Endoscopic Resection of Posterior Ankle Impingement: An Intraoperative Masterclass
Key Takeaway
Master the endoscopic treatment of posterior ankle impingement. This immersive guide details patient selection, comprehensive anatomy, meticulous intraoperative steps for os trigonum resection, and critical neurovascular safeguards. Learn to manage FHL pathology, prevent complications, and guide postoperative recovery for optimal patient outcomes, especially in high-demand athletes.
Comprehensive Introduction and Patho-Epidemiology
Posterior Ankle Impingement Syndrome (PAIS) represents a fascinating and often debilitating spectrum of hindfoot pathology characterized by chronic posterior ankle pain, which is classically exacerbated by forced or extreme plantarflexion. This clinical disorder is a common culprit in the athletic population, particularly among classical ballet dancers, elite soccer players, cricket fast bowlers, and gymnasts. In these disciplines, repetitive and extreme plantarflexion creates a mechanical abutment between the posterior tibial plafond and the superior aspect of the calcaneal tuberosity, resulting in what is ubiquitously referred to in orthopedic literature as the "nutcracker effect."
The nomenclature surrounding this syndrome is historically dense and varied, encompassing terms such as posterior block of the ankle, posterior triangle pain, talar compression syndrome, os trigonum syndrome, and nutcracker-type syndrome. Regardless of the specific terminology employed, the underlying pathophysiological cascade consistently involves the mechanical compression, crushing, or entrapment of intervening soft tissues or osseous structures. The most common offending osseous structures are an unfused os trigonum or a hypertrophic posterolateral process of the talus (often referred to as a Stieda process).

Pathogenesis is heavily rooted in either acute traumatic events or, more frequently, insidious repetitive microtrauma. When the ankle is forced into hyper-plantarflexion, the posterior capsuloligamentous complex and the synovial lining are subjected to immense compressive forces. Over time, this repetitive mechanical insult precipitates a cascade of chronic inflammation, reactive synovial hypertrophy, and capsular thickening. In cases involving an os trigonum, the synchondrosis connecting the ossicle to the main body of the talus may undergo repetitive stress fracturing or disruption, leading to a painful pseudoarthrosis. Furthermore, severe inversion ankle sprains can result in avulsion injuries of the posterior talofibular ligament (PTFL), which attaches directly to the os trigonum or posterior talar process, thereby destabilizing the region and inciting secondary impingement.
Understanding the epidemiology of PAIS requires an appreciation of the unique biomechanical demands placed on the affected patient populations. In ballet dancers performing en pointe or demi-pointe, the ankle and subtalar joints are forced into maximum plantarflexion, utilizing the posterior talar structures as a bony block to achieve stability. If the osseous anatomy is hypertrophic or if an os trigonum is present, this physiological block becomes pathological. Similarly, soccer players experience this mechanism during the follow-through phase of a powerful instep strike. Recognizing these demographic and biomechanical patterns is the first critical step in accurately diagnosing and effectively managing this complex syndrome.
Detailed Surgical Anatomy and Biomechanics
Mastery of the posterior ankle anatomy is the absolute prerequisite for safe and effective endoscopic intervention. This anatomical region is a highly condensed, complex crossroads of tendinous, ligamentous, and critical neurovascular structures. The margin for error is exceedingly narrow, demanding that the operating surgeon possesses a meticulous, three-dimensional understanding of the posterior hindfoot architecture.
Osteology of the Posterior Ankle
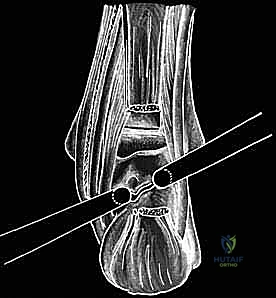
The focal point of posterior ankle osteology is the posterior process of the talus. This structure is anatomically divided by the sulcus for the flexor hallucis longus (FHL) tendon into a smaller posteromedial process and a larger, more prominent posterolateral process (the trigonal process). The os trigonum, when present, represents a secondary ossification center of the posterolateral talus. It typically begins to mineralize between the ages of 8 and 13 years. In the majority of the population, it fuses with the main body of the talus within one year of its appearance, forming the Stieda process. However, in approximately 1.7% to 7% of normal feet, this fusion fails to occur, leaving a separate ossicle that is often unilateral but can be bilateral in up.
When persisting as an independent entity, the os trigonum is a fully corticalized structure exhibiting three distinct anatomical surfaces. The anterior surface articulates with the posterolateral tubercle of the talus via a fibrous, fibrocartilaginous, or cartilaginous interface, effectively forming a synchondrosis. The inferior surface is articular and contributes to the posterior facet of the subtalar (talocalcaneal) joint. The posterior surface is non-articular, serving as a critical anchor point for the posterior talofibular ligament (PTFL) and the posterior talocalcaneal ligament. Understanding these attachments is vital during endoscopic resection, as these ligaments must be carefully released to mobilize and extract the ossicle.
Ligamentous and Tendinous Architecture
The ligamentous constraints of the posterior ankle contribute significantly to both stability and potential impingement. The PTFL, a key component of the lateral collateral ligament complex, traverses from the fibular malleolus to attach firmly onto the posterior surface of the os trigonum or the posterolateral talar tubercle. The posterior talocalcaneal ligament spans the gap between the talus and calcaneus posteriorly, often blending with the posterior joint capsule. Additionally, the deep layer of the flexor retinaculum forms the unyielding fibrous tunnels that house the deep posterior compartment tendons, while the fibuloastragalocalcaneal ligament of Rouviere and Canela Lazaro provides supplementary regional stability.

The tendinous anatomy is dominated by the contents of the deep posterior compartment: the tibialis posterior, the flexor digitorum longus (FDL), and the flexor hallucis longus (FHL). The FHL is of paramount surgical importance in posterior ankle endoscopy. It descends through a distinct fibro-osseous tunnel, utilizing the sulcus between the posteromedial and posterolateral processes of the talus as a pulley. Because of its intimate physical relationship with the os trigonum and the posterior joint capsule, the FHL is highly susceptible to secondary tenosynovitis in the setting of PAIS. The FHL tendon serves as the defining medial boundary of the safe working zone during endoscopic surgery; dissection medial to this structure is strictly contraindicated.
The Neurovascular Bundle: The Critical Zone
The most unforgiving aspect of posterior ankle anatomy is the proximity of the posterior tibial neurovascular bundle. Located immediately medial and superficial to the FHL tendon at the level of the ankle joint, this bundle contains the tibial nerve, the posterior tibial artery, and the accompanying venae comitantes. The tibial nerve is typically the most lateral structure within the bundle, placing it closest to the surgical field.
Iatrogenic injury to these structures carries catastrophic consequences. Damage to the tibial nerve can result in profound sensory deficits across the plantar aspect of the foot and motor weakness of the intrinsic foot musculature. Arterial or venous laceration can precipitate massive hemorrhage, obscure the endoscopic visual field entirely, and potentially lead to acute compartment syndrome of the deep posterior compartment. Furthermore, surgeons must be acutely aware of a rare but critical anatomical variant (present in 0–2% of cases) where the posterior tibial artery is hypoplastic or absent, and vascular supply to the foot is provided by a dominant peroneal artery that traverses the posterior ankle directly across the surgical field. Preoperative palpation of pedal pulses and careful review of cross-sectional imaging are mandatory to identify such variants.
Exhaustive Indications and Contraindications
The decision to proceed with endoscopic resection of posterior ankle impingement relies on a meticulous synthesis of the patient's history, physical examination findings, and advanced imaging studies, coupled with a documented failure of comprehensive non-operative management.
Surgical intervention is explicitly indicated for patients who present with chronic, debilitating posterior ankle pain that is reproducibly exacerbated by forced plantarflexion and who have not experienced clinically significant relief following a minimum of three to six months of conservative therapy. This conservative regimen must have included strict activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy (focusing on eccentric strengthening, proprioception, and FHL gliding exercises), and potentially a fluoroscopically or ultrasound-guided diagnostic/therapeutic corticosteroid injection into the posterior impingement space.

Specific pathological indications encompass a symptomatic os trigonum, a fractured or hypertrophic Stieda process, chronic posterior capsulitis with hypertrophic synovitis, and recalcitrant FHL tenosynovitis that occurs in conjunction with bony impingement. Furthermore, the endoscopic approach is highly favorable for addressing concomitant pathologies such as posterior compartment loose bodies, posterior tibial plafond osteophytes, or localized osteochondral lesions of the posterior talar dome.
| Category | Specific Clinical Scenarios |
|---|---|
| Absolute Indications | Symptomatic os trigonum failing >3 months conservative care; Hypertrophic Stieda process causing mechanical block; Symptomatic non-union of a posterior talar process fracture; Concomitant FHL tenosynovitis requiring release. |
| Relative Indications | Professional athletes requiring expedited return to play (may shorten conservative trial); Posterior ankle loose bodies; Mild to moderate posterior tibiotalar osteoarthritis with impingement. |
| Absolute Contraindications | Active localized or systemic infection; Severe peripheral vascular disease; Uncorrected coagulopathy; Gross ankle instability requiring open reconstruction. |
| Relative Contraindications | Extensive prior open posterior ankle surgery (due to altered anatomy and dense scar tissue); Severe, end-stage tibiotalar or subtalar osteoarthritis; Distortion of the neurovascular bundle anatomy. |

Contraindications must be rigorously respected to prevent disastrous outcomes. Absolute contraindications include active localized soft tissue infection, active osteomyelitis, severe peripheral vascular disease that compromises wound healing, and uncorrected coagulopathies. Relative contraindications include a history of extensive open posterior ankle surgery, as dense cicatricial scar tissue can completely obliterate the normal anatomical planes, making endoscopic navigation exceedingly treacherous and significantly increasing the risk of neurovascular injury.
Pre-Operative Planning, Templating, and Patient Positioning
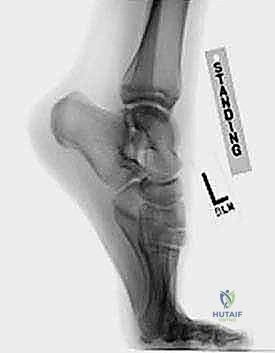
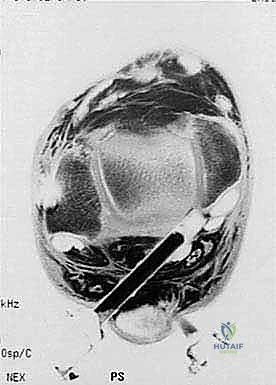
The foundation of a flawless endoscopic procedure is laid long before the initial incision is made. Comprehensive preoperative planning begins with an exhaustive review of all imaging modalities. Standard weight-bearing radiographs, including a true lateral view in maximum plantarflexion, are essential for visualizing the osseous impingement. However, Magnetic Resonance Imaging (MRI) is the gold standard and is absolutely mandatory for surgical planning. MRI allows for the precise evaluation of bone marrow edema within the os trigonum or posterior talus (confirming the osseous source of pain), the assessment of fluid within the FHL tendon sheath (indicating tenosynovitis), and the identification of any occult osteochondral lesions or anomalous soft tissue structures.

Computed Tomography (CT), particularly with 3D reconstructions, can be an invaluable adjunct when dealing with complex fracture patterns of the posterior process, large osteophytes, or when precise preoperative spatial templating of the osseous resection is required. The surgeon must mentally map the dimensions of the os trigonum and its relationship to the FHL sulcus based on these cross-sectional images.
Patient positioning is critical for optimal access and visualization. The procedure is universally performed with the patient in the prone position. General anesthesia or regional neuraxial anesthesia is utilized based on patient and anesthesiologist preference. A well-padded thigh tourniquet is applied to ensure a bloodless operative field. The patient is positioned such that the feet extend just past the edge of the operating table. This specific positioning is crucial as it allows the surgeon to freely and dynamically manipulate the ankle joint—specifically moving it through full ranges of plantarflexion and dorsiflexion—during the procedure to assess the adequacy of the resection and confirm the elimination of impingement.

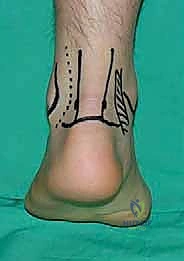
Meticulous surface anatomy marking is performed prior to exsanguination and tourniquet inflation. The medial and lateral borders of the Achilles tendon are outlined. The tips of the medial and lateral malleoli are marked. A horizontal line connecting the tip of the lateral malleolus to the Achilles tendon serves as the axis for portal placement. The posterolateral portal is marked just anterior to the lateral border of the Achilles tendon, at or slightly above the level of the lateral malleolus tip. The posteromedial portal is marked at the same horizontal level, just anterior to the medial border of the Achilles tendon.
Step-by-Step Surgical Approach and Resection Technique
The endoscopic resection of posterior ankle impingement is a masterclass in spatial awareness and precise soft tissue handling. We employ the classic two-portal hindfoot endoscopic technique originally popularized by C.N. van Dijk. The procedure utilizes a standard 4.0-mm, 30-degree arthroscope, though a 2.7-mm arthroscope may be used in smaller patients.
Establishing the Portals and Working Space
The procedure commences with the creation of the posterolateral portal. A vertical skin incision is made just anterior to the lateral border of the Achilles tendon. Subcutaneous tissues are bluntly spread with a small hemostat to avoid injury to the sural nerve, which courses distally and laterally in this vicinity. The arthroscope sheath with a blunt trocar is introduced through this portal, directed anteriorly toward the intermalleolar axis, aiming for the posterior aspect of the talus.
Next, the posteromedial portal is established. A similar vertical skin incision is made anterior to the medial border of the Achilles tendon. A mosquito hemostat is introduced and directed laterally to touch the arthroscope shaft, ensuring the instrument passes posterior to the neurovascular bundle. Once bone contact is made, the hemostat is slid down the shaft of the arthroscope to establish the working track. A 4.5-mm full-radius motorized shaver is then introduced through the posteromedial portal.

The initial endoscopic view is often obscured by the fatty tissue of Kager's triangle. The first critical step is the meticulous clearing of this "soft tissue triangle" to establish an adequate working space. Using the shaver with suction, the fatty tissue is carefully resected. The surgeon must maintain a clear orientation: the posterior talus is anterior, the subtalar joint is inferior, and the Achilles tendon is posterior.
Identifying the FHL: The Lifeline of the Posterior Ankle
As the working space is expanded medially, the most critical anatomical landmark must be identified: the Flexor Hallucis Longus (FHL) tendon. The FHL acts as the medial boundary of the safe zone; under absolutely no circumstances should resection occur medial to this tendon, as the tibial nerve and posterior tibial artery lie immediately adjacent to it. The FHL is identified by its characteristic location in the sulcus and its distinct muscle belly extending distally. To confirm its identity, the surgeon or an assistant dynamically flexes and extends the great toe, observing the corresponding excursion of the tendon within the endoscopic field.

Resection of the Os Trigonum and Impinging Structures
Once the FHL is safely identified and protected, attention is turned laterally to the impinging osseous structures. The posterior talofibular ligament (PTFL) and the posterior talocalcaneal ligament, which attach to the posterior surface of the os trigonum or Stieda process, are carefully released using a radiofrequency wand or a small arthroscopic elevator. This skeletonization is crucial for mobilizing the bone.
If an os trigonum is present, the synchondrosis connecting it to the talus is identified. An arthroscopic osteotome or a small periosteal elevator is introduced to lever the ossicle free. If the ossicle is large, it may need to be fragmented using a motorized burr or arthroscopic rongeurs before extraction through the portal. If the pathology is a hypertrophic Stieda process, a motorized burr is utilized to resect the overhanging bone until a smooth, contiguous contour is achieved between the posterior talus and the subtalar joint.

Throughout the resection, the surgeon must periodically perform dynamic testing. The ankle is forced into maximal plantarflexion while viewing endoscopically to ensure that all points of bony and soft tissue abutment between the tibia, talus, and calcaneus have been completely eradicated.
Addressing Concomitant Pathology
Following osseous resection, the FHL tendon must be thoroughly inspected. If tenosynovitis was identified preoperatively or visualized intraoperatively, an endoscopic FHL release is performed. The fibrous retinaculum overlying the FHL is carefully divided using a retrograde knife or arthroscopic scissors, and a thorough tenosynovectomy is performed utilizing a shaver. This ensures smooth gliding of the tendon and resolves the posteromedial pain component often associated with PAIS.

Once the resection is deemed complete and hemostasis is verified via temporary release of arthroscopic fluid pressure, the portals are closed with simple non-absorbable sutures, and a bulky, compressive sterile dressing is applied.
Complications, Incidence Rates, and Salvage Management
While endoscopic resection of posterior ankle impingement is highly successful and generally safe in experienced hands, it is not without significant risks. The deeply recessed anatomy and the proximity of critical neurovascular structures necessitate a profound respect for the potential complications.
Neurological injury is the most feared complication. The sural nerve is at risk during the establishment of the posterolateral portal. It can be injured by direct laceration, thermal damage from radiofrequency devices, or compression from aggressive retraction. The incidence of transient sural nerve neuropraxia ranges from 1% to 3%, while permanent injury is rare. The tibial nerve is at catastrophic risk if dissection strays medial to the FHL tendon. Tibial nerve injury can lead to debilitating plantar numbness, complex regional pain syndrome (CRPS), and intrinsic muscle paralysis.

Vascular injury to the posterior tibial artery or its branches can occur, particularly during aggressive debridement of the medial soft tissues. Minor venous bleeding is common and usually controlled with radiofrequency ablation or temporary elevation of fluid pressure. However, a major arterial laceration requires immediate conversion to an open posteromedial approach for vascular repair or ligation, depending on collateral flow.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Sural Nerve Injury | 1.0% - 3.0% | Blunt dissection through subcutaneous tissue; Avoid extreme lateral portal placement. | Observation for neuropraxia; Gabapentinoids; Rarely requires surgical neurolysis. |
| Tibial Nerve Injury | < 0.5% | Absolute adherence to the FHL as the medial boundary; No blind cutting medial to FHL. | Urgent open exploration and microsurgical repair if transected; Neuromodulation for CRPS. |
| Incomplete Resection | 2.0% - 4.0% | Dynamic intraoperative testing in full plantarflexion; Thorough preoperative CT templating. | Revision endoscopic or open resection if symptoms remain refractory. |
| FHL Tendon Rupture | < 0.5% | Avoid aggressive burring near the tendon; Judicious use of radiofrequency wands. | Open repair or tenodesis to FDL depending on the level and extent of the tear. |
| Portal Site Infection | 1.0% - 2.0% | Meticulous sterile technique; Proper portal closure without excessive tension. | Oral antibiotics for superficial infections; I&D for deep space infections. |

Incomplete resection of the os trigonum or Stieda process is a frustrating complication that leads to persistent impingement symptoms. This typically occurs when the surgeon fails to adequately visualize the most lateral or anterior extents of the ossicle, or fails to perform dynamic intraoperative testing. If conservative management fails postoperatively, a revision endoscopic or open procedure may be necessary.
Phased Post-Operative Rehabilitation Protocols
The success of an endoscopic posterior ankle procedure is heavily reliant on a structured, phased, and rigorously supervised postoperative rehabilitation protocol. The goals of rehabilitation are to protect the surgical site initially, restore full pain-free range of motion, and progressively return the athlete to their specific high-demand activities.
Phase 1: Protection and Edema Control (Days 1 to 14)
Immediately postoperatively, the patient is placed in a bulky compressive dressing and a posterior plaster splint or a rigid fracture boot with the ankle in a neutral position. Weight-bearing is typically restricted to touch-down or partial weight-bearing with crutches for the first 7 to 10 days to minimize swelling and protect the soft tissue healing. Strict elevation and cryotherapy are mandated. Early, gentle active and passive movement of the toes—specifically the hallux—is encouraged immediately to promote FHL gliding and prevent adherence within the fibro-osseous tunnel, especially if a tenosynovectomy was performed.
Phase 2: Restoration of Range of Motion (Weeks 2 to 4)
At the first postoperative visit (usually 10-14 days), sutures are removed, and the patient transitions to full weight-bearing in standard supportive footwear as tolerated. Formal physical therapy is initiated. The primary focus of Phase 2 is the aggressive restoration of ankle and subtalar range of motion. Active and active-assisted dorsiflexion and plantarflexion exercises are performed. Stationary cycling with low resistance is introduced. Manual therapy, including joint mobilizations and soft tissue massage around the portal sites, helps prevent restrictive scar tissue formation.

Phase 3: Strengthening and Proprioception (Weeks 4 to 8)
Once full, pain-free range of motion is achieved, the protocol shifts toward muscular strengthening and neuromuscular control. Progressive resistive exercises using elastic bands are utilized for the invertors, evertors, dorsiflexors, and plantarflexors. Eccentric loading of the Achilles and posterior tibial tendons is emphasized. Proprioceptive training begins with single-leg balance exercises on stable surfaces and progresses to unstable surfaces (BOSU ball, wobble board). Closed kinetic chain exercises, such as leg presses and controlled lunges, are integrated.

Phase 4: Return to Sport Specifics (Weeks 8+)
The final phase bridges the gap between clinical rehabilitation and full athletic participation. For ballet dancers, this involves a gradual, supervised return to demi-pointe and eventually en pointe work, ensuring that the posterior bony block has been completely eliminated and that the FHL can handle the immense loads. For soccer players, plyometrics, agility drills, and progressive kicking drills (starting with side-foot passes and progressing to full instep drives) are implemented. Clearance for full, unrestricted competition is typically granted between 8 and 12 weeks postoperatively, contingent upon the absence of pain, full strength, and the successful completion of sport-specific functional testing.

Summary of
Clinical & Radiographic Imaging Archive

