of safety for subsequent portal establishment.
Step-by-Step Surgical Approach and Debridement Technique
Open Lateral Epicondylar Fasciectomy (Nirschl Technique)
The open approach remains the gold standard against which all other techniques are measured, offering unparalleled direct visualization and tactile feedback of the pathologic tissues.
Step 1: Incision and Superficial Dissection
The procedure begins with a precise 3 to 5-centimeter longitudinal incision. The incision is centered over the lateral epicondyle, beginning just proximal to the epicondylar prominence and extending distally, strictly in line with the longitudinal axis of the forearm and the underlying extensor muscle fibers.

This orientation is critical; it aligns with Langer's lines to optimize cosmetic healing and, more importantly, keeps the dissection anterior to the critical LUCL complex. Following skin incision, sharp dissection is carried through the subcutaneous fat. Metzenbaum scissors are utilized for careful blunt spreading to expose the underlying deep antebrachial fascia, taking care to coagulate any crossing branches of the radial recurrent artery.
Step 2: Identifying the Extensor Interval
Once the deep fascia is exposed, the surgeon must identify the critical anatomic interval between the extensor carpi radialis longus (ECRL) and the extensor digitorum communis (EDC) aponeurosis. The ECRL is located anteriorly and is characterized by its distinct, reddish muscular belly extending further proximally. Conversely, the EDC aponeurosis lies posteriorly and presents as a glistening, whitish tendinous sheet originating directly from the epicondyle.

A subtle longitudinal fat stripe often demarcates this interval distally. Precise identification of this plane is the key to minimizing collateral tissue damage and directly accessing the underlying ECRB pathology.
Step 3: Splitting the Interval and Exposing the ECRB
Using a #15 scalpel blade, the deep fascia is incised longitudinally along the ECRL-EDC interval. The incision is carried proximally to the lateral epicondyle. A small, posterior-based flap of the EDC aponeurosis is gently elevated. Simultaneously, a Senn or rake retractor is used to retract the muscular belly of the ECRL strongly anteriorly.

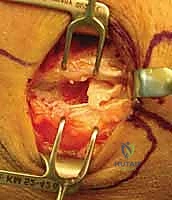
This maneuver acts like opening a book, revealing the origin of the ECRB deeply situated on the anterior aspect of the lateral epicondyle. At this juncture, the macroscopic pathology becomes evident. Healthy tendon is taut and pearlescent; in contrast, the tendinotic ECRB appears dull, grayish, friable, and disorganized, often lacking distinct longitudinal fibers.
Step 4: Debridement of the Angiofibroblastic Tissue
The core of the procedure is the meticulous excision of the diseased tissue. The surgeon utilizes the "Nirschl scratch test"—a tactile diagnostic maneuver where a #15 blade is scraped against the tendon. Pathologic, angiofibroblastic tissue is poorly cohesive and will easily peel or scrape away, whereas healthy collagenous tendon will resist the blade.
The degenerative ECRB origin is sharply excised down to the underlying lateral joint capsule. Often, the capsule itself is intimately involved in the degenerative process or has been breached by a chronic tendon tear, exposing the radiocapitellar joint.
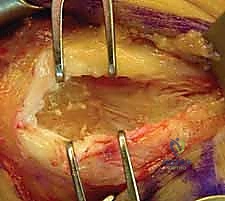
If the joint is exposed, a thorough visual inspection of the capitellum and radial head is performed. Any hypertrophic, impingement-causing synovial plica within the lateral gutter is sharply resected. The debridement is extended posteriorly to address the undersurface of the EDC if it demonstrates similar degenerative changes, but the surgeon must remain hyper-vigilant to stay anterior to the equator of the radial head to protect the LUCL.
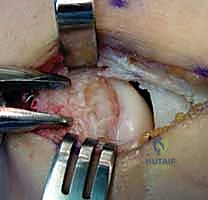
Step 5: Decortication and Closure
Once all pathologic soft tissue has been excised, attention is turned to the osseous footprint on the lateral epicondyle. To stimulate a robust, marrow-mediated healing response, the cortical bone of the ECRB footprint is decorticated. This is achieved using a small curette, a motorized burr, or by drilling multiple 2.0-mm holes into the footprint until punctate bleeding is observed from the cancellous bone.
Following thorough irrigation to remove bone debris, the wound is closed. The anteriorly retracted ECRL is allowed to fall back into position. The previously created EDC aponeurotic flap is loosely approximated to the ECRL fascia using interrupted absorbable sutures (e.g., 2-0 Vicryl).

It is imperative not to close this interval under excessive tension, as the primary goal is simply to restore the fascial envelope, not to tightly repair the resected ECRB back to the bone. The subcutaneous tissue and skin are closed in a standard fashion.
Arthroscopic Lateral Epicondylar Debridement
The arthroscopic technique offers the advantage of a comprehensive intra-articular evaluation and potentially less disruption of the overlying normal aponeurosis, facilitating a marginally faster early rehabilitation phase.
Step 1: Portal Placement and Diagnostic Sweep
Following joint insufflation, standard proximal anteromedial and proximal anterolateral portals are established. The arthroscope is initially introduced via the proximal anteromedial portal to view the lateral compartment. A thorough diagnostic sweep is performed, evaluating the coronoid, the radial head, the capitellum, and the lateral gutter.

The surgeon specifically looks for chondromalacia, loose bodies, and the
Clinical & Radiographic Imaging Archive




