Operative Management of Benign Osseous and Soft Tissue Lesions of the Hand

Key Takeaway
Benign osseous and soft tissue lesions of the hand, such as turret exostosis, calcinosis, and carpometacarpal bosses, frequently present with pain, mechanical impingement, or cosmetic deformity. Accurate diagnosis relies on clinical examination and targeted radiography. Management ranges from conservative therapies, including corticosteroid injections, to meticulous surgical excision. Operative intervention demands precise anatomical knowledge to protect adjacent neurovascular structures and extensor mechanisms, ensuring optimal functional recovery and minimizing recurrence rates.
Comprehensive Introduction and Patho-Epidemiology
The evaluation and management of benign osseous and soft tissue lesions of the hand and wrist require a meticulous, highly sophisticated understanding of complex regional anatomy, micro-biomechanics, and cellular pathology. While the nomenclature designates these lesions—ranging from reactive heterotopic bone formations to complex metabolic deposits—as non-malignant, their clinical behavior within the tightly constrained, unforgiving fascial compartments of the hand frequently leads to profound functional impairment. The hand is an organ of immense evolutionary specialization; even millimeter-scale space-occupying lesions can induce critical mechanical impingement on extensor mechanisms, severe compression of adjacent neurovascular bundles, and unrelenting inflammatory cascades. Consequently, the term "benign" must be interpreted strictly in an oncologic sense, as the structural morbidity inflicted by these entities can be devastating to manual dexterity and patient livelihood.
A turret exostosis represents a classic example of trauma-induced reactive pathology. Pathophysiologically, it is a smooth, dome-shaped, extracortical mass of mature lamellar bone that typically develops directly beneath the extensor apparatus on the dorsal aspect of the middle or proximal phalanx. The etiology is almost exclusively traumatic, stemming from a direct, blunt-force impact to the dorsum of the digit. This trauma shears the highly vascular periosteum, resulting in a localized subperiosteal hematoma. In a normal physiologic cascade, this hematoma would resorb; however, in turret exostosis, the hematoma undergoes fibrous organization and subsequent endochondral ossification, culminating in a rigid osseous prominence. Epidemiologically, this condition is most frequently observed in young, active adults, particularly manual laborers and contact sport athletes. It is imperative to clinically and radiographically differentiate a turret exostosis from an osteochondroma. Unlike an osteochondroma, a turret exostosis lacks a cartilaginous cap and does not exhibit cortical or medullary continuity with the underlying diaphysis of the phalanx.
In stark contrast to reactive osseous lesions, peripheral nerve hypertrophies present a formidable challenge of soft tissue infiltration. Conditions such as Déjérine-Sottas disease (a severe, early-onset hypertrophic demyelinating polyneuropathy) or lipofibromatous hamartoma (LFH) present with massive, fusiform, fibrofatty enlargement of major peripheral nerves, most notably the median nerve. The patho-epidemiology of LFH involves the anomalous proliferation of mature adipocytes and fibrous tissue within the epineurium and perineurium, progressively strangling the functional axonal fascicles. This condition frequently manifests in the first three decades of life and is highly associated with macrodactyly (nerve-territory overgrowth) in approximately one-third of cases. The profound enlargement transforms the nerve itself into a space-occupying lesion, precipitating severe compressive neuropathies within anatomic bottlenecks such as the carpal tunnel.
Furthermore, reactive calcinosis and the carpometacarpal (CMC) boss represent distinct pathophysiologic entities driven by metabolic deposition and degenerative micro-trauma, respectively. The exact etiology of reactive calcium deposits in the hand remains incompletely elucidated, though prevailing theories suggest that localized connective tissue degeneration—often precipitated by chronic microtrauma—lowers the local tissue pH, creating a biochemical nidus for secondary amorphous calcium carbonate and calcium phosphate deposition. Conversely, the CMC boss (carpe bossu) is a fixed, benign dorsal osteophyte protuberance located at the mating surfaces of the quadrangular CMC joints (typically the second and third metacarpal bases articulating with the trapezoid and capitate). Driven by repetitive mechanical stress, ligamentous laxity, and localized osteoarthritis, this osteophytic overgrowth creates mechanical conflict with the overlying extensor carpi radialis longus (ECRL) and brevis (ECRB) tendons, demanding precise surgical intervention when conservative measures fail.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of hand and wrist anatomy is the cornerstone of safe and effective surgical intervention for benign lesions. The dorsal apparatus of the digits, intimately involved in the pathology of turret exostosis, is an intricate confluence of tendinous and ligamentous structures. The extensor mechanism over the proximal phalanx consists of the central slip, the lateral bands, and the transverse retinacular ligaments. Beneath this apparatus lies a delicate, highly specialized gliding layer composed of dorsal periosteum and paratenon. A turret exostosis disrupts this biomechanical harmony by acting as a physical fulcrum, forcing the extensor hood to stretch abnormally over the bony dome during active flexion. This increases the tension within the extensor mechanism, leading to localized pain, premature fatigue of the lumbricals and interossei, and a measurable extension lag due to the mechanical disadvantage and attenuation of the central slip.
The anatomy of the carpal tunnel and the microarchitecture of the median nerve are critically relevant when addressing peripheral nerve hypertrophies such as lipofibromatous hamartoma. The carpal tunnel is a rigid fibro-osseous canal bounded dorsally by the carpal arch and volarly by the thick, unyielding transverse carpal ligament (TCL). The normal median nerve occupies approximately 20% of the cross-sectional area of this tunnel. In the presence of hypertrophic fibrofatty infiltration, the nerve's cross-sectional area can increase exponentially, occupying the entire available space and compressing adjacent digital flexor tendons. The intrinsic microvascular anatomy of the nerve—comprising the vasa nervorum within the epineurium and perineurium—is highly susceptible to increased interstitial pressure. When the pressure within the carpal tunnel exceeds capillary perfusion pressure (typically around 30-40 mmHg), profound intraneural ischemia ensues, leading to the catastrophic demyelination and axonal loss characteristic of advanced compressive neuropathy.
In the context of calcinosis, the flexor and extensor compartments of the wrist present specific anatomic vulnerabilities. The flexor carpi ulnaris (FCU) insertion into the proximal pole of the pisiform is the most frequent anatomical site for reactive calcium deposition in the upper extremity. The pisiform acts as a sesamoid bone, augmenting the mechanical advantage of the FCU. Calcium deposits in this region infiltrate the peritendinous tissues and the pisohamate ligament, inciting an intense, highly localized inflammatory cascade. The resulting edema and erythema can easily mimic acute suppurative tenosynovitis. The fascial constraints of Guyon's canal lie immediately adjacent to this insertion; thus, severe inflammatory swelling from FCU calcinosis can precipitate acute ulnar nerve compression, necessitating urgent decompression.
The quadrangular articulation of the carpometacarpal joints is a biomechanical keystone of the longitudinal and transverse carpal arches. The second and third CMC joints are inherently rigid, designed to provide a stable central pillar for forceful prehension. The ECRL inserts onto the dorsal base of the second metacarpal, while the ECRB inserts onto the dorsal base of the third metacarpal. A CMC boss develops precisely at this dorsal articular junction. Biomechanically, the presence of this osteophyte alters the moment arm of the radial wrist extensors. During active wrist extension, the ECRL and ECRB tendons are forced to bowstring or subluxate over the bony prominence, generating sheer forces that result in chronic tenosynovitis, adventitial bursitis, and, in severe cases, attritional tendon rupture. Understanding this precise biomechanical conflict is essential for determining the extent of surgical resection required to restore normal tendon kinematics.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for benign osseous and soft tissue lesions of the hand must be predicated on a rigorous evaluation of clinical symptoms, functional deficits, and the failure of exhaustive non-operative management. For turret exostosis, absolute indications for surgical excision include a progressive mechanical block to active digital flexion, persistent and debilitating pain that precludes normal occupational or recreational activities, and radiographic evidence of impending extensor tendon attrition over the osseous dome. Relative indications encompass cosmetic deformity in highly sensitive patients or diagnostic uncertainty where an aggressive parosteal osteosarcoma cannot be definitively ruled out via advanced imaging. Conversely, absolute contraindications include asymptomatic lesions discovered incidentally, active local soft tissue infection (e.g., cellulitis or paronychia), or profound medical comorbidities that render elective anesthesia unacceptably hazardous.
When evaluating massive peripheral nerve hypertrophies (e.g., lipofibromatous hamartoma), the surgical indications pivot sharply from excision to decompression. An absolute indication for surgical intervention is the presence of progressive motor weakness (e.g., thenar atrophy), unrelenting nocturnal pain, or advanced sensory deficits in the median nerve distribution that correlate with severe carpal tunnel compression. The primary objective is the release of the transverse carpal ligament to restore intraneural microvascular perfusion. Absolute contraindications in this scenario include any attempt at en bloc resection of the hypertrophic nerve, as this will result in catastrophic, irreversible loss of motor and sensory function to the radial three-and-a-half digits. Biopsy of the nerve is generally considered a relative contraindication unless malignancy is highly suspected; if performed, it must be strictly limited to the superficial epineurium under high-power microscopic magnification to avoid iatrogenic fascicular transection.
Surgical management of reactive calcinosis is strictly reserved for recalcitrant cases. The vast majority of these deposits are self-limiting, undergoing spontaneous rupture and macrophage-mediated resorption. However, surgical extirpation is absolutely indicated when a large, chronic deposit causes a persistent mechanical block, intractable pain refractory to corticosteroid injections, or threatens to erode through the overlying dermis, creating a chronic draining sinus. It is vital to differentiate isolated reactive calcinosis from systemic Calcinosis Circumscripta (associated with scleroderma or CREST syndrome). In systemic cases, surgical intervention is fraught with high complication rates, including catastrophic wound breakdown and aggressive recurrence; thus, systemic medical management remains the primary modality, rendering surgery a relative contraindication unless massive ulceration is present.
| Pathology / Lesion | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Turret Exostosis | Mechanical block to flexion, extensor tendon attrition, intractable pain, diagnostic uncertainty. | Active local infection, asymptomatic incidental findings. | Poor patient compliance with postoperative early AROM protocols. |
| Peripheral Nerve Hypertrophy (LFH) | Progressive motor/sensory deficit, severe carpal tunnel syndrome, intractable neuropathic pain (Decompression only). | En bloc resection of the nerve, asymptomatic presentation. | Epineurial biopsy (unless malignancy is highly suspected). |
| Reactive Calcinosis | Impending skin necrosis, chronic mechanical block, failure of prolonged conservative management. | Acute inflammatory phase (toothpaste stage) responsive to aspiration/injection. | Systemic Calcinosis Circumscripta (CREST syndrome) without ulceration. |
| Carpometacarpal (CMC) Boss | Refractory pain, severe tendon snapping/subluxation, failure of splinting and injections. | Painless cosmetic bump, active wrist joint infection. | Advanced, widespread radiocarpal osteoarthritis (requires more extensive fusion). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is non-negotiable for achieving optimal surgical outcomes in the tight confines of the hand. Advanced imaging modalities serve as the foundation of this preparation. For a suspected CMC boss, standard posteroanterior and lateral radiographs are frequently inadequate due to the complex bony overlap of the carpus. A specific tangential radiograph—the carpal boss view, obtained with the wrist in 30 degrees of supination and slight ulnar deviation—is absolutely required to profile the dorsal osteophyte accurately. This view allows the surgeon to template the exact volume of bone requiring resection. In cases of peripheral nerve hypertrophy, high-resolution Magnetic Resonance Imaging (MRI) without contrast is the gold standard. MRI of lipofibromatous hamartoma pathognomonically demonstrates the "coaxial cable" sign on axial T1-weighted images, characterized by enlarged, low-signal nerve fascicles interspersed within high-signal hyperplastic fibrofatty epineurial tissue. This finding confirms the diagnosis pre-operatively and prevents disastrous intraoperative attempts at mass excision.
Patient positioning and operating room setup must be standardized to ensure a bloodless, ergonomically optimized surgical field. The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Following standard sterile prep and drape, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 250 mmHg (or 100 mmHg above the patient's systolic blood pressure). A bloodless field is absolutely critical; even minor capillary bleeding can obscure the delicate epineurial vessels or the translucent paratenon, drastically increasing the risk of iatrogenic injury. The use of high-quality surgical loupe magnification (minimum 3.5x to 4.5x) and a dedicated fiber-optic headlight is mandatory for all procedures detailed in this chapter.
Anesthesia selection plays a pivotal role in the surgical strategy. While regional anesthesia (e.g., supraclavicular or axillary brachial plexus blocks) provides excellent intraoperative conditions and prolonged postoperative analgesia, the WALANT (Wide Awake Local Anesthesia No Tourniquet) technique is gaining significant traction for specific lesions. Using a mixture of 1% lidocaine and 1:100,000 epinephrine, WALANT allows the surgeon to dynamically assess tendon gliding and mechanical impingement intraoperatively. For instance, during the excision of a CMC boss, the awake patient can actively extend their wrist, allowing the surgeon to visualize in real-time whether the ECRL and ECRB tendons are still snapping over the resection bed, thereby confirming the adequacy of the osteophyte removal before closure.
Equipment preparation must anticipate the need for both delicate soft tissue handling and aggressive osseous resection. The surgical tray should include fine micro-instruments (e.g., tenotomy scissors, micro-forceps, Freer elevators), a variety of sharp micro-osteotomes, and a high-speed pneumatic burr with continuous saline irrigation. For revision cases of CMC boss requiring arthrodesis, the surgeon must ensure the availability of low-profile dorsal spanning plates, headless compression screws, and Kirschner wires (K-wires), alongside fluoroscopic C-arm imaging to confirm hardware placement and joint reduction.
Step-by-Step Surgical Approach and Fixation Technique
Turret Exostosis Excision
The surgical excision of a turret exostosis requires precise soft tissue handling to prevent postoperative extensor lag.
1. Incision: A midlateral incision is strictly utilized along the affected phalanx. A direct dorsal incision is contraindicated as it places the surgical scar directly over the extensor tendon, significantly increasing the risk of restrictive postoperative adhesions.
2. Exposure: The skin and delicate subcutaneous tissues are elevated as a full-thickness flap. The extensor apparatus is identified and gently retracted dorsally and contralaterally using fine Ragnell or Senn retractors to expose the underlying bony mass.
3. Periosteal Dissection: The dorsal periosteum is incised laterally along the border of the exostosis. Using a sharp Freer elevator, the periosteum is meticulously elevated from the underlying abnormal bone. Surgical Warning: Extreme care must be taken not to shred this periosteal sleeve. Preserving a smooth, continuous periosteal surface is critical for providing a frictionless gliding layer for the extensor apparatus postoperatively.
4. Resection: Using a sharp micro-osteotome or a fine rongeur, the dome-shaped exostosis is resected flush with the normal diaphyseal cortex of the phalanx. A high-speed burr can be used to smooth the residual cortical bed.
5. Closure: The periosteal sleeve is meticulously closed over the raw cancellous bone defect using fine 5-0 or 6-0 absorbable sutures (e.g., Vicryl). The extensor mechanism is allowed to fall back into its anatomic position, and the skin is closed with non-absorbable monofilament sutures.
Peripheral Nerve Hypertrophy Decompression
When encountering massive fibrofatty hypertrophy of the median nerve (e.g., Lipofibromatous Hamartoma), the surgical strategy is purely decompressive.
- Incision: A standard or slightly extended longitudinal palmar incision is made in line with the radial border of the ring finger, extending proximally across the wrist crease in a zig-zag fashion to prevent scar contracture.
- Exposure and Release: The palmar fascia is divided, and the transverse carpal ligament (TCL) is identified. The TCL is completely divided from its proximal edge at the antebrachial fascia to its distal extent at the superficial palmar arch.
- Nerve Inspection: The massively enlarged median nerve is inspected. The loss of normal fascicular architecture due to fibrofatty infiltration will be immediately apparent.
- Biopsy (If Mandated): If a biopsy is absolutely necessary to rule out malignant peripheral nerve sheath tumors, it is performed under 4.5x loupe or operative microscope magnification. A microscopic sliver of the superficial epineurium is sharply excised, strictly avoiding any functional axonal fascicles.
- Closure: Only the skin is closed. The TCL is left open to maximize spatial volume for the hypertrophic nerve.
Reactive Calcinosis Extirpation
Surgical intervention for reactive calcinosis focuses on complete removal of the inflammatory nidus without damaging adjacent structures.
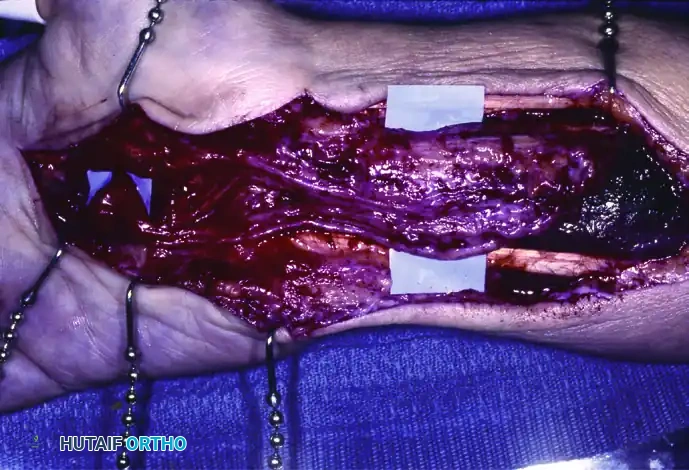
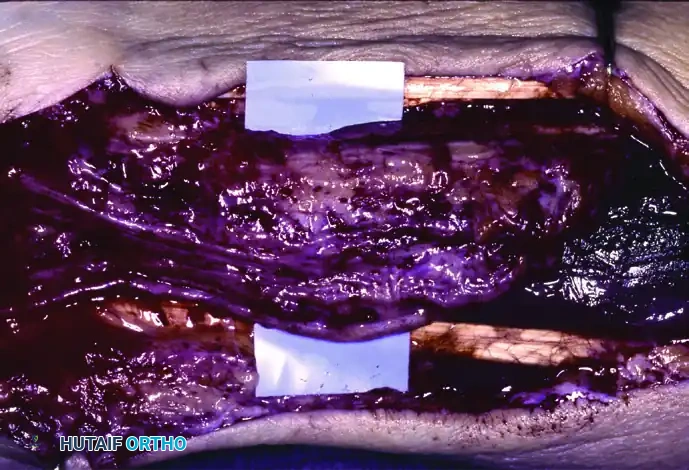
- Approach: For the most common site (FCU insertion), a longitudinal incision is made over the volar-ulnar aspect of the distal forearm, extending to the pisiform.
- Dissection: The ulnar neurovascular bundle, located immediately radial to the FCU, is identified and protected with vessel loops. The FCU tendon sheath is incised.
- Extirpation: The calcium deposit may present as a chalky, hard mass or a thick, toothpaste-like exudate. The material is meticulously curetted from the tendon substance and surrounding ligaments.
- Irrigation: The surgical bed is subjected to copious, high-volume saline irrigation to wash out any microscopic calcium crystals, which could otherwise precipitate a recurrent inflammatory cascade.
- Repair: Any significant iatrogenic defects in the FCU tendon are repaired with a running interlocking suture (e.g., 3-0 Prolene).
CMC Boss Excision and Arthrodesis
- Incision: A transverse incision in the skin creases over the dorsal prominence provides excellent cosmesis, though a longitudinal incision offers superior extensibility if arthrodesis is anticipated.
- Tendon Protection: The dorsal sensory branches of the radial nerve are identified and protected. The extensor retinaculum is incised longitudinally. The ECRL and ECRB tendons are mobilized and retracted radially or ulnarly. Surgical Warning: Meticulous care must be taken to protect the insertions of these tendons into the metacarpal bases to prevent devastating wrist extension weakness.
- Resection: The dorsal capsule is incised, exposing the osteophyte. Using a sharp osteotome or high-speed burr, the boss is resected flush with the normal dorsal cortex. The joint space is inspected for a concomitant ganglion stalk, which must be excised.
- Arthrodesis (For Recurrence): If this is a recurrent boss, simple excision is contraindicated. The CMC joint must be fused. The articular cartilage of the affected CMC joint is completely denuded down to bleeding subchondral bone using a high-speed burr. Cancellous bone graft (often harvested from the distal radius) is packed into the joint space. The joint is then rigidly fixed using a low-profile dorsal spanning titanium plate or crossed 0.045-inch K-wires.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for benign hand lesions, while often curative, carries a distinct profile of severe complications. The tight anatomic constraints mean that even minor postoperative edema or scarring can result in profound stiffness. Following the excision of a turret exostosis, the most common complication is the development of dense extensor tendon adhesions to the underlying bony resection bed. This occurs if the dorsal periosteum was inadequately repaired or iatrogenically destroyed during the approach. Patients present with a severe active extension lag and loss of passive flexion. Salvage management requires an aggressive secondary tenolysis, often coupled with the interposition of a synthetic gliding matrix or an adipofascial flap to recreate the lost periosteal barrier.
In the management of peripheral nerve hypertrophies, the most catastrophic complication is iatrogenic nerve injury during attempted biopsy or misguided excision. Transection of functional fascicles within a lipofibromatous hamartoma results in irreversible thenar paralysis and profound sensory loss. Because the nerve architecture is completely distorted by fibrofatty infiltration, primary end-to-end repair is impossible. Salvage management in these devastating scenarios relies on complex peripheral nerve transfers (e.g., transferring a branch of the anterior interosseous nerve to the recurrent motor branch of the median nerve) or tendon transfers (e.g., extensor indicis proprius to abductor pollicis brevis for opposition restoration).
Recurrence is the hallmark complication of CMC boss excision, with literature reporting recurrence rates as high as 15-20% following simple osteophyte resection. This is primarily driven by the failure to address the underlying micromotion and degenerative changes at the quadrangular articulation. When a patient presents with a painful, recurrent dorsal prominence, repeat simple excision is universally condemned due to the high risk of joint destabilization and subsequent failure. The definitive salvage strategy is a formal carpometacarpal joint arthrodesis, which completely eliminates the mechanical friction driving the osteophyte formation.
| Complication | Estimated Incidence | Primary Etiology | Salvage Strategy / Management |
|---|---|---|---|
| Extensor Tendon Adhesions (Turret Exostosis) | 10 - 15% | Failure to preserve/repair dorsal periosteum; delayed mobilization. | Aggressive hand therapy; secondary surgical tenolysis with adipofascial flap interposition. |
| Iatrogenic Nerve Injury (Nerve Hypertrophy) | < 2% (if decompression only) | Misguided attempt at mass excision or overly aggressive biopsy. | Nerve transfers (AIN to recurrent motor branch) or tendon transfers for opposition. |
| Recurrence of Osteophyte (CMC Boss) | 15 - 20% | Incomplete resection; failure to address underlying CMC micromotion. | Formal CMC joint arthrodesis (fusion) with bone grafting and rigid internal fixation. |
| Wound Breakdown / Fistula (Calcinosis) | 5 - 10% | Operating on systemic Calcinosis Circumscripta; inadequate tissue envelope. | Aggressive local wound care; delayed closure with local rotational flaps; systemic medical control. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be precisely tailored to the specific pathology addressed, balancing the competing demands of tissue healing and the prevention of restrictive adhesions. For soft tissue and reactive osseous excisions (e.g., Turret exostosis, simple CMC boss excision, or calcinosis removal), the rehabilitation is divided into three distinct phases.
Phase 1: Protection and Healing (Days 0-5)
Immediately postoperatively, the hand is immobilized in a bulky, non-compressive soft dressing augmented with a custom-molded orthoplast splint. For a turret exostosis, a dorsal blocking splint is utilized to keep the digit in slight extension, removing tension from the extensor apparatus while the periosteal repair solidifies. For a CMC boss, the wrist is splinted in 15-20 degrees of extension. Strict elevation above heart level is mandated to minimize interstitial edema, which is the primary precursor to fibrotic scarring.
Phase 2: Early Active Motion (Days 5-21)
Prolonged immobilization is the enemy of hand surgery. By postoperative day 5, the bulky surgical dressings are removed, and the patient is transitioned to a removable splint under the strict guidance of a certified hand therapist. Early Active Range of Motion (AROM) is initiated. For turret exostosis patients, isolated joint blocking exercises are employed to force the lateral bands and central slip to glide over the resection site, mechanically disrupting nascent cross-linked collagen adhesions. Passive range of motion (PROM) is generally avoided during this phase to prevent stretching or rupturing delicate capsular repairs.
Phase 3: Strengthening and Normalization (Weeks 3-8)
As the soft tissues achieve tensile strength, the rehabilitation protocol shifts toward dynamic strengthening and functional restoration. Splinting is gradually discontinued during the day. Modalities such as ultrasound therapy, fluidotherapy, and aggressive scar massage with silicone elastomer pads are utilized to soften the surgical incision and desensitize the area. Work conditioning programs are initiated for manual laborers to ensure a safe return to heavy occupational demands.
Arthrodesis-Specific Protocol:
In stark contrast, if a CMC joint arthrodesis was performed for a recurrent carpal boss, the rehabilitation timeline is significantly protracted. The wrist must remain rigidly immobilized in a short-arm cast or a rigid custom orthosis for a minimum of 6 to 8 weeks. Absolutely no active or passive wrist motion is permitted until definitive, bridging trabecular bone across the arthrodesis site is confirmed via serial radiographs or computed tomography (CT). Premature mobilization will inevitably lead to hardware failure, non-union, and chronic pain. Once radiographic union is achieved, a progressive weaning from the splint begins, followed by aggressive therapy to regain radiocarpal and midcarpal kinematics.
Summary of Landmark Literature and Clinical Guidelines
The operative management of benign hand lesions is heavily informed by decades of evolving orthopedic literature and established clinical guidelines. The definitive understanding of Turret exostosis was significantly advanced by Wissinger et al., who first comprehensively detailed the pathophysiology of subperiosteal hematoma ossification beneath the extensor apparatus. Their landmark work established the absolute necessity of a midlateral surgical approach and meticulous periosteal preservation, protocols that remain the gold standard in contemporary hand surgery board examinations (AAOS, FRCS).
Regarding peripheral nerve hypertrophies, the paradigm shift from attempted excision to strict decompression was solidified by the extensive clinical reviews from the Mayo Clinic (Amadio et al.). Their long-term outcome studies on lipofibromatous hamartoma definitively demonstrated that any attempt at intraneural dissection or mass extirpation universally resulted in catastrophic functional morbidity. Current clinical guidelines universally mandate that management be restricted to carpal tunnel release, with or without prophylactic epineurotomy, emphasizing that the preservation of neurological function vastly supersedes the desire to remove the benign mass.
The surgical algorithm for the carpometacarpal boss has been refined through rigorous comparative studies. Fusi et al. provided critical outcome data demonstrating the unacceptably high recurrence rates associated with simple excision in the presence of underlying degenerative CMC joint disease. Based on this literature, current clinical guidelines strongly recommend a detailed preoperative assessment of joint stability and arthritic changes.
