Critical Elbow Applied Surgical Anatomy: Enhance Your Practice
Key Takeaway
Discover the latest medical recommendations for Critical Elbow Applied Surgical Anatomy: Enhance Your Practice. **Elbow applied surgical** anatomy describes the hinge joint formed by the humerus, radius, and ulna, supported by strong collateral ligaments. Understanding its intricate structure and surrounding muscle groups is crucial for surgical planning. Complete exposure is often achieved through a posterior approach, while specific internervous planes guide precise anterolateral or medial surgical access, minimizing complications and preserving nerve integrity.
Introduction and Epidemiology
The elbow joint represents a highly constrained, complex articulation that demands precise anatomical restoration following trauma or degenerative changes to maintain upper extremity function. As a modified hinge (ginglymus) joint, it facilitates not only flexion and extension but also forearm rotation via its communication with the proximal radioulnar joint. A profound understanding of applied surgical anatomy is paramount for the orthopedic surgeon, as the dense concentration of neurovascular structures and the highly congruent osseous architecture leave little margin for surgical error.

Epidemiologically, elbow trauma accounts for a significant portion of orthopedic emergencies and elective reconstructions. Distal humerus fractures comprise approximately 2% of all adult fractures, while radial head fractures account for nearly one-third of all elbow fractures. Complex instability patterns, such as the "terrible triad" of the elbow (elbow dislocation combined with radial head and coronoid process fractures), present formidable challenges. The margin between functional recovery and debilitating stiffness or chronic instability is narrow. Consequently, surgical interventions must be predicated on a meticulous understanding of the osseous landmarks, capsuloligamentous restraints, and internervous planes to optimize exposure while minimizing iatrogenic morbidity.
Surgical Anatomy and Biomechanics
The osseous anatomy of the elbow dictates its kinematics and inherent stability. The distal end of the humerus articulates in two distinct areas. Laterally, the capitulum articulates with the radial head. Its geometry is hemispheric, allowing for complex multi-axial rotation during forearm pronation and supination while simultaneously maintaining radiocapitellar contact during flexion and extension. Medially, the trochlea articulates with the greater sigmoid notch of the ulna.
The trochlea resembles a spool of thread and extends further distally than the capitulum. This distal extension creates a spatial configuration that tilts the lower end of the humerus, yielding the physiological "carrying angle" of the joint (typically 10 to 15 degrees of valgus in full extension). The trochlea is deeply grooved; the boundaries of this groove are defined medially by a prominent, sharp ridge and laterally by a lower, more blunted ridge. A distinct ridge of bone separates the capitellar and trochlear articulations.
Biomechanically, the elbow relies on both primary and secondary stabilizers. The primary stabilizers are the ulnohumeral articulation, the medial collateral ligament (MCL) complex, and the lateral collateral ligament (LCL) complex.
The anterior bundle of the MCL is the primary restraint to valgus stress, particularly between 30 and 120 degrees of flexion. The LCL complex, specifically the lateral ulnar collateral ligament (LUCL), is the primary restraint to varus and posterolateral rotatory instability. The anterior and posterior capsules are relatively thin, thickened only in specific sections to allow the extensive arc of motion expected from a hinge joint.
Four distinct groups of muscles cross the elbow joint, creating specific anatomical compartments and intermuscular intervals:
1. Anteriorly, the flexors of the elbow (biceps brachii, brachialis), supplied primarily by the musculocutaneous nerve.
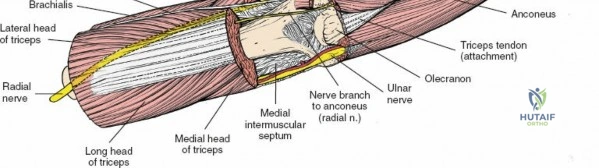
2. Posteriorly, the extensor of the elbow (triceps brachii), supplied by the radial nerve.
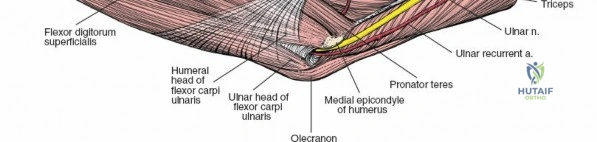
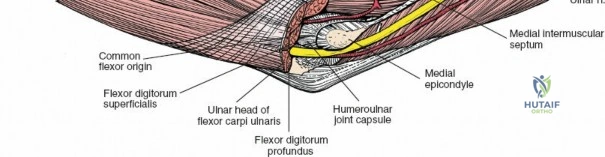
3. Medially, the flexor-pronator mass (pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris, flexor digitorum superficialis), supplied by the median and ulnar nerves. These originate from the medial epicondyle.
4. Laterally, the mobile wad and extensors (brachioradialis, extensor carpi radialis longus and brevis, supinator, extensor digitorum communis), supplied by the radial and posterior interosseous nerves. These originate from the lateral epicondyle and supracondylar ridge.
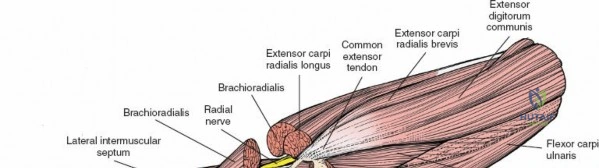
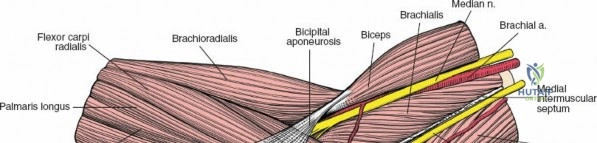
The medial and lateral muscle groups converge in the proximal forearm to form the cubital fossa. This triangular space is bordered medially by the pronator teres and laterally by the brachioradialis. The superior border is an imaginary line connecting the medial and lateral epicondyles. The contents, from medial to lateral, include the median nerve, brachial artery, biceps tendon, and radial nerve (often remembered by the mnemonic MBBR or TAN - Tendon, Artery, Nerve from lateral to medial).
Indications and Contraindications
Surgical intervention around the elbow is dictated by the necessity to restore articular congruity, re-establish joint stability, and allow for early active motion to prevent the rapid onset of capsular contracture.

Absolute indications include open fractures, vascular compromise, and irreducible dislocations. Relative indications encompass displaced intra-articular fractures, terrible triad injuries, and symptomatic chronic instability. Contraindications are generally related to severe systemic illness, active local infection, or a non-ambulatory patient with a painless pseudarthrosis that does not limit their baseline activities of daily living.

Operative and Non Operative Management Parameters
| Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Radial Head Fractures | Mason Type III/IV; Mechanical block to rotation; >30% articular involvement with >2mm step-off. | Mason Type I; Mason Type II without mechanical block; Non-displaced fractures. |
| Distal Humerus Fractures | Displaced intra-articular fractures; Supracondylar instability; Open fractures. | Non-displaced fractures; Severe dementia/non-ambulatory status (bag of bones technique). |
| Coronoid Fractures | O'Driscoll Anteromedial facet fractures; Type II/III associated with instability (Terrible Triad). | Isolated Type I (tip) fractures with a stable joint through a full arc of motion. |
| Elbow Dislocation | Persistent instability post-reduction; Incongruent joint; Associated complex fractures. | Stable joint post-closed reduction (concentric reduction maintained in extension). |
| Olecranon Fractures | Displaced fractures disrupting the extensor mechanism; Intra-articular step-off >2mm. | Non-displaced fractures with intact active extension against gravity. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is mandatory. Standard anteroposterior and lateral radiographs are requisite, but computed tomography (CT) with 3D reconstructions has become the gold standard for evaluating complex articular comminution, particularly in distal humerus and coronoid fractures.

Patient positioning is dictated by the surgical approach chosen, which in turn is driven by the pathology.
1. Supine Position: Utilized primarily for anterior and anterolateral approaches. The arm is extended on a radiolucent hand table. A sterile tourniquet may be utilized. This position is excellent for radial head excision/replacement, capitellar fractures, and anterior capsular release.
2. Lateral Decubitus Position: The patient is placed in the lateral position with the operative arm draped over a well-padded post (e.g., L-bar). This allows the elbow to rest at 90 degrees of flexion and provides excellent access to the posterior, medial, and lateral aspects of the joint. It is highly advantageous for total elbow arthroplasty and complex distal humerus fractures.

- Prone Position: The arm is draped over a bolster. This provides unparalleled access to the posterior humerus and olecranon. It is frequently used for triceps-sparing or olecranon osteotomy approaches to the distal humerus. However, airway management and anesthesiology considerations make this position more complex to set up.

Regardless of the position, meticulous padding of all bony prominences (particularly the contralateral fibular head and ulnar nerve) is imperative to prevent perioperative compression neuropathies. A sterile tourniquet is typically applied high on the brachium to ensure adequate exposure of the surgical field while maintaining a bloodless environment for the identification of critical neurovascular structures.
Detailed Surgical Approach and Technique
The shape of the bones comprising the elbow joint and the presence of strong collateral ligaments make it difficult to explore the joint completely without extensive dissection. Medial and lateral approaches provide limited access unless extended. Complete exposure is obtained most easily through a posterior approach. However, navigating the internervous planes allows for targeted, safe access to specific anatomical zones.
Anterior and Anterolateral Approaches
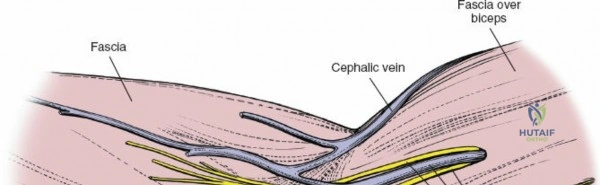
The anterolateral approach utilizes the internervous plane between the anterior and lateral muscle groups. Specifically, this is the interval between the brachialis (supplied by the musculocutaneous nerve) and the brachioradialis (supplied by the radial nerve).

During dissection, the lateral cutaneous nerve of the forearm must be identified and protected in the subcutaneous tissue. As the interval is developed, the radial nerve is identified lying between the brachialis and brachioradialis. The nerve must be gently retracted laterally. The anterior capsule is then exposed by retracting the brachialis medially. This approach is highly effective for addressing capitellar fractures, anterior capsular contractures, and proximal radius pathology.
Medial Approaches
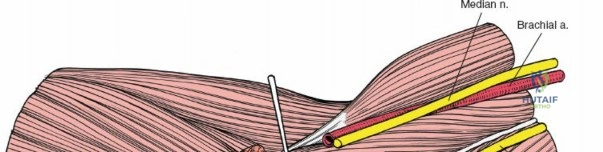
The medial approach exploits the internervous plane between the anterior and medial muscle groups: the brachialis (musculocutaneous nerve) and the pronator teres (median nerve).
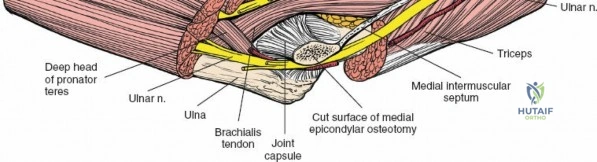
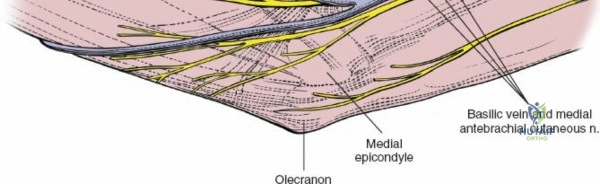
The medial antebrachial cutaneous nerve is at risk during the superficial dissection. The ulnar nerve must be identified posteriorly behind the medial epicondyle and protected; it is often routinely decompressed or transposed depending on the extent of the medial dissection required. The median nerve and brachial artery are protected by retracting the pronator teres medially and the brachialis laterally. This approach provides direct access to the medial collateral ligament complex, the coronoid process (via an "over-the-top" or split flexor-pronator mass technique), and the medial aspect of the distal humerus.

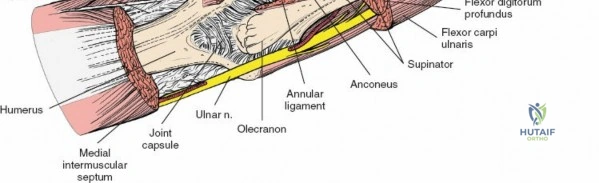
Posterolateral Approach of Kocher
This is the workhorse approach for the radial head and capitellum. It utilizes a true internervous plane between two members of the lateral group: the anconeus muscle (supplied by the radial nerve) and the extensor carpi ulnaris (ECU) muscle (supplied by the posterior interosseous nerve, a major branch of the radial nerve).

The incision is made from the lateral epicondyle directed distally toward the ulnar crest. The anconeus is retracted posteriorly and the ECU anteriorly. Deep to this interval lies the lateral collateral ligament complex and the joint capsule.

The capsule must be incised anterior to the equator of the radial head to avoid iatrogenic injury to the lateral ulnar collateral ligament (LUCL), which inserts on the supinator crest of the ulna. Furthermore, dissection distal to the annular ligament places the posterior interosseous nerve (PIN) at significant risk as it winds through the supinator muscle. Pronating the forearm during distal exposure moves the PIN anteriorly, maximizing the safe zone.

Lateral Approach
A pseudointernervous plane exists between the lateral and posterior groups of muscles. It is not a true internervous plane because both groups are supplied by the radial nerve. However, the plane is highly useful because the radial nerve gives off its branches well proximal to the elbow joint.

This interval falls between the brachioradialis and the triceps muscles. It is utilized to expose the lateral column of the distal humerus. The radial nerve must be identified proximally as it pierces the lateral intermuscular septum to pass from the posterior to the anterior compartment, ensuring its protection during plate osteosynthesis of the lateral column.

Posterior Approaches
Complete exposure of the distal humerus articular surface requires a posterior approach. The skin incision is typically a posterior midline incision, curving slightly radially around the tip of the olecranon to prevent a painful scar over the bony prominence.

Deep dissection options include:
1. Olecranon Osteotomy: Provides the greatest visualization of the articular surface. A chevron osteotomy is performed bare-area of the greater sigmoid notch. The olecranon and attached triceps are reflected proximally.
2. Triceps-Reflecting (Bryan-Morrey): The triceps is detached from the olecranon along with the periosteum and reflected laterally.
3. Triceps-Sparing (Paratricipital): Windows are created medially and laterally to the triceps. Useful for extra-articular fractures or simple intra-articular splits.
4. Triceps-Reflecting Anconeus Pedicle (TRAP): A modification preserving the anconeus pedicle for better vascularity.
In all posterior approaches, the ulnar nerve must be identified, neurolysed, and protected throughout the procedure.
Complications and Management
Surgical management of the elbow is fraught with potential complications due to the unforgiving nature of the joint capsule and the proximity of delicate neurovascular structures. Meticulous surgical technique, anatomical handling of tissues, and rigid internal fixation are required to mitigate these risks.

Post-traumatic stiffness is the most common complication following elbow surgery. The anterior capsule is highly prone to fibroblastic proliferation and contracture. Heterotopic ossification (HO) is another significant risk, particularly in patients with head trauma, burns, or extensive soft tissue stripping.
Neurovascular injuries, either from the initial trauma or iatrogenic during exposure, require immediate recognition. The ulnar nerve is highly susceptible to traction neuritis or entrapment in scar tissue. The posterior interosseous nerve (PIN) is at risk during lateral and anterolateral exposures.
Incidence and Salvage Strategies for Complications
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Elbow Stiffness | 15% - 20% | Prolonged immobilization; Capsular contracture; Prominent hardware. | Aggressive physical therapy; Static progressive splinting; Open or arthroscopic capsular release. |
| Ulnar Neuropathy | 10% - 15% | Traction during surgery; Hardware impingement; Post-op swelling. | Observation if mild; Hardware removal; Ulnar nerve neurolysis and anterior transposition. |
| Heterotopic Ossification | 5% - 10% | Severe trauma; Concomitant TBI; Delayed surgery; Excessive tissue stripping. | Prophylaxis (Indomethacin/Radiation); Surgical excision once bone is mature (typically >6 months) with normal serum alkaline phosphatase. |
| Hardware Failure / Nonunion | 2% - 5% | Inadequate fixation; Poor bone quality (osteoporosis); Infection. | Revision open reduction internal fixation (ORIF) with bone grafting; Consideration of Total Elbow Arthroplasty (TEA) in older patients. |
| PIN Injury | 1% - 3% | Dissection distal to the annular ligament; Retractor pressure. | Observation for neuropraxia (EMG at 6 weeks); Tendon transfers if permanent deficit occurs. |
Post Operative Rehabilitation Protocols
The overarching goal of elbow rehabilitation is the immediate initiation of active and active-assisted range of motion to prevent capsular contracture. The elbow tolerates immobilization poorly; immobilization beyond two to three weeks is strongly associated with permanent motion deficits.

In the immediate postoperative phase (Days 1-14), edema control and pain management are prioritized. If rigid internal fixation has been achieved, active motion within a safe arc is initiated. For example, following a terrible triad repair, the elbow is often stable in pronation (which tightens the medial structures and protects the lateral repair). Therefore, extension exercises are performed with the forearm in pronation.
In the intermediate phase (Weeks 2-6), static progressive splinting may be introduced if the patient is not achieving anticipated milestones (typically aiming for an arc of 30 to 130 degrees). Passive stretching is generally avoided as it can induce microtrauma, exacerbating inflammation and promoting heterotopic ossification.
In the late phase (Weeks 6-12), strengthening exercises are incorporated as radiographic evidence of bone healing becomes apparent. Return to heavy labor or sports is typically delayed until 4 to 6 months postoperatively, contingent upon the restoration of functional strength and stability.
Summary of Key Literature and Guidelines
Academic mastery of elbow surgery requires familiarity with foundational biomechanical and clinical literature. Morrey's seminal work on the kinematics of the elbow established the concept of the instant center of rotation and the primary/secondary stabilizers, forming the basis for modern ligamentous reconstruction.
O'Driscoll's description of posterolateral rotatory instability (PLRI) revolutionized the understanding of lateral collateral ligament injuries, shifting the focus to the anatomical reconstruction of the LUCL. Furthermore, Jupiter's principles for the management of distal humerus fractures—emphasizing rigid bicolumnar fixation with plates placed in orthogonal or parallel configurations—remain the gold standard for achieving stability sufficient to permit early motion.
Current guidelines from orthopedic trauma societies strongly advocate for early surgical intervention in complex elbow instability, minimizing reliance on prolonged cast immobilization. The integration of 3D-printed patient-specific instrumentation and advanced arthroscopic techniques continues to evolve, yet the fundamental requirement remains unchanged: a profound, applied understanding of elbow surgical anatomy.
