Operative Management of Hand Soft Tissue Tumors: Hemangioma and Glomus Tumor
Key Takeaway
Cavernous hemangiomas and glomus tumors represent distinct soft tissue pathologies in the hand requiring precise surgical management. While hemangiomas present as soft, collapsible masses with distended venous sinuses, glomus tumors are characterized by the classic triad of pain, cold sensitivity, and point tenderness. This guide details the pathophysiology, diagnostic criteria, and step-by-step surgical techniques for marginal and complete excision of these complex vascular and neuromyoarterial lesions.
Comprehensive Introduction and Patho-Epidemiology
Soft tissue tumors of the hand and upper extremity encompass a highly diverse array of neoplastic, hamartomatous, and non-neoplastic reactive lesions. Because of the exquisitely dense and complex anatomy of the hand—where critical neurovascular, tendinous, and osseous structures are confined within tight fascial compartments—even histologically benign lesions can precipitate profound functional impairment, sensory deficits, and debilitating pain. Among the most clinically significant and surgically challenging of these are vascular malformations (specifically cavernous hemangiomas) and neuromyoarterial lesions, such as the glomus tumor. Furthermore, solid encapsulated masses like giant cell tumors of the tendon sheath (GCTTS) and digital fibromas represent a massive proportion of the daily surgical volume for the practicing hand surgeon.
The epidemiological distribution of these tumors is uniquely skewed compared to the rest of the appendicular skeleton. The hand is the epicenter for glomus tumors, harboring approximately 75% of all such lesions found in the human body. These rare, benign hamartomas arise from the neuromyoarterial glomus body and present with a classic triad of symptoms that often elude initial diagnosis, leading to protracted patient suffering. Conversely, cavernous hemangiomas represent complex vascular malformations composed of dilated, endothelium-lined venous sinuses. It is imperative to distinguish the cavernous hemangioma from the capillary superficial infantile hemangioma (the so-called "strawberry hemangioma"). The infantile capillary variant is driven by endothelial proliferation, typically undergoes rapid postnatal growth, and spontaneously involutes by age seven, rarely necessitating surgical intervention. In stark contrast, cavernous hemangiomas do not involute; they infiltrate local subcutaneous fat, interosseous musculature, and occasionally erode into adjacent cortical bone, rendering complete surgical extirpation exceptionally difficult.
Giant cell tumors of the tendon sheath (GCTTS) represent the second most common benign soft tissue tumor of the hand, superseded only by the ubiquitous ganglion cyst. Patho-epidemiologically, GCTTS is considered a localized form of pigmented villonodular synovitis (PVNS), driven by a reactive, non-neoplastic proliferation of mononuclear cells, heavily laden with hemosiderin and accompanied by multinucleated giant cells and lipid-filled foam cells. Recent cytogenetic analyses have identified translocations involving the colony-stimulating factor 1 (CSF1) gene on chromosome 1p13 in a subset of these tumors, suggesting a clonal neoplastic etiology in certain variants. Meanwhile, digital fibromas, though less common, present as slow-growing, well-encapsulated masses that cause insidious pulp enlargement and secondary mass-effect neuropathy on the terminal arborizations of the digital nerves.
While discussing the patho-epidemiology of soft tissue tumors, the orthopedic surgeon must remain vigilant regarding the risk of malignant transformation, particularly in specific syndromic populations. In patients afflicted with Neurofibromatosis Type 1 (von Recklinghausen disease), plexiform neurofibromas carry a documented 8% to 15% lifetime risk of malignant transformation into Malignant Peripheral Nerve Sheath Tumors (MPNST). This high-grade sarcoma demands immediate, aggressive multidisciplinary oncologic management. Any neurofibromatous lesion that exhibits sudden logarithmic growth, becomes painful at rest, or precipitates new-onset focal neurologic deficits must be treated with high clinical suspicion, mandating wide oncologic excision rather than marginal enucleation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the microanatomy of the hand is the absolute prerequisite for the safe extirpation of these intricate soft tissue tumors. The glomus tumor, for instance, is inextricably linked to the anatomy of the normal glomus body. The glomus body is a specialized, highly organized neuromyoarterial receptor situated primarily in the reticular layer of the dermis, with a striking concentration in the subungual regions of the digits, the volar pads, and the palm. Physiologically, it functions as an arteriovenous dermal shunt, playing a critical role in thermoregulation and localized blood pressure modulation.
Microscopically, the normal glomus body consists of an afferent arteriole, an anastomotic vessel known as the Sucquet-Hoyer canal, an efferent venule, an intraglomerular retinaculum, and a surrounding capsule. The Sucquet-Hoyer canal is lined by specialized endothelial cells and surrounded by layers of cuboidal glomus cells. These glomus cells are modified smooth muscle cells rich in actin filaments. Hyperplasia of these cellular components yields the glomus tumor. Histologically, the tumor is heavily innervated by nonmyelinated sympathetic nerve fibers that are densely intermixed with thick-walled capillaries. It is the contraction of these modified smooth muscle cells around the engorged vascular channels, combined with the dense sympathetic innervation, that generates the severe, lancinating, paroxysmal pain characteristic of the lesion, particularly when exposed to thermal or mechanical stimuli.
The surgical anatomy of the nail bed is equally critical when addressing subungual glomus tumors. The perionychium consists of the nail bed (sterile matrix) and the nail fold (germinal matrix). The germinal matrix, located proximal to the lunula, is responsible for 90% of nail plate production. The sterile matrix extends distally from the lunula to the hyponychium and provides adherence for the growing nail plate. Subungual glomus tumors are predominantly located beneath the sterile matrix. Surgical access requires precise elevation of the nail plate and a longitudinal incision through the sterile matrix. Transverse incisions or traumatic handling of the germinal matrix will invariably result in irreversible nail dystrophy, ridging, or a split nail deformity, which can be as cosmetically and functionally distressing to the patient as the original tumor.
In the context of cavernous hemangiomas and giant cell tumors of the tendon sheath, the anatomy of the flexor tendon sheath and the digital neurovascular bundles dictates the surgical approach. Cavernous hemangiomas frequently lack a true capsule, instead presenting as a diffuse labyrinth of distended venous sinuses that interdigitate with the neurovascular bundles, the lumbrical muscles, and the flexor pulleys. Attempting to dissect these lesions requires meticulous microvascular technique to avoid catastrophic devascularization of the digit. GCTTS, conversely, is typically well-encapsulated but originates directly from the synovial lining of the tendon sheath or adjacent interphalangeal joints. These tumors frequently wrap circumferentially around the flexor tendons, occasionally extending dorsally past the neurovascular bundles (the "collar-button" extension). The surgeon must navigate the Cleland and Grayson ligaments to safely mobilize the neurovascular bundles, ensuring complete marginal excision of the tumor without inducing iatrogenic nerve injury or compromising the critical annular pulleys (A2 and A4) required for flexor tendon biomechanics.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for hand soft tissue tumors requires a meticulous risk-benefit analysis, balancing the severity of the patient's symptoms against the inherent risks of iatrogenic neurovascular injury, postoperative contracture, and tumor recurrence. Conservative management is often the initial strategy for diffuse, asymptomatic, or mildly symptomatic cavernous hemangiomas. Custom-fitted compression garments, such as Isotoner gloves or custom Coban wrapping, can effectively collapse the venous sinuses, reduce hydrostatic engorgement, and alleviate aching pain. However, when these lesions produce severe pain, functional limitation, or significant cosmetic deformity, surgical excision becomes indicated.
A critical, life-threatening contraindication to immediate surgical intervention in large cavernous hemangiomas is the presence of Kasabach-Merritt Syndrome. Typically associated with lesions larger than 5 cm, this syndrome is a profound consumptive coagulopathy driven by secondary platelet sequestration within the tumor's extensive vascular labyrinth. The localized intravascular coagulation depletes systemic clotting factors, leading to profound thrombocytopenia and a paradoxical systemic bleeding diathesis. Any surgical incision in a patient with unoptimized Kasabach-Merritt Syndrome can result in fatal hemorrhage. Early, aggressive multidisciplinary treatment with hematology—utilizing systemic corticosteroids, vincristine, interferon-alpha, or localized embolization—is strictly indicated to normalize coagulation parameters prior to any surgical consideration.
For glomus tumors, surgical excision is almost universally indicated upon diagnosis, given the profound morbidity associated with the lesion. The diagnosis is heavily reliant on the classic clinical triad: paroxysmal lancinating pain, severe cold hypersensitivity, and exquisite point tenderness. These symptoms are validated through provocative testing. The Love test involves applying direct pressure to the tumor with a small, firm object (like a pinhead); pain is sharply localized, and moving the pin even a millimeter away elicits no response. The Ice Water test involves immersing the digit in cold water, which reproducibly triggers severe discomfort. Finally, the Hildreth test is pathognomonic: inflation of a proximal tourniquet to exsanguinate the limb relieves the pain of the Love test, and release of the tourniquet causes the pain to immediately return. When this triad is present, operative enucleation is indicated to restore patient quality of life.
| Clinical Condition | Primary Indications for Surgery | Absolute/Relative Contraindications |
|---|---|---|
| Cavernous Hemangioma | Severe pain, functional impairment, progressive compartment enlargement, failure of compression therapy. | Unoptimized Kasabach-Merritt Syndrome (Absolute), asymptomatic diffuse lesions where excision would sacrifice critical nerves (Relative). |
| Glomus Tumor | Presence of classic diagnostic triad (pain, cold sensitivity, point tenderness), positive Love/Hildreth tests, visible subungual deformity. | Active paronychia or local skin infection over the operative site (Relative - delay until resolved). |
| GCTTS | Progressive enlargement, mechanical block to digit flexion/extension, secondary cortical bone erosion. | None absolute; relative contraindications include severe medical comorbidities precluding anesthesia. |
| Digital Fibroma | Secondary sensory nerve compromise (mass effect), progressive pulp enlargement causing functional deficit. | Asymptomatic, non-growing lesions in high-risk surgical candidates (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning and advanced imaging are the cornerstones of successful soft tissue tumor extirpation in the hand. While the diagnosis of GCTTS or a digital fibroma can often be made clinically, imaging is essential for delineating the extent of vascular malformations and localizing occult glomus tumors. Standard plain radiographs should always be the initial imaging modality. In the case of cavernous hemangiomas, the presence of calcifications, known as phleboliths, is a hallmark diagnostic sign. These represent calcified thrombi within the stagnant venous sinuses of the lesion. For GCTTS and glomus tumors, radiographs may reveal extrinsic cortical scalloping or focal cystic erosions of the underlying phalanx due to chronic pressure from the adjacent mass.
When a glomus tumor is clinically suspected based on the classic triad but remains invisible to the naked eye (as occurs in the 25% of cases located in the digital pulp or palm rather than the subungual space), High-Resolution Magnetic Resonance Imaging (MRI) is the gold standard. Utilizing a dedicated hand coil and gadolinium contrast, the glomus tumor typically appears as a well-demarcated, highly vascular mass demonstrating low signal intensity on T1-weighted images and bright, high signal intensity on T2-weighted and STIR sequences. Following gadolinium administration, the lesion exhibits intense, rapid enhancement. MRI is equally critical for cavernous hemangiomas to map the full three-dimensional extent of the venous sinuses, their infiltration into adjacent muscle bellies, and their proximity to major neurovascular bundles, allowing the surgeon to plan potential staged excisions or preoperative embolization.

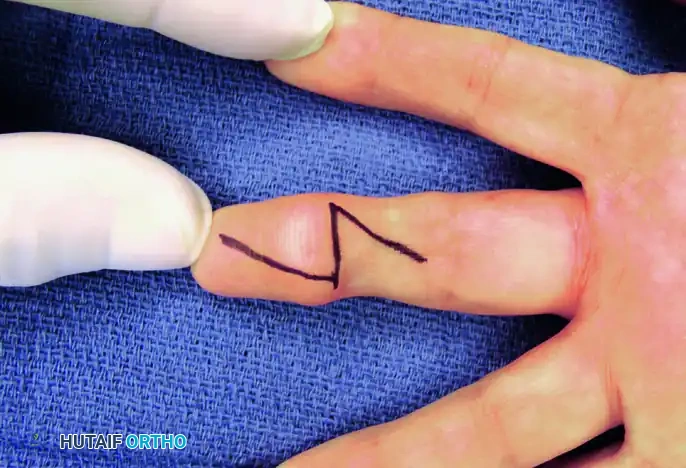
Figure: Preoperative marking of the Brunner zigzag incision designed to expose the flexor surface mass while preventing flexion contractures.
Patient positioning and anesthetic management must be meticulously tailored to the specific tumor type. The patient is placed supine with the operative extremity extended on a radiolucent hand table. Regional anesthesia, specifically an axillary or supraclavicular brachial plexus block, is highly preferred over general anesthesia. The regional block provides excellent intraoperative muscle relaxation, profound postoperative pain control, and, crucially, a sympathectomy effect that induces profound vasodilation. This vasodilation improves distal perfusion and aids in the identification of ischemic boundaries during complex resections.
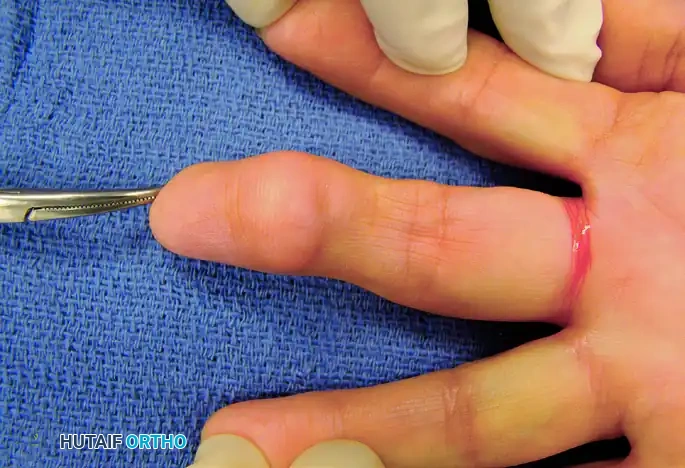
Figure: Clinical presentation of a fibroma resulting in gradual pulp enlargement of the digit.

Figure: Lateral view demonstrating the asymmetric volar swelling caused by the underlying fibroma.
Tourniquet management is perhaps the most critical preoperative variable. For solid tumors like GCTTS, fibromas, and glomus tumors, standard exsanguination with an Esmarch bandage followed by pneumatic tourniquet inflation (typically 250 mmHg) provides the necessary bloodless field. However, for cavernous hemangiomas, the "Partial Exsanguination" technique is strictly required. The surgeon must not tightly exsanguinate the limb with an Esmarch bandage. Instead, the arm is simply elevated for 2 to 3 minutes before inflating the pneumatic tourniquet. This deliberate technique allows residual blood to partially fill the cavernous sinuses. Intraoperatively, this trapped blood outlines the true extent of the tumor with a distinct bluish hue, making it significantly easier to differentiate the delicate vascular malformation from surrounding healthy adipose and muscle tissue.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to hand tumors requires a mastery of soft tissue handling, utilizing magnification (loupes or an operating microscope) to ensure complete marginal excision while preserving the microscopic arborizations of the digital nerves and vessels.
Excision of Cavernous Hemangioma
The surgical extirpation of a cavernous hemangioma begins with the aforementioned partial exsanguination technique. Depending on the tumor's location, a Brunner zigzag incision or a mid-axial incision is utilized. The Brunner incision prevents postoperative linear scar contractures across the flexion creases. Once the skin flaps are elevated, the surgeon encounters the bluish, engorged venous sinuses. Meticulous, blunt and sharp dissection is required to peel the malformation away from the neurovascular bundles. Bipolar electrocautery is essential to systematically ligate the feeding vessels without causing thermal necrosis to adjacent nerves. In cases of massive, diffuse infiltration where a single-stage removal would compromise the vascular viability of the digit, a staged procedure is mandated. During the first stage, the primary feeding branches are ligated, and the tumor is partially debulked. This induces ischemic shrinkage of the remaining lesion, allowing for a safer, more definitive second-stage excision several months later.
Subungual Glomus Tumor Excision
The transungual approach is the standard of care for subungual glomus tumors. Following digital block anesthesia and the application of a sterile finger tourniquet, a periosteal elevator or curved tenotomy scissors are used to gently separate the nail plate from the underlying sterile matrix and the overlying eponychial fold. The nail plate is completely removed and preserved in sterile saline. The sterile matrix is then inspected under magnification; the tumor typically presents as a 2 to 5 millimeter bluish or purple discoloration. A longitudinal incision is made directly over the mass through the sterile matrix. Transverse incisions are strictly avoided to prevent disruption of the longitudinal growth pattern of the nail. The glomus tumor is usually well-encapsulated and can be carefully enucleated using a small curette or fine tenotomy scissors. Following enucleation, the sterile matrix must be meticulously repaired using 6-0 or 7-0 absorbable sutures (e.g., chromic gut or Vicryl Rapide). Finally, the native nail plate (or a silicone substitute) is fenestrated to allow hematoma egress and placed back into the eponychial fold to stent the matrix open, preventing synechiae formation during healing.
Marginal Excision of GCTTS and Fibromas
For solid tumors like GCTTS and digital fibromas, marginal excision is the definitive treatment.

Figure: Clinical presentation of a Giant Cell Tumor on the flexor surface of the ring finger, demonstrating a firm, lobulated mass.
Figure: Midline palmar oblique approach marked over the volar aspect of the affected digit.
A Brunner or midline palmar oblique incision is marked and executed. The skin flaps are elevated full-thickness to protect the subdermal vascular plexus.
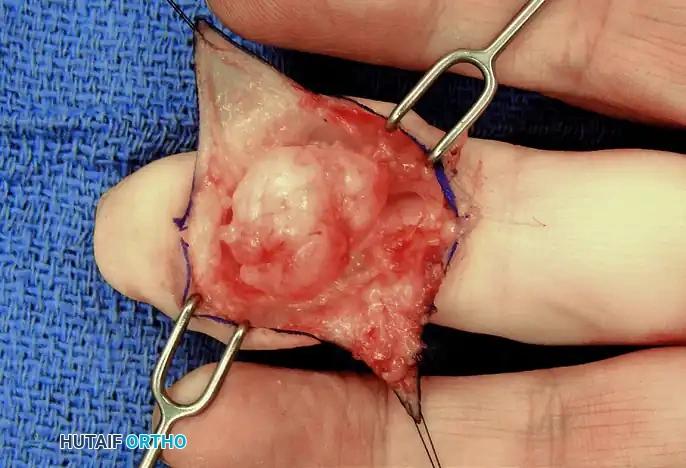
Figure: Exposure of the well-encapsulated fibroma tumor in situ, demonstrating displacement of the local subcutaneous tissues.
During the dissection of a GCTTS, the mass is easily identifiable by its characteristic yellowish-brown, lobulated appearance, a result of dense hemosiderin deposition. The digital nerve and artery are often displaced or draped over the tumor capsule. These structures must be identified proximally in normal tissue and traced distally, gently retracting them with vessel loops.
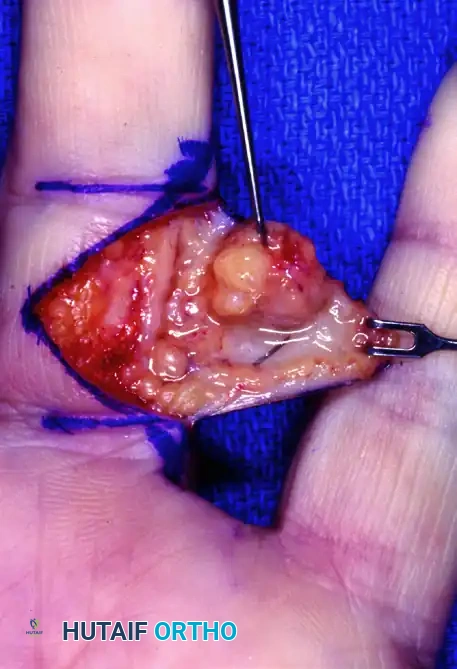
Figure: Surgical dissection showing a well-encapsulated giant cell tumor with its typical yellowish-brown color, carefully separated from the digital neurovascular bundle.
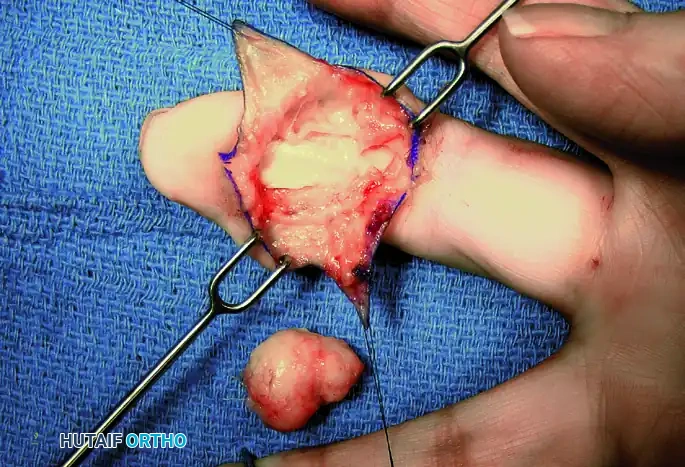
Figure: Marginal excision of the tumor, carefully peeling the capsule away from the underlying flexor tendon sheath.
The tumor is then sharply excised from its origin on the flexor tendon sheath or joint capsule. It is critical to inspect the adjacent joints, particularly the distal interphalangeal (DIP) joint, to ensure no satellite lesions or "collar-button" extensions are left behind, as retained fragments are the primary cause of recurrence.
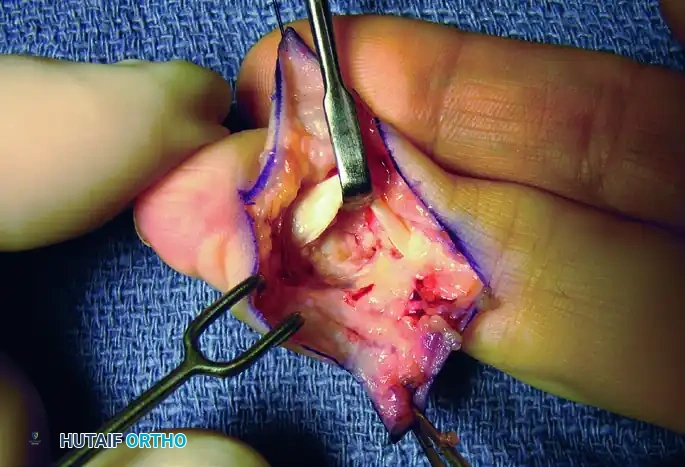
Figure: Final inspection of the distal interphalangeal (DIP) joint and flexor sheath for any additional tumor deposits prior to closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of hand soft tissue tumors carries a distinct profile of postoperative complications. The dense architectural constraints of the hand mean that even minor postoperative edema or scarring can translate into significant functional deficits. The surgeon must be intimately familiar with these risks to adequately counsel patients and implement rapid salvage protocols when necessary.
For cavernous hemangiomas, the most frustrating complication is tumor persistence or recurrence. Because these malformations often lack a true histological capsule and interdigitate with normal muscular and adipose tissues, achieving negative microscopic margins without sacrificing vital structures is frequently impossible. Recurrence rates for diffuse cavernous hemangiomas can approach 20% to 30%. When recurrence occurs and becomes symptomatic, salvage management typically involves targeted sclerotherapy, embolization, or repeat debulking. Radiation therapy, while historically used for recalcitrant vascular lesions, is now strongly discouraged for benign cavernous hemangiomas of the hand due to an unacceptably high risk of radiation-induced fibrosis, joint contractures, delayed skin necrosis, and the catastrophic potential for secondary malignant transformation into angiosarcoma.
Glomus tumor excision is highly successful in eradicating pain, but it carries specific risks related to the nail apparatus. The most common complication is postoperative nail dystrophy, including longitudinal ridging or a split nail deformity. This occurs if the germinal matrix is inadvertently injured during dissection or if the sterile matrix is not meticulously reapproximated. The incidence of nail deformity ranges from 5% to 15%. Salvage management for a symptomatic split nail requires re-operation to excise the scarred matrix and perform a sterile matrix graft, typically harvested from the ipsilateral great toe. Furthermore, recurrence of glomus tumor symptoms occurs in approximately 10% of cases. Early recurrence (within weeks) typically indicates incomplete excision, whereas late recurrence (after several years) suggests the development of a synchronous, separate glomus tumor, demanding repeat MRI evaluation and enucleation.
GCTTS is notorious for its high recurrence rate, which is reported to be between 10% and 45% in the literature, depending on the length of follow-up and the thoroughness of the initial marginal excision. Factors predisposing to recurrence include the presence of degenerative joint disease in the adjacent articulation, tumor extension into the interphalangeal joint capsule, and the presence of occult satellite lesions. To mitigate this, aggressive marginal excision utilizing magnification is mandatory. If recurrence occurs, revision excision is the standard salvage pathway, occasionally supplemented by localized adjuvant radiotherapy in multiply recurrent, highly aggressive, but histologically benign cases.
| Tumor Type | Primary Complications | Incidence Rate | Salvage Management Strategy |
|---|---|---|---|
| Cavernous Hemangioma | Persistence/Recurrence, Hematoma, Digital Ischemia | 20% - 30% | Repeat debulking, sclerotherapy, localized embolization. Avoid radiation. |
| Glomus Tumor | Nail dystrophy (split nail, ridging), Recurrence, Matrix scarring | 5% - 15% | Sterile matrix grafting (from great toe), repeat MRI and revision enucleation. |
| GCTTS | Local recurrence, Digital stiffness, Tendon adhesion | 10% - 45% | Revision marginal excision, aggressive hand therapy, tenolysis if required. |
| MPNST (NF1) | Metastasis, Local recurrence, High mortality | Variable | Wide oncologic resection, amputation, adjuvant chemo/radiotherapy. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome following the excision of any hand tumor is as heavily dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The primary goals of the rehabilitation phase are to minimize debilitating edema, prevent flexor tendon adhesions, restore full active and passive range of motion, and manage scar tissue hypersensitivity. Regardless of whether the excised tumor was a hemangioma, glomus, GCTTS, or fibroma, a standardized, phased approach is universally applied.
Phase I: Immobilization and Edema Control (Days 0 to 5)
Immediately following wound closure in the operating room, a bulky, non-compressive soft dressing is applied, reinforced with a volar plaster or fiberglass orthosis. The hand is strictly immobilized in the intrinsic-plus position—frequently referred to as the "safe position." This requires the wrist to be extended 20 to 30 degrees, the metacarpophalangeal (MCP) joints flexed to 70 to 90 degrees, and the interphalangeal (IP) joints maintained in full extension. Biomechanically, this position places the collateral ligaments of the MCP joints at their maximal length (preventing extension contractures) and maintains the volar plates of the IP joints under tension (preventing flexion contractures). Strict elevation of the extremity above the level of the heart is mandated for the first 48 to 72 hours to minimize throbbing pain, venous congestion, and hematoma formation.
Phase II: Early Mobilization and Wound Healing (Days 6 to 14)
Once the initial inflammatory phase subsides, the bulky surgical dressing is removed. If the wound is healing without signs of dehiscence or active infection, a lighter dressing is applied, and the patient is transitioned to a removable custom thermoplastic splint. Under the direct supervision of a certified hand therapist (CHT), active and active-assisted range of motion (ROM) exercises are initiated. Early mobilization is critical, particularly following the excision of GCTTS or hemangiomas that intimately involve the flexor tendon sheath, to facilitate tendon gliding and prevent restrictive tenosynovial adhesions. Tendon gliding exercises (straight fist, hook fist, and composite fist) are performed multiple times daily. Suture removal is typically scheduled between 10 to 14 days postoperatively, contingent upon complete epithelialization of the incision.
Phase III: Scar Management and Desensitization (Weeks 3 to 8)
As the wound fully matures, the focus of rehabilitation shifts toward scar management and sensory re-education. Aggressive retrograde scar massage is initiated using emollients to break down underlying collagen cross-linking and prevent perineural fibrosis around the digital nerves. Silicone gel sheeting is highly recommended to flatten and soften the surgical
