Congenital Arteriovenous Fistulas & Hand Lesions: Surgical Guide
Key Takeaway
Congenital arteriovenous fistulas and tumor-like lesions of the hand require meticulous surgical management. This comprehensive guide details the pathophysiology, diagnostic imaging, and step-by-step operative techniques for arteriovenous fistulas, pyogenic granulomas, gouty tophi, and traumatic neuromas. Emphasizing evidence-based approaches, it provides orthopedic surgeons with critical insights into microvascular dissection, nerve transposition, and soft tissue reconstruction to optimize functional outcomes and minimize postoperative complications.
Comprehensive Introduction and Patho-Epidemiology
The upper extremity is uniquely susceptible to a diverse array of vascular, inflammatory, and neoplastic-like lesions that present significant diagnostic and therapeutic challenges to the orthopedic surgeon. Among the most hemodynamically complex are congenital arteriovenous fistulas (CAVFs). These lesions represent a profound structural anomaly resulting from the embryological failure of the common vascular anlage to differentiate into distinct, mature arterial and venous channels. Occurring predominantly between the fourth and tenth weeks of gestation, this arrest in vascular organogenesis yields persistent, abnormal macroscopic and microscopic shunts between the high-pressure arterial system and the low-pressure venous circulation, entirely bypassing the intervening capillary beds. The epidemiological prevalence of isolated upper extremity CAVFs remains low, but their clinical impact is disproportionately severe, often manifesting within the first two decades of life and exhibiting a slight female predominance.
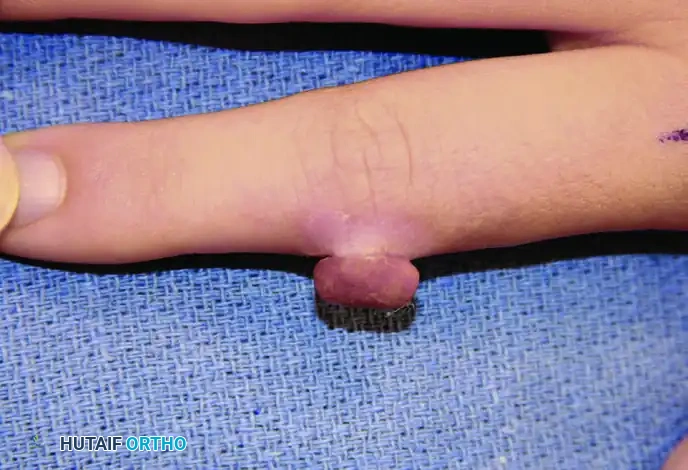
Beyond true vascular malformations, the hand surgeon frequently encounters highly vascularized pseudotumors, most notably the pyogenic granuloma. Despite its deeply entrenched historical misnomer, a pyogenic granuloma is neither infectious (pyogenic) nor granulomatous in its histopathology. It is formally classified as a lobular capillary hemangioma—a benign, rapidly growing vascular proliferation of granulation tissue. Epidemiologically, these lesions exhibit a bimodal distribution, frequently erupting in children and young adults, as well as pregnant women (granuloma gravidarum), strongly suggesting a hormonal catalyst acting synergistically with minor, often unnoticed penetrating trauma. The resultant lesion is a friable, erythematous nodule that overhangs the surrounding normal epidermis, characterized by an unstable, highly vascular nature that renders it prone to profuse, recurrent hemorrhage with minimal mechanical provocation.
Inflammatory and reactive lesions further complicate the differential diagnosis of hand masses. Foreign body granulomas represent a chronic, localized inflammatory response to retained exogenous material, such as wood splinters, glass, metallic fragments, or retained suture material. When the innate immune system, specifically macrophages, cannot enzymatically degrade or phagocytose the foreign nidus, they undergo fusion to form multinucleated foreign-body giant cells. Fibroblasts are subsequently recruited via a cascade of cytokines, encapsulating the offending agent within a dense, firm, fibrous capsule. Similarly, gouty arthropathy introduces a metabolic etiology to soft tissue and osseous lesions. Driven by systemic hyperuricemia, monosodium urate (MSU) crystals precipitate within joints, ligaments, tendons, and subcutaneous tissues. In advanced, poorly controlled disease, massive tophaceous deposits accumulate, triggering a profound inflammatory cascade that activates osteoclasts and inhibits osteoblasts, leading to aggressive, localized bone resorption that can easily mimic primary osseous malignancies or chronic osteomyelitis.
Finally, the peripheral nervous system contributes its own distinct pathology in the form of traumatic neuromas. A traumatic neuroma is not a true neoplasm; rather, it is a disorganized, hyperplastic proliferation of axons, Schwann cells, and perineurial fibroblasts occurring secondary to the complete or partial transection of a peripheral nerve. Following nerve injury, the distal segment undergoes Wallerian degeneration, while the proximal stump attempts regeneration via axonal growth cones. If these regenerating fibers fail to bridge the gap to the distal stump—due to interposing scar tissue, wide physical separation, or amputation—they coil into a tangled, bulbous mass. This creates an exquisitely tender, mechanosensitive lesion that severely impairs hand function. Less commonly, the surgeon may encounter rare neuropathies such as Déjérine-Sottas disease (Charcot-Marie-Tooth disease type 3), characterized by "onion bulb" formations of Schwann cells, or calcinosis circumscripta, which involves the deposition of insoluble calcium phosphate lobules within the ischemic subcutaneous tissues of patients with autoimmune connective tissue disorders like the CREST variant of scleroderma.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of a congenital arteriovenous fistula is defined by its chaotic, microscopic, and diffuse anomalous communications, collectively termed the nidus. Unlike acquired traumatic fistulas, which typically present as a single, distinct communication between a major artery and a corresponding vein, CAVFs feature a complex arborization of feeding arteries and draining veins that lack normal structural integrity. Biomechanically, the presence of these anomalous shunts drastically alters local and regional hemodynamics. The shunting of arterial blood directly into the venous system leads to localized venous hypertension, venous engorgement, and secondary varicosities. The veins, unequipped to handle arterial pressures, undergo reactive intimal hyperplasia and smooth muscle hypertrophy, a process known as "arterialization."
The diversion of flow through the low-resistance fistulous nidus induces a profound "steal phenomenon." According to Poiseuille's law, fluid will follow the path of least resistance; thus, the distal capillary beds are systematically deprived of adequate perfusion. This chronic diversion leads to distal tissue ischemia, delayed wound healing, and chronic secondary ulceration. Furthermore, the increased regional blood flow often stimulates asymmetric limb hypertrophy—both in soft tissue and bone—a hallmark of conditions such as Parkes Weber syndrome. Unlike glomus tumors, which are exquisitely painful due to their rich sympathetic innervation and location within the neurovascular glomus body, uncomplicated CAVFs are typically painless. However, secondary ischemic ulcerations, localized infections, or the sheer mass effect of the engorged vessels can incite severe nociceptive pain.
In the context of pyogenic granulomas, the surgical anatomy is deceptively complex. While the lesion appears as a superficial, pedunculated, or sessile exophytic mass, its critical anatomy lies deep to the epidermal surface. The lesion is surrounded by a characteristic collarette of hyperplastic epidermis, but the true driver of the lobular capillary hemangioma is its deep vascular base, which extends vertically into the subcutaneous tissue. Failure to recognize and anatomically resect this deep feeding pedicle is the primary biomechanical and anatomical reason for the unacceptably high recurrence rates associated with superficial shave excisions or chemical cauterization.
Gouty arthropathy presents a vastly different anatomical challenge. Tophaceous deposits exhibit a predilection for relatively avascular tissues, such as tendon sheaths, bursae, and articular cartilage. In the hand, flexor tenosynovial tophi are particularly problematic. The chalky, toothpaste-like urate deposits infiltrate the paratenon and the tendon substance itself, mechanically restricting excursion within the retinacular pulley system and frequently precipitating acute carpal tunnel syndrome via volume expansion within the inextensible carpal canal. Radiographically, the massive bone destruction caused by osteoclast activation manifests as well-defined, "punched-out" lytic lesions in the metaphysis and diaphysis, often with sclerotic margins and overhanging edges of cortical bone, classically known as Martel's sign.

The anatomy of a traumatic neuroma is rooted in the microarchitecture of the peripheral nerve. A normal peripheral nerve consists of axons bundled into fascicles, surrounded by the endoneurium, perineurium, and epineurium. In a neuroma, this organized architecture is entirely lost. The tangled mass of regenerating axons and proliferating Schwann cells lacks the protective perineurial barrier, rendering the naked axons highly susceptible to mechanical stimulation and ectopic spontaneous discharge. Biomechanically, neuromas located in superficial, unpadded areas (such as a digital amputation stump) are subjected to constant compressive and shear forces during normal hand use, translating directly into debilitating neuropathic pain.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for complex hand lesions must be meticulously weighed against the inherent risks of neurovascular compromise, wound healing failure, and lesion recurrence. The diffuse nature of congenital arteriovenous fistulas, the ischemic environment of calcinosis circumscripta, and the systemic metabolic derangements of gout require a highly tailored approach.
Indications and Contraindications for Surgical Management
| Pathology | Absolute Indications | Relative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Congenital Arteriovenous Fistula (CAVF) | Impending/active tissue necrosis (gangrene); High-output cardiac failure; Uncontrollable hemorrhage. | Recalcitrant ischemic ulceration; Severe functional impairment; Disabling pain. | Inability to achieve en bloc resection (partial excision guarantees exacerbation). | Asymptomatic lesions; Diffuse infiltration involving critical motor nerves without limb-threatening ischemia. |
| Pyogenic Granuloma | Recurrent, profuse hemorrhage; Diagnostic uncertainty (need to rule out amelanotic melanoma). | Functional impairment due to location; Cosmetic deformity causing severe distress. | None. | Active, untreated local cellulitis (requires antibiotic optimization prior to excision). |
| Foreign Body Granuloma | Chronic, draining sinus tract; Superimposed deep space infection; Proximity to neurovascular structures causing compression. | Painful palpable mass; Restriction of tendon excursion. | None. | Asymptomatic, deeply embedded, inert radiopaque foreign bodies (e.g., small metallic fragments). |
| Gouty Arthropathy (Tophi) | Impending/actual skin necrosis over a massive tophus; Acute compression neuropathy (e.g., Carpal Tunnel Syndrome). | Severe pain/functional block; Joint destruction requiring arthrodesis. | Medically unoptimized acute gout flare (unless compartment syndrome or severe infection is suspected). | Poor soft tissue envelope with high risk of postoperative necrosis; Uncontrolled hyperuricemia. |
| Traumatic Neuroma | Intractable, mechanosensitive pain refractory to conservative measures (desensitization, gabapentinoids). | Interference with prosthetic fitting; Severe phantom limb pain amenable to TMR. | Active regional pain syndrome (CRPS) lacking isolated neuroma pathology. | Poorly motivated patient; Inadequate soft tissue bed for transposition. |
| Calcinosis Circumscripta | Intractable pain; Severe mechanical interference with grip; Chronic, draining ulcerations. | Impending skin erosion. | Extensive surgical dissection in the setting of severe, unoptimized Raynaud's ischemia. | Asymptomatic deposits; Diffuse miliary calcifications not amenable to focal excision. |
The surgical eradication of CAVFs is notoriously challenging. Partial excision inevitably leads to rapid recurrence, exacerbation of collateral flow, and a worsening of the steal phenomenon. Therefore, if preoperative imaging indicates that en bloc resection is anatomically impossible without sacrificing the functional viability of the limb, surgical extirpation is contraindicated, and palliative endovascular embolization remains the primary modality. Similarly, in calcinosis circumscripta associated with CREST syndrome, the surrounding soft tissues are typically profoundly ischemic due to underlying microvascular disease. Extensive surgical dissection frequently results in catastrophic wound breakdown, delayed healing, and secondary osteomyelitis. Therefore, surgery must be strictly limited to the conservative, partial excision of the most prominent, symptomatic calcific lobules.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful outcomes in the surgical management of complex upper extremity lesions. For congenital arteriovenous fistulas, clinical suspicion should be high in patients presenting with unilateral upper extremity varicosities, localized elevated skin temperature, palpable thrills, or continuous machinery murmurs. Definitive diagnosis and surgical mapping rely heavily on advanced imaging modalities. Digital Subtraction Angiography (DSA) remains the gold standard. It reveals the precise architectural anatomy in real-time, demonstrating proximal arterial dilation, rapid and abnormal filling of the distal arterial tree, early venous opacification, and the exact location and extent of the fistulous nidus. Magnetic Resonance Angiography (MRA) is an essential adjunct, providing excellent soft-tissue contrast to evaluate the extent of muscle, fascial, and bone involvement without ionizing radiation.
Once the CAVF architecture is mapped, a multidisciplinary approach involving interventional radiology is mandatory. Preoperative endovascular embolization is often performed 24 to 48 hours prior to surgical resection. Utilizing coils, Onyx, or n-butyl cyanoacrylate (NBCA) glue, major feeding vessels are occluded. This critical step significantly reduces intraoperative hemorrhage, shrinks the nidus, and delineates the margins of the malformation, making subsequent en bloc resection technically feasible.
For gouty arthropathy, dual-energy computed tomography (DECT) has revolutionized preoperative planning. DECT can specifically identify and color-code monosodium urate deposits, allowing the surgeon to accurately map the extent of intratendinous and intra-articular tophaceous infiltration prior to making an incision. In cases of foreign body granulomas, while radiopaque materials (glass, metal) are easily identified on standard orthogonal radiographs, radiolucent materials (wood, thorns) require high-resolution ultrasonography or MRI for precise three-dimensional localization to minimize surgical exploration time.
Patient positioning is critical for optimal access and intraoperative flexibility. The patient is positioned supine with the operative arm extended onto a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm. In the case of CAVFs, the tourniquet may be left uninflated initially. This allows the surgeon to visually and palpably identify the pulsatile fistulous tracts and engorged draining veins under normal hemodynamic conditions. Once the lesion is mapped on the skin with a surgical marker, the arm is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to provide a bloodless field. Loupe magnification (minimum 3.5x) or an operating microscope is positioned, and a microsurgical instrument tray must be immediately available.
Step-by-Step Surgical Approach and Fixation Technique
Excision of Congenital Arteriovenous Fistulas
The surgical approach to a CAVF requires meticulous, unhurried dissection. Following tourniquet inflation, an expansile incision is made, often incorporating previous biopsy scars or overlying ischemic skin that requires excision. Utilizing loupe magnification, the surgeon must meticulously trace and ligate all feeding arteries and draining veins immediately adjacent to the nidus. Bipolar electrocautery, fine silk ties, and titanium microsurgical clips are employed extensively. The entire vascular malformation must be excised en bloc. The surgeon must resist the temptation to enter the nidus, as this will precipitate uncontrollable hemorrhage upon tourniquet deflation and guarantee incomplete resection.
Extensive resections often leave significant soft-tissue defects. Primary closure is rarely possible without undue tension, which would precipitate skin necrosis. Staged procedures are frequently required. The wound may be temporarily managed with negative pressure wound therapy (NPWT) to stimulate a healthy granulating bed. Definitive soft tissue reconstruction is then achieved utilizing full-thickness skin grafting, regional pedicled flaps (e.g., radial forearm flap), or free tissue transfer (e.g., anterolateral thigh flap), depending on the volume of the defect and the exposure of underlying neurovascular or tendinous structures.
Extirpation of Pyogenic Granulomas
Definitive management of a pyogenic granuloma requires formal surgical excision; conservative measures like silver nitrate cauterization yield unacceptably high recurrence rates. Under a digital block using 1% lidocaine without epinephrine (to avoid exacerbating digital ischemia), the digit is prepped. A simple shave excision is inadequate. The surgeon must perform a full-thickness elliptical excision utilizing a #15 blade. The ellipse must encompass the entire exophytic lesion, the surrounding collarette of hyperplastic skin, and, crucially, the deep vascular base extending into the subcutaneous tissue down to the level of the superficial fascia.

Following excision, meticulous hemostasis is achieved with bipolar cautery. The defect is closed primarily with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 nylon) using vertical mattress techniques to ensure eversion of the skin edges. If the defect is too large for primary closure without tension, a small full-thickness skin graft, harvested from the hypothenar eminence or the volar wrist crease, should be applied and secured with a tie-over bolster dressing. All excised specimens must be sent for histopathological examination to rule out amelanotic melanoma or squamous cell carcinoma.
Management of Gouty Tophi and Foreign Body Granulomas
Surgical intervention for massive gouty tophi requires a delicate balance between adequate debridement and tissue preservation. Incisions must be planned carefully, as the skin overlying large tophi is often attenuated, ischemic, and prone to postoperative necrosis. Once the skin flaps are elevated, the tophi are meticulously enucleated. The chalky urate deposits are curetted from the bone and soft tissues. When debriding intratendinous tophi, extreme care must be taken to preserve the continuity of the tendon and its paratenon. Aggressive resection can lead to iatrogenic tendon rupture. Dead space must be minimized during closure, and non-viable overlying skin must be excised, leaving the wound to heal by secondary intention or covering it with a local flap.
For foreign body granulomas, surgical removal is curative. Under regional anesthesia and tourniquet control, an incision is made directly over the palpable mass. The dense fibrous capsule is incised, and the granulomatous tissue, along with the centralized foreign nidus, is completely excised en bloc. Thorough irrigation and sharp debridement of the surrounding reactive tissue are mandatory before primary closure to prevent secondary infection or sterile sinus tract formation.
Neuroma Transposition and Targeted Muscle Reinnervation
The goal of neuroma surgery is not to prevent neuroma formation—which is a physiological inevitability of a cut nerve—but to relocate the neuroma to a protected, asymptomatic environment. The neuroma is identified and sharply excised back to healthy, organized fascicular tissue using a fresh #15 blade or nerve scissors.
For simple transposition, the proximal nerve stump is mobilized and buried deep within a well-vascularized muscle belly (e.g., transposing a superficial radial nerve neuroma into the brachioradialis muscle) or implanted into a drilled hole in adjacent bone. This shields the regenerating nerve ending from mechanical stimulation. Alternatively, Targeted Muscle Reinnervation (TMR) may be employed. In this advanced technique, the proximal nerve stump is transferred and coapted to a nearby redundant motor branch of a muscle using 8-0 or 9-0 epineurial sutures and fibrin glue. This provides the regenerating axons with a physiological target, preventing neuroma formation and significantly reducing both localized and phantom limb pain.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for these complex lesions carries a significant risk profile. Complications can arise from the underlying pathology itself, technical errors during excision, or failures in soft tissue reconstruction.
Complication Matrix and Salvage Protocols
| Complication | Associated Pathology | Estimated Incidence | Etiology / Risk Factors | Salvage Management |
|---|---|---|---|---|
| Massive Hemorrhage | CAVF | 5 - 15% | Incomplete embolization; Inadvertent entry into the fistulous nidus; Premature tourniquet deflation. | Immediate manual pressure; Re-inflation of tourniquet; Proximal vascular control; Application of hemostatic agents (e.g., Floseal); Ligation of main feeding trunks. |
| Rapid Lesion Recurrence | CAVF, Pyogenic Granuloma | 20 - 40% (CAVF) / 10% (PG) | Partial or subtotal excision; Failure to resect the deep vascular base of a pyogenic granuloma. | Re-imaging (DSA/MRA); Revision en bloc resection; Wide elliptical excision for PG recurrence; Consideration of amputation for recalcitrant, limb-threatening CAVF. |
| Iatrogenic Tendon Rupture | Gouty Arthropathy | 5 - 10% | Over-aggressive curettage of intratendinous tophi; Compromise of the paratenon leading to avascular necrosis of the tendon. | Tendon transfer (e.g., EIP to EPL); Intercalary tendon grafting (e.g., palmaris longus); Tenodesis or joint arthrodesis if grafting is unfeasible. |
| Wound Dehiscence / Skin Necrosis | Gout, Calcinosis Circumscripta | 15 - 25% | Closure under tension; Incision through attenuated, ischemic skin overlying tophi; Underlying microvascular disease (Raynaud's). | Debridement of necrotic tissue; Negative Pressure Wound Therapy (NPWT); Healing by secondary intention; Local or regional flap coverage. |
| Recurrent Neuropathic Pain | Traumatic Neuroma | 10 - 20% | Failure to transpose the nerve stump deep to muscle/bone; Inadequate resection of the proximal diseased fascicles. | Revision exploration; Resection of recurrent neuroma; Implementation of Targeted Muscle Reinnervation (TMR) or regenerative peripheral nerve interfaces (RPNIs). |
| Infection / Osteomyelitis | Foreign Body Granuloma, Calcinosis | 2 - 8% | Retained organic foreign material (wood); Chronic draining ulcerations over calcific deposits. | Aggressive serial surgical debridement; Hardware removal if present; Intravenous culture-directed antibiotic therapy; Bone resection/amputation in refractory cases. |
The most devastating complication in the management of CAVFs is rapid, aggressive recurrence following incomplete resection. The resulting hemodynamics often feature an exacerbated steal phenomenon and a more diffuse, chaotic nidus that is exponentially more difficult to treat. Salvage management in these scenarios requires a return to the multidisciplinary board, repeat high-resolution angiography, and often necessitates radical resection, up to and including major limb amputation, to prevent high-output cardiac failure or fatal hemorrhage.
In the treatment of pyogenic granulomas, the primary surgical pitfall is a failure to send the excised specimen for histopathological examination. Amelanotic melanoma can perfectly mimic a pyogenic granuloma clinically. A missed diagnosis due to discarded tissue is a catastrophic medico-legal and oncological error.
Phased Post-Operative Rehabilitation Protocols
Post-operative rehabilitation must be strictly tailored to the specific lesion excised and the nature of the soft tissue reconstruction. A generalized, phased approach is utilized, modified heavily by the presence of skin grafts, flaps, or nerve transpositions.
Phase 1: Protection and Tissue Healing (Weeks 0 to 2)
The primary goal in the immediate postoperative period is the protection of the surgical repair, prevention of hematoma formation, and optimization of wound healing.
* Immobilization: Following extensive CAVF resections, flap reconstructions, or gout tophi enucleations, the extremity is immobilized in a bulky, non-compressive intrinsic-plus splint (wrist in 20 degrees extension, MCPs in 70 degrees flexion, IPs fully extended).
* Edema Control: Strict elevation of the extremity above the level of the heart is mandatory to minimize venous congestion, particularly crucial after the excision of vascular anomalies.
* Wound Care: Dressings remain intact for the first 5-7 days unless signs of infection or excessive strike-through bleeding occur. For pyogenic granuloma excisions closed primarily, simple protective bandaging is sufficient.
Phase 2: Early Mobilization and Scar Management (Weeks 2 to 6)
Once sutures are removed and the incisions are deemed stable, the focus shifts to restoring glide and preventing restrictive adhesions.
* Range of Motion (ROM): Active and active-assisted ROM exercises are initiated. Following gouty tophi removal from flexor tendons, early protected active mobilization is critical to prevent dense tenosynovial adhesions.
* Scar Management: Aggressive scar massage, silicone sheeting, and compression garments (e.g., Isotoner gloves) are introduced to soften the surgical scar and manage residual edema.
* Desensitization: For patients recovering from neuroma resection and transposition, a formal desensitization program is initiated. This involves bombarding the peripheral nervous system with varying textures (silk, cotton, Velcro), temperatures, and localized vibration to raise the threshold for mechanosensitive pain and integrate the newly transposed nerve ending.
Phase 3: Functional Restoration and Strengthening (Weeks 6 to 12)
As tissue tensile strength normalizes, rehabilitation transitions to functional recovery.
* Strengthening: Progressive resistive exercises utilizing putty, hand dynamometers, and free weights are incorporated.
* Work Conditioning: Therapy is tailored to the patient's specific occupational demands. For patients with calcinosis circumscripta or gout, therapy must also include joint protection strategies and ergonomic modifications to prevent recurrent mechanical trauma to susceptible areas.
* Monitoring: Patients are closely monitored for signs of lesion recurrence (e.g., return of pulsatile masses in CAVF, recurrent exophytic growth in pyogenic granuloma, or localized Tinel's sign in neuroma), which necessitates immediate surgical re-evaluation.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of vascular and pseudotumorous lesions of the upper extremity is guided by several foundational texts and classification systems. The International Society for the Study of Vascular Anomalies (ISSVA) classification remains the definitive framework for distinguishing true congenital arteriovenous fistulas (vascular malformations with endothelial cell turnover proportional to somatic growth) from infantile hemangiomas and benign reactive proliferations like pyogenic granulomas (lobular capillary hemangiomas). This distinction is critical, as it dictates the necessity of preoperative embolization and the absolute requirement for en bloc resection in CAVFs.
In the realm of peripheral nerve surgery, the pioneering work by Dumanian et al. on Targeted Muscle Reinnervation (TMR) has revolutionized the management of traumatic neuromas. Their clinical guidelines establish that providing a physiological motor target for regenerating sensory axons significantly outperforms traditional simple transposition techniques in reducing both localized neuroma pain and phantom limb phenomena.
For metabolic and reactive lesions, the American College of Rheumatology (ACR) guidelines emphasize the utility of Dual-Energy CT (DECT) in the preoperative mapping of gouty tophi, allowing for precise, tendon-sparing surgical approaches. Furthermore, oncological guidelines universally mandate the histopathological evaluation of all excised pyogenic granulomas, driven by landmark case series demonstrating the devastating consequences of misdiagnosed amelanotic melanomas masquerading as benign vascular lesions. Adherence to these established protocols ensures a comprehensive, safe, and biologically sound approach to these complex upper extremity pathologies.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicin" ---
