En Bloc Resection of Posterior Thigh Sarcoma: A Masterclass in Hamstring Myomectomy
Key Takeaway
Master the complex en bloc resection of posterior thigh sarcomas, focusing on hamstring myomectomy. This masterclass covers comprehensive anatomy, meticulous intraoperative technique from incision to closure, and critical pearls for preserving the sciatic nerve. Fellows will learn patient positioning, dissection strategies, tumor removal, and essential postoperative management to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of soft tissue sarcomas (STS) of the extremities has undergone a paradigm shift over the past four decades, evolving from radical amputations to sophisticated limb-salvage procedures combined with multimodal adjuvant therapies. Among the various anatomical zones encountered by the orthopedic oncologist, the posterior compartment of the thigh presents a uniquely demanding surgical landscape. En bloc resection of a posterior thigh sarcoma—essentially a radical hamstring myomectomy—is a formidable undertaking that requires an intimate understanding of cross-sectional anatomy, meticulous surgical technique, and a profound respect for the sciatic nerve. This procedure represents a masterclass in balancing aggressive oncologic clearance with the preservation of functional biomechanics.
Posterior thigh sarcomas, while statistically less frequent than their anterior compartment counterparts, encompass a diverse array of histologic subtypes. Pleomorphic dermal sarcomas, myxoid liposarcomas, synovial sarcomas, and malignant peripheral nerve sheath tumors (MPNSTs) are frequently isolated in this region. The insidious nature of these tumors often leads to delayed clinical presentation; patients typically present with a painless, progressively enlarging mass deep within the muscular layers. Because the posterior compartment offers a relatively large potential space, tumors can achieve significant volume before causing mechanical symptoms or compressive neuropathy of the sciatic nerve.
The fundamental oncologic principle dictating the surgical approach is the concept of the pseudocapsule and the reactive zone. Soft tissue sarcomas expand centrifugally, compressing surrounding normal tissue to form a pseudocapsule. However, this pseudocapsule is invariably breached by microscopic satellite tumor cells residing within the adjacent reactive zone. Therefore, a simple "shelling out" or marginal excision is oncologically unacceptable, carrying a local recurrence rate approaching 90%. The absolute surgical objective is an R0 resection—the en bloc removal of the tumor along with a continuous, uninterrupted cuff of normal, healthy tissue in all dimensions.
Achieving this R0 margin in the posterior thigh is complicated by the proximity of critical neurovascular structures. The multidisciplinary tumor board approach is indispensable, integrating the expertise of orthopedic oncologists, musculoskeletal radiologists, radiation oncologists, and medical oncologists. Neoadjuvant radiotherapy is frequently employed to sterilize the reactive zone, effectively thickening the pseudocapsule and potentially allowing for closer, yet oncologically safe, margins near critical structures. The ultimate goal remains unequivocal: eradicate the primary disease, prevent local recurrence, and maximize the patient's postoperative functional capacity and overall quality of life.
Detailed Surgical Anatomy and Biomechanics
Osteology and Muscular Architecture
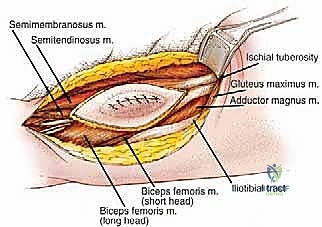
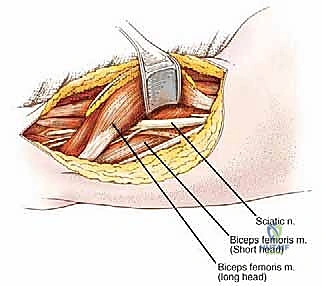
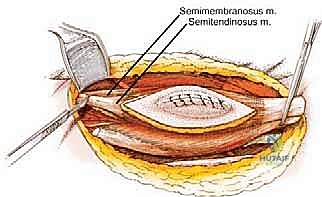
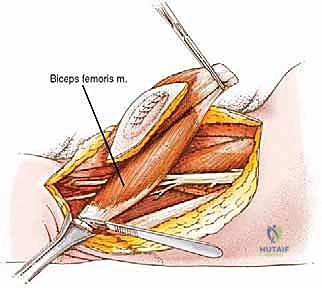
Before initiating any surgical intervention, the operating surgeon must possess an absolute, three-dimensional mastery of the posterior thigh's surgical anatomy. The posterior compartment, commonly referred to as the hamstring compartment, is delineated by three primary muscle bellies originating from the ischial tuberosity: the semimembranosus, the semitendinosus, and the long head of the biceps femoris. Additionally, the short head of the biceps femoris contributes to the lateral aspect of the compartment, originating from the linea aspera and the lateral supracondylar line of the femur.
The semimembranosus descends to insert onto the posterior aspect of the medial tibial condyle, while the semitendinosus transitions into a long, distinct tendon that inserts onto the medial surface of the proximal tibia as part of the pes anserinus. Laterally, the long and short heads of the biceps femoris converge to form a common tendon that inserts onto the head of the fibula and the lateral tibial condyle. Biomechanically, these muscles are the primary flexors of the knee joint and secondary extensors of the hip joint. A complete en bloc resection of this compartment necessitates a profound understanding of these origin and insertion points to ensure complete compartmental clearance when high-grade lesions dictate a radical approach.
The Sciatic Nerve: The Anatomical Dictator
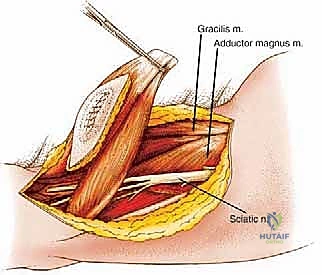
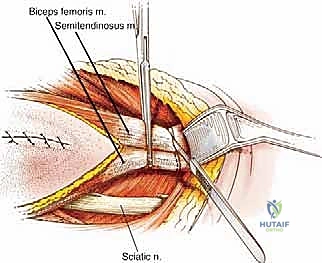
The sciatic nerve is the undisputed anatomical dictator of the posterior compartment. Its preservation, whenever oncologically feasible, is the primary determinant of postoperative limb function. Descending from the greater sciatic foramen, the nerve enters the posterior thigh lateral to the ischial tuberosity and deep to the long head of the biceps femoris. It courses distally along the posterior aspect of the adductor magnus. Typically, in the distal third of the thigh or at the apex of the popliteal fossa, it bifurcates into the tibial nerve and the common peroneal nerve.
Crucially, the sciatic nerve is invested in a robust epineurial sheath. This thick, protective fascial layer often acts as a natural biological barrier, resisting direct tumor invasion. Consequently, even massive sarcomas within the posterior compartment frequently displace, rather than invade, the nerve. This anatomical nuance allows for meticulous epineurial dissection—peeling the nerve away from the tumor's reactive zone—to achieve a marginal, yet functional, limb salvage. However, if the tumor originates directly from the nerve (as in an MPNST) or demonstrates frank macroscopic invasion through the epineurium, an en bloc resection of the sciatic nerve becomes an unavoidable oncologic necessity.
Neurovascular Supply and Compartmental Boundaries
While the posterior compartment lacks a singular, dominant axial artery like the superficial femoral artery in the anterior compartment, its vascular supply is complex and surgically significant. Blood is supplied primarily via a series of perforating branches arising from the profunda femoris artery. These vessels pierce the adductor magnus to enter the posterior compartment, providing robust vascularity to the hamstrings. During resection, these perforators must be systematically identified, isolated, and ligated; failure to do so results in profound hemorrhage that obscures the surgical field and compromises margin assessment.
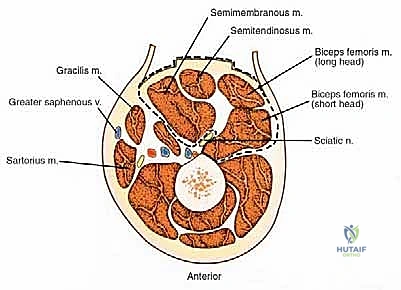
The compartmental boundaries must be rigidly respected during an en bloc resection. The anterior boundary is formed by the posterior intermuscular septum and the posterior surface of the femur (linea aspera). The medial boundary consists of the adductor magnus and gracilis muscles. The lateral boundary is defined by the vastus lateralis and the iliotibial (IT) tract. The posterior boundary is the enveloping fascia lata and the overlying subcutaneous tissue and skin. Understanding these fascial planes allows the surgeon to utilize them as natural barriers, resecting the entire compartment from origin to insertion when necessary.
Exhaustive Indications and Contraindications
The decision to proceed with an en bloc resection of a posterior thigh sarcoma is highly nuanced, requiring a meticulous risk-benefit analysis tailored to the individual patient's tumor biology, anatomical involvement, and physiologic reserve. The absolute indication for this procedure is a biopsy-proven, intermediate- or high-grade soft tissue sarcoma localized to the posterior compartment of the thigh, where preoperative imaging suggests that wide or radical margins can be achieved without compromising the viability of the distal extremity.
Relative indications include low-grade sarcomas or locally aggressive benign neoplasms (such as aggressive fibromatosis/desmoid tumors) that have failed conservative management or are causing progressive neurologic compromise due to sciatic nerve compression. In cases of recurrent sarcoma following previous marginal excision, an en bloc compartmental resection is often the only viable salvage strategy to prevent catastrophic fungating disease or systemic metastasis. The surgeon must carefully weigh the functional morbidity of a massive hamstring resection against the oncologic imperative of local disease control.
Contraindications to limb-salvage surgery in this region are primarily dictated by the inability to achieve negative margins without rendering the limb functionally useless or ischemic. If a tumor circumferentially encases the superficial femoral artery and vein, and vascular reconstruction is deemed impossible due to the extent of disease or patient comorbidities, an amputation (hip disarticulation or high transfemoral) is indicated. Similarly, massive soft tissue destruction that precludes adequate soft tissue coverage, even with free tissue transfer, represents a severe contraindication to limb salvage.
Furthermore, the presence of diffuse skip metastases within the limb, severe and uncorrectable medical comorbidities that prohibit prolonged anesthesia, or an infected, fungating tumor mass with systemic sepsis may force the surgeon to abandon limb salvage in favor of a rapid, life-saving amputation. The decision matrix is complex, and the patient must be extensively counseled regarding the potential for intraoperative conversion to amputation should the intraoperative findings preclude a safe R0 resection.
| Category | Specific Factors | Clinical Implications |
|---|---|---|
| Absolute Indications | Biopsy-proven primary STS isolated to posterior thigh; Ability to achieve R0 margins. | Standard of care for limb salvage; high probability of local control. |
| Relative Indications | Recurrent STS; Desmoid tumors with severe symptoms; Palliative resection for pain control. | Requires careful multidisciplinary planning; higher risk of complications. |
| Absolute Contraindications | Unreconstructable major vascular encasement; Inability to achieve negative margins; Massive skin involvement precluding flap coverage. | Necessitates amputation (hip disarticulation or high transfemoral) to achieve local control. |
| Relative Contraindications | Pathologic fracture of the femur; Extensive skip lesions; Severe cardiopulmonary comorbidities. | May require modified surgical approach, neoadjuvant therapy, or palliative management. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities
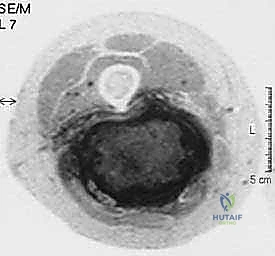
Meticulous preoperative planning is the absolute cornerstone of a successful oncologic resection. The surgical strategy is entirely dependent on high-resolution, multi-planar imaging. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard. We rely on T1-weighted images to assess regional anatomy and marrow involvement, while T2-weighted and STIR (Short Tau Inversion Recovery) sequences are critical for delineating the tumor's pseudocapsule, identifying peritumoral edema (the reactive zone), and mapping the exact relationship of the mass to the sciatic nerve.
Computed Tomography (CT) of the affected extremity is utilized specifically to evaluate cortical bone integrity. If the tumor abuts the linea aspera or the ischial tuberosity, CT provides superior detail regarding cortical erosion or frank bony invasion, which would mandate an en bloc resection of the involved bone (e.g., a partial cortical excision or a segmental femoral resection). Furthermore, staging imaging, including a high-resolution CT of the chest to rule out pulmonary metastases, is mandatory prior to any definitive surgical intervention.

Surgical Templating and Margin Delineation
Based on the advanced imaging, the surgeon meticulously templates the resection margins. For high-grade sarcomas, the standard approach is a wide excision, aiming for a margin of normal tissue in all directions. In the posterior thigh, this often translates to a complete myomectomy of the involved hamstring muscle from origin to insertion. The fascial boundaries of the compartment are mapped out as the planned surgical margins. If the tumor is in close proximity to the sciatic nerve, the surgical plan must explicitly state whether the nerve will be dissected free (epifascicular dissection) or sacrificed en bloc.
In cases where the tumor extends distally into the popliteal fossa, the relationship to the popliteal artery and vein becomes critical. Preoperative CT angiography or conventional angiography may be indicated to map the vascular tree and plan for potential vascular bypass or reconstruction. The surgical team must be prepared with appropriate vascular conduits (e.g., reversed saphenous vein graft) and the necessary expertise to perform microvascular anastomoses if the popliteal vessels must be sacrificed to achieve negative margins.
Patient Positioning and Operating Room Setup
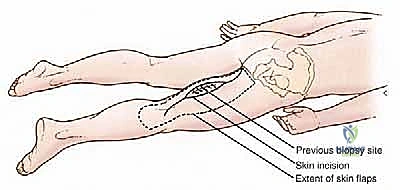
The patient is positioned prone on the operating table, a posture that provides unparalleled, unhindered access to the entire posterior thigh, gluteal region, and popliteal fossa. Meticulous attention to padding is paramount to prevent devastating decubitus ulcers and peripheral nerve palsies. Chest rolls are placed longitudinally from the clavicle to the iliac crest to ensure adequate respiratory excursion and prevent abdominal compression, which can lead to increased venous bleeding via the epidural venous plexus.
The arms are carefully positioned on padded arm boards, typically abducted less than 90 degrees and slightly externally rotated, to rigorously avoid brachial plexus traction injuries. The knees and ankles are supported with gel pads, ensuring the toes are free-floating. The operating room setup must include immediate access to intraoperative C-arm fluoroscopy to confirm proximal bony landmarks (such as the ischial tuberosity) if required. Intraoperative nerve monitoring, including somatosensory evoked potentials (SSEPs) and direct electromyography (EMG), is frequently utilized to assist in identifying and protecting the sciatic nerve during complex dissections.

Step-by-Step Surgical Approach and Fixation Technique
Incision Planning and Flap Elevation
The surgical approach begins with a meticulously planned longitudinal incision over the posterior thigh. The precise placement is dictated by the tumor's location and, critically, the site of the previous percutaneous core needle biopsy. The biopsy tract is considered contaminated with malignant cells and must be excised en bloc with the primary tumor. We outline a generous ellipse of skin incorporating the biopsy scar, ensuring a minimum of a 2-cm margin of healthy skin in all directions. The longitudinal incision is then extended proximally toward the gluteal fold and distally toward the popliteal fossa as needed for adequate exposure.
Using electrocautery, the skin incision is deepened, and robust fasciocutaneous flaps are raised medially and laterally. The thickness of these flaps is critical; they must be raised just superficial to the deep investing fascia of the thigh (fascia lata) to ensure adequate vascularity and prevent postoperative skin necrosis. The medial flap is dissected until the border of the gracilis muscle is identified, while the lateral flap is elevated to expose the iliotibial (IT) tract. This wide exposure is essential for visualizing the entire compartmental anatomy and establishing control of the normal tissues surrounding the tumor.

Deep Fascial Incision and Proximal/Distal Control
Once the fasciocutaneous flaps are widely retracted, the deep fascia is incised longitudinally, far away from the palpable tumor mass. The fundamental principle of oncologic surgery is to approach the tumor from known, normal anatomy into the abnormal. We begin by identifying the normal hamstring musculature well proximal and distal to the reactive zone. By establishing control of the normal tissues first, we can safely mobilize the entire compartment without inadvertently breaching the tumor pseudocapsule.
The proximal dissection involves identifying the origins of the hamstrings at the ischial tuberosity. Depending on the proximal extent of the tumor, the muscles may be detached directly from the bone using heavy electrocautery or an osteotome. Distally, the tendons of the semimembranosus, semitendinosus, and biceps femoris are identified and isolated. If a complete compartmental resection is required, these tendons are transected near their insertions on the tibia and fibula. This proximal and distal isolation effectively creates a mobile, isolated block of tissue containing the tumor.

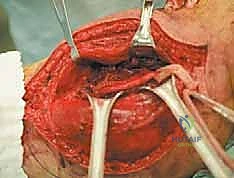
Sciatic Nerve Neurolysis and Vascular Ligation
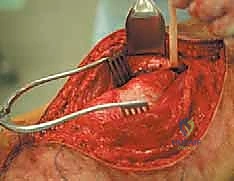
The most critical and technically demanding phase of the operation is the management of the sciatic nerve. The nerve must be identified in virgin, unscarred tissue, typically high in the proximal thigh near the gluteus maximus border, or distally in the popliteal fossa. Once identified, it is encircled with a vessel loop and meticulously traced toward the tumor mass. If the nerve is merely displaced by the tumor, a careful epineurial dissection is performed. Using magnifying loupes and tenotomy scissors, the surgeon separates the nerve from the tumor's pseudocapsule, leaving the thick epineurium intact as the surgical margin.
Simultaneously, the vascular supply to the posterior compartment must be systematically dismantled. As the hamstring block is mobilized medially or laterally, the perforating branches of the profunda femoris artery are encountered piercing the adductor magnus. These vessels are short, friable, and under high pressure. They must be individually isolated, securely clamped, and ligated with heavy non-absorbable sutures or surgical clips. Indiscriminate use of electrocautery on these perforators frequently leads to retraction into the adductor compartment, resulting in massive, difficult-to-control hemorrhage.

En Bloc Resection and Defect Reconstruction
With the sciatic nerve safely mobilized and protected, and the vascular perforators ligated, the deep margin of the resection is addressed. This often involves dissecting along the posterior surface of the adductor magnus and the linea aspera of the femur. If the tumor is adherent to the periosteum, a sharp periosteal elevator is used to strip the periosteum en bloc with the tumor. In cases of frank cortical involvement, a motorized burr or oscillating saw is used to perform a partial cortical excision, ensuring an adequate bony margin.
Once the entire specimen is freed, it is delivered from the wound en bloc and immediately oriented for the pathologist with surgical clips or sutures. The massive resulting defect is then meticulously irrigated with sterile water (to lyse any potential free-floating tumor cells via osmotic shock) and inspected for hemostasis. Due to the deep, dead space created by a total hamstring myomectomy, closed suction drains are mandatory. While primary closure of the fasciocutaneous flaps is often possible, massive resections or irradiated fields may require the expertise of a plastic surgeon for local muscle rotational flaps (e.g., a pedicled gastrocnemius flap) or split-thickness skin grafting to achieve tension-free coverage.

Complications, Incidence Rates, and Salvage Management
Wound Healing and Infectious Complications
The most frequent complications following radical resection of posterior thigh sarcomas are related to wound healing. The incidence of major wound complications (dehiscence, deep infection, flap necrosis) ranges from 15% to 35%, and this rate is significantly amplified if the patient has received neoadjuvant radiotherapy. The radiation damages the microvasculature, leading to tissue hypoxia and impaired fibroblast proliferation. Seroma formation is also ubiquitous due to the massive dead space created by the myomectomy.
Management of these wound complications requires aggressive, early intervention. Superficial dehiscence may be managed with local wound care, but deep infections or significant flap necrosis mandate immediate return to the operating room for radical debridement. Negative Pressure Wound Therapy (NPWT/VAC dressings) is highly effective in managing large dead spaces and promoting granulation tissue. In severe cases where critical structures (like the sciatic nerve or femur) are exposed, reconstructive plastic surgery utilizing pedicled or free tissue transfer is required to salvage the limb and prevent catastrophic secondary hemorrhage.
Neurologic and Vascular Deficits
Neurologic complications are directly related to the manipulation or resection of the sciatic nerve. Transient neuropraxia due to traction or epineurial dissection occurs in approximately 10-20% of cases and typically resolves over several months. However, if the sciatic nerve is sacrificed en bloc to achieve oncologic margins, the patient will suffer a permanent, profound deficit. This manifests as a complete loss of motor function below the knee (foot drop, loss of plantar flexion) and loss of sensation in the foot and lateral leg.
Vascular injuries, particularly to the profunda femoris perforators or the popliteal vessels, can lead to significant intraoperative hemorrhage or postoperative hematoma formation. Deep Vein Thrombosis (DVT) is a significant risk due to
