Masterclass: Limb-Sparing Resection of Popliteal Fossa Sarcomas

Key Takeaway
This masterclass guides orthopaedic fellows through limb-sparing popliteal fossa sarcoma resection. We cover meticulous preoperative planning, exact patient positioning, and comprehensive surgical anatomy focusing on neurovascular structures. Follow a granular, real-time intraoperative execution from incision to closure, emphasizing technique, instrument use, and critical decision-making. Learn pearls, pitfalls, and postoperative care for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a masterclass in a highly demanding, yet incredibly rewarding oncologic procedure: the limb-sparing resection of a soft tissue sarcoma (STS) localized within the popliteal fossa. This represents a rare and formidable pathology, accounting for less than 5% of all extremity soft tissue sarcomas. However, the popliteal fossa's dense anatomical topography makes performing a wide, oncologically sound margin resection notoriously difficult. The surgeon is constantly battling the dual imperatives of achieving an R0 (microscopically negative) resection margin while simultaneously preserving the critical periarticular neurovascular structures that dictate distal limb viability and function.
The histological landscape of popliteal sarcomas is diverse, frequently encompassing synovial sarcomas, undifferentiated pleomorphic sarcomas (UPS), myxoid liposarcomas, and malignant peripheral nerve sheath tumors (MPNSTs). Unlike carcinomas, which primarily spread via the lymphatic system, these mesenchymal malignancies demonstrate a predilection for aggressive local expansion along longitudinal fascial planes and hematogenous metastasis, predominantly to the pulmonary parenchyma. The biological behavior of these tumors necessitates a profound understanding of compartmental anatomy. In the popliteal fossa, true anatomical compartments are ill-defined, and the loose areolar tissue permits rapid, unhindered multidirectional tumor growth, frequently leading to early abutment or encasement of the popliteal vessels and the sciatic nerve bifurcations.
Historically, the standard of care for a high-grade sarcoma in this location was an above-knee amputation, given the prohibitive morbidity associated with local recurrence and the technical limitations of complex vascular reconstruction. However, modern orthopedic oncology has undergone a radical paradigm shift. The advent of sophisticated neoadjuvant therapies—specifically conformal radiotherapy and, in selected histologies, systemic chemotherapy—has fundamentally altered our surgical approach. These modalities induce tumor necrosis, generate a dense pseudocapsule, and sterilize microscopic peripheral disease, thereby enabling limb-salvage surgery in over 90% of extremity sarcoma cases. Yet, the popliteal fossa remains one of the final frontiers where the decision between limb salvage and amputation demands excruciatingly careful patient selection.
We must also acknowledge the "popliteal paradox." Tumors in this region are frequently subjected to delayed diagnosis because their initial clinical presentation—a vague, painless posterior knee fullness—is routinely misattributed to ubiquitous, benign pathologies such as Baker's cysts, popliteal artery aneurysms, or deep vein thromboses. This delay allows the sarcoma to achieve substantial volume, further complicating the eventual surgical extirpation. Therefore, our goal today transcends mere tumor removal; it is an exercise in precise anatomical dissection, strategic vascular management, and comprehensive functional reconstruction, demanding the highest echelon of surgical acumen.
Detailed Surgical Anatomy and Biomechanics
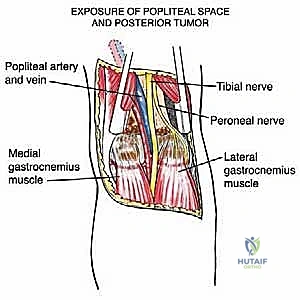
Before we make any incisions, let us meticulously refresh our understanding of this critical anatomical diamond. The popliteal space is a complex, diamond-shaped region at the posterior aspect of the knee, acting as the primary conduit for neurovascular structures transitioning from the thigh to the leg. Mastery of this 3D topography is the absolute prerequisite for safe oncologic resection.
The boundaries of the popliteal fossa are formed by the dynamic muscular tendinous units of the knee. Medially, the superior boundary is dictated by the robust bellies and tendons of the semimembranosus and semitendinosus muscles. Laterally, the superior boundary is formed by the biceps femoris muscle, beneath which the common peroneal nerve takes its perilous course. The inferior apex is constructed by the medial and lateral heads of the gastrocnemius muscle as they converge to form the sural triceps. The floor of the fossa is rigid, consisting of the posterior popliteal surface of the distal femur, the dense posterior capsule of the knee joint (reinforced by the oblique popliteal ligament), and the popliteus muscle overlying the proximal tibia.
The roof of this space is formed by the popliteal fascia, a continuation of the fascia lata. This fascial layer is deceptively thin and lies in terrifyingly intimate proximity to the superficial neurovascular bundle, particularly the common peroneal nerve and the short saphenous vein. When raising posterior skin flaps, an inexperienced surgeon can easily breach this fascia and inadvertently transect these structures. The popliteal artery is the deepest structure within the fossa, entering through the adductor hiatus and lying directly apposed to the posterior knee capsule. As it traverses obliquely, it provides vital collateral circulation via the superior, middle, and inferior genicular arteries. The inferior genicular vessels are of paramount surgical importance; they firmly tether the popliteal artery to the joint capsule and must be systematically identified and ligated to allow for adequate mobilization of the primary vessel away from a deep-seated tumor.
Superficial to the artery lies the popliteal vein, which receives the short saphenous vein piercing the popliteal fascia. While the popliteal vein can occasionally be sacrificed if oncologically necessary—relying on the greater saphenous vein for collateral drainage—simultaneous damage to the ipsilateral greater saphenous system will precipitate catastrophic venous hypertension and limb loss. The nervous architecture is equally critical. The tibial nerve enters lateral to the artery, crosses superficially to its medial aspect, and dives between the gastrocnemius heads. The common peroneal nerve slopes down the superolateral border along the biceps femoris tendon, wrapping around the fibular neck where it is highly susceptible to traction injury or inadvertent transection during the distal lateral exposure.
Exhaustive Indications and Contraindications
The decision to proceed with a limb-sparing resection in the popliteal fossa is never made in isolation; it is the culmination of rigorous multidisciplinary tumor board deliberation. The primary indication is a biopsy-proven, localized soft tissue sarcoma where preoperative imaging confirms that an R0 resection margin can be achieved without rendering the distal limb ischemic or functionally useless. The patient must have adequate physiological reserve to tolerate a potentially prolonged procedure that may include complex microvascular reconstruction and local muscle flap transfers. Furthermore, the patient must be committed to an arduous, months-long postoperative rehabilitation protocol.
Contraindications, conversely, are strict and must be respected to prevent devastating outcomes. Absolute contraindications include the circumferential encasement of the major neurovascular bundle (popliteal artery, vein, and tibial nerve) over a substantial length, where en bloc resection would require massive, multi-structure reconstruction that is technically unfeasible or carries an unacceptably high risk of failure. Extensive tumor fungation through the skin, uncontrollable deep infection within the tumor bed, or massive intra-articular extension necessitating an extra-articular total knee resection often tip the scales toward amputation, as the functional outcome of a salvaged but insensate, paralyzed, and stiff limb is vastly inferior to a well-fitted modern prosthesis.
Relative contraindications require nuanced clinical judgment. These include advanced patient age, severe peripheral vascular disease, profound diabetic neuropathy, or significant cardiopulmonary comorbidities that preclude lengthy anesthesia. In such scenarios, the physiological toll of a 6-to-8 hour limb-salvage operation, coupled with the high metabolic demand of wound healing and flap integration, may exceed the patient's capacity. Additionally, if the expected functional outcome following the necessary resection of major motor nerves (e.g., the entire tibial nerve) results in an insensate plantar surface and a flail foot, primary amputation must be strongly considered and discussed explicitly with the patient.
Indications and Contraindications Matrix
| Category | Limb-Sparing Resection | Primary Amputation |
|---|---|---|
| Oncologic Status | Localized disease; R0 margin achievable. | Massive local recurrence; impossible R0 margin. |
| Neurovascular | Displacement/abutment of vessels; reconstructable. | Circumferential encasement of artery/vein AND nerve. |
| Joint Involvement | Extra-capsular or minimal capsular adherence. | Massive intra-articular extension. |
| Functional Expectation | Sensate plantar foot; stable knee; functional motor units. | Insensate foot; flail extremity; severe chronic pain. |
| Patient Physiology | Medically fit for prolonged surgery and rehab. | Severe comorbidities; inability to tolerate long anesthesia. |
Pre-Operative Planning, Templating, and Patient Positioning
Our success today hinges entirely on meticulous, obsessive preoperative planning. Leaving anything to chance in the popliteal fossa is a recipe for surgical disaster. The cornerstone of our planning is advanced, multi-modal imaging. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the absolute gold standard. We must critically evaluate the axial, coronal, and sagittal sequences to define the tumor's volume, its precise relationship to the neurovascular bundle, and the integrity of the posterior knee joint capsule.
Fellows, observe this MRI. This is a typical popliteal sarcoma, distinct from a Baker's cyst. Notice the heterogeneous signal intensity and lack of a simple fluid-filled cystic structure.
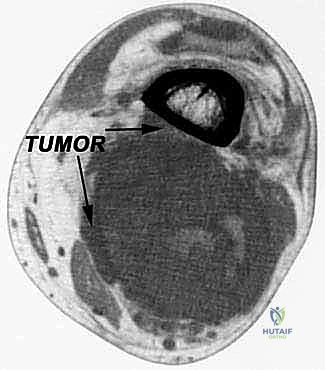
Here, in the axial plane, you can appreciate the large, solid soft tissue mass displacing the medial head of the gastrocnemius.
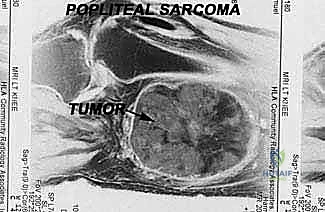
And this sagittal view clearly shows its relationship to the adjacent femur and knee joint capsule. Crucially, the capsule appears pushed but not frankly invaded, suggesting an extra-articular resection is viable.
Beyond MRI, Computed Tomography (CT) of the chest is mandatory for pulmonary staging, and a CT of the extremity is highly useful if there is any suspicion of cortical bone erosion. Furthermore, we routinely perform preoperative angiography or CT angiography. This is not merely an academic exercise; it is a vital roadmap.
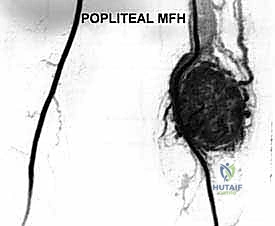
This angiogram reveals an extremely vascular sarcoma with significant neovascularization. This mapping guides potential preoperative embolization to mitigate intraoperative hemorrhage and alerts us to aberrant vascular anatomy.
Patient positioning and preparation demand equal rigor. The patient is placed in the prone position on a radiolucent operative table, ensuring all bony prominences are meticulously padded to prevent pressure neuropraxias.

As you can see here, the prone position allows optimal, gravity-assisted exposure of the posterior aspect of the knee and thigh. A high-thigh pneumatic tourniquet is applied but left uninflated; we rely on precise hemostasis, reserving the tourniquet only for catastrophic vascular injury.
Critically, both lower limbs are prepped and draped sterilely. The contralateral leg is our designated donor site for a reversed greater saphenous vein graft. If intraoperative findings dictate the en bloc resection of the popliteal artery or vein to achieve negative margins, we must have immediate access to autologous conduit without breaking scrub or repositioning the patient.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, the planning phase is complete. Gloves on, instruments ready. We proceed with the extirpation. Our primary goal with the incision is to achieve wide, extensile exposure while vigorously protecting the superficial venous and nervous structures.
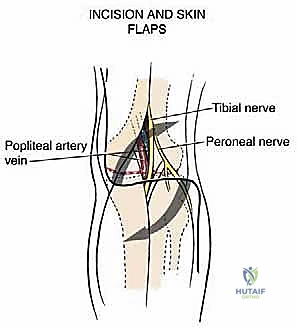
We utilize a classic, lazy S-shaped incision. The proximal limb begins medially over the distal third of the thigh, crosses the popliteal crease obliquely, and extends distally along the lateral aspect of the proximal calf.
Observe the planned incision line. The medial-proximal arm allows early identification of the popliteal vessels exiting the adductor hiatus. The lateral-distal arm provides exposure of the common peroneal nerve and avoids the medially located greater saphenous vein, our vital venous collateral.
Once the skin is incised, we raise thick subfascial flaps. I cannot stress this enough: the popliteal fascia is exceedingly thin. You must dissect with extreme caution. We begin by identifying the neurovascular structures in normal, unviolated tissue planes proximal and distal to the tumor mass. Proximally, we locate the sciatic nerve as it emerges from beneath the long head of the biceps femoris.
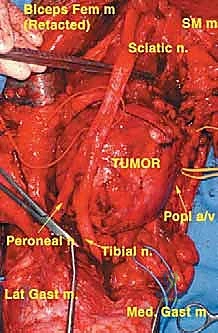
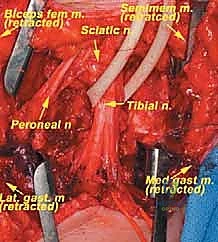
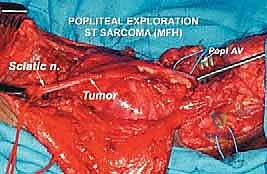
Here, you can clearly see the sciatic nerve and its bifurcation into the tibial and common peroneal nerves, cleanly identified, encircled with vessel loops, and secured away from the tumor bed.
We systematically trace these nerves distally. The common peroneal nerve is mobilized laterally, and the tibial nerve is tracked as it dives between the gastrocnemius heads.
Following neural isolation, we address the vascular bundle. The popliteal artery and vein are identified at the adductor hiatus. Using delicate, blunt dissection and right-angle clamps, we mobilize the vessels. This requires the systematic identification, clipping, and division of multiple genicular branches that tether the vessels to the tumor capsule.
Notice the meticulous skeletonization of the popliteal vessels. We use silastic loops for gentle traction. If the tumor is intimately adherent to the adventitia, we do not hesitate to resect the involved vascular segment en bloc to ensure oncologic safety.
Deep dissection continues. We are now elevating the tumor off the posterior capsule of the knee. If the preoperative MRI or intraoperative tactile feedback suggests capsular invasion, the posterior capsule is taken en bloc with the specimen, exposing the femoral condyles.
With the neurovascular structures safely retracted, the tumor is resected en bloc with a cuff of normal surrounding muscle (typically portions of the gastrocnemius or hamstrings).
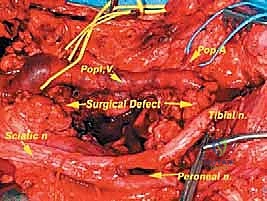
The extirpation is complete. Observe the massive, clean tumor bed. The neurovascular bundle is intact but completely skeletonized. The posterior knee capsule has been partially resected, revealing the articular cartilage.
This is the resected specimen. It is immediately oriented with sutures for the pathologist to ensure accurate margin assessment. A true R0 resection is the ultimate determinant of patient survival.
Reconstruction is the final, critical phase. If vascular bypass was required, our vascular surgery colleagues perform the saphenous vein interposition grafts. Following this, we must ensure robust soft tissue coverage over the exposed vessels and nerves to prevent desiccation and catastrophic blowout, especially in the setting of prior neoadjuvant radiation.

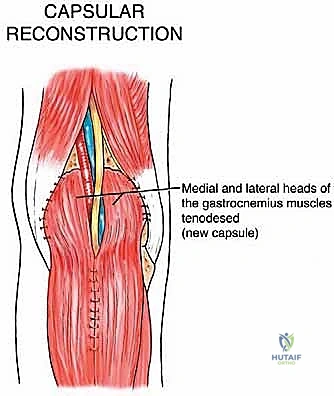
Here, we are utilizing a medial gastrocnemius rotational flap. The muscle belly is mobilized and rotated to obliterate the dead space and provide vascularized coverage over the critical structures and the exposed knee joint.
The deep fascial layers are meticulously closed over closed-suction drains. The skin is approximated without tension. If tension is present, split-thickness skin grafting over the muscle flap is mandatory.

The final postoperative result. The limb is viable, the incisions are clean, and the patient is placed in a well-padded posterior splint in slight flexion to remove tension from the posterior wound and any vascular anastomoses.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, limb-sparing resections in the popliteal fossa carry a formidable complication profile. The dense anatomy, combined with the tissue-depleting effects of neoadjuvant radiotherapy, creates a hostile environment for wound healing. The most immediate and life-threatening complications are vascular. Arterial thrombosis or anastomotic rupture can occur in up to 5-10% of cases requiring vascular reconstruction. Immediate signs include loss of distal pulses, pallor, and a rapidly expanding popliteal hematoma. Management requires emergent return to the operating theater for thrombectomy, revision of the anastomosis, or potentially an extra-anatomic bypass.
Neurological deficits are unfortunately common, ranging from transient neuropraxia due to traction, to permanent neurotmesis. The common peroneal nerve is uniquely vulnerable; injury results in a devastating foot drop. While neuropraxic injuries may recover over 6 to 12 months, complete transections require prompt microsurgical repair or nerve grafting. If recovery fails, salvage management involves a posterior tibial tendon transfer to the dorsum of the foot to restore active dorsiflexion, coupled with an Ankle-Foot Orthosis (AFO).
Wound complications—including seroma, hematoma, wound dehiscence, and deep surgical site infections—are the most frequent morbidities, occurring in 20-35% of irradiated patients. The popliteal fossa creates a massive dead space post-resection. Meticulous hemostasis, prolonged use of closed-suction drains, and prophylactic muscle flaps (like the gastrocnemius flap) are critical preventative measures. If deep infection occurs, aggressive serial debridements and targeted intravenous antibiotics are required. Ultimately, if the neurovascular bundle becomes hopelessly infected or if there is a massive, unresectable local oncologic recurrence, secondary above-knee amputation remains the definitive salvage procedure to save the patient's life.
Complication Profile and Management Strategy
| Complication | Estimated Incidence | Immediate/Salvage Management |
|---|---|---|
| Wound Dehiscence / Necrosis | 20% - 35% (higher with XRT) | VAC therapy, serial debridement, secondary flap coverage (e.g., ALT free flap). |
| Neuropraxia (Peroneal/Tibial) | 10% - 15% | Observation, EMG at 6 weeks, physical therapy, AFO for foot drop. |
| Vascular Graft Thrombosis | 5% - 10% | Emergent return to OR, thrombectomy, revision of bypass graft. |
| Deep Surgical Site Infection | 5% - 12% | Aggressive I&D, retention of hardware/grafts if possible, long-term IV antibiotics. |
| Local Oncologic Recurrence | 5% - 10% (at 5 years) | Re-staging, possible re-resection if feasible; highly likely to require amputation. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a popliteal sarcoma resection is a marathon, not a sprint. The protocol must be heavily customized based on the extent of muscular resection, the presence of vascular grafts, and the neurological status of the limb. Phase I (Weeks 0-2) is entirely focused on wound healing and the protection of surgical repairs. The limb is immobilized in a hinged knee brace locked in 10 to 15 degrees of flexion. This slight flexion is critical; it eliminates tension on the posterior skin flaps, the sciatic nerve, and any delicate vascular anastomoses
