Surgical Anatomy of the Arm: Navigating Key Neurovascular Structures

Key Takeaway
Here are the crucial details you must know about Surgical Anatomy of the Arm: Navigating Key Neurovascular Structures. The anatomy of the arm consists of two major muscle compartments. The anterior flexor compartment contains the coracobrachialis, biceps brachii, and brachialis muscles, supplied by the musculocutaneous nerve. The posterior extensor compartment comprises the triceps brachii, supplied by the radial nerve. Critical neurovascular structures, including the radial nerve, traverse these compartments, making their interrelationships essential for surgical understanding.
As an academic orthopedic surgeon and medical educator, it is imperative to possess a comprehensive and nuanced understanding of the surgical anatomy of the arm. The region's intricate interplay of musculature, bone, and critical neurovascular structures necessitates meticulous planning and execution during any operative intervention. This document serves as a high-yield reference, designed for orthopedic surgeons, residents, and medical students, emphasizing the practical implications of anatomy in navigating complex surgical scenarios within the arm.
Introduction and Epidemiology
The human arm is a marvel of evolutionary engineering, providing both power and dexterity essential for activities of daily living, work, and sport. Consequently, injuries and conditions affecting the arm are prevalent, often necessitating surgical intervention to restore form and function. Fractures of the humerus, nerve compression syndromes, and vascular compromise represent common pathologies encountered by orthopedic surgeons.
Humeral shaft fractures, for instance, account for approximately 3-5% of all fractures, with a bimodal distribution peaking in young males (high-energy trauma) and elderly females (low-energy falls). These fractures carry a significant risk of associated neurovascular injury, particularly to the radial nerve, given its intimate course around the humeral shaft. Proximal humeral fractures are common in the elderly, often involving the surgical neck, which lies in close proximity to the axillary nerve. Distal humeral fractures, while less common, frequently involve the median and ulnar nerves and the brachial artery, demanding precise anatomical understanding for successful outcomes.
The high incidence of these injuries, coupled with the functional importance of the arm and the vulnerability of its neurovascular contents, underscores the critical need for a detailed comprehension of surgical anatomy. This guide will meticulously detail the anatomical landmarks, compartments, and neurovascular pathways to facilitate safer and more effective surgical approaches.
Surgical Anatomy and Biomechanics
The arm, or brachium, extends from the shoulder to the elbow, housing muscles responsible for shoulder, elbow, and forearm movement, along with the major neurovascular bundles supplying the entire upper limb distal to the axilla.
Muscular Compartments and Intermuscular Septa
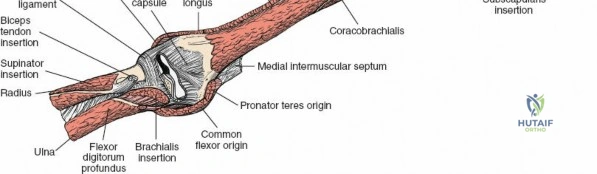
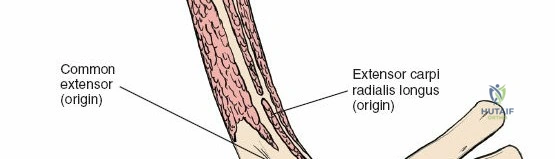
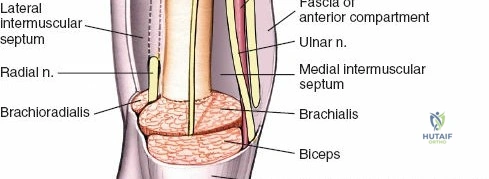
The arm is divided into two primary fascial compartments by medial and lateral intermuscular septa, which extend from the deep fascia to the humerus. These septa are crucial surgical landmarks, often providing relatively avascular planes for dissection.
Anterior Flexor Compartment
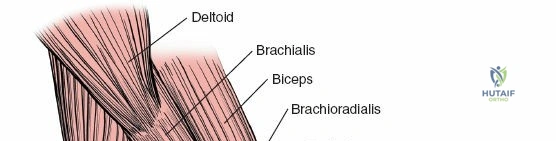
This compartment contains three muscles, all primarily involved in elbow flexion and supplied by the musculocutaneous nerve:
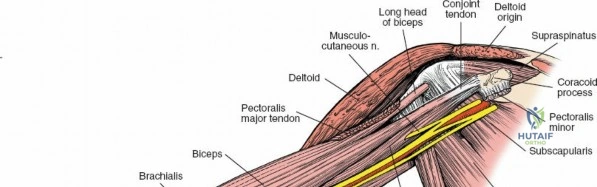
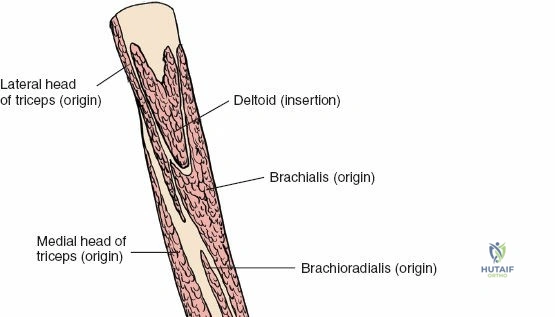
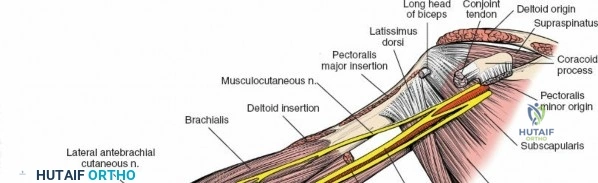
1. Coracobrachialis: Originates from the coracoid process of the scapula and inserts onto the medial surface of the mid-humeral shaft. It assists in shoulder flexion and adduction. The musculocutaneous nerve often pierces this muscle.
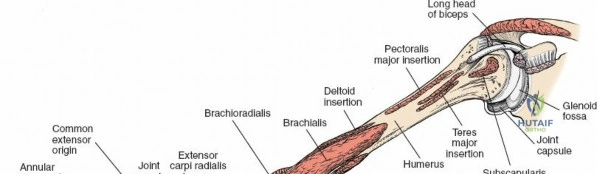
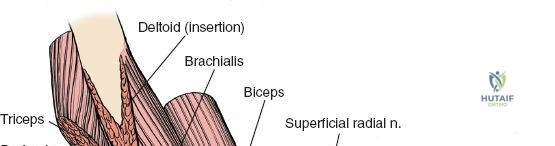
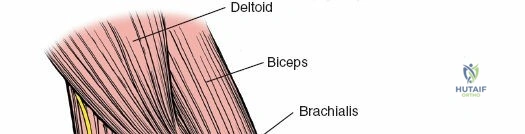
2. Biceps Brachii: Composed of a long head (originating from the supraglenoid tubercle of the scapula) and a short head (originating from the coracoid process). Both heads unite to form a common belly, inserting via a strong tendon onto the radial tuberosity and through the bicipital aponeurosis into the deep fascia of the forearm. It is a powerful supinator of the forearm and flexor of the elbow.
3. Brachialis: Lies deep to the biceps brachii, originating from the anterior surface of the distal half of the humerus and inserting onto the coronoid process and tuberosity of the ulna. It is the primary pure flexor of the elbow.
All three muscles of the anterior compartment are supplied by the musculocutaneous nerve.
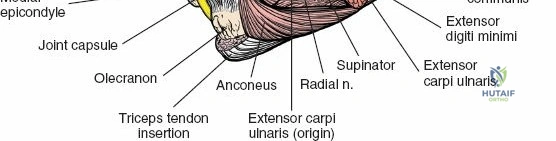
Posterior Extensor Compartment
This compartment consists primarily of one large muscle, the triceps brachii, which is the sole extensor of the elbow and is supplied by the radial nerve.
1. Triceps Brachii: Composed of three heads:
* Long Head: Originates from the infraglenoid tubercle of the scapula, contributing to shoulder extension and adduction.
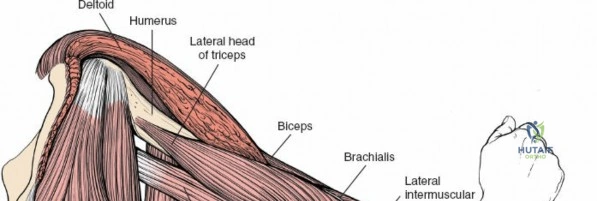
* Lateral Head: Originates from the posterior surface of the humerus, superior to the radial groove.
* Medial Head: Originates from the posterior surface of the humerus, inferior to the radial groove.
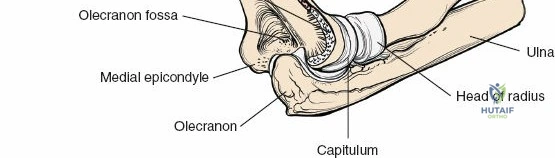
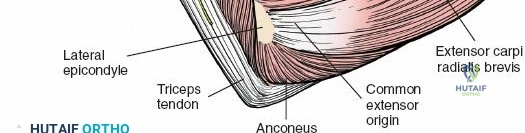
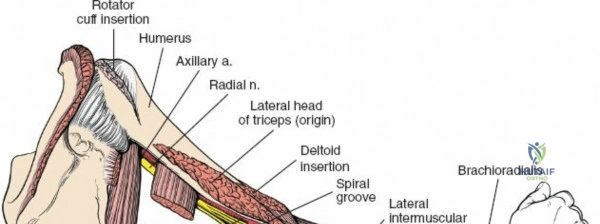
All three heads converge to insert via a common tendon onto the olecranon process of the ulna. The radial nerve courses intimately with the medial head within the spiral groove.

In the distal two-thirds of the arm, these muscle compartments are distinctly separated by lateral and medial intermuscular septa, which provide significant structural barriers and guide surgical dissection.
Key Neurovascular Structures
Navigating the arm surgically demands precise knowledge of the course and relations of its major nerves and vessels to prevent iatrogenic injury.
Nerves of the Arm
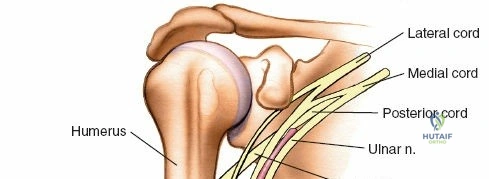
The major nerves of the arm are continuations of the brachial plexus.
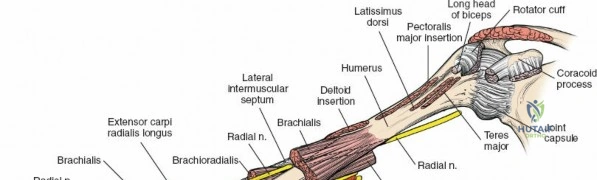
Radial Nerve
The radial nerve (C5-T1) is particularly vulnerable to injury during humeral shaft fractures, especially in the middle and distal thirds of the humerus.
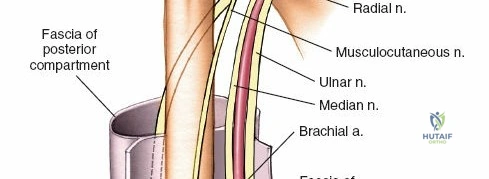
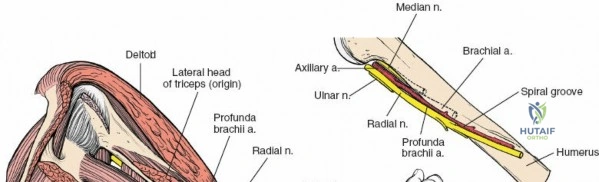
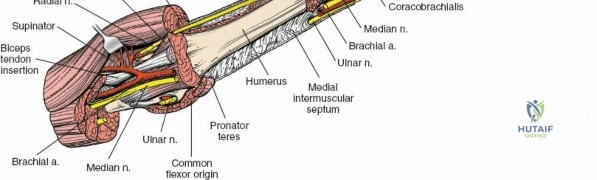
It descends posterior to the brachial artery, anterior to the long head of the triceps, and then passes inferiorly and laterally, winding around the posterior aspect of the humerus in the spiral groove (radial groove) between the lateral and medial heads of the triceps.
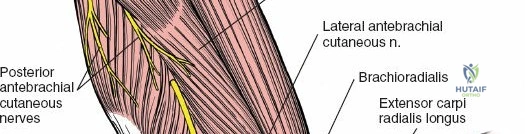
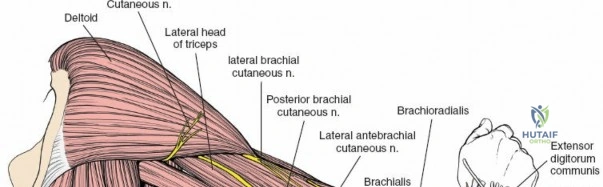
Here, it is accompanied by the profunda brachii artery. As it spirals, it gives off branches to the three heads of the triceps and the anconeus, as well as the posterior cutaneous nerve of the arm and the inferior lateral cutaneous nerve of the arm. It then pierces the lateral intermuscular septum to enter the anterior compartment, lying between the brachialis and brachioradialis muscles, just proximal to the lateral epicondyle.

In the cubital fossa, it divides into its deep (posterior interosseous) and superficial terminal branches. The presence of a new radial nerve palsy following fracture reduction, or in a closed fracture, is a strong indication for nerve exploration to rule out entrapment.
Median Nerve
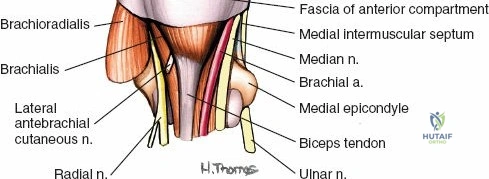
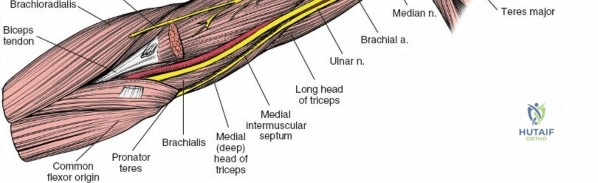
The median nerve (C5-T1) descends on the lateral side of the brachial artery in the proximal arm, crossing anterior to the artery (or sometimes posterior to it) to lie on its medial side in the distal arm. It does not give off any branches in the arm itself but supplies the majority of the flexor-pronator muscles of the forearm and thenar eminence. It is a critical structure to protect during anterior and anteromedial approaches to the distal humerus.
Ulnar Nerve
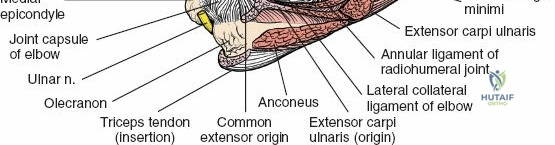
The ulnar nerve (C7-T1) courses initially on the medial aspect of the arm, deep to the biceps and medial to the brachial artery. In the mid-arm, it pierces the medial intermuscular septum to enter the posterior compartment. It then descends along the medial head of the triceps, lying directly on the posterior surface of the medial epicondyle in the cubital tunnel. It gives no branches in the arm and is particularly susceptible to iatrogenic injury during procedures around the elbow.
Musculocutaneous Nerve
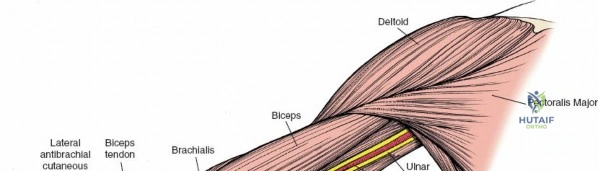
The musculocutaneous nerve (C5-C7) typically pierces the coracobrachialis muscle within the proximal arm. It then descends between the biceps brachii and brachialis muscles, supplying all three muscles of the anterior compartment. It emerges laterally to the biceps tendon as the lateral cutaneous nerve of the forearm (or lateral antebrachial cutaneous nerve), a sensory nerve. This nerve is at risk during anterior shoulder and proximal arm approaches.
Axillary Nerve
The axillary nerve (C5-C6) is typically considered a nerve of the shoulder and axilla, but its proximity to the surgical neck of the humerus makes it highly relevant for proximal humeral fracture fixation. It wraps around the surgical neck, supplying the deltoid and teres minor muscles. It is at significant risk during deltopectoral and deltoid-splitting approaches to the proximal humerus.

Vessels of the Arm
The primary arterial supply to the arm is the brachial artery and its branches, originating as a continuation of the axillary artery.
Brachial Artery
The brachial artery is the main arterial trunk of the arm. It begins at the inferior border of the teres major muscle and courses distally to the cubital fossa, where it typically bifurcates into the radial and ulnar arteries. In the arm, it lies medial to the humerus, deep to the biceps, and is closely accompanied by the median nerve.
It provides numerous muscular branches. The most significant branch in the arm is the profunda brachii artery.
Profunda Brachii Artery (Deep Brachial Artery)
This large artery branches off the brachial artery in the proximal arm and accompanies the radial nerve in the spiral groove of the humerus. It supplies the triceps muscle and the humerus itself, forming anastomoses around the elbow. Its presence with the radial nerve makes both structures vulnerable in mid-shaft humeral fractures.
Brachial Veins
Typically, two brachial veins accompany the brachial artery, forming venae comitantes, which eventually merge to form the axillary vein.
Superficial Veins
The cephalic vein (lateral aspect) and basilic vein (medial aspect) are major superficial veins. The basilic vein pierces the deep fascia in the mid-arm to join the brachial veins, while the cephalic vein continues into the deltopectoral groove. Both are important landmarks and can be mistaken for deeper structures or injured during superficial dissection.

Biomechanics and Functional Relevance
The arm's anatomical design facilitates complex movements. The muscles provide the motive force, while the nerves coordinate these actions and provide sensory feedback. The integrity of the humerus is paramount for transmitting forces from the shoulder to the elbow. Disruptions, such as fractures, not only compromise bone stability but also place the surrounding neurovascular structures at risk, leading to significant functional deficits if not managed appropriately. Understanding the biomechanical consequences of each injury pattern helps guide surgical strategy to restore optimal function.

Indications and Contraindications
Surgical intervention in the arm is considered when non-operative management is unlikely to achieve satisfactory functional outcomes or when critical structures are compromised.
Operative Indications
- Humeral Shaft Fractures:
- Open fractures.
- Failure of closed reduction or maintenance of reduction.
- Polytrauma patients requiring early mobilization of other injuries.
- Segmental humeral fractures.
- Floating elbow injury (ipsilateral forearm and humeral fracture).
- Associated neurovascular injury (e.g., irreducible nerve entrapment, vascular compromise).
- Pathological fractures.
- Fractures with significant soft tissue interposition.
- Nonunion or symptomatic malunion.
- Proximal Humeral Fractures:
- Highly displaced unstable fractures (e.g., Neer 3-part, 4-part).
- Fracture-dislocations.
- Head-splitting fractures.
- Failure of non-operative management.
- Distal Humeral Fractures:
- Most displaced intra-articular fractures.
- Significant displacement of supracondylar fractures in adults.
- Nerve Entrapment/Compression Syndromes:
- Persistent or progressive neurological deficit despite conservative measures.
- Acute nerve entrapment secondary to fracture or dislocation (e.g., radial nerve in spiral groove).
- Vascular Injury:
- Acute arterial transection or thrombosis requiring repair.
- Pseudoaneurysm formation.
- Tumors:
- Primary bone or soft tissue tumors requiring resection and reconstruction.
Non Operative Indications
- Humeral Shaft Fractures:
- Minimally displaced stable fractures.
- Closed fractures without neurovascular compromise.
- Fractures amenable to functional bracing (e.g., coaptation splint followed by Sarmiento brace).
- Patients with significant comorbidities precluding surgery.
- Proximal Humeral Fractures:
- Minimally displaced fractures (Neer 1-part, stable 2-part surgical neck fractures).
- Elderly patients with low functional demands and acceptable alignment.
- Distal Humeral Fractures:
- Undisplaced epicondylar fractures.
- Stable, well-aligned supracondylar fractures in adults.
Contraindications for Surgery
- Absolute Contraindications:
- Active systemic infection or severe local soft tissue infection at the surgical site.
- Severe comorbidities where the risk of surgery outweighs the potential benefit (e.g., unstable cardiac condition, severe respiratory compromise).
- Relative Contraindications:
- Poor soft tissue envelope or compromised skin integrity precluding safe wound closure.
- Extensive open wounds requiring initial debridement and delayed closure.
- Patient non-compliance with post-operative rehabilitation.
| Indication Type | Specific Conditions (Operative) | Specific Conditions (Non-Operative) |
|---|---|---|
| Humeral Shaft | Open fractures, failed closed reduction, polytrauma, segmental, neurovascular injury, nonunion | Minimally displaced closed fractures, stable patterns, functional bracing suitable |
| Proximal Humerus | Displaced 3-4 part fractures, fracture-dislocations, head split, failed conservative management | Neer 1-part/stable 2-part fractures, elderly with low demands, acceptable alignment |
| Distal Humerus | Most displaced intra-articular fractures, significant adult supracondylar displacement | Undisplaced epicondylar fractures, stable supracondylar fractures with minimal displacement |
| Nerve Pathology | Progressive deficit, irreducible nerve entrapment secondary to fracture or dislocation | Mild symptoms, no progression, non-traumatic entrapment responsive to physical therapy/injections |
| Vascular Injury | Acute transection, thrombosis, pseudoaneurysm requiring repair | Minor contusion without flow compromise, spasm responsive to observation/vasodilators |
| Other | Pathological fractures, tumors, significant soft tissue interposition, compartment syndrome (rare in arm) | No surgical indication, extensive comorbidities outweighing benefits, patient preference for conservative care |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is paramount to anticipate anatomical challenges and optimize outcomes.
Pre Operative Planning
- Imaging Review:
- Plain Radiographs: AP and lateral views are standard. Oblique views or traction views can assist in delineating fracture patterns.
- Computed Tomography (CT): Essential for complex intra-articular fractures (proximal and distal humerus), assessing comminution, and identifying occult fracture lines. CT angiography may be used for suspected vascular injury.
- Magnetic Resonance Imaging (MRI): Useful for soft tissue assessment, nerve contusions or entrapment, tumor evaluation, or in cases of chronic pain where nerve pathology is suspected.
- Nerve Conduction Studies (NCS) and Electromyography (EMG): Indicated for pre-existing neurological deficits to establish a baseline and assess the extent of nerve damage, particularly in cases of radial nerve palsy.
- Surgical Approach Selection: Based on fracture location, pattern, soft tissue status, and associated neurovascular injuries. The goal is to maximize exposure while minimizing iatrogenic damage.
- Hardware Templating: Pre-operative templating with X-rays or CT models helps determine appropriate plate length, screw sizes, and potential need for specialized implants (e.g., locking plates for osteopenic bone, intramedullary nails).
- Neurovascular Assessment: Meticulous documentation of pre-operative neurovascular status is crucial. Discuss potential for nerve exploration, repair, or grafting with the patient if pre-existing deficits or high suspicion for injury.
- Tourniquet Considerations: Most arm surgeries benefit from a tourniquet for a bloodless field, which enhances visualization of critical structures. Ensure appropriate cuff size and pressure. Consider alternative techniques like hypotensive anesthesia for prolonged cases or when a tourniquet is contraindicated.
Patient Positioning
Proper patient positioning is critical for optimal surgical exposure, C-arm access, and patient safety. Neurovascular structures must be protected from stretch or compression.
-
Lateral Decubitus Position:
- Indication: Excellent for posterior approaches to the humerus (e.g., for radial nerve exposure, posterior plating of humeral shaft fractures), and posterior approaches to the distal humerus.
- Setup: Patient is positioned on their side with the injured arm draped freely over an arm rest, often supported by pillows or a bolster. Axillary roll placed to protect the contralateral axilla. Careful padding of pressure points (e.g., peroneal nerve at fibular head, ulnar nerve at elbow, bony prominences).
- Advantages: Allows full elbow flexion and extension. Good C-arm access.

-
Supine Position:
- Indication: Useful for anterior or anterolateral approaches to the humerus, especially for proximal or distal humeral fractures, and when an extensile approach from shoulder to elbow is required.
- Setup: Patient supine on the operating table. The arm can be placed on a hand table for anterior approaches or draped free for anterolateral approaches, allowing manipulation. Head in neutral position.
- Advantages: Easy access for anesthesia and resuscitation. More comfortable for longer cases.
-
Beach Chair Position:
- Indication: Primarily for proximal humeral fractures, allowing good visualization of the deltopectoral interval.
- Setup: Patient seated at approximately 45-60 degrees. Head supported, arm draped free.
- Advantages: Good for deltopectoral approach.
- Disadvantages: Risk of hypotension, careful head and neck positioning to prevent brachial plexus stretch.
Regardless of position, ensure adequate padding of all bony prominences, particular attention to the ulnar nerve at the elbow, peroneal nerve at the fibular head, and brachial plexus in the axilla.

Detailed Surgical Approach and Technique
Surgical approaches to the arm are tailored to the pathology and location, always prioritizing the identification and protection of neurovascular structures.
General Principles of Dissection
- Tourniquet Application: Typically applied high on the arm or at the root of the limb for a bloodless field.
- Layered Dissection: Meticulous identification of skin, subcutaneous tissue, superficial veins (cephalic, basilic), cutaneous nerves (medial/lateral cutaneous nerves of the arm/forearm).
- Internervous Planes: Utilize fascial planes to avoid muscle damage and minimize bleeding. These planes often lie between muscles supplied by different nerves or between different heads of the same muscle.
- Neurovascular Identification: Proactive identification and careful retraction of major nerves and vessels are paramount. Avoid excessive traction or compression. Use vessel loops for gentle retraction.
- Hemostasis: Maintain a dry field to optimize visualization.
Surgical Approaches to the Humerus
Anterior (Henry) Approach
- Indication: Proximal to distal third humeral fractures, exposure of the brachial artery, median and musculocutaneous nerves, especially for distal humeral shaft or supracondylar fractures.
- Incision: Longitudinal incision from the deltopectoral groove to the distal arm, along the medial border of the biceps.
- Internervous Plane:
- Proximal: Between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves). Deeper, between the deltoid and biceps (musculocutaneous nerve).
- Distal: Between the brachialis (musculocutaneous nerve) and brachioradialis (radial nerve), or directly through the brachialis.
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and ligate or retract the cephalic vein laterally and the medial cutaneous nerve of the forearm medially.
- In the proximal arm, enter the deltopectoral interval.
- Retract the biceps laterally. Identify the musculocutaneous nerve entering the coracobrachialis.
- Carefully identify the brachial artery and median nerve, which typically lie medial to the biceps. Retract these structures medially. The ulnar nerve lies even more medially, posterior to the medial intermuscular septum.
- Deep to the biceps, the brachialis muscle covers the humerus. Incise the brachialis longitudinally in its midline, or retract it.
- The humerus can then be exposed.

Anterolateral Approach
- Indication: Midshaft humeral fractures, especially for radial nerve exploration or plate fixation.
- Incision: Longitudinal incision along the lateral border of the biceps, extending distally towards the brachioradialis.
- Internervous Plane: Between the biceps (musculocutaneous nerve) and the triceps (radial nerve) or brachioradialis (radial nerve).
- Dissection:
- Incise skin and subcutaneous tissue. Identify and protect the cephalic vein (laterally) and the lateral cutaneous nerve of the forearm (terminal branch of musculocutaneous nerve).
- Identify the lateral border of the biceps and retract it medially.
- Deep to the biceps, expose the brachialis muscle. The radial nerve typically emerges from the posterior compartment by piercing the lateral intermuscular septum to lie between the brachialis and brachioradialis in the distal arm. Trace it proximally into the spiral groove if necessary.
- The humerus is exposed by splitting the brachialis or retracting it.

Posterior Approach (Direct Posterior or Triceps Sparing)
- Indication: Humeral shaft fractures (posterior plating), distal humeral fractures, extensive radial nerve exploration.
- Incision: Longitudinal incision directly over the posterior aspect of the arm, overlying the triceps.
- Internervous Plane: Between the long head (radial nerve) and lateral head (radial nerve) of the triceps.
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect the posterior cutaneous nerves of the arm and forearm.
- Expose the triceps muscle.
- Direct Posterior: Split the triceps longitudinally in the midline. The radial nerve typically lies deep to the lateral head, then posterior to the humerus in the spiral groove, and then between the medial and lateral heads distally. It is crucial to identify and protect the radial nerve and its accompanying profunda brachii artery.
- Triceps Sparing (Paratricipital): Develop the interval between the long and lateral heads of the triceps. The radial nerve is found emerging from deep to the lateral head to lie on the humerus.
- Olecranon Osteotomy: For optimal exposure of intra-articular distal humerus fractures, an olecranon osteotomy may be performed. The osteotomy is typically chevron-shaped and fixed with an intramedullary screw or tension band wiring.



Deltopectoral Approach
- Indication: Proximal humeral fractures, total shoulder arthroplasty.
- Incision: Longitudinal incision in the deltopectoral groove.
- Internervous Plane: Between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves).
- Dissection:
- Identify and ligate or retract the cephalic vein.
- Retract the deltoid laterally and the pectoralis major medially.
- Identify the clavipectoral fascia, which is incised to expose the conjoint tendon (coracobrachialis and short head of biceps), and the subscapularis.
- Carefully protect the axillary nerve, which runs circumferentially around the surgical neck of the humerus, approximately 5-7 cm distal to the acromion.


Fracture Reduction and Fixation
Once the humerus is exposed and neurovascular structures are protected, reduction and fixation proceed.
- Reduction: Achieved through direct manipulation, traction, or via fracture fragment clamps. Indirect reduction techniques (ligamentotaxis, plate as a reduction aid) minimize soft tissue stripping.
- Fixation:
- Plate and Screw Fixation: Most common for humeral shaft fractures. Plates can be applied anteriorly, anterolaterally, or posteriorly.
- Anterior Plating: Offers good mechanical stability. Requires meticulous retraction of neurovascular bundle.
- Anterolateral Plating: Often preferred for midshaft fractures, allowing identification and protection of the radial nerve. The plate can be applied over the nerve (with careful interposition) or deep to it.
- Posterior Plating: Excellent for posterior comminution, requiring identification of the radial nerve in the spiral groove.
- Intramedullary Nailing: Can be an option for certain diaphyseal fractures, either antegrade or retrograde. Potential risks include shoulder impingement (antegrade) or elbow pain (retrograde) and iatrogenic nerve injury during insertion or interlocking screw placement.
- External Fixation: Reserved for open fractures with significant contamination, severe soft tissue loss, or polytrauma.
- Plate and Screw Fixation: Most common for humeral shaft fractures. Plates can be applied anteriorly, anterolaterally, or posteriorly.
Throughout the fixation process, particular attention must be paid to the location of neurovascular structures. During screw placement, a safe zone must be respected. For example, during anterolateral plating, ensure the radial nerve is identified and retracted or protected before drilling. For posterior plating, the radial nerve is superficial to the plate.




Nerve Exploration and Repair
If a pre-existing nerve palsy does not resolve after reduction, or if a new nerve palsy develops, surgical exploration is often warranted. During exploration, the nerve is carefully identified, decompressed, and inspected for contusion, laceration, or entrapment within fracture fragments. Primary repair may be performed if the nerve is transected, or grafting considered for significant gaps.


Wound Closure
After achieving hemostasis and verifying stable fixation, the wound is closed in layers. Deep fascia is approximated, followed by subcutaneous tissue and skin. Drain placement may be considered in cases of extensive dissection or significant hematoma potential.
Complications and Management
Surgical interventions in the arm, while generally safe, carry inherent risks, particularly related to the density of neurovascular structures.


Common Complications
- Nerve Injury:
- Radial Nerve Palsy: Most frequent complication, especially with humeral shaft fractures (incidence up to 18% in some series). Can be due to contusion, traction, entrapment, or iatrogenic injury during dissection or drilling. Prognosis for spontaneous recovery is good for neurapraxia, but persistent deficit warrants exploration.
- Axillary Nerve Injury: Risk with proximal humeral approaches.
- Median/Ulnar Nerve Injury: Less common with humeral shaft fractures but significant risk with distal humeral or elbow region surgery.
- Musculocutaneous Nerve Injury: Possible during anterior approaches to the proximal arm.
- Vascular Injury:
- Brachial Artery Injury: Laceration, thrombosis, or pseudoaneurysm. Can lead to compartment syndrome or limb ischemia. Requires immediate vascular consultation and repair.
- Profunda Brachii Artery Injury: Less severe but can cause significant bleeding.
- Nonunion/Delayed Union: Failure of bone healing, more common in open fractures, comminuted fractures, or those with extensive soft tissue stripping. May require revision surgery with bone grafting.
- Malunion: Healing in an unacceptable alignment, potentially leading to functional deficit or cosmetic deformity. Corrective osteotomy may be indicated.
- Infection: Superficial or deep wound infection. Requires antibiotics, debridement, and potentially hardware removal in chronic cases.
- Hardware Failure: Plate breakage, screw pullout, or loosening. Often due to nonunion or inadequate fixation.
- Compartment Syndrome: Rare in the arm but a surgical emergency. Can result from significant trauma, vascular injury, or prolonged tourniquet time. Requires emergent fasciotomy.
- Heterotopic Ossification: Aberrant bone formation in soft tissues, particularly around the elbow. Can cause loss of motion. Prophylaxis with NSAIDs or radiation may be used.
- Stiffness: Especially of the elbow or shoulder, common after prolonged immobilization or complex intra-articular fractures.
| Complication | Incidence (Approx.) | Salvage/Management Strategy |
|---|---|---|
| Radial Nerve Palsy | 5-18% for humeral shaft fxs | Observation (3-6 mo) for neurapraxia, surgical exploration for entrapment/transection |
| Nonunion | 2-10% | Revision surgery, plate exchange, bone grafting (autograft/allograft), IM nailing |
| Malunion | Variable | Corrective osteotomy for symptomatic deformity or functional deficit |
| Infection (Deep) | 1-5% | Debridement, IV antibiotics, hardware removal (if chronic), vacuum-assisted closure |
| Vascular Injury | <1% (major vessel) | Immediate vascular repair (primary, graft), thrombectomy, fasciotomy for compartment syndrome |
| Axillary Nerve Injury | 1-5% (proximal humerus) | Observation, EMG monitoring, nerve exploration if no recovery after 3-6 months |
| Ulnar Nerve Palsy | <1% (humeral shaft), higher with distal humerus | Observation, nerve transposition for entrapment, surgical exploration for transection |
| Hardware Failure | 2-5% | Revision surgery, stronger fixation, address underlying nonunion |
| Compartment Syndrome | Rare | Emergent fasciotomy |
| Stiffness | Common (especially elbow/shoulder) | Aggressive physical therapy, dynamic/static splinting, manipulation under anesthesia, arthrolysis |
| Heterotopic Ossification | 10-20% (post-trauma elbow) | Prophylaxis (NSAIDs/radiation), surgical excision for severe symptomatic cases |
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for restoring function and preventing complications. Protocols are tailored to the specific injury, surgical technique, and patient factors.
Initial Phase (0-2 Weeks)
- Goals: Pain and edema control, protection of surgical repair, gentle range of motion (ROM) for adjacent joints, maintaining soft tissue mobility.
- Immobilization:
- Sling or cast/brace, depending on fracture stability and surgeon preference.
- For humeral shaft fractures, functional brace often applied after initial wound healing (e.g., 1-2 weeks).
- Exercises:
- Finger, wrist, and elbow (if not restricted by injury) active ROM.
- Pendulum exercises for the shoulder (if proximal humerus is stable).
- Ice, elevation, and gentle soft tissue massage for edema management.
- Nerve gliding exercises if nerve exploration/repair was performed.
- Weight Bearing: Non-weight bearing on the affected arm.
Intermediate Phase (2-6 Weeks)
- Goals: Gradual increase in active ROM, initiation of light strengthening, continue protecting healing structures.
- Immobilization: Progressive decrease in sling use, continue functional bracing as indicated.
- Exercises:
- Active-assisted and active ROM for shoulder and elbow as tolerated, respecting fracture stability.
- Gentle isometric strengthening for muscles not directly involved in the injury or fixation.
- Continue nerve gliding.
- Focus on scapular stabilization.
Advanced Phase (6+ Weeks)
- Goals: Progressive strengthening, return to functional activities, maximize range of motion and endurance.
- Exercises:
- Progressive resistive exercises for all muscle groups, gradually increasing load and intensity.
- Proprioceptive and balance exercises.
- Functional activities simulating daily tasks.
- Continue stretching and mobility exercises to address any residual stiffness.
- Return to Activity: Gradual return to light activities at 3-4 months, sports-specific training at 4-6 months, and contact sports at 6+ months, depending on radiographic healing and clinical recovery.
- Neurological Recovery: Ongoing assessment of nerve recovery. If no signs of recovery are observed within expected timelines, further investigation (EMG, NCS) or surgical re-exploration may be considered.
Specific Considerations
- Nerve Repair/Graft: Rehabilitation will be slower, with focus on protecting the repair site, gentle ROM, and monitoring for signs of reinnervation.
- Vascular Repair: Strict protection from excessive movement or compression initially.
- Distal Humeral Fractures: Early, controlled motion of the elbow is often crucial to prevent stiffness, but must balance with fracture stability.

Summary of Key Literature and Guidelines
The surgical management of arm pathologies, particularly humeral fractures, has evolved significantly, guided by clinical outcomes and anatomical insights. Current guidelines emphasize careful patient selection, meticulous surgical technique, and structured rehabilitation.
- Humeral Shaft Fractures: While historically treated non-operatively with functional bracing, surgical fixation is increasingly common for specific indications. Meta-analyses and randomized controlled trials have shown similar union rates between functional bracing and surgical fixation for closed, isolated humeral shaft fractures, but surgical fixation often results in faster return to function and lower rates of malunion. However, the risk of iatrogenic radial nerve palsy is higher with surgery. The decision between operative and non-operative management must be individualized, considering fracture pattern, patient comorbidities, and functional demands.
- Radial Nerve Palsy with Humeral Fractures: The consensus typically favors observation for radial nerve palsy associated with closed humeral shaft fractures, given the high rate (up to 90%) of spontaneous recovery, especially for neurapraxia. Exploration is indicated for open fractures, failure of nerve recovery after 3-6 months, or new/worsening palsy after closed reduction.
- Proximal Humeral Fractures: For complex, displaced fractures (Neer 3- and 4-part), surgical options include open reduction internal fixation (ORIF) with locking plates, intramedullary nails, reverse total shoulder arthroplasty (RTSA), or hemiarthroplasty. Literature supports RTSA for elderly patients with osteoporotic bone or rotator cuff compromise.
- Distal Humeral Fractures: Intra-articular distal humeral fractures almost universally require ORIF to restore articular congruence and achieve stable fixation for early motion. Dual plating (medial and lateral) is often preferred for optimal stability. The ulnar nerve is frequently transposed anteriorly during these approaches to protect it.
- Anatomical Studies: Ongoing anatomical studies continue to refine safe zones for plating and screw placement, especially concerning the radial nerve in the spiral groove and the axillary nerve at the surgical neck. These studies inform current best practices and help minimize iatrogenic injury.
Adherence to established principles of surgical anatomy, coupled with evidence-based decision-making and a thorough understanding of potential complications, ensures optimal outcomes for patients undergoing surgery of the arm. Continuous education and anatomical review remain cornerstones of orthopedic surgical excellence.
Clinical & Radiographic Imaging