Masterclass in Wide Resection and Reconstruction of Soleus Muscle Sarcomas
Key Takeaway
This masterclass guides orthopaedic fellows through wide soleus muscle sarcoma resection. We cover meticulous preoperative planning, detailed surgical anatomy, precise intraoperative steps including neurovascular protection, and advanced Gore-Tex reconstruction techniques. Emphasis is placed on achieving negative margins while preserving limb function. Postoperative care and complication management are also thoroughly discussed, ensuring comprehensive understanding of this challenging procedure.
Comprehensive Introduction and Patho-Epidemiology
The management of soft tissue sarcomas of the lower extremity represents one of the most profound evolutions in modern orthopedic oncology. Historically, the diagnosis of a high-grade sarcoma deep within the posterior compartment of the leg was an unequivocal mandate for above-knee amputation. The sheer anatomical density of the popliteal fossa and the deep posterior compartment, coupled with the aggressive biological behavior of these tumors, made limb-salvage a perilous endeavor fraught with unacceptable rates of local recurrence. However, the contemporary era of orthopedic oncology has witnessed a paradigm shift, driven by high-resolution multi-planar imaging, refined neoadjuvant chemoradiation protocols, and advanced microvascular reconstructive techniques. Today, limb-salvage surgery is not merely an alternative; it is the gold standard, achieving equivalent overall survival rates to amputation while preserving a functional, sensate limb.
Malignant tumors arising primarily within the soleus muscle are relatively rare, representing a distinct subset of lower extremity soft tissue sarcomas. The most frequently encountered histologies in this anatomical region include undifferentiated pleomorphic sarcoma (formerly malignant fibrous histiocytoma), synovial sarcoma, liposarcoma, and alveolar soft part sarcoma. Each of these histotypes exhibits unique biological behaviors, metastatic predilections, and responses to systemic therapies. For instance, alveolar soft part sarcomas, often found in younger patients, are notoriously vascular and have a high propensity for early pulmonary and cerebral metastasis, necessitating meticulous systemic staging and often dictating a robust neoadjuvant approach prior to surgical intervention.
The successful execution of a wide resection of a soleus sarcoma is a formidable surgical challenge that demands a masterful command of lower extremity anatomy. The surgeon must navigate a three-dimensional labyrinth of critical neurovascular structures, most notably the popliteal trifurcation and the tibial nerve, which often lie in perilous proximity to the tumor pseudocapsule. The overarching objective of the procedure is uncompromising: the en bloc resection of the tumor with a contiguous cuff of normal, healthy tissue in all dimensions to achieve negative (R0) oncologic margins. Compromising the margin to spare a nerve or vessel is an oncologic failure that invariably leads to local recurrence, a scenario that exponentially increases the morbidity of subsequent salvage procedures and significantly diminishes overall survival.
Achieving this delicate balance between oncologic radicality and functional preservation requires a highly orchestrated, multidisciplinary approach. The orthopedic oncologist does not operate in a vacuum; success is predicated on seamless collaboration with musculoskeletal radiologists, soft tissue pathologists, medical oncologists, radiation oncologists, and often, plastic and microvascular surgeons. The preoperative tumor board is the crucible where the surgical strategy is forged, synthesizing imaging data, biopsy histology, and the patient's physiological reserve to formulate a bespoke treatment algorithm. When executed with precision, the wide resection and reconstruction of a soleus sarcoma epitomizes the pinnacle of limb-salvage surgery, restoring the patient not just to life, but to a life of mobility and independence.
Detailed Surgical Anatomy and Biomechanics
Osteology and Compartmental Architecture
A profound, almost intuitive understanding of the posterior compartment's architectural framework is the absolute prerequisite for safe navigation during soleus resection. The leg is divided into four distinct fascial compartments: anterior, lateral, superficial posterior, and deep posterior. The superficial and deep posterior compartments are separated by the transverse intermuscular septum, a critical fascial condensation that serves as both an anatomical boundary and a potential barrier to tumor extension. The superficial posterior compartment houses the triceps surae—the medial and lateral heads of the gastrocnemius and the underlying soleus—along with the diminutive plantaris muscle.
The osteological boundaries of this region dictate the potential vectors of tumor expansion and the necessary extent of surgical exposure. The posterior surfaces of the tibia and fibula, connected by the robust interosseous membrane, form the unyielding anterior floor of the posterior compartments. Tumors arising in the deep aspect of the soleus can exert significant pressure against these osseous structures, potentially inducing periosteal reaction or, in aggressive cases, direct cortical invasion. The proximal origin of the soleus is particularly complex, arising in a horseshoe configuration from the posterior aspect of the fibular head, the proximal third of the fibular shaft, the soleal line of the tibia, and a dense, fibrous tendinous arch that spans the interosseous space.
This tendinous arch of the soleus is a structure of paramount surgical significance. It forms a rigid anatomical hiatus through which the popliteal artery, popliteal vein, and tibial nerve transition from the popliteal fossa into the deep posterior compartment. Tumors located in the proximal soleus frequently abut or encase this hiatus, making the dissection in this specific zone the most treacherous phase of the operation. The surgeon must meticulously release this arch to mobilize the neurovascular bundle, a maneuver that requires exceptional precision to avoid catastrophic hemorrhage or profound denervation of the distal extremity.
The Triceps Surae Complex and Achilles Mechanism
The triceps surae is the primary biomechanical engine of the lower extremity, generating the immense plantar flexion torque required for the push-off phase of the gait cycle. The gastrocnemius, a biarticular muscle with origins on the medial and lateral femoral condyles, crosses both the knee and the ankle joints. It functions primarily as a fast-twitch, power-generating muscle, highly active during sprinting and jumping. In contrast, the soleus is a uniarticular muscle, crossing only the ankle joint. Composed predominantly of slow-twitch muscle fibers, it is the tireless workhorse of posture and sustained ambulation, constantly fine-tuning ankle position to maintain the body's center of gravity over the base of support.
The convergence of these three muscle bellies forms the Achilles tendon, the thickest and strongest tendon in the human body. The aponeurosis of the anterior aspect of the gastrocnemius joins the aponeurosis of the posterior aspect of the soleus to form a conjoint tendon that inserts into the posterior calcaneal tuberosity. During a wide resection of the soleus, the biomechanical integrity of this complex is invariably compromised. If the entire soleus must be resected, the patient will experience a significant, though often clinically tolerable, deficit in sustained plantar flexion endurance.
However, if the resection requires the sacrifice of the overlying gastrocnemius or a substantial portion of the Achilles tendon itself to achieve negative margins, the resulting functional deficit is profound. In such instances, the reconstructive phase of the operation becomes just as critical as the extirpative phase. The surgeon must employ advanced reconstructive techniques, such as flexor hallucis longus (FHL) tendon transfer or the use of massive allografts, to restore continuity and tension to the Achilles mechanism. Failure to adequately reconstruct the plantar flexion apparatus will leave the patient with a devastating calcaneal gait, characterized by an inability to propel the body forward, rendering the salvaged limb functionally inferior to a well-fitted modern prosthesis.
Neurovascular Topography of the Posterior Leg
The popliteal fossa and the deep posterior compartment are densely packed with vital neurovascular structures that dictate the limits of surgical resection. The popliteal artery, the direct continuation of the superficial femoral artery, enters the popliteal fossa through the adductor hiatus and descends vertically. At the distal border of the popliteus muscle, it undergoes a critical trifurcation, dividing into the anterior tibial artery, the posterior tibial artery, and the peroneal artery. The posterior tibial artery and the peroneal artery run deep to the soleus muscle, accompanied by their respective venae comitantes.
The innervation of the posterior compartment is equally complex and critical. The sciatic nerve typically bifurcates at the apex of the popliteal fossa into the common peroneal nerve and the tibial nerve. The tibial nerve continues vertically down the midline of the fossa, superficial to the popliteal vessels, and passes deep to the tendinous arch of the soleus. It provides motor branches to the superficial and deep posterior compartment musculature and sensory innervation to the plantar aspect of the foot. The common peroneal nerve courses laterally, hugging the medial border of the biceps femoris tendon before wrapping around the fibular neck.
During the resection of a soleus sarcoma, the preservation of the tibial nerve is the absolute priority. While the sacrifice of one or even two of the trifurcation vessels can often be tolerated due to the robust collateral circulation of the leg, the resection of the tibial nerve results in a profoundly insensate plantar foot and a complete loss of active plantar flexion. An insensate foot in a limb-salvage patient is highly susceptible to unrecognized trauma, chronic ulceration, and catastrophic deep infection, often culminating in a delayed, highly morbid amputation. Therefore, if preoperative imaging or intraoperative exploration reveals that the tumor irresectably encases the tibial nerve, the surgeon must be prepared to abandon limb-salvage and proceed with an above-knee amputation.
Exhaustive Indications and Contraindications
Patient Selection for Limb Salvage
The decision to proceed with a wide resection and limb-salvage surgery for a soleus sarcoma is highly individualized, requiring a meticulous synthesis of oncologic, anatomical, and patient-specific variables. The primary indication for this procedure is a biopsy-proven, primary malignant soft tissue sarcoma that is anatomically confined to the superficial posterior compartment of the leg, specifically arising within or primarily involving the soleus muscle. The tumor must be amenable to en bloc resection with negative margins without compromising the critical neurovascular structures required for a viable, functional limb.
Patient selection extends beyond the anatomical characteristics of the tumor. The physiological age, medical comorbidities, and postoperative functional demands of the patient must be rigorously evaluated. Limb-salvage surgery is an arduous undertaking, often requiring prolonged operative times, significant blood loss, and a grueling, months-long rehabilitation protocol. Patients with severe peripheral vascular disease, poorly controlled diabetes mellitus, or profound cardiopulmonary compromise may not tolerate the physiological stress of the procedure or the subsequent wound healing demands. In such frail populations, a primary amputation, which offers a faster definitive oncologic clearance and a more rapid return to baseline mobility with a prosthesis, may be the more prudent and compassionate choice.
Furthermore, the patient's psychological resilience and adherence to complex postoperative instructions are critical determinants of success. The rehabilitation following a major muscle resection and tendon reconstruction requires intense dedication to physical therapy and strict adherence to weight-bearing restrictions. Patients who lack the cognitive capacity, social support network, or personal motivation to engage in this rigorous process are at a high risk for reconstructive failure, joint contractures, and chronic pain, ultimately resulting in a limb that is a burden rather than a benefit.
Oncologic and Anatomic Prerequisites
The oncologic prerequisites for limb-salvage are absolute: the surgeon must be confident in the ability to achieve R0 margins. If achieving a negative margin requires leaving the patient with a flail, insensate, or ischemic limb, the procedure is contraindicated. Neoadjuvant therapies, particularly external beam radiation therapy and systemic chemotherapy, play a pivotal role in converting marginally resectable tumors into clearly resectable ones. Radiation therapy induces tumor necrosis and pseudocapsule thickening, effectively sterilizing the peripheral reactive zone and allowing for closer, yet oncologically safe, surgical margins.
Anatomical contraindications are primarily dictated by the tumor's relationship to the popliteal neurovascular bundle and the underlying bone. While the encasement of a single distal vessel (e.g., the posterior tibial artery) can often be managed with vascular ligation or bypass grafting, the extensive involvement of the popliteal artery proximal to the trifurcation significantly escalates the complexity and risk of the procedure. Similarly, while focal periosteal involvement can be addressed with an en bloc cortical window resection, extensive medullary invasion of the tibia or fibula necessitates an intercalary bone resection and complex osteoarticular reconstruction, moving the procedure beyond the scope of a standard soft tissue resection.
| Category | Indications for Wide Resection | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anatomical | Tumor confined to soleus/superficial posterior compartment. | Circumferential encasement of the main Tibial Nerve. | Encasement of the Popliteal Artery requiring complex bypass. |
| Oncologic | Biopsy-proven sarcoma, achievable R0 margins. | Inability to achieve negative margins without amputation. | Extensive fungating tumor with severe skin involvement. |
| Osseous | No bone involvement, or minimal periosteal reaction. | Massive medullary invasion of Tibia/Fibula. | Focal cortical invasion requiring large intercalary resection. |
| Patient Factors | Good physiological reserve, compliant with rehab. | Severe peripheral vascular disease, insensate foot pre-op. | Poorly controlled diabetes, severe cardiopulmonary disease. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities and Staging
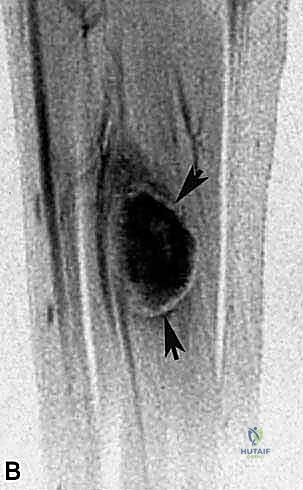
The battle for a successful limb-salvage is invariably won or lost in the preoperative planning phase. The cornerstone of this planning is high-resolution, multi-planar Magnetic Resonance Imaging (MRI) with and without intravenous contrast. We demand T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences in axial, coronal, and sagittal planes. The MRI serves as the definitive roadmap, allowing us to precisely delineate the tumor's volume, its intramedullary or extramedullary extension, and its critical spatial relationship to the popliteal trifurcation, the tibial nerve, and the fascial boundaries of the posterior compartment.
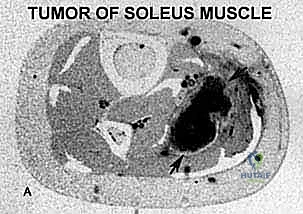
We scrutinize every single axial slice to identify the "pinch points"—the areas where the tumor pseudocapsule comes within millimeters of critical structures. If the tumor abuts the bone, we look for loss of the low-signal cortical line, which suggests periosteal invasion. If the tumor is proximal, we meticulously trace the path of the popliteal vessels and the tibial nerve through the tendinous arch of the soleus.
Complementary imaging is equally vital. A high-resolution Computed Tomography (CT) scan of the chest is mandatory for all high-grade sarcomas to rule out pulmonary metastasis, the most common site of distant spread. A whole-body technetium-99m bone scan is routinely obtained to evaluate for osseous metastases and to further assess any suspicious areas of cortical uptake adjacent to the primary tumor. In cases where the MRI suggests vascular encasement or significant displacement, a CT angiogram or conventional biplane angiography is invaluable. This allows us to map the precise vascular anatomy, identify the dominant arterial supply to the foot, and plan for potential vascular reconstruction or bypass if major vessel sacrifice is anticipated.
Biopsy Principles and Tract Management
The biopsy is not merely a diagnostic prerequisite; it is the first, and arguably most critical, surgical step in the management of a sarcoma. A poorly planned or executed biopsy can contaminate virgin tissue planes, seed the neurovascular bundle with tumor cells, and irrevocably convert a resectable tumor into an amputation. The absolute cardinal rule of orthopedic oncology is that the biopsy tract must be considered contaminated with tumor cells and must be excised en bloc with the definitive specimen.
For soleus sarcomas, we strongly advocate for an image-guided core needle biopsy. This technique provides sufficient tissue architecture for accurate histopathological grading and molecular subtyping while minimizing tissue trauma and hematoma formation. The biopsy trajectory must be meticulously planned in direct consultation with the operating surgeon. The needle must be introduced through the posterior midline of the calf, directly over the bulk of the tumor, ensuring that the entire tract lies within the planned elliptical skin incision for the definitive resection.
Under no circumstances should the biopsy needle traverse the anterior or lateral compartments, nor should it be directed near the popliteal fossa or the course of the common peroneal nerve. Trans-compartmental biopsies contaminate multiple surgical planes, requiring massive, morbid resections to achieve clear margins. Furthermore, meticulous hemostasis must be achieved at the biopsy site to prevent a tracking hematoma, which can disseminate tumor cells extensively through the subcutaneous tissues and fascial planes, drastically expanding the required volume of resection.
Patient Positioning and Operative Room Setup
The physical setup of the operating room and the positioning of the patient are critical for ensuring optimal exposure and safety during this exhaustive procedure. Following the induction of general endotracheal anesthesia, the patient is carefully transitioned onto the operating table in the prone position. This is a highly coordinated maneuver requiring the entire surgical and anesthesia team to protect the airway and prevent cervical spine injury.
Once prone, meticulous attention is paid to pressure point padding. The face is placed in a specialized foam prone-view helmet to protect the eyes from pressure necrosis and ensure endotracheal tube patency. The chest and pelvis are supported on longitudinal gel rolls to allow for unhindered diaphragmatic excursion and to decompress the abdomen, which minimizes venous engorgement and reduces intraoperative bleeding. The knees are slightly flexed, and the ankles are supported on a padded bolster to prevent excessive tension on the Achilles tendon and the posterior neurovascular structures.
The entire lower extremity, from the gluteal fold to the tips of the toes, is meticulously prepped and draped in a sterile fashion. We utilize a sterile tourniquet placed high on the proximal thigh. While the tourniquet is applied, we routinely do not inflate it at the beginning of the case. Operating without a tourniquet allows for the continuous assessment of tissue perfusion, immediate identification of vascular injury, and precise hemostasis as the dissection proceeds. The tourniquet is held in reserve, to be inflated only in the event of catastrophic, uncontrolled hemorrhage from the popliteal vessels. A radiolucent operating table is mandatory, and a C-arm fluoroscopy unit is positioned in the room, ready for immediate deployment if intraoperative assessment of osseous margins or vascular flow is required.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Flap Elevation, and Exposure
The surgical approach begins with a meticulously planned incision designed to provide extensile exposure while facilitating primary closure or local flap coverage. A longitudinal, posterior midline incision is typically employed, extending from the distal aspect of the popliteal fossa down to the musculotendinous junction of the Achilles tendon. The incision must be designed as an ellipse to incorporate the entire biopsy tract, including the skin puncture site and the underlying subcutaneous tissue.
Using a #10 scalpel, the skin and subcutaneous tissues are incised down to the deep fascia of the leg. It is imperative to raise thick, full-thickness fasciocutaneous flaps medially and laterally. We utilize sharp dissection with Metzenbaum scissors and precise electrocautery to separate the subcutaneous fat from the underlying deep fascia, preserving the delicate subdermal vascular plexus. Thin flaps are highly prone to marginal necrosis, a devastating complication that exposes the underlying reconstructed tissues and neurovascular structures to desiccation and infection.
As the flaps are elevated, we identify and protect the lesser saphenous vein and the sural nerve, which course vertically in the posterior midline. Depending on the tumor's superficial extent, these structures may need to be sacrificed and resected en bloc with the specimen to ensure adequate margins. The deep fascia is then incised longitudinally, exposing the gleaming epimysium of the medial and lateral heads of the gastrocnemius muscle.
Neurovascular Dissection and Protection
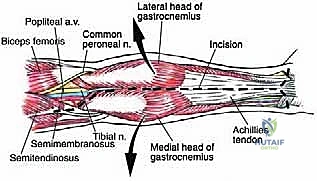
Before any deep dissection or tumor manipulation occurs, the critical neurovascular structures must be definitively identified and secured. This is the most perilous phase of the operation. We begin laterally, carefully dissecting the subcutaneous tissues overlying the fibular head to identify the common peroneal nerve. The nerve is traced from its origin at the sciatic bifurcation, around the fibular neck, and into the anterior compartment. A vessel loop is gently passed around the nerve to allow for atraumatic retraction and continuous visual confirmation of its safety throughout the procedure.

Attention is then directed to the proximal extent of the incision in the popliteal fossa. The deep fascia is carefully opened, and the fat of the popliteal fossa is gently teased apart using blunt dissection and right-angle forceps. The tibial nerve is identified as the most superficial and lateral structure within the central neurovascular bundle. It is meticulously mobilized and protected with a vessel loop.
Deep and medial to the tibial nerve lies the popliteal vein, and deeper still, resting against the posterior capsule of the knee joint, is the popliteal artery. These vessels are traced distally to the tendinous arch of the soleus. If the tumor encroaches upon this hiatus, the arch must be carefully divided to allow the vessels and nerve to fall away from the tumor pseudocapsule. Small, bridging venous branches are meticulously ligated with fine silk ties or surgical clips; relying solely on electrocautery in this dense vascular network is an invitation for postoperative hematoma.
Gastrocnemius Mobilization and Soleus Resection
With the neurovascular structures secured, the exposure of the deep-seated soleus tumor requires the mobilization of the overlying gastrocnemius muscle. The medial and lateral sural arteries, which provide the dominant blood supply to the respective gastrocnemius heads, are identified as they branch from the popliteal artery. If the entire triceps surae must be resected, these pedicles are ligated. However, if the gastrocnemius is clinically free of tumor and can be spared to maintain function and provide soft tissue coverage, these pedicles are meticulously preserved.

To access the soleus, the raphe between the medial and lateral heads of the gastrocnemius is sharply divided. The origins of the gastrocnemius heads from the femoral condyles can be released if maximal proximal exposure is required. The gastrocnemius muscle bellies are then reflected medially and laterally, revealing the underlying soleus and the encapsulated sarcoma.
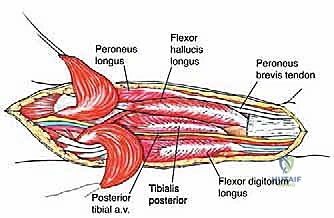
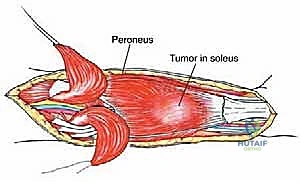
The resection of the soleus proceeds from distal to proximal. The soleus contribution to the Achilles tendon is transected with a generous margin distal to the tumor. The muscle is then elevated off the deep transverse intermuscular septum, which separates it from the deep posterior compartment (tibialis posterior, flexor digitorum longus, flexor hallucis longus).
The dissection plane must remain strictly extra-capsular, taking a cuff of normal muscle and fascia with the tumor. As the dissection proceeds proximally, extreme caution is exercised as the soleus is detached from its origins on the tibia and fibula. The posterior tibial vessels and the tibial nerve, lying immediately deep to the soleus, are kept under direct vision and continuously protected with a retractor. The en bloc specimen is finally delivered from the wound, oriented with sutures for the pathologist, and sent for immediate frozen section analysis of the margins.
Defect Reconstruction and Soft Tissue Coverage
The creation of a massive defect in the posterior compartment necessitates a robust and meticulously planned reconstruction. If the resection required the sacrifice of the popliteal artery or its major trifurcation branches, immediate vascular reconstruction is paramount.

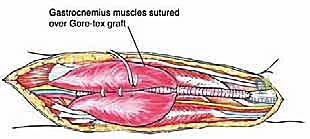
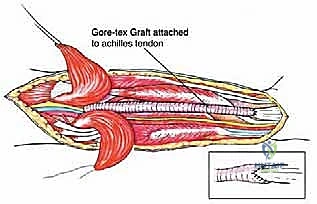
As demonstrated in complex cases, if a primary end-to-end anastomosis is impossible due to the length of the resected segment, an interposition graft must be utilized. While reversed saphenous vein from the contralateral leg is the autologous conduit of choice, a synthetic Gore-Tex (ePTFE) vascular graft can be employed effectively to bridge large defects and restore pulsatile flow to the distal extremity.

Following vascular restoration, attention turns to functional reconstruction. If the soleus alone was resected, the preserved gastrocnemius heads can often be re-approximated
Clinical & Radiographic Imaging Archive