Physeal Bar Resection: A Masterclass in Growth Plate Salvage and Deformity Correction
Key Takeaway
Join us in the OR for a masterclass on physeal bar resection. We'll meticulously dissect the anatomy, detail preoperative planning, and guide you through every intraoperative micro-step. Learn precise techniques for bar removal, interposition material placement, and immediate post-op care. Understand critical pearls, pitfalls, and strategies for optimal pediatric growth plate salvage and deformity correction.
Welcome, fellows, to the operating theater. Today, we are tackling a fascinating and critical pediatric orthopedic challenge: the excision of a physeal bar. This procedure, while seemingly straightforward in its conceptual goal, demands meticulous preoperative planning, precise intraoperative execution, and a profound, nuanced understanding of growth plate physiology. Our ultimate objective is to salvage the remaining growth potential of the affected bone and to correct, or entirely prevent, the progressive, debilitating deformities that characterize this pathology in our young, skeletally immature patients.
Comprehensive Introduction and Patho-Epidemiology
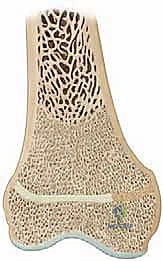
Before we even consider touching a scalpel, we must revisit the fundamental cellular biology and structural mechanics of the physis. The physis, or epiphyseal growth plate, is a highly specialized, dynamic cartilaginous structure solely responsible for the longitudinal growth of long bones. It is not merely a layer of cartilage; it is a meticulously organized, metabolically demanding tissue composed of four distinct, sequential cell layers, each with a highly specific physiologic mandate.
The first layer is the Resting Zone, located most proximally to the epiphysis. This layer acts as a critical reserve of chondrocytes and synthesizes the matrix components necessary for the subsequent layers. Immediately adjacent is the Proliferative Zone, where chondrocytes undergo rapid mitosis, increasing exponentially in number and arranging themselves into characteristic longitudinal columns. Following this is the Hypertrophic Zone, where chondrocytes cease dividing and instead enlarge significantly, accumulating lipids, glycogen, and alkaline phosphatase. This specific region is where the vast majority of true longitudinal growth physically occurs. Finally, the Enchondral Ossification Zone is the most distal layer, where hypertrophic chondrocytes undergo programmed cell death (apoptosis), and the remaining calcified cartilage matrix is invaded by metaphyseal blood vessels and osteoblasts, culminating in the deposition of new trabecular bone.
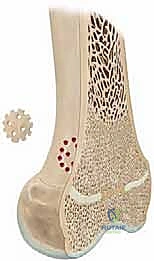
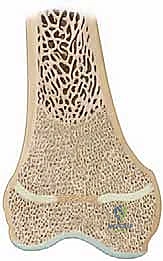
A physeal bar, technically defined as a partial premature physeal arrest, is an aberrant, pathological osseous bridge that forms across this delicate cartilaginous barrier. This bone bridge physically connects the epiphyseal trabecular bone directly to the metaphyseal trabecular bone. This bony tether acts as an unyielding mechanical restraint, restricting normal longitudinal growth in the affected focal area while the surrounding, healthy physis continues to expand. This differential growth leads to predictable, progressive, and often severe clinical consequences, primarily angular deformity and limb-length discrepancy.
The pathogenesis of these bars is classically rooted in a breach of the cartilage barrier. The most ubiquitous culprit is trauma, specifically pediatric physeal fractures categorized under the Salter-Harris classification system (particularly types III, IV, and severe compression type V injuries). When a fracture line vertically traverses the germinal cell layers or catastrophically disrupts the overall physeal integrity, the healing process allows metaphyseal and epiphyseal bone to unite directly across the defect. Beyond trauma, severe infections such as osteomyelitis or septic arthritis can enzymatically destroy the physis. Less commonly, localized cell death due to profound ischemia, iatrogenic thermal injury, or prolonged rigid hardware placement across the physis can precipitate bar formation.
Consider the biomechanical and anatomical differences between the distal femoral physis and the distal radial physis. Distal radial physeal fractures are exceedingly common in pediatric orthopedics, yet subsequent physeal bar formation remains relatively rare. Conversely, distal femoral physeal fractures are far less common, but the inherent risk of bar formation post-injury is exponentially higher. This discrepancy is largely due to the complex, three-dimensional biconcave configuration of the distal femoral physis. This intricate geometry requires a massive transfer of kinetic energy to fracture, and when it does fail, the likelihood of severe comminution and violation of the protective cartilage barrier is vastly increased, thereby setting the stage for aggressive physeal bar formation.
Detailed Surgical Anatomy and Biomechanics
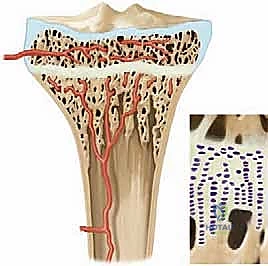
To successfully resect a physeal bar, the operating surgeon must possess an intimate understanding of the vascular anatomy supplying the physis. The physis acts not only as a physical barrier separating the trabecular bone of the epiphysis from the metaphysis, but also as a strict, impermeable barrier to blood flow. It strictly separates the epiphyseal blood supply from the metaphyseal blood supply. This dual vascularity is critical to understand because it dictates the survival of the growth plate following injury or surgical intervention.

The epiphyseal arteries are the lifeblood of the physis. They supply the resting and proliferative zones—the germinal layers where growth originates. If the epiphyseal blood supply is compromised by trauma or aggressive surgical dissection, the germinal cells undergo ischemic necrosis, permanently halting growth and virtually guaranteeing bar formation regardless of any resection attempts. Conversely, the metaphyseal vessels only supply the zone of enchondral ossification. While disruption here may temporarily delay the ossification process, it does not kill the germinal chondrocytes, and the physis can often recover. Therefore, our surgical approach must meticulously preserve the epiphyseal vascular ring at all costs.
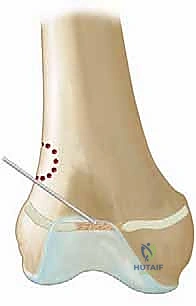
Biomechanically, the location of the physeal bar dictates the specific type of deformity the patient will develop. A peripheral bar acts as an asymmetric tether. As the central and contralateral portions of the physis continue their normal longitudinal expansion, the tethered periphery cannot yield, resulting in a progressive angular deformity. For example, a lateral bar in the distal femur will inevitably lead to progressive genu valgum. In contrast, a purely central bar acts as a global tether. The peripheral physis attempts to grow, but is held back centrally, leading to a "tenting" or "cupping" of the metaphysis into the epiphysis. While central bars may not cause immediate angular deformity, they cause a profound and rapid global growth arrest, leading to severe limb-length discrepancies.
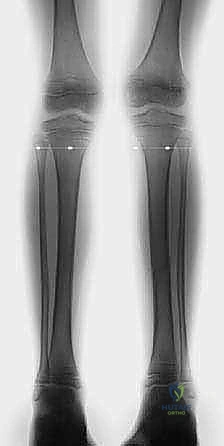
Furthermore, in two-bone segments such as the forearm (radius and ulna) or the lower leg (tibia and fibula), a physeal bar affecting only one bone introduces complex biomechanical challenges. If the distal tibial physis arrests due to a bar, but the distal fibula continues to grow, the fibula will progressively migrate distally, leading to a severe varus deformity of the ankle joint, altered joint contact mechanics, and early-onset degenerative joint disease. Recognizing these biomechanical realities is essential for determining the timing and necessity of surgical intervention.
Exhaustive Indications and Contraindications
The decision to proceed with a physeal bar resection is highly nuanced and depends on a delicate calculus involving the patient's chronological age, skeletal age, the specific anatomical location of the bar, and the precise size of the osseous bridge. Not every physeal bar is a surgical candidate, and inappropriate patient selection will lead to surgical failure and unnecessary morbidity.
The primary indication for physeal bar resection is the presence of a documented, enlarging osseous bar in a skeletally immature patient who possesses significant remaining growth potential. The classical teaching, which remains the gold standard, dictates that the patient should have at least two years of anticipated growth remaining, or the potential to achieve at least two centimeters of longitudinal growth from the affected physis. If the patient is nearing skeletal maturity, the morbidity of the procedure outweighs the negligible growth that might be salvaged, and alternative procedures like contralateral epiphysiodesis or acute osteotomy are preferred.
Another critical prognostic indicator is the cross-sectional area of the physeal bar relative to the total area of the physis. Extensive clinical studies and historical data pioneered by Langenskiöld demonstrate that resection is most successful when the bar occupies less than 50% of the total cross-sectional area of the physis. Bars exceeding this 50% threshold have caused such extensive, irreversible damage to the surrounding germinal cell layers that even a technically perfect resection rarely results in meaningful resumption of longitudinal growth. However, exceptions exist; in very young patients (e.g., a 4-year-old) with a massive 60% bar, resection might still be attempted as a salvage procedure, as even a partial restoration of growth over a decade can significantly reduce the final limb-length discrepancy.
| Parameter | Favorable Indications for Resection | Absolute/Relative Contraindications |
|---|---|---|
| Remaining Growth | > 2 years or > 2 cm anticipated growth | < 1 year or < 1 cm anticipated growth |
| Bar Size (Area) | < 50% of total physeal cross-section | > 50% of total physeal cross-section (Relative) |
| Skeletal Age | Skeletally immature (e.g., Girls < 12, Boys < 14) | Approaching skeletal maturity |
| Infection Status | No active infection | Active osteomyelitis or septic joint |
| Physeal Integrity | Healthy surrounding cartilage visible on MRI | Global ischemic necrosis of the entire physis |
| Deformity | Mild to moderate, correctable with resumed growth | Severe rigid deformity requiring acute osteotomy |
It is also crucial to acknowledge that physeal bar resection is primarily a procedure to restore longitudinal growth and prevent further angular deformity. While some spontaneous correction of existing angular deformity can occur through resumed asymmetric growth (the Hueter-Volkmann principle), it is highly unpredictable. Therefore, if a severe angular deformity (>15-20 degrees) is already present at the time of diagnosis, bar resection alone will likely be insufficient, and a concomitant or staged corrective osteotomy must be factored into the comprehensive treatment plan.
Pre-Operative Planning, Templating, and Patient Positioning
Our journey begins long before the patient enters the operating room. A thorough, exhaustive preoperative evaluation is paramount, relying heavily on advanced imaging modalities to create a precise surgical blueprint. Standard radiographs, while useful for initial screening, are grossly inadequate for planning a bar resection.
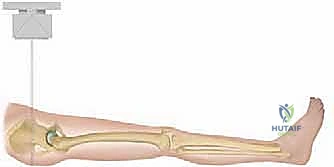
We begin with long-length standing radiographs, specifically true scanograms or teleoroentgenograms, to accurately quantify the existing limb-length discrepancy and measure any coronal or sagittal plane angular deformities. A true scanogram utilizes a slit beam of radiation that moves down the length of the extremity, completely eliminating radiographic magnification and allowing for precise, direct measurements. We also obtain a radiograph of the left hand and wrist to accurately determine the patient's skeletal age using the Greulich and Pyle atlas, which is far more reliable than chronological age for predicting remaining growth.
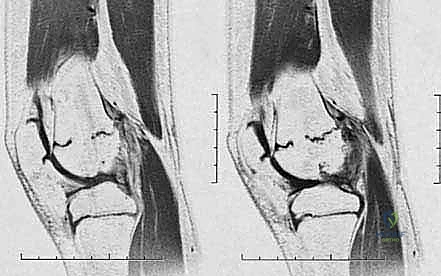
Once the presence of a bar is confirmed, fine-cut Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) is absolutely essential. Modern protocols favor MRI as it avoids ionizing radiation and provides superior visualization of the non-ossified cartilaginous physis. We obtain axial, coronal, and sagittal plane images with slice thicknesses of 1 to 2 millimeters. These images are utilized to perform "bar mapping." We meticulously trace the outline of the bony bar across multiple axial slices, calculating its precise cross-sectional area and its exact geographic location (anterior, posterior, medial, lateral, central, or peripheral).

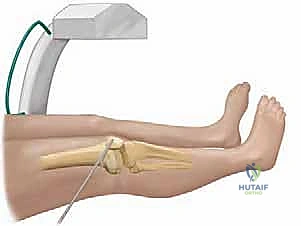
This 3D map is our definitive surgical guide. It dictates our surgical approach. Peripheral bars are accessed via a direct cortical approach, removing the overlying bone to expose the bar. Central bars, surrounded by a ring of healthy physis, require a metaphyseal window approach, tunneling down through the metaphysis to reach the bar from the "inside out" without violating the healthy peripheral cartilage. Patient positioning is dictated by this map. For a distal femoral central bar, the patient is positioned supine on a radiolucent table. A sterile tourniquet is applied high on the thigh. Fluoroscopy must be available and positioned to allow for orthogonal views (AP and lateral) without compromising the sterile field. We ensure the limb is draped free to allow for full range of motion, which aids in fluoroscopic visualization and intraoperative assessment.
Step-by-Step Surgical Approach and Fixation Technique
The surgical technique for physeal bar resection requires the precision of a jeweler and the anatomical respect of a neurosurgeon. We will detail the approach for a central physeal bar utilizing a metaphyseal window, as this represents the most technically demanding scenario.
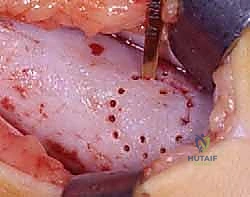
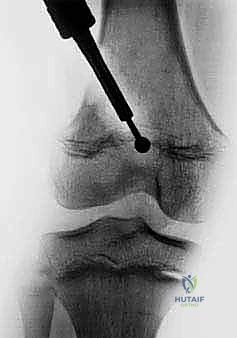
Following standard exsanguination and tourniquet inflation, a longitudinal incision is made over the metaphysis, carefully avoiding the perichondrial ring of LaCroix and the groove of Ranvier, which house the vital peripheral germinal cells. The periosteum is incised and gently elevated. Using fluoroscopic guidance, a rectangular metaphyseal cortical window is marked out, typically 1.5 to 2 centimeters proximal to the physis. This window is carefully created using a high-speed burr or fine osteotomes. The cortical bone flap is preserved in a moist sponge for later replacement.
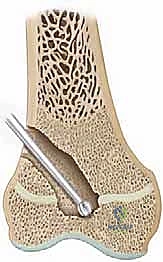
Once inside the metaphyseal cancellous bone, we utilize curettes and a high-speed motorized burr to excavate a tunnel directly toward the mapped location of the central bar. Frequent fluoroscopic checks in both AP and lateral planes are mandatory to ensure the trajectory is accurate and to prevent inadvertent plunging through the epiphysis into the joint space. As we approach the bar, the consistency of the bone changes; the bar itself is typically dense, sclerotic bone, contrasting sharply with the softer surrounding metaphyseal cancellous bone.

The resection of the bar must be absolute. We use angled curettes and the burr to meticulously remove all sclerotic bone until we visualize normal, healthy, translucent bluish-white physeal cartilage on all sides of the cavity. Visualization is the most challenging aspect of this procedure. We frequently employ small dental mirrors or a 30-degree, 2.7mm arthroscope inserted into the metaphyseal cavity to look "down" onto the epiphyseal side of the resection. Any residual bone left bridging the gap will act as a nidus for immediate bar recurrence. The resection cavity is then thoroughly irrigated with pulsatile lavage to remove all microscopic bone debris, which could also induce ectopic ossification.
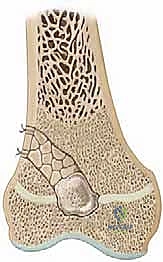
Once the resection is complete and confirmed visually and fluoroscopically, the resulting dead space must be filled with an interpositional material to physically block hematoma formation and subsequent bone regeneration. Autologous fat is the gold standard. We typically harvest a generous graft of subcutaneous fat from a separate small incision in the gluteal fold or from the edge of the primary incision. The fat graft must be handled atraumatically. It is packed tightly into the defect, ensuring it completely covers the exposed epiphyseal and metaphyseal bone surfaces.
Crucially, before final packing, we place a small, sterile radiopaque marker—such as a titanium hemoclip or a piece of stainless steel wire—directly at the epiphyseal base of the fat graft. This marker is vital for postoperative monitoring; as the physis resumes growth, the metaphysis will grow away from the epiphysis, and the distance between this marker and the metaphyseal window will visibly increase on serial radiographs, confirming successful growth restoration. Finally, the metaphyseal cortical window is replaced, and the periosteum and soft tissues are meticulously closed in layers.

Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and flawless execution, physeal bar resection carries a significant risk profile. The most devastating complication is the recurrence of the physeal bar, which historically occurs in 15% to 30% of cases, depending on the initial size of the bar and the specific etiology. Recurrence is almost always due to incomplete initial resection, failure of the interpositional material to adequately fill the dead space, or the presence of microscopic bone dust left in the cavity.

Another notable complication is the failure to correct existing angular deformity. As previously stated, the primary goal of resection is to restore longitudinal growth; spontaneous correction of severe angular deformity is unreliable. If a patient presents with a 20-degree valgus deformity, bar resection alone will likely leave them with residual valgus, even if longitudinal growth resumes perfectly. In these instances, a salvage or secondary procedure, such as a corrective closing or opening wedge osteotomy, or guided growth (hemiepiphysiodesis) on the contralateral side of the physis, must be employed.
Iatrogenic injury to the healthy remaining physis during the surgical approach or resection is a critical error. Aggressive burring or poor visualization can easily destroy the adjacent normal germinal cells, effectively expanding the size of the bar and worsening the prognosis. Furthermore, aggressive excavation of the epiphysis can lead to joint penetration, resulting in septic arthritis, hemarthrosis, or premature degenerative joint disease.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Bar Recurrence | 15% - 30% | Meticulous mapping, complete resection, arthroscopic visualization, tight fat packing. | Repeat resection (if indications still met), complete epiphysiodesis + limb lengthening. |
| Residual Angular Deformity | 40% - 60% | Preoperative counseling, realistic expectations. | Concomitant or staged corrective osteotomy, guided growth (8-plates). |
| Iatrogenic Physeal Injury | 5% - 10% | Use of fine burrs, avoiding the perichondrial ring, continuous fluoroscopy. | Contralateral epiphysiodesis to balance growth, limb lengthening. |
| Joint Penetration | < 5% | Careful depth control with burr, orthogonal fluoroscopy, avoiding excessive epiphyseal excavation. | Immediate joint irrigation, repair of articular cartilage if possible, close monitoring. |
| Infection (Deep) | 1% - 2% | Strict sterile technique, prophylactic antibiotics, meticulous hemostasis. | Aggressive surgical debridement, removal of fat graft, targeted IV antibiotics. |
When a resection fails and the bar recurs, the salvage options depend heavily on the patient's remaining growth. If significant growth remains, a repeat resection can be attempted, though success rates plummet on revision surgery. More commonly, if the patient is older or the recurrence is massive, the salvage pathway shifts towards complete surgical epiphysiodesis of the affected growth plate to halt the progressive angular deformity, combined with an epiphysiodesis of the contralateral limb to manage the final limb-length discrepancy, or a formal limb lengthening procedure (e.g., using an Ilizarov or Taylor Spatial Frame) if the discrepancy is projected to be severe.
Phased Post-Operative Rehabilitation Protocols
The immediate postoperative phase is focused on protecting the surgical site, managing pain, and preventing joint stiffness. Upon completion of the procedure, a bulky, soft sterile dressing is applied. Depending on the extent of the metaphyseal window and the inherent stability of the bone, a posterior splint or a hinged knee brace (for distal femoral or proximal tibial procedures) may be utilized for 1 to 2 weeks to provide soft tissue rest.
Weight-bearing status is carefully titrated. For isolated bar resections without concomitant osteotomies, patients are typically made non-weight-bearing or toe-touch weight-bearing on crutches for the first 3 to 4 weeks. This protects the metaphyseal cortical window from stress fractures while it incorporates and heals. Early, gentle active and active-assisted range of motion exercises for the adjacent joints are initiated within the first week to prevent arthrofibrosis, particularly in the knee following distal femoral procedures.
The critical phase of postoperative monitoring begins at the 3-month mark. Standard AP and lateral radiographs are obtained to assess the position of the radiopaque marker placed during surgery. We are looking for the "Harris growth arrest line"—a transverse line of sclerotic bone that forms parallel to the physis at the time of surgery due to the temporary cessation of growth. If the surgery is successful, subsequent radiographs at 6 and 12 months will show the physis (and the radiopaque marker) migrating away from this arrest line and the metaphyseal window, providing undeniable, objective evidence of resumed longitudinal growth.

Patients must be followed longitudinally with serial clinical examinations and scanograms every 6 months until they reach complete skeletal maturity. This long-term vigilance is mandatory because a physeal bar can recur silently months or even years after a seemingly successful initial resection. The rehabilitation protocol is not merely about immediate physical therapy; it is a commitment to a multi-year radiographic and clinical surveillance program to ensure the ultimate goal of skeletal symmetry is achieved.
Summary of Landmark Literature and Clinical Guidelines
The foundational principles of physeal bar resection we employ today are deeply rooted in the pioneering work of several orthopedic giants. The modern era of this procedure was arguably ushered in by Langenskiöld in the 1960s and 1970s. His seminal animal studies and subsequent clinical series definitively established that a bony bridge across the physis could be surgically excised and the resulting cavity filled with an interpositional material (he initially utilized autologous fat) to
