Masterclass: Limb-Sparing Quadriceps Resection for Sarcoma
Key Takeaway
This masterclass details limb-sparing quadriceps resection for sarcomas, guiding fellows through comprehensive anatomy, meticulous preoperative planning, and granular intraoperative execution. We cover precise dissection, neurovascular protection, and advanced reconstructive techniques, emphasizing critical pearls and pitfalls. Learn patient positioning, incision planning, and muscle-specific resections, along with essential postoperative care for optimal functional outcomes in these complex oncologic cases.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater and to this definitive masterclass. Today, we are tackling a challenging yet immensely rewarding oncologic procedure: a limb-sparing quadriceps resection for a soft tissue sarcoma. This operation demands meticulous preoperative planning, precise three-dimensional anatomical knowledge, and unwavering surgical discipline. Our fundamental goal is not merely the eradication of the tumor with negative oncologic margins, but also the maximization of functional limb preservation, which significantly dictates our patients' long-term quality of life and ambulatory independence.
The quadriceps muscle group represents the single most common anatomical site for the development of extremity soft tissue sarcomas (STS). Within this robust anterior compartment, we frequently encounter a diverse array of histologic subtypes, most notably pleomorphic liposarcomas, undifferentiated pleomorphic sarcomas (formerly malignant fibrous histiocytomas), myxofibrosarcomas, and leiomyosarcomas. While these neoplasms can present insidiously as remarkably large, painless, deeply seated masses, the contemporary paradigm of multidisciplinary oncologic care has revolutionized our surgical approach. Advancements in multimodal therapy—specifically the utilization of neoadjuvant (induction) radiotherapy to sterilize the reactive pseudocapsule and adjuvant systemic therapies for high-grade histologies—allow us to perform safe limb-sparing resections in over 90% of patients.
Historically, massive tumors of the anterior thigh, particularly those encroaching upon the femoral neurovascular bundle, were managed with radical amputation or hip disarticulation. Today, that approach is largely obsolete. A critical paradigm shift in orthopedic oncology is the understanding that femoral nerve sacrifice is not an absolute contraindication for limb-sparing resection. While the loss of the femoral nerve inherently paralyzes the quadriceps, resulting in a profound loss of active knee extension, modern reconstructive techniques and orthotic management (such as knee-ankle-foot orthoses or dynamic bracing) permit functional, plantigrade ambulation. We can often achieve functional knee stability and patellar tracking even when the entire quadriceps muscle is resected en bloc.
Epidemiologically, soft tissue sarcomas of the extremity exhibit a bimodal age distribution, though the specific subtypes encountered in the thigh predominantly affect adults in their fifth to seventh decades of life. The biological behavior of these tumors is dictated by their histologic grade, size, and depth relative to the investing fascia. High-grade, deep tumors larger than 5 centimeters carry a substantial risk of both local recurrence and distant metastasis, primarily to the lungs. Therefore, the surgical extirpation must be viewed not in isolation, but as the central mechanical component of a comprehensive, systemic treatment strategy designed to achieve local control while mitigating the risk of distant failure.
Detailed Surgical Anatomy and Biomechanics
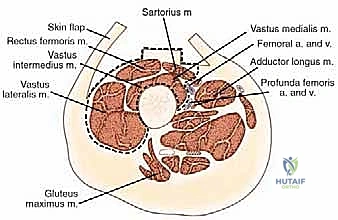
Let us begin by rigorously refreshing our understanding of the thigh's intricate topographical and cross-sectional anatomy, as this constitutes the bedrock of safe and oncologically sound surgery. The thigh is anatomically segregated into three distinct fascial compartments, each enveloped by the unyielding fascia lata and separated by robust intermuscular septa. The Anterior Compartment, our primary operative field today, houses the quadriceps femoris muscle group and the sartorius muscle. The Medial Compartment contains the adductor musculature (adductor longus, brevis, magnus, pectineus, and gracilis), while the Posterior Compartment is composed of the hamstring muscles (semitendinosus, semimembranosus, and biceps femoris). The thick fascial layers separating these compartments—the medial and lateral intermuscular septa—are critical anatomical barriers that often dictate the natural containment of tumor growth, preventing early trans-compartmental spread.
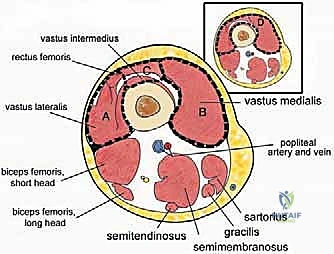
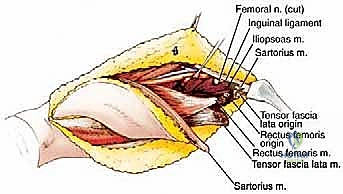
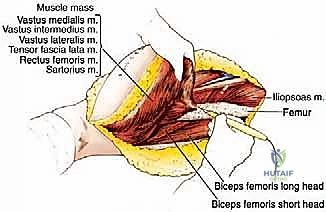
The quadriceps femoris itself is a complex functional unit comprising four distinct muscle bellies. The Rectus Femoris (RF) is unique as a biarticular muscle, crossing both the hip and knee joints. It arises via two distinct heads: the straight head from the anterior inferior iliac spine (AIIS) and the reflected head from the supra-acetabular groove. The Vastus Medialis (VM) arises from the intertrochanteric line and the medial lip of the linea aspera, inserting into the medial patellar retinaculum. The Vastus Lateralis (VL) originates from the greater trochanter and the lateral lip of the linea aspera. Deep to the rectus femoris lies the Vastus Intermedius (VI), arising from the anterior and lateral surfaces of the femoral shaft. Critically, from an oncologic perspective, the vastus intermedius acts as a protective physiological barrier, shielding the underlying femoral cortex from direct tumor extension by lesions originating in the more superficial quadriceps components.
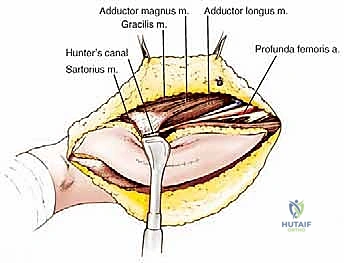
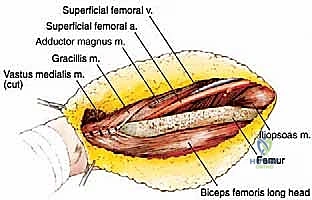
The femoral triangle and the adductor (Hunter's) canal represent vital anatomical landmarks, particularly for proximal resections. The femoral triangle is bounded superiorly by the inguinal ligament, medially by the lateral border of the adductor longus, and laterally by the medial border of the sartorius. Within this space, from lateral to medial, lie the femoral nerve, femoral artery, and femoral vein. The femoral nerve arborizes rapidly to innervate the quadriceps. The superficial femoral artery and vein continue distally into the adductor canal. These vessels run along the medial wall of the canal, separated from the vastus medialis by a thick, aponeurotic fascial layer. This specific fascial plane often provides a crucial, tumor-free margin for safe resection, allowing the surgeon to dissect the tumor away from the neurovascular bundle without violating the reactive zone.
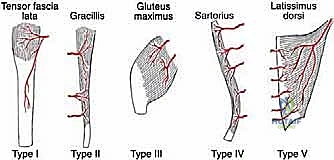
When massive resections necessitate local muscle transfers to obliterate dead space or reconstruct the extensor mechanism, understanding the precise vascular supply of these flaps is paramount. According to the Mathes and Nahai classification, the sartorius muscle exhibits a Type IV segmental vascular pattern, supplied by multiple pedicles from the superficial femoral artery. Division of more than three pedicles during elevation risks distal necrosis. Conversely, the hamstring muscles (e.g., biceps femoris, semitendinosus) possess a Type II vascular pattern, with dominant proximal pedicles from the profunda femoris and minor distal pedicles. This allows for reliable, complete mobilization of the hamstrings provided the dominant proximal pedicle is meticulously preserved.
Exhaustive Indications and Contraindications
The decision to proceed with a limb-sparing quadriceps resection must be made following a rigorous, multidisciplinary evaluation. The absolute primary indication for this procedure is the presence of a biopsy-proven soft tissue sarcoma located within the anterior compartment of the thigh, where preoperative imaging and staging indicate that an R0 (microscopically negative) resection margin can be achieved without compromising the fundamental viability of the limb. Limb salvage is indicated for almost all Enneking Stage IA, IB, IIA, and IIB tumors, provided the anatomical constraints allow for complete extirpation. Furthermore, even in the presence of isolated, resectable pulmonary metastases (Stage III), local tumor control via limb-sparing surgery is indicated to prevent fungation, intractable pain, and loss of local function, thereby maintaining the patient's quality of life during systemic therapy.
However, the surgeon must be acutely aware of the contraindications, which dictate when limb salvage is either oncologically unsafe or functionally inferior to amputation. A critical evaluation of the neurovascular bundle is required. While femoral nerve involvement is no longer an absolute contraindication, simultaneous encasement of the superficial femoral artery, femoral vein, and sciatic nerve (a rare but catastrophic presentation) often precludes functional limb salvage. If achieving an R0 margin requires the resection of all major motor nerves and vascular conduits to the lower extremity, resulting in a flail, insensate, and ischemic limb, an above-knee amputation or hip disarticulation is the more prudent and humane choice.
Relative contraindications demand a highly nuanced risk-benefit analysis. Extensive cutaneous involvement requiring massive soft tissue resection and complex free-flap reconstruction in a severely malnourished or medically compromised host (e.g., severe peripheral vascular disease, uncontrolled diabetes) represents a significant relative contraindication. Similarly, a pathologic fracture through a tumor-infiltrated femur complicates limb salvage enormously, as the fracture hematoma disseminates microscopic disease throughout the compartment, often necessitating an en bloc extra-articular resection of the femur and total femur replacement, significantly escalating the morbidity of the procedure.
| Factor | Indication for Limb-Sparing Resection | Contraindication (Relative or Absolute) |
|---|---|---|
| Tumor Margins | High probability of achieving R0/R1 margins. | Inability to achieve R0/R1 margins (Absolute). |
| Neurovascular | Displacement of NAV; isolated femoral nerve involvement. | Encasement of major vessels AND sciatic nerve (Absolute). |
| Bone Involvement | Periosteal reaction only; resectable cortical erosion. | Pathologic fracture with massive hematoma contamination (Relative). |
| Soft Tissue/Skin | Adequate local tissue for closure or reliable local flap. | Massive skin involvement requiring complex free flap in poor host (Relative). |
| Patient Status | Medically fit for prolonged surgery and rehabilitation. | Uncontrollable sepsis; severe cardiopulmonary disease (Absolute). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough and obsessive preoperative planning is non-negotiable for these complex oncologic resections. The foundation of this planning rests upon high-resolution, multi-planar imaging. Magnetic Resonance Imaging (MRI) with and without gadolinium contrast is the gold standard for defining the local extent of the tumor. We meticulously analyze T1-weighted images to assess bone marrow involvement, while T2-weighted fat-suppressed images delineate the reactive edema zone and the tumor's relationship to the intermuscular septa and neurovascular structures. Computed Tomography (CT) of the chest, abdomen, and pelvis is mandatory for systemic staging to rule out pulmonary or visceral metastases.
If the MRI demonstrates the tumor abutting or displacing the superficial femoral or profunda femoris vessels, CT Angiography or MR Angiography is strongly indicated. This evaluates the patency of these vessels and helps formulate a contingency plan for vascular reconstruction. For instance, if the profunda femoris must be ligated to achieve margins on a massive proximal tumor, we must be absolutely certain that the superficial femoral artery is patent and capable of supplying the distal extremity. Furthermore, a three-phase technetium-99m bone scan can be useful; increased periosteal uptake adjacent to the tumor necessitates en bloc resection of the underlying periosteum, and occasionally a sliver of cortical bone, to ensure a negative deep margin.
The biopsy technique is a critical component of preoperative planning. We strongly advocate for image-guided core needle biopsy over open incisional biopsy, as it provides reliable histologic grading with minimal tissue contamination. The biopsy tract must be meticulously planned. It must be oriented longitudinally, directly in line with the planned definitive surgical incision, and placed over the most prominent, superficial aspect of the tumor without crossing any uninvolved anatomical compartments. Transgressing major neurovascular structures during biopsy is a catastrophic error, as the resulting hematoma will disseminate tumor cells, potentially converting a limb-sparing candidate into an amputee.
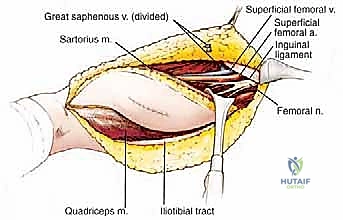
In the operating room, meticulous patient positioning sets the stage for a successful resection. The patient is placed in the supine position on a radiolucent operating table. A thick gel bolster is placed beneath the ipsilateral buttock. This maneuver slightly elevates the pelvis and internally rotates the hip, dramatically improving surgical access to the lateral and posterior aspects of the thigh, which is particularly crucial when dissecting the lateral intermuscular septum or exposing the proximal femoral triangle. Crucially, the entire ipsilateral lower extremity must be prepped and draped free to allow for dynamic manipulation during the resection. Furthermore, the contralateral lower extremity must also be prepped and draped into the sterile field; this is an essential contingency plan, providing immediate access for harvesting a reversed saphenous vein graft should the ipsilateral femoral vessels require en bloc resection and reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Flap Elevation
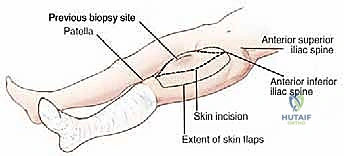
The surgical approach begins with precise incision planning. Using a sterile surgical marker, the palpable borders of the tumor are outlined, followed by the planned incision. For a comprehensive quadriceps resection, we utilize a long, longitudinal elliptical incision. This incision typically extends from the anterior inferior iliac spine (AIIS) proximally, traversing distally to the superior pole of the patella. The ellipse must widely encompass the previous core needle biopsy site, incorporating a minimum of 1 to 2 centimeters of healthy skin margin around the tract to prevent local seeding. If preoperative MRI indicates tumor extension toward the extensor mechanism insertion, the incision is extended distally over the patella down to the tibial tubercle.
Following the skin incision, full-thickness dermo-subcutaneous flaps are elevated medially and laterally. The critical plane of dissection here is strictly superficial to the fascia lata. It is imperative to maintain the integrity of the fascia lata at this stage, as it serves as the superficial anatomical barrier containing the tumor within the anterior compartment. The medial flap is elevated to expose the sartorius and the adductor musculature, while the lateral flap is mobilized to expose the iliotibial band and the lateral intermuscular septum. Meticulous hemostasis is maintained throughout flap elevation using electrocautery to ligate perforating vessels, minimizing postoperative hematoma formation.
Deep Dissection and Neurovascular Isolation
Once the flaps are elevated, the deep dissection commences with the identification and isolation of the critical neurovascular structures. The deep fascia is incised medially, parallel to the medial border of the sartorius muscle, to enter the femoral triangle. The femoral artery and vein are identified and carefully traced distally into the adductor canal. Vascular loops are placed around the vessels for control.

The dissection proceeds by developing the plane between the superficial femoral vessels and the medial aspect of the vastus medialis. This is often an avascular plane, save for specific perforating branches that must be meticulously identified, ligated, and divided.
Attention is then turned to the femoral nerve. If the tumor is localized to the distal or lateral quadriceps, the main trunk of the femoral nerve can often be preserved, sacrificing only the specific motor branches entering the involved muscle bellies. However, if the tumor originates in the proximal rectus femoris or vastus intermedius and encases the nerve, the nerve must be sacrificed en bloc with the specimen to ensure an R0 margin.

As the dissection progresses laterally, the lateral intermuscular septum is identified. The vastus lateralis is separated from the biceps femoris along this septum. Perforating branches from the profunda femoris artery piercing the septum must be anticipated and securely ligated.
En Bloc Resection of the Quadriceps
With the medial, lateral, and neurovascular boundaries established, the proximal and distal extents of the resection are addressed. Proximally, the origins of the involved muscles are detached. For a complete quadriceps resection, the rectus femoris is transected at its origin on the AIIS, and the vasti are elevated off the intertrochanteric line and linea aspera.
The deep margin is typically the anterior cortex of the femur. The vastus intermedius is elevated off the periosteum. If preoperative imaging or intraoperative inspection suggests periosteal adherence, the periosteum is incised longitudinally adjacent to the linea aspera and stripped circumferentially, leaving it attached to the deep surface of the tumor mass.

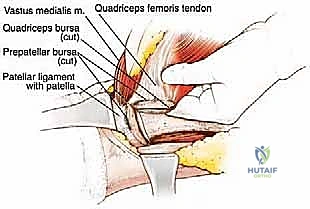
Distally, the quadriceps tendon is transected. If the tumor is proximal, a cuff of normal tendon may be preserved for subsequent reconstruction. If the tumor extends distally, the tendon is transected at the superior pole of the patella. The entire tumor, enveloped within its muscular and fascial boundaries, is then delivered en bloc from the surgical field and sent for immediate pathological evaluation of the margins.
Extensor Mechanism Reconstruction
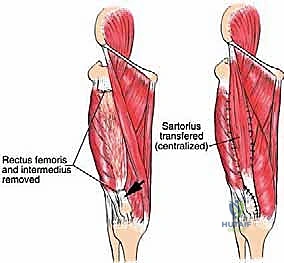
Following extirpation, the massive anatomical defect and loss of the extensor mechanism must be addressed. If a partial resection was performed (e.g., isolated vastus lateralis excision), the remaining vastus medialis and rectus femoris can often be mobilized and sutured together to centralize the pull on the patella.
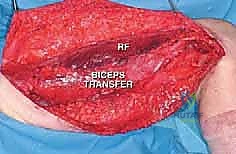
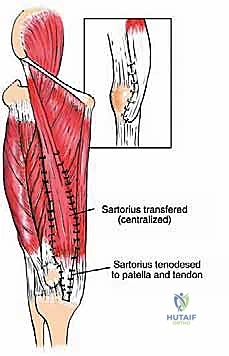
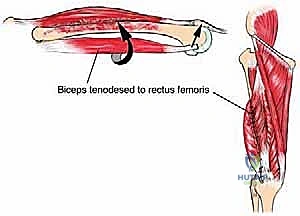
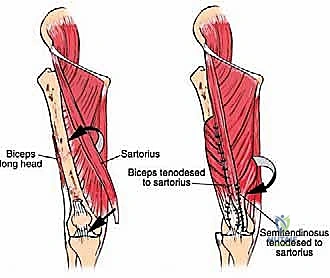
In cases of complete quadriceps resection, reconstruction is highly complex. Options include the transfer of the medial or lateral hamstring muscles (biceps femoris or semitendinosus/gracilis) to the patella to restore active extension. Alternatively, if active extension cannot be restored (e.g., due to femoral nerve sacrifice), static stabilization of the patella is crucial to prevent subluxation and provide a stable fulcrum for passive extension during the swing phase of gait. This can be achieved using synthetic mesh, allograft tendon (such as Achilles tendon allograft), or local fascial flaps to tether the patella to the proximal femur or remaining viable tissues.
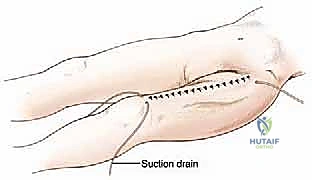
Meticulous closure is performed over large-bore closed suction drains. The subcutaneous tissues are approximated to eliminate dead space, and the skin is closed with non-absorbable sutures or staples, keeping in mind that these tissues have often been subjected to neoadjuvant radiation.
Complications, Incidence Rates, and Salvage Management
The radical nature of a limb-sparing quadriceps resection, frequently compounded by the tissue-depleting effects of neoadjuvant radiotherapy, inherently carries a substantial risk profile. Wound complications are the most frequently encountered morbidity, with reported incidence rates ranging from 25% to 35%. These manifest as delayed healing, wound dehiscence, profound seroma formation, or deep surgical site infections. The massive dead space created by the extirpation of the quadriceps serves as a nidus for fluid accumulation. Meticulous intraoperative hemostasis, prolonged use of closed-suction drains, and occasionally, the prophylactic use of pedicled muscle flaps (such as a gastrocnemius flap for distal defects or a rectus abdominis flap for massive proximal defects) are critical strategies to mitigate these risks.
Neurovascular complications, while less frequent, are potentially devastating. Deep vein thrombosis (DVT) and subsequent pulmonary embolism (PE) are significant risks due to prolonged operative times, vessel manipulation, and postoperative immobility. Routine mechanical and pharmacological prophylaxis is mandatory. Inadvertent injury to the superficial femoral artery or vein during tumor dissection can lead to catastrophic limb ischemia or massive hemorrhage; immediate vascular surgery consultation and interposition grafting with a reversed saphenous vein are required for salvage. Ischemic neuropathy of the sciatic nerve can also occur secondary to prolonged retraction or altered vascular dynamics within the thigh.
Oncologic failures remain the most feared complications. Local recurrence (LR) occurs in approximately 10% to 15% of patients, heavily dependent on the histologic grade and the adequacy of the surgical margins. An R1 (microscopically positive) or R2 (macroscopically positive) margin dramatically increases the LR rate. Management of a local recurrence requires a rigorous restaging process. If the recurrence is isolated and anatomically amenable, a radical re-excision may be attempted; however, recurrent tumors frequently involve critical neurovascular structures previously exposed, often necessitating a salvage amputation to achieve local control. Distant metastasis, primarily to the lungs, dictates a poor prognosis and necessitates aggressive systemic chemotherapy or targeted biologic therapies.
| Complication Category | Specific Complication | Estimated Incidence | Salvage Management / Mitigation Strategy |
|---|---|---|---|
| Wound / Soft Tissue | Dehiscence, Seroma, Deep Infection | 25% - 35% | Prolonged drains, negative pressure wound therapy, pedicled flap coverage, aggressive IV antibiotics. |
| Neurovascular | DVT / PE, Arterial Thrombosis | 5% - 10% |
